
Abstract
Early diagnosis of cancer through screening can reduce deaths and treatment burden if the people invited participate. Yet inequalities in screening participation remain: ethnic minority groups in particular experience barriers to cancer screening that need to be addressed in order to contribute to improving equality in health outcomes. Community-centred, participatory approaches can ensure that cancer screening interventions are culturally appropriate to the communities they are intended to serve. Virtual participatory research faces unique challenges in building the rapport required for successful collaboration between participants and researchers. This article describes the successful adaption of face-to-face participatory methods to co-designing, online, an intervention using faith-based messages to reduce cancer screening barriers. Based on the World Café method, we conducted four two-hour workshops by video call with a group of 10 Muslim women (29–65 years) from Glasgow, UK. Activities included (i) plenary and small-group discussions, (ii) graphic recording, and (iii) expert presentations. The workshops covered four topics: Islam and health, screening barriers, faith-based messages for screening barriers, and delivering a faith-based intervention. Anonymous feedback questionnaires evaluating each workshop showed the women found the workshops interesting, informative, and helpful. They reported being glad they had participated. Our findings highlight the importance of interactive discussion and low participant burden to optimise online co-design. The workshops created a faith-based cancer screening intervention engaging and accessible to Muslim women.
Keywords
Introduction
Participatory approaches are key strategies in addressing health inequalities (South et al., 2019) and the Medical Research Council’s guidance on complex interventions indicates the importance of designing, developing, and delivering interventions in partnership with target populations (Craig et al., 2008). Participatory approaches have been used successfully to co-design interventions to improve breast cancer screening uptake (Padela et al., 2015, 2016, 2018, 2019).
Although cancer screening participation in Scotland has achieved its target rates for cervical, breast, and colorectal screening (Public Health, 2020, 2021b, 2021a), inequalities persist with lower participation rates among ethnic minorities, particularly Muslim women (Campbell et al., 2020; Priestly, 2021). Many barriers and facilitators to cancer screening exist, suggesting a complex interplay between factors at multiple levels, including individual, socio-cultural, institutional, and structural factors (Kazi et al., 2021; Robb, 2021; Siddiq et al., 2020). Individual factors include language and health literacy, lack of in-depth knowledge of cancer screening, fear, beliefs about screening, and the idea that screening is not required without symptoms (Kazi et al., 2021; Lofters et al., 2018; Racine & Isik Andsoy, 2022; Shirazi et al., 2013; Vahabi & Lofters, 2016). Socio-cultural factors include delaying screening because of stigma (Islam et al., 2017; Khan & Woolhead, 2015; Szarewski et al., 2009), disgust of colorectal screening (Palmer et al., 2015; Robb, 2021), gender norms, such as putting the health of the family before the woman’s health (Islam et al., 2017), and embarrassment and modesty (Moey et al., 2022). A perceived lack of female clinicians has been found to be a barrier to seeking healthcare for Muslim women, highlighting not only the need for gender concordant healthcare, but also for healthcare providers to make navigating such a request as easy as possible (Azhar et al., 2022; Vu et al., 2016). Religious beliefs in relation to healthcare and cancer screening are complex but some studies indicated that higher levels of religiosity have been associated with delays in seeking healthcare (Azhar et al., 2022; Vu et al., 2016). Negative religious coping, viewing health problems as a punishment from God (Padela et al., 2015), and fatalistic beliefs have been reported in the literature (Moey et al., 2022). Structural factors include cost (Islam et al., 2017) and perceived discrimination (Azhar et al., 2022).
The multifactorial nature of these barriers and facilitators indicate that interventions aimed at increasing uptake should be multidimensional. However, interventions aimed at improving uptake on a population level seem to work less well than targeted interventions (Marlow et al., 2017). Healthcare providers and planners must capitalise on facilitating factors and minimise deterring factors to optimise uptake of screening. Cultural tailoring can address screening barriers by integrating factors like culture or religion into health promotion and can contribute to tackling cancer inequalities (Escribá-Agüir et al., 2016; Padela et al., 2018; Pratt et al., 2017). Faith-based messaging has been used in breast screening interventions for Muslim women, for example by highlighting that Islam encourages women to take responsibility for looking after their bodies (Padela et al., 2016, 2018). Community-centred and participatory approaches have been shown to improve effectiveness of health interventions (O’Mara-Eves et al., 2013). Community-centred and participatory approaches include collaborations and partnerships, where professionals work in partnership with communities at any stage of the project, including the planning, designing, and delivery of interventions (South et al., 2019). Community-centred approaches involve the activation of assets within communities to foster equity and social connectedness (Public Health England, 2020). Co-production based on equal and reciprocal relationships between the community and professionals and peer-based interventions, in which the community and peers are actively involved in the delivery of interventions, are key elements of community-centred and participatory approaches in health research (South et al., 2019). Evidence has shown that the more the participatory approach is led by the community, and the more within their control, the more effective the approach (O’Mara-Eves et al., 2013).
