
Abstract
Much of the practice of nursing continues to be based on tacit rather than explicit knowledge, with children’s nursing practice worldwide nuanced by local cultures of caring. The development of Afrocentric nursing practice models and tools challenges researchers to find methods which enable promising local practices to be identified and described. Visual research methods are an emerging approach within nursing and health research. However, detailed accounts of the implementation of these methods in clinical nursing settings are scarce. Visual methods (graphic facilitation, sociograms, and photographic elicitation) formed a core part of the data collection strategy for a qualitative observational study of nursing practices in relation to the involvement of families in the care of their hospitalized children in Southern Africa. We draw on this experience to provide a detailed account of the implementation of these methods and reflect on their effectiveness. Practical suggestions for using visual methods applicable to a variety of clinical nursing settings are offered based on implementation experience. We advocate that the use of these methods within the context of health research requires better anticipation of specific ethical considerations. We conclude that visual methods can contribute usefully to the development of new models of nursing practice, with strengths that include helping to anchor dialogue, supporting the articulation of conceptually rich practice narratives and explanations, and acting as a useful adjunct to communication between nurses and researchers.
Keywords
Introduction
To work most effectively, nurses need knowledge of contextually specific best practice nursing models which are aligned with the needs, resources, and cultures of the environments in which they practice. Context plays an important role in the education of health-care professionals. Benner describes clinical practice as socially embedded knowledge which often relies on practical know-how and compassionate meeting of the other (Benner & Benner, 1999). Children’s nurses in Africa work in contexts that are very different to those of the global North where “best practice” guidelines are usually researched and guidelines are formulated on the research in those settings. Material specific to the global North continues to be deeply valued and underpins most nursing education provided in Africa. There is however a growing awareness that the development of specifically African nursing knowledge, as well as the transfer of useful learning, can be impeded by a situation where the nations of the global North have continued to export ideas and import people (Crisp, 2010).
While the importance of developing Afrocentric nursing models and tools to support evidence-based safe nursing practice is increasingly recognized (World Health Organization [WHO], 2016), the process of developing these models remains a challenge. As nursing researchers and educators working to build children’s nursing capacity in Africa, we aim to equip Africa’s nurses with evidence-based, context-specific, and culturally aligned practice development tools which are designed, evaluated, and implemented in the continent’s health-care settings.
The process of researching nursing practice in African settings requires the selection of methods which are sufficiently sensitive to complex social, professional, and organizational cultural factors. As researchers working in this context, we became increasingly curious about the potential for visual research methods to support the identification and articulation of tacit and socially embedded, often “invisible,” nursing knowledge. In this article, we report in some depth on our experiences of applying these visual methods within the context of one particular study. This article is organized as follows.
– Firstly, background information about the current state of the application of visual methods to nursing research is provided, highlighting reported strengths and gaps in the knowledge base.
– Next, we briefly explore the challenges and barriers to uncovering evidence of “real” nursing knowledge, practices, and ethics in South Africa’s historically and politically complex society, explaining our interest in whether visual methods could contribute to Afrocentric nursing knowledge development.
– The main body of this article takes the form of practically oriented accounts of how we applied multiple visual and image-based research methods in practice. Beginning with a very brief overview of the study design, the implementation of the three visual methods (graphic facilitation, sociograms, and photographic elicitation) is then described in turn, with examples of the type of data generated. We also consider the benefits of using different visual methods in combination.
– Finally, we discuss our collective learning through the process and share our tentative reflections about the potential benefits of applying visual methods in qualitative nursing research, including Afrocentric nursing research.
Background
Visual Methods and Nursing Research
While interest in visual research methods is growing, it appears that visual research methods remain underutilized in nursing research (Byrne, Daykin, & Coad, 2016; Glaw, Inder, Kable, & Hazelton, 2017). A review of the literature in 2004 by Riley and Manias (2004) identified limited examples of visual research in clinical nursing settings. A subsequent review by Byrne, Daykin, and Coad (2016) identified no additional new publications directly concerned with the application of visual research methods to clinical nursing practice.
The literature in this field includes a small number of studies employing visual methods to research nursing practice in Brazil (Gimenes, Marck, Atila, & Cassiani, 2015), Australia (Riley & Manias, 2003), and Uganda (Fournier, Mill, Kipp, & Walusimbi, 2007), as well as the use of visual methods to elicit information from specific patient populations to directly inform nursing practice, for example, with children in the United Kingdom (Carter & Ford, 2013; Coad, 2007), and in relation to adult mental health in Australia (Glaw, Kable, Hazelton, & Inder, 2017). Visual methods reported by these studies included the use of arts-based approaches such as drawings and collage to inform nursing practice through enhanced understanding of children’s experiences of care (Carter & Ford, 2013; Coad, 2007) and the use of photography as a route to nursing practice reflection and practice improvement (Gimenes et al., 2015; Riley & Manias, 2003) as well as broader organizational change (Fournier et al., 2007).
The reported strengths and advantages of using visual methods in nursing research include identifying real as opposed to idealized practices (Gimenes et al., 2015), facilitating communication (Carter & Ford, 2013), fostering openness and building trust between participants and researchers (Gimenes et al., 2015) including with communities which may be suspicious or resentful of intrusion (Castleden & Garvin, 2008), increasing participants’ power (Castleden & Garvin, 2008) and control over research situations (Coad, 2007), and the development of nurses’ “voice” (Fournier et al., 2007). Positive outcomes have been reported to arise from the use of visual research methods with nurses, including enhancement of nurses abilities to directly effect change in their practice environments (Fournier et al., 2007; Gimenes et al., 2015; Riley & Manias, 2004) and the generation of knowledge which indirectly contributes to improvement through greater awareness of the experiences of seldom-heard service users such as children (Carter & Ford, 2013).
The limitations of previous studies, as highlighted by Riley and Castleden, have led to recommendations that future studies should explain how authors have managed the implementation of visual methods in clinical settings (Riley & Manias, 2004) and called for more detailed descriptions of data analysis (Castleden & Garvin, 2008). Most published studies report on the use of a single visual method. It appears to be unusual for multiple visual methods to be employed within a single study of nursing practice, which is the strategy that we describe in this article.
The Challenge of Articulating African Nursing Knowledge
Nurses acquire power when they articulate knowledge embedded in their practice (Buresh & Gordon, 2006; Smith, 1990). Before a practice can be articulated, it must first become visible and then be acknowledged. The social and cultural norms of the communities that nurses and families come from are easily rendered “invisible” as a result of nurses’ professional status and the assertion of different organizational cultural values (Penny & Windsor, 2017).