Participatory research has, however, faced new challenges due to the protective measures introduced during the COVID-19 pandemic, including physical distancing (Hall et al., 2021), which has necessitated the use of online research methods. Beyond pandemics, online participatory research has importance as it can increase access for groups who would otherwise struggle to participate in traditional face-to-face research, such as those with caring responsibilities who may have no time to travel to participate in research, for people with health conditions who are unable to meet the physical demands of attending traditional research programmes, or for those less comfortable in social situations (Wilding et al., 2020). While some research has been published on online qualitative data collection (Synnot et al., 2014), guidance for remote participatory research is only just emerging (Hall et al., 2021). Our experience of conducting online co-design workshops can address this gap and offers useful insights to other researchers. Our virtual online co-design approach allowed us to develop a faith-based intervention to encourage cancer screening uptake among Muslim women (Christie-de Jong et al., 2022), based on the work by Padela and colleagues (Padela et al., 2018, 2019; Vu et al., 2018). The intervention was highly acceptable according to post-intervention qualitative assessment of participant experience (Sekhon et al., 2017).
This article has two aims: i) To describe how we adapted the World Café approach (Aldred, 2009; Carson, 2011) to facilitate a series of virtual co-design workshops ii) To describe the development of a faith-based intervention to improve cancer screening uptake among Muslim women in Scotland
Method
Sampling Approach and Recruitment
Muslim women residing in Scotland, aged 25–74 years, were eligible to be part of the co-design group. This age range covered all three cancer screening programmes: breast, colorectal and cervical. To obtain wide-ranging perspectives, we sought to reflect ethnic diversity in our co-design group and use purposive sampling to invite potential co-design group members based on age and ethnicity. Although Muslim women of all ethnicities share some social and cultural contexts and attend the same mosques and community organisations, they form an ethnically diverse group; ethnicity, culture, and religion are entangled and are likely to influence attitudes in complex ways, particularly in relation to health behaviour (Chen & Kerr, 2018).
We liaised with local stakeholder and community groups to recruit co-design group members (N = 10) between November 2020 and January 2021. RA and FC contacted eight well-known mosques, religious centres, and community groups in Glasgow to inform them about the study and encourage potential co-design group members to contact RA. We aimed to recruit both in Sunni and Shia communities. Due to physical distancing restrictions during the COVID-19 pandemic, some Imams and community leaders had difficulties getting in touch with potential participants. One Sunni mosque and one Shia religious centre were able to support recruitment by distributing the study invitation letter and participant information sheet among their members. RA set up WhatsApp groups and used phone calls to identify suitable meeting times and establish rapport with potential co-design group members. This approach was particularly valuable as we were unable to recruit in person. We used snowball sampling to further support recruitment, which can be an effective method when working with ethnic minorities (Farooqi et al., 2018).
Participatory Research Design
This study used a community-centred co-design approach with four workshops based on the World Café method (Carson, 2011) to develop the intervention—faith-based messages and their delivery—in collaboration with the intervention target group. The purpose of the World Café method is to provide a comfortable informal setting, which facilitates the inclusion and exchange of diverse views on a topic (Carson, 2011). One benefit of the World Café method is that it enables researchers to engage deeply with the communities they serve and thus generate richer insights (Estacio & Karic, 2016). This method has been used successfully with marginalised groups (Page & Temple-Malt, 2018). Including diverse views in our co-design workshops ensured our faith-based messages would be relevant to Muslim women with diverse ethnic backgrounds and delivered accessibly and engagingly.
Another benefit of the World Café is its focus on asking questions that enable researchers to learn from what is already working well. While this approach elicits responses that are positive and constructive, a disadvantage may be that the emphasis on collaboration among World Café participants can overstate group consensus and overlook structural challenges to social issues (Aldred, 2009). To ameliorate these concerns, every workshop ended with a member-checking exercise to ensure the research team understood the co-design group’s discussion accurately. Where appropriate, we followed up with the co-design group on the research team’s conclusions from interim workshop findings in subsequent workshops.
Workshop activities were designed iteratively to account for discussion in previous workshops. Each workshop focused on a distinct topic: 1. How does Islam advise about health screening? 2. Barriers to cancer screening and faith-based messages 3. Bringing faith-based screening advice to Muslim women 4. Training the messengers/intervention development
Adapting the Participatory Workshop Approach to a Virtual Setting
The World Café method is based on seven design principles, which guided our adaptation of this method for use with online video calls: (i) context setting; (ii) creating hospitable space; (iii) exploring significant questions; (iv) encouraging everyone’s contribution; (v) connecting diverse perspectives; (vi) listening for patterns; (vii) making and sharing collective discoveries (Brown & Isaacs, 2005).
We chose the video conference software, Zoom, as it could facilitate all workshop activities. We held four two-hour online workshops, in February and March 2021, facilitated by MK with the help of RA, FC, and, of a pool of six volunteers, five took notes and provided technical support online or by phone.
As part of the World Café method (Brown & Isaacs, 2005) all sessions were graphic-recorded by LG who created visual summaries of each workshop discussion (Figures 1–4). Throughout each workshop, LG drew and wrote on a digital poster using a graphic tablet, capturing the essence of ideas and views expressed by attendees. When there were smaller breakout groups, a volunteer note taker was present in each of these and would send notes to the graphic recorder via the chat function. Additionally, after the small group discussions, a spokesperson from each group would summarise what was discussed, providing another opportunity for LG to hear the discussion points. Between each workshop, LG would finalise the poster of the previous workshop (tidying up images and incorporating any unattended notes) and the final poster was presented to the attendees at the start of the following workshop. This process was used to (i) demonstrate to co-design group members that their voices were being heard, and (ii) enable the co-design group to identify patterns in reflective discussion of the graphics at the end of each workshop (Kelly, 2005). Graphic representation of Workshop 1. Graphic representation of Workshop 2. Graphic representation of Workshop 3. Graphic representation of Workshop 4.



While co-design group members already had some rapport with RA and FC, MK was unknown to them until the first workshop. MK, LG, FC, and three of the volunteers are white European women. RA and three of the volunteers were Muslim women.
Prior to each workshop RA shared the workshop timetable (Appendix 1) with the co-design group via WhatsApp. Once the co-design group joined the Zoom call, they were admitted to the meeting and encouraged to check their microphones and cameras were working. To further create a relaxed atmosphere, we encouraged co-design group members to make themselves comfortable in their physical location as we would have done, for example by providing refreshments, in a face-to-face meeting. We also reminded the group that interruptions by pets or children were okay, and encouraged them to turn on their cameras for better interaction. MK opened each workshop with a reminder of the purpose of the project overall and each workshop specifically. She explained how to use different functions of the Zoom call and who to call in case of technical difficulties. She also reminded the co-design group that we might need to interrupt discussions to cover all planned activities and that we might directly ask specific members to speak, to ensure everyone had a chance to share their views, which can be more difficult in a virtual setting. MK also emphasised that participation in each workshop was voluntary before inviting everyone on the video call to introduce themselves in a brief ice-breaker task to familiarise the women with each other and with speaking on camera. Typical for the World Café method (Brown & Isaacs, 2005), the workshops used small group discussions in breakout rooms and plenary discussions. We also included short presentations and polls to engage the co-design group. We refrained from using additional virtual tools to make the workshops as accessible as possible and allow co-design group members to join on smaller screens, such as phones or tablets.
Following each workshop, to assess their experience and allow us to improve subsequent workshops, we asked the co-design group to complete an online questionnaire hosted on Qualtrics. RA shared the questionnaire link with the co-design group via WhatsApp. In the questionnaire, we asked the co-design group to select all applicable responses to indicate whether they found each workshop interesting, informative, fun, boring, worthwhile, easy, relevant, difficult, or helpful. We also asked whether they were glad to have come to the meeting and for any other comments, with open-response boxes for both questions.
Following the third workshop, co-design group members were asked to complete a demographic questionnaire collecting information on age, education level, marital status, employment, country of birth, and time spent living in the UK. The workshop experience questionnaires were analysed using frequency statistics and content analysis to assess the co-design group’s perceptions of the virtual co-design workshops and inform activity planning for subsequent workshops.
Intervention Development
FC collated the notes and graphic recordings for each workshop to provide a summary of the co-design group’s views, which were reviewed by MK and RA. We anticipated that the co-design group would report barriers to cancer screening outside the scope of the project, such as structural barriers. MK used the Behaviour Change Wheel (D’Lima et al., 2020) to (i) distinguish which of the screening barriers identified in Workshop 1 were most amenable to intervention functions that could be operationalised as faith-based messages in Workshop 2, and (ii) link these barriers to the most suitable faith-based messages provided by the co-design group or previous research. The Behaviour Change Wheel provides a framework to select appropriate intervention approaches based on available evidence and contextual factors (D’Lima et al., 2020). In this way MK identified motivational barriers amenable to change in a faith-based educational intervention and linked to them suitable faith-based messages. KAR and FC reviewed and discussed MK’s coding of the barriers and linked messages.
Results
The Co-Design Group
Nine women participated in Workshops 1 and 2, and 10 participated in Workshops 3 and 4. All identified as Muslim. Two women were aged 25–34 years. Six women were aged 35–44 years. One woman was aged 45–54 years and one woman was older than 64 years. Most were married and educated beyond secondary school qualifications. Three women worked part- or full-time, four were homemakers, and two unemployed. One woman responded ‘Other’, but did not describe further. Six women were born in the UK and identified as British-Asian, three were born in Pakistan and one in Syria. Of those born outside the UK, three had lived in the UK for more than 10 years and one for less than 5 years.
Workshop 1: How Does Islam Advise About Health Screening?
Workshop Delivery
Starting the meeting with an ice breaker question (Appendix 1) introduced co-design group members to each other and familiarised them with the virtual setting. One woman used this opportunity to learn how to avoid audio interference (e.g. echoes) while helping her mother—who also participated in the co-design group—with using Zoom. Sharing how the women spent breaks in the workshop in the chat, further established group cohesion. Small-group discussions in three virtual breakout rooms encouraged more reserved women to speak and allowed more women to share their views and personal experiences simultaneously, while plenary discussion highlighted agreements and differing experiences across the entire co-design group and promoted self-reflection on those differences. The co-design group appeared to appreciate MK’s short presentation of colorectal, breast, and cervical screening programmes in Scotland for the new information it provided them. At the end of Workshop 1, reviewing the graphic recording (Figure 1) with the group allowed them to elaborate on key take aways from the workshop. Requests from the women for NHS screening programme leaflets to be shared with them, further highlighted the women’s desire for more information about cancer screening. We shared links to the screening leaflets in English, Arabic and Urdu with the co-design group in the WhatsApp group following the workshop.