Despite forming the largest part of the health workforce, underestimation and undervaluing of nurses’ contribution adds to the “invisibility of nurses” globally (United Kingdom All-Party Parliamentary Group on Global Health, 2016; WHO, 2016). This is certainly true in Africa, where a variety of factors including gender, class, and race mean that nurses’ voices are seldom heard (Fournier et al., 2007). The complex political legacy of South Africa, where the inequitable health system established under colonialism was further distorted by apartheid, extends an enduring influence on what has been termed nursing’s “divided sisterhood” (Marks, 1994), further contributing to a situation where many promising aspects of local children’s nursing practice lack visibility and formal expression and where few nursing practices have been intentionally designed in or customized to deliver best outcomes in African health-care settings.
Visual Methods and the Lens of Resource Scarcity
There is a documented tendency for studies of African nursing practice to focus on describing deficiencies (Fournier et al., 2007), meaning that situations and the practice of nursing are often viewed through the lens of resource scarcity. In our experience, nurses most readily describe their practices in relation to resources and adverse outcomes. This means that nurses’ narratives are often about shortages, “not being heard,” and problems rather than what they do or the nature of their practice.
In this context, descriptions of local models of care or practice are not always easy to elicit. A mind-set which focuses on the lack of resources can distort enquiries into nursing practice, contributing to the marginalization of nurses’ voices (Fournier et al., 2007). We were curious to see whether visual methods could help nurses and researchers to identify aspects of practice that are working well, including examples of what has been termed “invisible excellence” (Harvey, 2002), in keeping with principles of appreciative inquiry, as well as avoiding (often unfavourable) comparisons with higher resourced settings which are not culturally or contextually relevant.
Involvement of Families in the Care of Hospitalized Children in Africa—An Example of an Invisible Practice
Practices informed by nursing ethics, practices, and nursing knowledge may be absent from nurses’ accounts because they run counter to the idealized notions of “good” practice that form part of formal nursing education (Leininger, 1985). Haegert (2000) argues that professional nursing ethics in Africa have been developed with reference to Western moral philosophy, with an individualistic, masculine, and noncontextual emphasis on rules and duties. It is possible that the sociocultural circumstances and especially community-oriented caring traditions of both nurses and families in African cultures influence nursing practice (Söderbäck & Christensson, 2007), but that these practices lack formal expression and are at odds with what Africa’s nurses are taught to value through their professional education.
One such aspect of nursing practice is the involvement of families in caring for hospitalized children. In Eastern and African cultures, parents are widely expected to play an active part in the care of a hospitalized child (Pongjaturawit & Harrigan, 2003), with family presence and capacity regarded as a resource by many health professionals (Makworo, 2013; Nkomazana, Mash, & Phaladze, 2015; Phiri, Kafulafula, & Chorwe-Sungani, 2017; Söderbäck & Christensson, 2007). This literature suggests the existence of distinctive nursing ethics and practices related to family involvement and maternal presence in African health-care settings which differ from “best practices” developed in, for example, the UK and America (Institute for Family Centred Care, 2004; Society of Pediatric Nurses, 2003). The extent of nurses’ practices in relation to family involvement in African settings remains largely unquantified, and the nature of the underpinning philosophies and rationales is underexplored.
Using Visual Research Methods to Research Nursing Practice
We used visual research techniques as a core part of the data collection strategy to describe nursing practice in relation to involving families in the care of hospitalized children in five paediatric care settings in South Africa. We hope to publish the findings of this research in detail elsewhere.
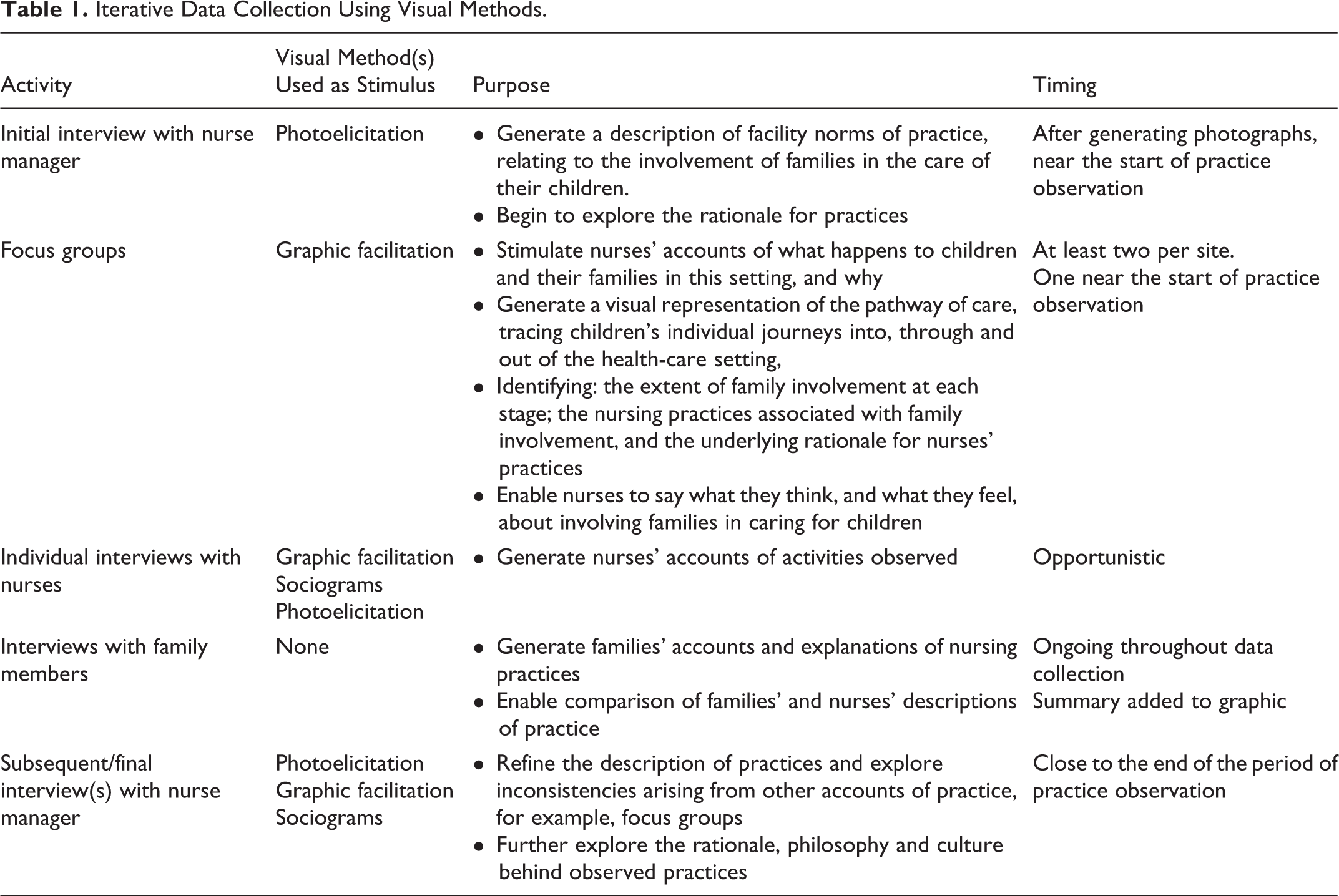
Graphic facilitation (to generate a visual depiction of family involvement in the pathway of care), sociograms, and photoelicitation were implemented concomitantly through a qualitative case study design which used visual methods to support iterative narrative data collection in conjunction with focus groups and individual interviews (see Table 1).