Co-Design Group Experience
Eight women completed the feedback questionnaire after Workshop 1. Six reported that the workshop was interesting and two indicated that they found it informative. All respondents said they were glad they had attended. In open response comments they added that the workshop was helpful, and easy to understand. One woman reported that she had not expected the workshop to include group discussion. She suggested the co-design group should receive questions for discussion in advance to better prepare their answers. We addressed this in the WhatsApp group by making the co-design group aware that, discussion topics were listed on the workshop timetables the women received before each workshop.
Intervention Development
The focus of this workshop was for the co-design group to start thinking about the place of health and screening within their faith to determine the optimal content of the intervention. Co-design group members said that the intervention should acknowledge the prominent place of health in their faith and also that Islam is a liberal religion without restrictions to seeking healthcare. For example, they expressed that Muslims are given their bodies by Allah and it is their responsibility to look after them, and that Muslims are allowed to use any healthcare, including cancer screening. The group’s discussion suggested that the intervention should highlight that Islam values prevention over cure. The co-design group felt that the intervention should emphasise that Islam encouraged women to become stronger by engaging in health behaviours like cancer screening.
The women explained that, while Imams provided useful general information about health, some women may have misconceptions about what Islam permits. They emphasised that embarrassment was due to cultural, not religious, barriers; Islam would not prevent women from getting screened if only a male healthcare provider were available.
The co-design group also argued that health education, as part of the intervention, would be important, because some women may not know enough about cancer screening. Some co-design group members felt uncertain themselves about the different screening tests, and few discussed colorectal screening. They also explained that the language in results letters was incomprehensible and scary, and offering health education in multiple languages may help to tackle barriers—suggesting the intervention could benefit from the support of interpreters.
Workshop 2: Barriers to Cancer Screening and Faith-Based Messages
Workshop Delivery
The icebreaker activity starting Workshop 2 reminded the women of each other’s names and re-established rapport. Plenary discussion enabled the co-design group to explore screening barriers in greater depth. Using the poll function in Zoom further helped the group achieve a consensus on the three most important screening barriers. Using electronic polling rather than a show of hands, as would be typical in face-to-face meetings, had the advantage that it was anonymous which may have been preferable to the co-design group, and to audiences more generally. Similar to working in small groups at individual tables in face-to-face meetings, working in smaller breakout groups enabled the co-design group to quickly generate a large pool of faith-based messages (Figure 2) to refine in subsequent workshops.
Co-Design Group Experience
Six women completed the feedback questionnaire following Workshop 2; five found the workshop interesting, informative, and helpful. Three reported the workshop was easy to understand. All agreed that they were glad they had attended the workshop. In open comments one woman described the workshop as a “way to share knowledge, experiences and viewpoints”; another added that she looked forward to the next workshop.
Intervention Development
Common Barriers to Cancer Screening Poll Results.
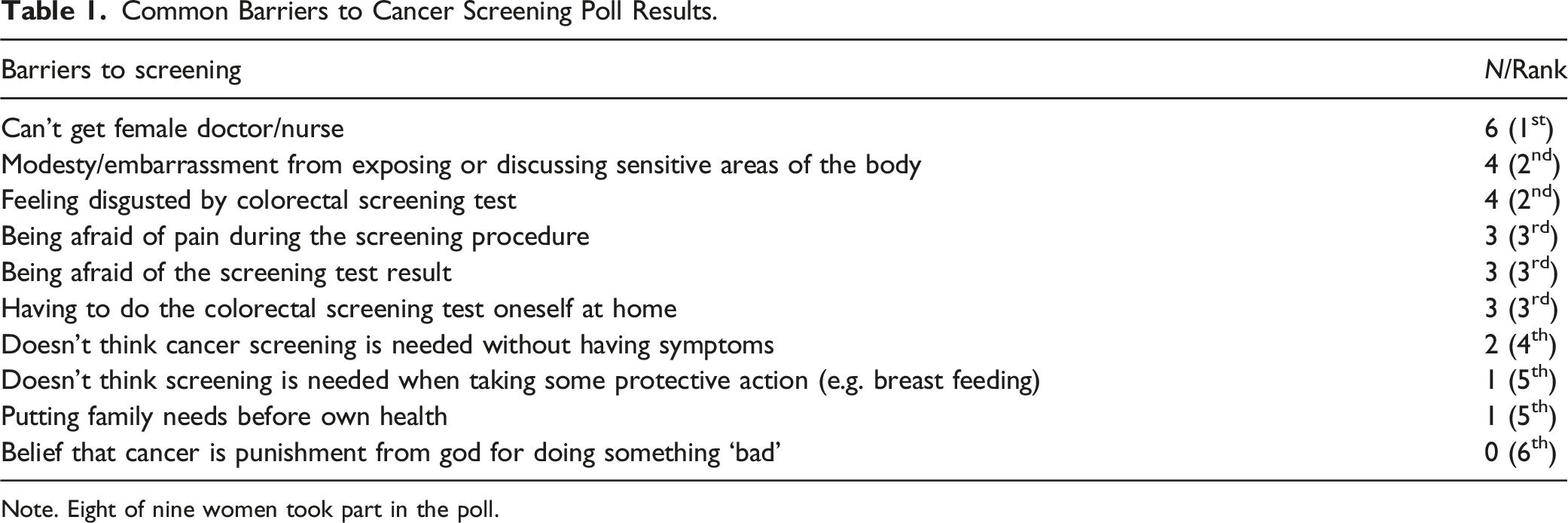
Note. Eight of nine women took part in the poll.
The co-design group felt that to tackle the disgust from colorectal screening, Islam tells women that health is a priority above cleanliness. Another message to tackle lack of awareness was that Islam teaches ‘there is no shame in seeking knowledge’ and screening is one way to gain knowledge about one’s body. Furthermore, women should be taught that Islam perceives them to be the priority and if women cannot care for themselves, they cannot care for their families. The women also felt that Muslim men’s awareness of breast, cervical, and colorectal screening was important, as they may be involved in health care decisions for their female family members. While some women thought women’s health topics should be talked about more openly to reduce stigma, others were uncomfortable with their family members thinking about parts of their bodies the women usually covered.
Workshop 3: Bringing Faith-Based Screening Advice to Muslim Women
Workshop Delivery
In preparation for the third workshop, we used the Behaviour Change Wheel to identify barriers amenable to change through faith-based messages discussed in Workshop 2. The co-design group reflected on the way the researchers had matched screening barriers to the faith-based messages developed in the previous workshop. This achieved in-depth discussion and feedback on wording and suitability of the faith-based messages for particular barriers, as shown in (Christie-de Jong et al., 2022). Working in breakout groups successfully generated a variety of ideas for how faith-based messages should be delivered in an intervention and by whom. A short presentation on the role and value of peer educators by RA familiarised the co-design group with the concept and enabled them to evaluate the potential benefits of peer-led interventions and to consider volunteering as a peer educator in our intervention. This workshop covered a wide spectrum of intervention aspects, so that returning to graphic recording (Figure 3) at the end of the session provided the research team and the co-design group with a useful overview of the key ideas for intervention content and delivery.
Co-Design Group Experience
Ten women completed the feedback questionnaire following Workshop 3. They reported being glad they had attended the workshop and finding it interesting. Four women found the workshops informative or helpful, and three found it easy to understand.
Intervention Development
The co-design group approved of the faith-based messages, with small changes to the wording. They felt the intervention should include personal accounts of Muslim women’s experiences of cancer and screening. They also suggested that healthcare professionals, ideally from Muslim communities, and a female religious scholar should attend the intervention—they did not feel comfortable discussing women’s health issues with a man, including an Imam. The women thought the venue should be a familiar and comfortable mosque or hall, although they acknowledged this was impossible at that time, due to the pandemic and accepted that the intervention could be delivered online.
They also felt trust and confidentiality were key to a successful intervention as women may be scared or embarrassed to discuss screening and concerned about their information being shared in their community. The co-design group thought peer educators should be from their own communities and also of a range of ages, so they could speak to each age group. The co-design group wanted peer educators to be good listeners and receive training and support in their role. At the end of this workshop, the women were asked to consider acting as peer educators; five volunteered.
Workshop 4: Training the Messengers/Intervention Development
Workshop Delivery
Working in small breakout groups allowed the co-design group to provide wide-ranging feedback on the draft intervention at the start of Workshop 4. MK, RA, and FC used the graphic summary of Workshop 3 (Figure 3) to explain how the intervention had arisen from the groups previous discussions. MK provided a short introduction to group facilitation skills and then women interested in being peer educators in the intervention practised facilitating a discussion in the breakout rooms. This gave the women an opportunity to practice these skills with a small group of people. In the final plenary discussion the co-design group shared their experiences of facilitating a discussion and reflected on further support needed to be peer educators.
Co-Design Group Experience
Three women completed the feedback questionnaire following the final workshop. As with previous workshops, they found it interesting (n = 3), informative (n = 2), easy to understand (n = 2), and helpful (n = 1), and were glad they had attended. Reflecting on all four meetings, one woman commented that “These sessions have been wonderful. I’ve learnt a lot throughout these 4 sessions. I enjoyed listening and taking part too”.
Intervention Development
Figure 4 provides a summary of the co-design group’s views on the draft intervention and peer educator training.
The women particularly liked the inclusion of four key elements: 1. Opportunity to discuss barriers to screening, led by peer educators 2. Healthcare provider (GP) presenting health education on cancer screening 3. Two videos of Muslim women sharing experiences of cancer and screening 4. Female religious scholar (Alimah) presenting the view on screening from the perspective of Islam
The co-design group believed having an initial group discussion that allowed women to share their views on barriers to screening would ensure that intervention participants would feel their views were valued. The co-design group felt that women telling their own stories of cancer screening and treatment would be most impactful. They valued having the perspective of a healthcare professional as well as the Alimah, and the combination would encourage women to attend screening. The order of the elements was discussed at length. The co-design group felt that allowing women to express their views first may serve as an ice breaker and allow the healthcare professional and the Alimah to refer to the barriers discussed. The finalised intervention timetable is described elsewhere (Christie-de Jong et al., 2022).