Iterative Data Collection Using Visual Methods.
Characteristics of Participants, Researchers, and Settings
The settings where nursing practices were observed were a nurse-led program for technology-dependent children at a tertiary paediatric hospital in Cape Town, an intensive care unit in a regional hospital in the Overberg district, a neonatal unit at a secondary health facility in Cape Town, a general paediatric ward in a tertiary hospital in Cape Town, and a paediatric ward in a district hospital in a rural area of KwaZulu-Natal. All were state-run facilities. 1 Nursing care in each of the settings was led by a nurse with a qualification in paediatrics or child health nursing, who was recruited to the study as a key informant. Across the five settings, a total of 68 nurses were recruited to participate directly or indirectly in the study, of whom the majority (64/68) were female, with most (44/68) aged between 30 and 49 years. A total of seven home languages were reported, with isiXhosa the most common (24/68), followed by Afrikaans (14) and isiZulu (12). The “working languages” of the settings where we collected data were English, Afrikaans, and isiZulu; 48 nurses were involved in 10 focus groups which included graphic facilitation; 8 nurses participated in interviews which included photoelicitation; and researchers generated 41 sociograms based on observation. The core research team comprised four postgraduate qualified nurse researchers and one psychologist. The data collection team for each setting included at least one researcher with experience of practicing in a contextually similar facility and at least one researcher with the corresponding “working language” at full professional or bilingual proficiency.
We did not set out to formally evaluate the application of visual methods as part of the study design, so the accounts provided represent our subjective personal and collective reflections and understandings. The processes used to develop these reflections on our experiences of using visual methods included:
– Group debriefings at the end of data collection for each site, with all researchers involved. These sessions focused on identifying process improvements needed or made.
– A graphic record was used to capture these practical reflections, displayed in the researchers’ shared workspace, with researchers adding to it throughout the process of data analysis and report writing. This record was referred to at the planning stage for each new site with process refinements made accordingly.
– A workshop for key participants and researchers was held to debrief on the process, with key points incorporated into a written record.
In the sections that follow a description is provided for each of the three visual methods used, drawing on key concepts connected to their development and use within nursing research. The approach taken to implement the methods in the context of the study is then detailed. Our experience of working with these methods is provided, derived from the processes described above, documenting the refinements that were made to research processes as we learned about their application. In addition, practical learning points are presented. An overview of the interviews and focus groups conducted is provided in Table 1, showing which visual methods were used as stimuli to elicit data.
Graphic Facilitation
What is graphic facilitation?
Graphic facilitation has been widely used in organizational and business development but seems to be little used in health-care research (Leonard, Bonaconsa, Ssenyonga, & Coetzee, 2017). Graphic facilitation has been used as a tool to establish shared understanding and agendas and used as an interactive way of promoting engagement in group discussions (Sibbet, 2001). A key feature of the tool is the way that information depicted graphically can be refined and consolidated in dialogue with participants, with the researcher/recorder using simple images and text (Crane, 1993; Leonard et al., 2017; Valenza & Adkins, 2009) to create a clear picture of a complex situation (Ball, 1998).
A degree of artistic skill is required to create graphic records, but considerable guidance on using icons, calligraphy, color, and other techniques is available for practitioners wishing to develop their graphic competence (see, e.g., Sibbet, 2012). The “trick” of creating a large and attractive graphic can be impressive. The cognitive work involved on the part of the researchers and participants is less obvious, but far more important (Valenza & Adkins, 2009). The real skill of graphic facilitation, as Valenza and Adkins (2009) advises, is to avoid premature “concretization” of the ideas and information represented in the graphic. Researchers need to facilitate the group effectively, applying skills and knowledge of group processes and dynamics to support the process of enquiry.
Why use graphic facilitation?
We used graphic facilitation to capture information generated through the initial focus group and interviews, generating a visual pathway of care which was then collaboratively explored by participants during subsequent focus groups and interviews. The selection of the pathway of care as the focus for the graphic provided an opportunity to explore nurses’ narrative accounts of what happens in practice, without predetermining which events and actions were relevant (Leininger, 1985). Visualising care as a pathway has been previously shown to help nurses describe what happens in their practice settings, helping to generate a “bigger picture” of what happens in day-to-day practice (Leonard et al., 2017). The ability to notice and attend to emotional states, and an awareness of long-term as well as short-term needs, are features of nursing knowledge as defined by Benner (Benner & Benner, 1999). By using the care pathway, we hoped to stimulate a holistic account of practice that included both tacit and explicit knowledge.
Implementation approach
The process of generating a graphic record was initiated at the first focus group with nurses in each setting, using the discussion guide shown in Table 2. The graphic record was displayed in each setting for the duration of the data collection process and was reviewed by participants and amended iteratively to incorporate new inputs. An example of a graphic record generated using this process can be seen in Figure 1.
Schedule for Focus Groups Relating to Graphic Facilitation of the Pathway of Care.


A graphic record depicting family involvement in relation to the pathway of care.
Our expectation, informed by our experiences of using graphic facilitation within teaching, learning, and clinical practice development, was that the graphic would help to anchor discussions by providing a shared visual point of reference, while allowing multiple perspectives to be identified and explored (Leonard et al., 2017). This expectation was met. The dialogue shown in Figure 2 shows how one particular topic (mothers who struggle to be involved in caring for their child in hospital and nurses’ responses) was unpacked over two focus groups and an interview.
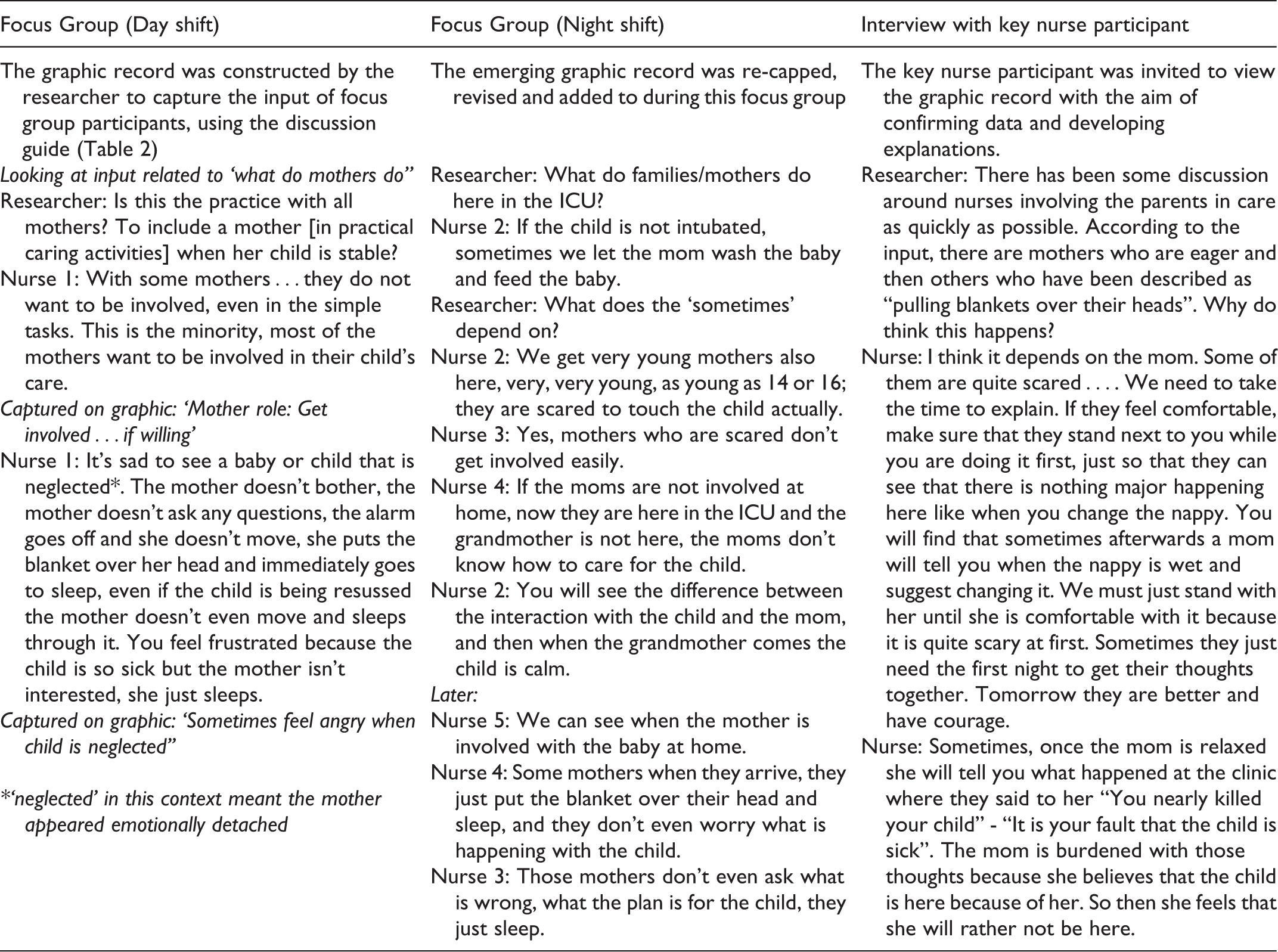
Dialogue 1: Example of sequential dialogue stimulated by a graphic record.
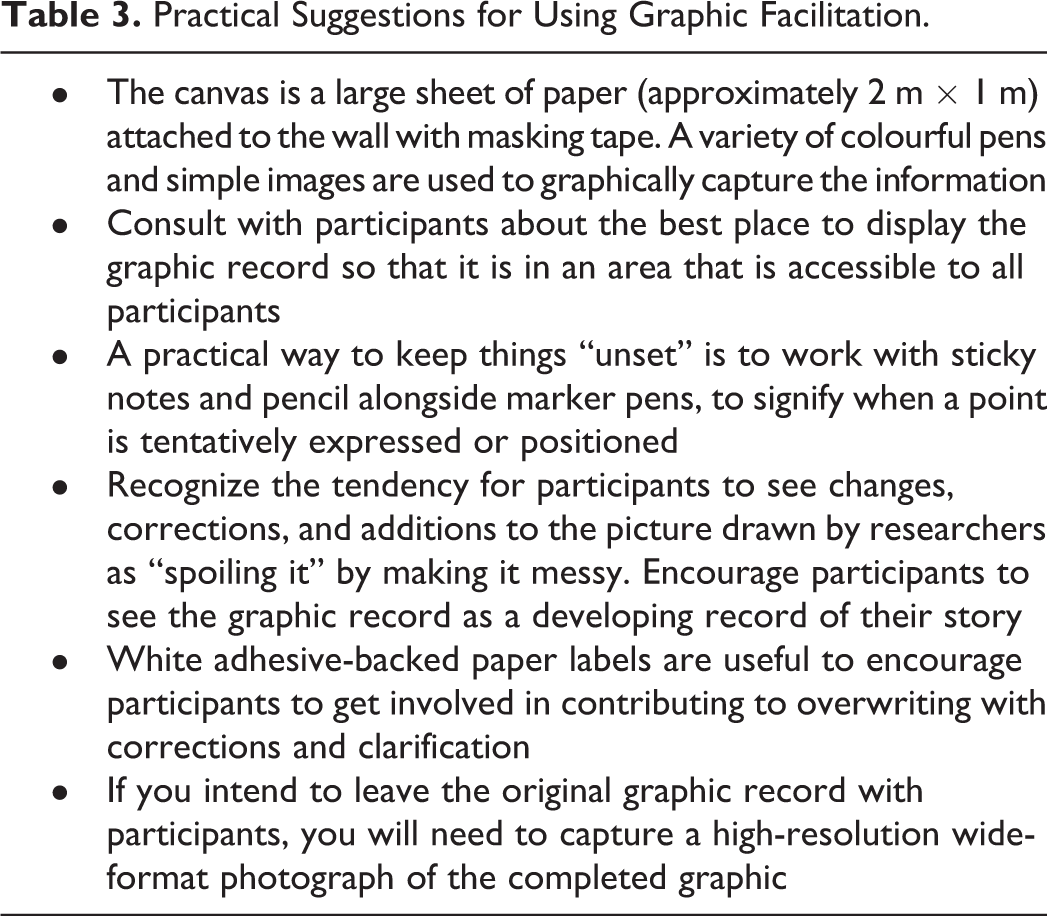
Suggestions for implementing graphic facilitation based on our experiences are offered in Table 3. Our experience of graphic facilitation aligns with the experiences reported from previous studies, with participants appearing to find the process of cocreating the graphic to be energizing and engaging (Ball, 1998; Leonard et al., 2017). The focus groups were often lively and good humoured. Nurses were often happy to sustain extended dialogues between themselves with little prompting needed.