Co-design group members felt nervous about being peer educators and discussed whether they would feel more comfortable running a group discussion rather than the entire intervention session and whether further training could be provided in advance of the intervention meeting.
Discussion
This article aims firstly, to describe adaptations to the World Café approach (Aldred, 2009; Carson, 2011) to facilitate four virtual co-design workshops, and secondly, to describe the development of a faith-based intervention to improve cancer screening uptake for Muslim women using the adapted World Café approach. Community-centred participatory research allowed us to co-design a tailored educational health intervention using faith-based messages to encourage cancer screening with members of the target population. Involving this community in designing intervention content and delivery provided us with a clearer understanding of how the women we worked with viewed their health behaviours from the perspective of their religion. They also helped us identify appropriate language to use in the faith-based messages and their preferred information sources (healthcare professionals, Alimah, women with lived experience, and peer educators) to deliver these messages.
Community involvement also provided insight into preferred intervention settings, with a preference for face-to-face over online meetings. Having to accommodate physical distancing restrictions during the COVID-19 pandemic challenged us to deliver engaging and accessible online-delivered co-design workshops. Not only did this effort result in an intervention deliverable both online and face-to-face, but the high acceptability of our intervention to participants (Christie-de Jong et al., 2022) suggest that we successfully adapted a community-centred co-design approach to an online setting.
Reflections on Remotely Delivered Co-Design Research
The positive responses in our post-workshop surveys indicate we successfully converted the World Café approach to a virtual setting. Hall and colleagues (2021) discuss a variety of measures that may have contributed to fostering collaboration and a trusting environment.
Engagement
In line with Hall et al. (2021), the interactivity and variety of tasks and presentations appeared to make the experience enriching and engaging, in addition to group and plenary discussions promoting self-reflection and sharing of stories. We actively sought to reduce burden on the co-design group by keeping each workshop to 2 hours, including 10 minutes of break time. This also facilitated dynamic progression from one activity to the next during workshops. Similarly, follow-up surveys assessed the workshop experience with a limited number of items.
Accessibility
To address different levels of computer access and literacy, we planned the workshops with awareness that the co-design group may join on smart phones or tablets as well as computers. We had a team member at each workshop solely to support anyone with technical difficulties and provided brief instructions at the beginning of each workshop on how to use Zoom. Users may access this software without installing the programme on their devices, so our co-design group could easily join the workshop by clicking on one link. We also avoided additional online tools, for example for visual or text-based collaboration, which allowed everyone to take part fully in the study with only one window open on their devices. This may also have been helpful for co-design group members less confident in reading or writing in English and allowed the group to focus solely on the video call. Nevertheless, some women on devices with smaller screens reported difficulties seeing shared documents, like the graphic summaries, which we addressed by enlarging details of the summaries as they were being discussed and by emailing these to the co-design group after the workshop.
Confidentiality
The co-design group appeared to feel comfortable discussing potentially sensitive topics in their home environment. Everyone had their cameras on, but some women chose to turn them off to attend to children. To further put the co-design group at ease, we let them know that we would not record the workshops and would take written notes instead (Löhr et al., 2020). Similarly, using electronic polling rather than a show of hands, as is common in face-to-face workshops, allowed group members to express their opinions anonymously. Virtual polling applications can now be integrated into face-to-face meetings also and can provide the benefits of anonymity to virtual as well as face-to-face interactions.
Building Rapport
Access to community gatekeepers was especially important during recruitment and proved challenging to facilitate during the pandemic, as gatekeepers managed the severe impact, including deaths, of COVID-19 on the community. Our team remained in contact with key gatekeepers, however, and we expanded reach through snowball sampling. In addition, we built early rapport with the co-design group in a WhatsApp group. Icebreakers consolidated rapport and breaks during the workshops also provided opportunities for spontaneous interaction and connection; we suggested break activities aimed at encouraging the women to make themselves more comfortable during the video call, for example make your favourite drink. Sharing what they had done facilitated spontaneous conversation, but this appeared to work best when facilitators led by example. Informal conversation is likely to occur more freely in longer comfort breaks in face-to-face workshops that accommodate queueing for refreshments.
Meeting Preparation
While the necessary time and effort to prepare for each virtual workshop appeared to be similar as for face-to-face workshops, the type of required preparation differed. For example, we did not have to prepare a venue for the workshop, clear up afterward, or provide refreshments; we did, however, have briefing meetings with the workshop team. Co-facilitators communicated intensively about workshop activities and materials, so they could each deliver each workshop in case others had technical difficulties. The workshop team also included an IT support volunteer not required in a face-to-face workshop.
Synnot and colleagues (2014) found that qualitative data gathered in online discussion forums were more topic-focused, but less interactive compared to face-to-face focus group data. Video calls using our workshop approach appear to reintroduce the opportunity for interaction, presumably by mimicking a face-to-face environment. Although we cannot say how workshop outcomes may have differed in a face-to-face context, previous research leads us to expect minimal differences (Synnot et al., 2014).