Practical Suggestions for Using Graphic Facilitation.
The graphic record was used as a stimulus to dialogue outside the initial focus groups in which they were developed, often supporting a sequential process starting with an initial description of practice, then adding detail and identifying exceptions, before exploring underlying assumptions and beliefs (see Figure 2). Researchers were able to stand by the graphic record with participants both during and after focus groups and ask nurses to expand on or clarify particular points. We were careful to ask not only “what” but also “why” and “how.”
The graphic record was displayed on a wall for the duration of data collection, in a place identified by nurses as suitable. This was usually the staff room or a teaching room. An unanticipated consequence of this was that the graphic record was not visible to families, since it was displayed in nurses’ private space. In this study context, this was a limitation on the use of visual methods with families, and interviewing formed the only method of data collection employed with families.
Reflections and practical learning
The type of data generated through using the graphic record as a stimulus exhibited the holistic accounts of nursing knowledge and nursing practice described by Benner, Tanner, and Chesla (1996). As Figure 2 exemplifies, the depictions and narratives that emerged often demonstrated nurses’ holistic awareness of the journey made by the child and the family and how nursing knowledge included culturally influenced factors such as extended family dynamics and intergenerational patterns of caring. In this setting, “standing with mothers” emerged as a core description of the philosophy of care, denoting intentional practices to communicate parity and solidarity between nurses and mothers in the face of challenging circumstances.
The graphic record prompted comments from many nurses, who expressed satisfaction and excitement that their words and the information they had shared with the researchers through focus groups and interviews were now on prominent display. On many occasions, nurses were seen to bring colleagues to view the graphic record and seemed proud to have their practice represented in this way, with a typical response being: “Look—that’s what we said!” It helped to create a sense that the researchers were “hearing.” Participants in all settings asked for and received the original graphic to keep, indicating a positive response to being heard which suggests that research objectives in this regard were met using visual methods.
Sociograms
What are sociograms?
A sociogram is a diagrammatic tool which maps structure and patterns of interpersonal lines of communication (Hollander, 1978) to produce what Moreno, in early work on the technique, termed “sociometric fact” (as cited in Freeman, 2000). Sociograms are therefore a way of measuring the intangible aspects of group interactions, including what have been termed “insubstantial phenomena” such as ideas, opinions, and feelings (Leedy & Ormrod, 2010), as well as aspects of nursing communication norms connected to power, inclusion, and exclusion.
Decisions about technique, aesthetics, and readability should be approached mindfully when devising sociograms, as they can influence interpretation (Hogan, Carrasco, & Wellman, 2007). Freeman (2000) provides a comprehensive description of the different types of visualization that can be employed to create sociograms. We elected to record and depict observations using a form of sociogram called a directed graph. Individuals were depicted by points, and communication among the individuals was represented by lines. The direction of communication was indicated by arrowheads, and color coding denoted the nature of the communication according to coding devised in advance by the researchers, making it possible to capture who is talking to who, about what. An example of a sociogram is shown in Figure 3.

Sociogram depicting a patient care interaction.
Why use sociograms?
Clarity about the purpose of enquiry is key, since sociograms can be organized to capture many different dimensions of information within a network (Huang, Eades, & Hong, 2005). While sociograms are often used to record and analyze social networks in the abstract, our intention was to record and analyze interactions in real time. We set out to observe a variety of ward events including bedside nursing and multidisciplinary team handovers, clinical procedures, treatments and therapy sessions, and interactions between children, families, and health-care professionals and ancillary staff. We therefore elected to show the placement of individuals according to their physical position in relation to the child.
Implementation approach
We recorded the sociograms by hand, using pen and paper. Although it has become increasingly common to use digital technologies in sociometrics (Freeman, 2000), there are advantages to using pen and paper in fieldwork situations (Hogan et al., 2007). The immediacy of capturing an event through hand drawing creates an image that participants can be involved in interpreting straight away. As well as supporting participation, this minimizes problems of inaccurate or insufficiently detailed recall and assists with reliability of interpretation (Huang et al., 2005).
It is possible to subject the data embodied in sociograms to sophisticated quantitative analysis (Freeman, 2000). We initially considered quantitative analysis of the sociograms to be a necessary rigour. However, the reduction of a visual web of interactions to a numerical tally was not particularly instructive. This is a known limitation of hand drawn sociograms (Huang et al., 2005). The use of sociograms was however of value in making the patterns of interaction between health professionals and families visible in a way that was tangible to participants and researchers and in providing a stimulus for conversations about communication and practice. The dialogue below, stimulated by the sociogram shown in Figure 4, which depicts a dense cluster of communication initiated by an advanced nurse practitioner during a multidisciplinary case conference meeting, illustrates this. This is one of a series of sociograms that were captured in a multidisciplinary ward round and case review meeting, involving only health-care professionals and held in a meeting room adjacent to the ward. A simplified form of directed graph was adopted, using arrows on lines to indicate multiple occurrences, because of the very dense and rapid nature of the communication during this event.

Sociogram related to Dialogue 2.
Dialogue 2
[pulls face and looks uncomfortable, turns away] That’s dreadful! Is that me? [correctly identifies node on sociogram]
Yes—why don’t you like that?
Look at it—I’m doing all the talking!
Are you? Let’s look at what these arrows mean. These ones are where you are asking questions, like to [the speech and language therapist]…and [to the medical officer]. And then these lines are them answering you—it’s them talking. And here you are giving information, like when you said that Mum was learning really quickly.
I suppose it is really. I mean, making sure the family is considered, making sure that people [allied professions] speak up, that there is a complete picture of the child and the situation at home, that is important to me.
To me, that’s what this diagram shows. All these “lines” coming and going around you—isn’t that care co-ordination?
I suppose so [looks at sociogram]. I think I still look very talkative [laughs]. But it’s teamwork really, at the end of the day it’s what it takes to get the child home.
You still don’t look happy! Let me ask you, what do you think this picture would look like if you weren’t there?
Oh.…The team are very good. Very caring. But I do think…if I couldn’t be there…Well, I think everyone needs to be heard, especially the young ones. And I try to bring in [nurse], she needs to contribute, because she is on the ward, and has that relationship with the mothers, the little ones, you know. I do think this [diagram] is interesting actually. I wouldn’t have said it looked like this. I still don’t like it but I am getting used to it.
During this conversation, the sociogram functioned as a visual anchor, objectively depicting the observed patterns of communication, while the nurse and the researcher were able to persevere together through this nurse’s initial discomfort with acknowledging her status as a clinical leader, working toward the expression of the nurse’s values and beliefs about child- and family-centered care.