Implications of the Workshop Findings
Faith-based interventions have appropriately addressed attitudes and barriers to breast cancer screening in particular in previous research (Padela et al., 2018, 2019). Our findings indicate such faith-based interventions can be extended to address all three types of screening for breast, cervical, and colorectal cancer. In addition, our findings further highlight the need for gender-concordant healthcare for Muslim women (Padela et al., 2016; Vu et al., 2018), although our co-design group acknowledged that embarrassment as a screening barrier was rooted more in culture than religion (Islam et al., 2017). In contrast to previous work (Padela et al., 2016), we found protection of health was more important than protection of modesty. However, like Padela et al. (2015), we also found that modesty barriers may be reduced by providing exclusively female staff for screening and increasing awareness that women may request female staff for any follow-up procedures.
The limited discussion of colorectal screening in our co-design group supports existing evidence of low awareness of colorectal cancer and screening in Muslim communities (Crawford et al., 2016; Kazi et al., 2021; Siddiq et al., 2020). Our co-design group felt fear of what screening might find, disgust from faecal sampling, and having to do colorectal screening themselves were important barriers to address in the intervention.
As in previous research (Padela et al., 2015), breast and cervical screening appeared to be motivated particularly by cancer in women’s families. Our co-design group viewed screening positively. Although they described discomfort and fear in relation to breast and cervical screening, they reported that they had got used to this and were willing to encourage others to participate in screening. However, they described some structural barriers that prevented other women from doing so. For example, they felt screening results letters could be difficult to understand and frightening, which is in line with research across the general population (von Wagner et al., 2011). Older Muslim women, especially, appear to have unmet needs for health information in alternative languages (Islam et al., 2017). The co-design group also perceived low levels of knowledge about cancer screening in their communities and of understanding Islamic permission of uptake of medical procedures.
Our findings offer some explanation of international evidence of increased barriers to cancer screening participation in Muslim communities during the COVID-19 pandemic (Campbell et al., 2021; Carethers et al., 2020), including increased anxiety about leaving home and using healthcare, and difficulties getting healthcare appointments.
Key messages to address the barriers identified by our co-design group can be conceptualised using the “Reframe, Reprioritise and Reframe “3R” model (Padela et al., 2018). Padela’s 3R model tackles beliefs that hinder the adoption of a health behaviour, through three strategies: (1) reframing the belief within a religious context that is meaningful to participants, (2) reprioritising the belief by introducing a more resonant religious belief, or (3) reforming the belief by identifying logical flaws or theological misinterpretations. For example, the message that Muslim women are worried about healthcare being delivered by a man could be reframed by providing a new target belief that women could live out their preference for female healthcare providers as this can be requested within the National Health Service in the UK. The reprioritisation strategy could highlight the women’s religious duty to be stewards of their bodies, which includes cancer screening. The reforming strategy informs women that according to Islam, important healthcare could be provided by a male health professional if essential and no alternative healthcare provider is available (Padela et al., 2018). Our work adds key messages for cervical and colorectal screening, for example that the great value of health justified the acceptance of impure procedures like faecal sampling (Reprioritise).
Our findings echo evidence that taking care of their health, including cancer screening, was a religious duty (Padela et al., 2016; Vu et al., 2018). Previous work has discussed the complex interplay of God’s decree and personal agency regarding breast cancer and screening (Padela et al., 2016). Our findings agree with the view of medicine as God-given, for people to use, and that Islam placed no restrictions on the permissibility of any medical procedures.
In line with previous research identifying demand for educational interventions (Islam et al., 2017), non-religious messages about the advantages of cancer prevention and early diagnosis through screening were important to our co-design group.
Previous research (Islam, et al., 2017; Vu et al., 2018) has identified existing religious meetings as opportunities for health education. Our co-design group agreed that mosques would provide a suitable venue for our intervention meeting, but emphasised that familiarity and comfort of the venue were the most important characteristics.
The group had conflicting views about including men in the intervention. In line with previous work (Vu et al., 2018), our co-design group perceived Muslim scholars as important sources of healthcare advice and encouragement, and saw the value in male family members understanding the importance of and supporting cancer screening; several women, however, felt uncomfortable about learning about cancer screening in the presence of men. They argued that men should attend separate meetings. Similar to Vu and colleagues’ participants, our co-design group supported the use of peer educators and emphasised that these would need to be women trusted and respected in the community. Vu et al. also reported a desire for peer educators to have religious and clinical knowledge. This was not raised in our work, but our co-design group identified healthcare providers, female religious scholars, and women with lived experience as essential sources of information, who can attend to religious and clinical aspects of the intervention. In taking on the role of peer educators themselves however, our co-design group agreed that training to perform this role is necessary.
In previous research, participants welcomed the group setting of health education classes (Vu et al., 2018). Although our co-design group agreed that sharing of personal screening experiences would engage intervention participants, they needed the intervention delivery to emphasise and ensure confidentiality, to address concerns around gossip and embarrassment.