Reflections and practical learning
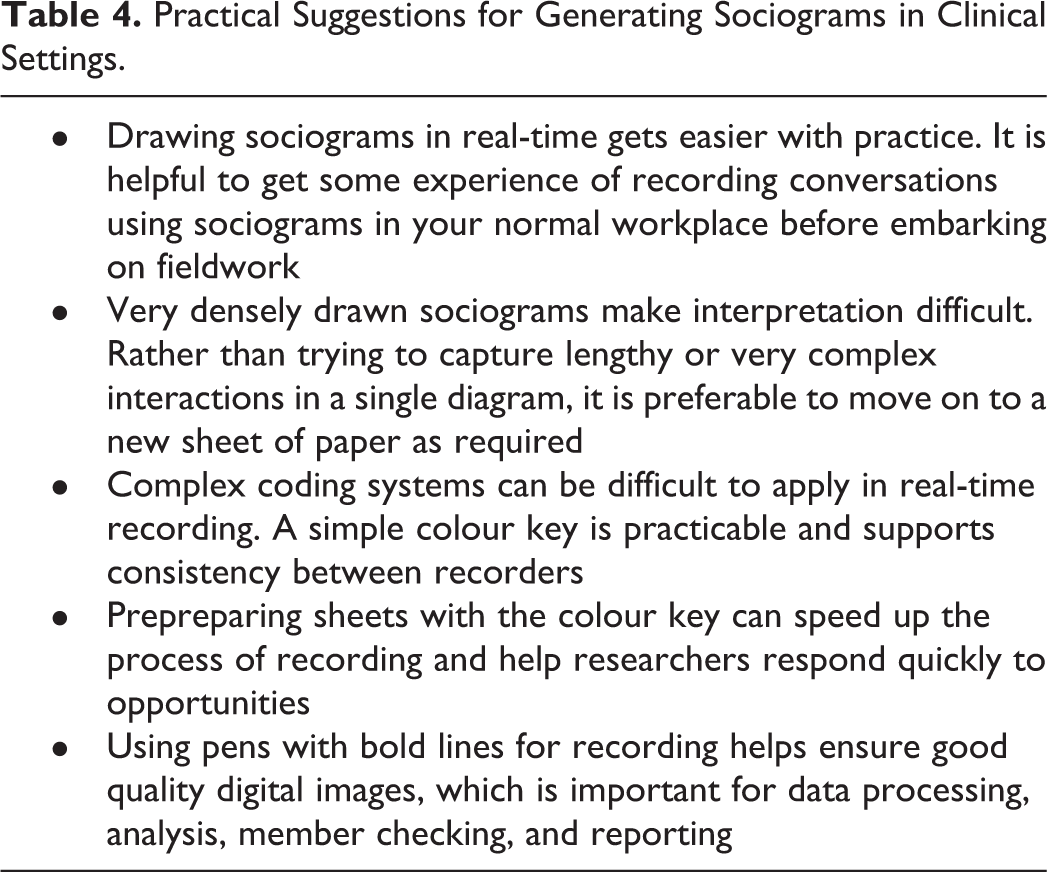
The practical implementation of sociograms was initially challenging. The first sociograms produced by the researchers were densely drawn, which made interpretation and analysis difficult. Accurate charting of sociograms requires the researcher to pay attention to the patterns and intentions of interaction without getting drawn in to content or meaning in the moment of recording. Suggestions based on the practical refinements made are summarized in Table 4. Of all the visual methods employed in this study, the sight of the researchers drawing sociograms stimulated the most curiosity in participants who often expressed interest in the technique and initiated dialogue about the patterns of communication depicted.
Practical Suggestions for Generating Sociograms in Clinical Settings.
Photographic Elicitation
Photographic elicitation uses photography as a stimulus to interviewing (Banks & Zeitlyn, 2015; Emmison, Smith, & Mayall, 2012). Photographs serve as visual anchors and catalysts for dialogue between participants, whether singly or in groups, and researchers. Narrative accounts and responses to the images are elicited from participants (Riley & Manias, 2004).
Implementation approach
We used photoelicitation to generate a visual depiction of nursing practice, by pairing images with descriptions provided by nurse-participants and family members using the space and facilities, as suggested by Hurworth (Hurworth, Clark, Martin, & Thomsen, 2005). Photoelicitation often, but not always, places the camera—and therefore the selection of images—in the hands of participants (Liebenberg, 2018). Initially, it had been envisaged that the nurses would undertake the photography unaccompanied. In the first two settings, the nurses were hesitant about their ability to use the digital camera and asked instead that the researcher undertake the actual photography. The researcher therefore operated the camera as the participant led a tour of the setting and directed the images to be captured. Working to a preestablished guide (see Table 5), the participant directed the researcher to take images of facilities, equipment, fixtures, and events that were deemed to be connected to the practice of involving families in the care of their hospitalized child. We subsequently concluded that the decision to use a complicated and expensive camera limited the use of the method because it deterred participants from taking control (see Table 6), although the images generated in collaboration between researchers and nurses were still successful as a stimulus to narrative data collection. Other practical learning points generated through the experience of conducting photoelicitation are offered in Table 6.
Image Guide for Photoelicitation.

Practical Suggestions for Using Photoelicitation in Clinical Settings.

Reflections
Previous accounts have described using photoelicitation to identify and describe practices. We found some indications of a further strength. Photoelicitation appeared to support critical practice reflection and the articulation of not just actions but more abstract concepts including reasoning and deeply held values. Dialogues arising from the image of the chair (Figure 5) illustrate this.

An example of an image generated through photoelicitation (a chair in which mothers’ sleep and rest).
Dialogue 3
So the mums are always around? One of the challenges that was identified in the focus groups was that mothers can be watching what nurses are doing. Do you get some nurses who struggle to cope with that?
You do get some. They need to know that you must let the mother be the nurse.
Dialogue 4
In response to the image of the chair, this nurse spoke about her personal philosophy of care in a way that made explicit her belief in mothers’ capacity to care for children:
You should learn to trust people. If you don’t trust them, how should they trust you to look after their children? I also think it’s not just what you do, it’s the way you do things. It’s just a relationship that you build up with the person, the trust between the two. Because if you don’t trust them, you will always not [never] be sure that they are doing the right thing.
Employing Multiple Visual Methods in Combination
The three types of visual method were implemented in combination, as part of an integrated approach to data collection. There was considerable overlap between the application of the methods in practice. The process of exploring embedded meaning from photographs and sociograms continued throughout the period of practice observation and contributed directly to the quality of data elicited through graphic facilitation during focus groups and interviews. Our examination of the literature suggests that our approach was somewhat unusual in employing multiple visual methods within a single study, and we consider that the three methods worked well as a complementary approach.
The strategy of using visual methods to stimulate nurses’ engagement in individual and focus group interviews was particularly valuable in relation to supporting sustained and iterative participant engagement leading to the generation of accurate, detailed and conceptually rich accounts of practice, as illustrated above (see Dialogue 2). We found most of the immediate practical challenges of implementing visual methods to be surmountable with practice.
As the various examples above illustrate, we discerned two main benefits of using visual methods. Firstly, visual methods appeared to be useful as a tool to inspire sustained collaboration. Secondly, visual methods appeared to support the construction of accurate and holistic descriptions of nursing practice.
Visual Methods as a Tool to Inspire Sustained Collaboration
The work described in this article included more than 84 hours of engaged dialogue with nurses, often in the realm of tacit and personal knowledge and experience. Given that nurses are often viewed as having high levels of distrust, suspicion, or indifference toward researchers (Benner, Tanner, & Chesla, 1996; Leininger, 1985), and in view of the specific factors contributing to the marginalization of nurses’ voices in South Africa (Marks, 1994), this is encouraging.
The use of three types of visual methods in combination seemed to confer trust and a degree of insider status on the researchers. It was noted that even if a nurse participant had not been directly involved in an activity, such as capturing photographs, the nurse participant would allude to the fact that the researcher had “seen” an element of practice. We perceived this as helpful in moderating dynamics associated with power, race, language, and class, consistent with known strengths of visual research techniques (Gaventa & Cornwall, 2008; Lorenz & Kolb, 2009).
At a very practical level, visual methods were helpful in mitigating the interruptions that are a familiar real-world feature of interviewing nurses in the clinical environment. Being able to refer to a photograph or a specific point on the graphic record was helpful in maintaining or reestablishing focus and answering the question “Sorry, where were we?” within a conversation, as well anchoring dialogues successively over a longer period.
The second practical benefit of visual methods that we discerned was the dimension they added to spoken communication. This is especially relevant in the multilingual nations of Africa, including South Africa which is a country with eleven official languages. It is also a benefit which may be relevant elsewhere given the increasingly international nature of the nursing workforce in many countries of the world. While almost all nurses were used to conducting workplace communication in English, we noted that nurses drew on visual data to achieve greater clarity in communication during dialogue with researchers in English. This applied particularly to nurses’ apparent willingness to persevere in articulating explanations of practice and abstract thinking. Dialogue 5 was anchored by the element of a graphic record shown in Figure 6, which was repeatedly gestured to by the nurses speaking.

Graphic record.
Dialogue 5
If a mother arrives with a child who is, let’s say eight years old, what happens with him?
She stays. Usually she stays. If she is willing to stay.
It seems like most choose to stay, so why do they choose to stay?
[widespread laughter—seems like this was a question to which the answer should be obvious]
Because they love their child! And the babies also understand more of their mothers than with other people. Even with the medication, the babies will take it more easily with the mothers than with us.
The dialogue that unfolded expressed an important practice rationale for the continuous presence of mothers in this paediatric ward, which extended to cosleeping. Nurses saw the mothers as mediating the frightening hospital environment for their child, by providing an interface between the child and the nurse. Nurses regarded this as beneficial for children, since it lessened distress and improved acceptance of treatment, as well as making nurses’ work more manageable.
In this way, as described by Harper (2002), the images served as something around which nurses and researchers could gather together, committed to a process of “figuring something out together” (Harper, 2002, p. 23). We speculate that because as researchers we had “seen” an aspect of practice through a variety of visual media, nurses perceived that our interest was genuine and were therefore patient in finding the words to explain nuanced concepts. We do not advocate the use of visual methods as an alternative to first language interviewing where this is possible, but our experience suggests it may be a useful adjunct to verbal communication between individuals who share a language but have different linguistic proficiencies.
Constructing Holistic Descriptions of “Real” Nursing Practice
Visual methods offer a way of documenting what really happens in nursing practice, which is an essential first step toward accurate interpretation. Because visual methods offer participants a fresh perspective on “daily and familiar” activities and objects they can contribute to the development of accurate descriptions and interpretations of practice (Harper, 2002; Leininger, 1985). Graphic facilitation and photoelicitation were helpful in sustaining focused enquiry into observed patterns and routines and the use of space and equipment to generate more detailed and accurate accounts of previously “invisible” practice. As one senior nurse participant said at the end of the process, after reviewing the report: “The descriptions were very accurate about what happens [here]. It was nice to have it in words. The philosophy is getting children home, back with their families.”
Achieving accuracy of description and interpretation is often difficult because of the tendency of professionals to offer “nearly perfect” (Leininger, 1985) and “overly tidy” (Hogan et al., 2007) accounts of practice which emphasize the elements of practice which nurses have been taught to value. Visual methods further supported a way of seeing and of knowing that sits within a holistic approach to enquiry, taking account of the many factors that make up “practice” and helping nurses to point, for example, to tacit relational practices, involvement skills, and the contributions of family members as an integral part of “what happens here,” supporting accuracy. This is important in enabling promising local practices to be identified, since practices such as cosleeping for mothers and children, or the delegation of the majority of physical care to mothers, may run counter to the “good” practice that is taught in Africa’s nursing schools.
Having enabled the identification of practices that had been invisible either because of familiarity or marginalization, visual methods continued to support the exploration of nursing practice, practice narratives and explanations. The data generated went far beyond practically oriented descriptive accounts of “what happens.” With visual data as a trigger, as Dialogue 6 demonstrates, senior nurses were able to clearly articulate the rationales underlying observed nursing practices in relation to working with families in the care of their hospitalized child (an observation also exemplified in Dialogue 1).
Dialogue 6
Focus group with graphic record capturing “What nurses think and feel about including mothers in care?”
Mothers being present make it easy to reach a child for any procedures.
So that the child will have love from mum, and comply with medicines.
It helps the nurses to render quality nursing care as some work is done by the mothers and that saves time.
Interview with senior nurse, using graphic record and photographs as a stimulus,
We promote a healthy whole for the child. If the child is alone they cry, they do not eat, and so we allow the mothers to stay together with their child. It is easy to heal faster with a mother.
It appeared that these philosophies and values were well embedded since, as Dialogue 6 shows, more junior staff also expressed these values in ways that were simplified but usually consistent with the statements made by senior colleagues. In our experience with nurses in local settings, such rich data are unlikely to be generated by conventional observation or interviewing alone.
Methodological and Implementation Challenges
As stated earlier, the limitations of previous studies have led to recommendations that future studies should provide descriptions of how challenges regarding trustworthiness, ethics, and the treatment of visual material within data analysis were addressed. The remainder of this article provides a brief account of the way that we addressed these issues.