Strengths and Limitations
Available research time was a principally limiting factor in how much the co-design process could be led by the co-design group (Brunton et al., 2017). Being restricted to four workshops meant we had limited time for the co-design group to consider different intervention approaches, and we could not hand over the co-design process fully. Instead, we commenced the workshops with a pre-conceived idea, aiming to co-design a faith-based intervention to optimally use our workshop time and resources.
Brief evaluation after each workshop showed that the co-design group found each workshop engaging. While no women responded negatively when asked if they were glad to have participated in each workshop, this phrasing could be a leading question. Nevertheless, their responses align with other evaluation data and the women completed the evaluation questionnaires anonymously and privately to reduce demand characteristics.
Recruitment through mosques and religious resource centres is likely to have resulted in a sample of women for whom religion is particularly influential in health behaviours. Further research is required to determine whether the religious elements of the intervention make it less relevant to Muslim women recruited through other community groups rather than mosques and religious centres.
In addition, by requiring the co-design group to be proficient in English, we may have recruited a more acculturated and more highly educated sample. This level of knowledge allowed the co-design group to articulate and prioritise which needs the intervention should address. It is also possible however that a highly educated co-design group may be unable to represent Muslim women with language barriers to accessing healthcare. Our focus group evaluation of the intervention highlighted the need for information in alternative languages (Christie-de Jong et al., 2022).
All co-design group members resided in Glasgow. Their views may differ from Muslim women residing elsewhere. For example, women in rural areas may have different preferences for intervention delivery or experience other access barriers, like travel to appointments. Nevertheless, Glasgow has the largest proportion of Muslims living in Scotland (43%) and most of the Muslim population in Scotland live in cities (Elshayyal, 2016).
We were unable to recruit Black Muslim women to the co-design workshops. Further research to assess the acceptability of the faith-based intervention should attend particularly to experiences of Muslim women from communities not represented in our sample. Aside from sharing a ‘God-centred framework of health’, Muslims are a diverse group, with differing interpretations of Islam and religious values. This study did not measure religiosity, which could be an important factor in determining effectiveness of faith-based interventions (Padela et al., 2015). However, good health is perceived in the Muslim faith as the greatest blessing from God (Attum et al., 2022), and the belief that one should take responsibility for one’s health is rooted in Islam and can work as an enabling factor to screening (Azaiza & Cohen et al., 2008; Lau et al., 2022).
Furthermore, two of the workshop facilitators were non-religious, white European women who may have been perceived as outsiders. This may have led, for example, to the co-design group’s emphasis on their religion as liberal rather than restrictive in relation to healthcare. However, Ryan and colleagues (2011) argue not only that the deciding characteristics to establish a researcher’s outsider status are often opaque (e.g. our researchers’ gender may have had greater importance to the research relationship than their ethnicity), but also that outsider researchers may encourage less self-censorship. This is in keeping with our co-design group’s concerns about confidentiality of community education interventions and demand for trustworthy peer educators.
Hosting the workshops online allowed us to include women from different areas of Glasgow without burdening them with additional time and cost to travel to a physical venue and increased women’s availability for the workshops. Women who were looking after children appreciated being able to do this during the workshops instead of having to organise external childcare. While some women were unable to attend the workshop during weekdays due to work commitments, others would have been unable to attend on weekends. We strove to choose the dates and times that suited the majority of women interested in participating in the workshop.
Our reliance on women to use their own devices and internet connections to join this research may have prevented those with limited access to information technology or to the internet from taking part (Hall et al., 2021). If similar future research is to avoid exacerbating health inequalities, researchers should budget and plan for research that enables access to Internet-connected devices.
Conclusions
This study is among the first to adapt existing participatory methods for remote delivery and presents an example of how to do so successfully. Recent advances in virtual communication and collaboration tools allowed us to facilitate four co-design workshops to create a virtual intervention to encourage engagement with cancer screening among Muslim women. This intervention focuses on faith-based messages to support screening in combination with women’s lived experiences, peer education, and GP-delivered screening information. Early evaluation with another group of Muslim women has demonstrated the intervention’s acceptability to participants, feasible delivery, and potential to increase cancer screening uptake (Christie-de Jong et al., 2022). Further research will establish the feasibility of a randomised controlled trial to test intervention effectiveness in Scotland and the North East of England and compare intervention delivery in-person and online.
Supplemental Material
Supplemental Material - Adapting Participatory Workshops to a Virtual Setting: Co-Design With Muslim Women of a Faith-Based Intervention to Encourage Cancer Screening Uptake
Supplemental Material for Adapting Participatory Workshops to a Virtual Setting: Co-Design With Muslim Women of a Faith-Based Intervention to Encourage Cancer Screening Uptake by Marie Kotzur, Rana Amiri, Lauren Gatting, Kathryn A. Robb, Jonathan Ling, John D. Mooney, and Floor Christie-de Jong in International Journal of Qualitative Methods
Footnotes
Acknowledgements
We thank Afag Elsheikh, Aghnaa Gayatri, Clara Kurtidu, Hooran Khattak, Laura Bell, and Katy Holloran who supported the delivery of the workshops.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Scottish Government, Scottish Inequalities Fund [grant number n/a].
Ethical Statement
Data Accessibility Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.