Trustworthiness of Visual Methods
Carter and Ford (2013) remind researchers of the need to consider the potential for visual methods to shape the data collected, since visual methods inherently involve coconstruction of data. This coconstruction is triadic in nature between the participant, researcher, and the “trigger” provided by the visual method (Carter & Ford, 2013). The nature of the trigger can shape the data collected and researchers are advised to be mindful of this. Our approach to minimizing this risk was to exercise a deliberate awareness of the contributions of participants, researchers, and “triggers.” Nurses contributed in-depth understanding of practices, and tacit understanding of the rationale and values that underpin them. Nurses provided descriptions of practice in their setting, derived from their direct experience and to some extent their training. It would not be reasonable to expect nurses to articulate an explanatory account of a practice which has not previously been described as an entity. The contribution of researchers in this process was to provide external perspective based on knowledge of other contexts and theoretical understandings, using this to probe for detail or explore the “fit” of possible explanations with nurses. Visual methods were helpful in establishing a wider frame of reference which supported the development of descriptions and explanations of practice as part of a “bigger picture.”
Photoelicitation and sociograms, as implemented in our study, appeared to involve a relatively low risk of data shaping as both capture what participants identify or do. Graphic facilitation involves greater potential to shape data, as it requires the researcher to transform spoken information into images. This risk was partially ameliorated by constructing the graphic record over multiple sessions, informed by interviews and focus groups. We also aimed to be transparent when revising the graphic, acknowledging when things had not been recorded correctly, and encouraging nurses to help us make the record better.
While acknowledging the potential for visual methods to shape the data collected, in our experience, we consider that the iterative possibilities of visual methods contributed substantially to trustworthiness. It is possible to subject the same image/depiction of practice to multiple perspectives several times over, identifying and exploring inconsistencies, before arriving at an explanation which derives from and is authentic to observed practices.
Ethical Implementation of Visual Methods
It has been acknowledged that established institutional frameworks for overseeing the ethical conduct of biomedical research are unlikely to provide a comprehensive basis for assessing the appropriateness of visual methods (Banks & Zeitlyn, 2015; Riley & Manias, 2004), particularly in relation to their impact on participants. Specific considerations apply in relation to negotiating access and gaining consent for photoelicitation (Castleden & Garvin, 2008; Coad, 2007). There are also ethical considerations which stem from the participatory nature of visual methods.
We consider that the greatest strengths of visual methods also present the greatest challenges to their ethical application. Visual methods are a powerful tool with which to establish trust and openness and can lead to the articulation of tacit knowledge, resulting in invisible nursing practices becoming visible. During data collection, we discerned a concern among many nurses that observation would expose deficiencies in practice or result in unfavourable comparisons with other settings. We also noted that nurses described aspects of practice that were acknowledged to be counter to institutional policies. Examples included locally amended visiting policies which allowed the continuous presence of mothers and extended presence for fathers and other family members, and the provision of amenities to mothers which the facility did not normally accord to “nonpatients.” These aspects of practice represented local practice innovations intended to facilitate the involvement of families in caring for their hospitalized child and appeared to be beneficial and consistent with informed rationales. Some practices were however unofficial, not having been formally negotiated or approved by facility management.
There is an ethical dimension to the identification of these practices. Southern Africa’s health systems are a challenging environment for nurses. A variety of factors, including resource constraints, contribute to a documented organizational culture in some hospitals which is quick to attribute individual blame, leaving nurses fearing punishment if they are found to be in contravention of official policies (Ally, Nel, & Jacobs, 2016).
It is therefore important to anticipate the implications of examining informal and tacit practices through the powerful lens of visual methods prior to implementation (see Table 7). We found two aspects of the study design supported ethical conduct in this regard. Firstly, our study took an appreciative inquiry stance. Having purposively selected settings that had been suggested to us as embodying promising practices in the involvement of families, we were able to structure data collection and presentation of findings to focus on “what works well and why” (Whitney & Cooperrider, 2011). This lens brought an element of safety to data collection and the presentation of findings, and we were transparent that the intended product of the research was an articulation of promising practices. In this way, we were able to enlist the authority of our status as researchers in order to amplify the voices of the nurses who were describing the innovative practices they had developed.
Practical Suggestions for Ethical Conduct of Visual Methods to Describe Invisible Nursing Practice.

Analysing Visual Data
The lack of clarity regarding the status of visual data and confusion about how to analyze it and present it have been repeatedly highlighted (Carter & Ford, 2013; Riley & Manias, 2004). Riley and Manias (2004) urge researchers to be explicit about the describing their approach to analyzing visual data to demonstrate scholarly rigour and increase acceptance of visual methods by the nursing research community. Prosser and Schwartz (1998) advocate that visual methods should be employed in ways that are consistent with the methodological strategy of the whole study. There remains, however, little guidance or description of detailed processes relating to qualitative content analysis of data collected through visual methods.
We concur with the view expressed by Riley and Manias (2004) that some of the confusion regarding the treatment of visual sources in data analysis derives from the transfer of methods initially developed in other fields (notably Participatory Action Research), to more pragmatically oriented studies of nursing practice.
We elected to use graphic facilitation, sociograms, and photoelicitation as stimuli for the generation of narrative data through consultative activity in the form of interviewing and focus groups. We therefore adopted conventional strategies for analysis of the transcribed material that arose from interviewing and focus groups stimulated by visual methods, subjecting the transcribed material to thematic analysis and, subsequently, cross-case study analysis.
Conclusion
Our initial goal was to generate a descriptive account of a specific aspect of nursing practice in Africa. Within our own research context, our experiences lead us to conclude that visual methods appear to offer numerous benefits in enabling identification and exploration of implicit nursing practices, resulting in nurses’ voices being heard, and invisible nursing practices becoming visible. “Standing with mothers,” “promoting a healthy whole” (by minimizing separation of the mother and child), and “letting the mother be the nurse” represent distinctive values and culturally specific caring practices which were successfully articulated through the use of visual methods. In the context of the study we describe, the data elicited provide a rich basis for further work to conceptualize an Afrocentric model of nursing practice in relation to involving families in the care of hospitalized children.
Footnotes
Acknowledgments
We gratefully acknowledge the nurse participants who invited us into their workspaces and shared so wholeheartedly in this work. Thobeka Duma made a valuable contribution to data collection and analysis in KwaZulu-Natal.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The activities and data described in this article formed part of a study that was approved by the Human Research Ethics Committee of the University of Cape Town (HREC REF: 411/2017). Individual consent was provided by all respondents and participants.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Child Nurse Practice Development Initiative receives funding from ELMA Philanthropies, Vitol, the Harry Crossley Foundation, and the Children’s Hospital Trust.