
Abstract
A deficit framing continues to surround the perceived capabilities of people with dementia to comprehend and engage with cartographic maps. While some people with dementia might experience issues with wayfinding and spatial orientation, this has frequently been unfairly extended to all people living with dementia. From the perspective of qualitative research, the potentials for how mapping might contribute methodologically to understanding how some people with dementia negotiate and experience place has yet to be fully realised. A nascent turn towards geographic concepts of space and place has seen social health and dementia researchers acknowledging the vitality of place and neighbourhoods for understanding how everyday life unfolds relationally for people with dementia. However, creative methods to capture these spatial experiences are needed. This paper describes the nature of the scaffolds that supported involvement of people with dementia into a qualitative GIS project. These scaffolds were essential for supporting participants to trace out their narratives, histories, connections and barriers to engagement in their familiar neighbourhoods. We demonstrate via an Australian example how scaffolded sketch mapping interviews and crowdsourced maps offer tangible and evocative means to pin their lived experiences to the map. For place-based dementia research, qualitative GIS offers two paths forward. First, with the relevant scaffolds in place, the imaginative power of the map can engage people with dementia in qualitative research about the places they know and frequent. Second, spatial visualisations are imbued with political agency, acting as a conduit toward meaningful change in their local communities.
Keywords
Introduction
Humans have been making and using maps for millennia. From viewing and engaging with map images perhaps as tactile objects (such as a paper atlas or an office floor plan) or nowadays as digital media, maps and spatial technologies remain an everyday part of our lives. But maps are more than devices that convey spatial relations. They also hold potent performative qualities, both recording and creating the worlds they set out to document (Crampton, 2009; Rose-Redwood & Glass, 2014).
Despite recognition that mapping is a deeply embedded and universal cultural practice (Stea et al., 1996) a deficit framing continues to surround the perceived capabilities of people with dementia to comprehend and engage with cartographic maps. While some people with dementia might present with issues associated with wayfinding and spatial orientation, this has been unfairly extended to all people living with dementia. The potentials for how mapping might contribute methodologically to understanding how people with dementia negotiate and experience place has yet to be fully realised. This paper demonstrates two kinds of qualitative mapping practices – sketching and crowdsourcing – that revealed otherwise hidden and politically powerful spatial narratives about everyday life with dementia in the community.
This paper’s structure begins first with a background to GIS, its uptake in health research contexts, alongside the turn toward place in social health research. After outlining the research project and its study site, we describe the sketch mapping methodology and the scaffolds we deployed to produce the key analytical results from this interview technique. Next we outline the crowdsourcing technique and the attendant scaffolds required, before discussing unforeseen positives from this distributed and public-facing data collection phase. Our discussion section then reflects on the scaffolds for the two engagement techniques and underscores the necessity of putting the lived experience of people living with dementia ‘on the map’.
Mapping in the Context of Health and Dementia
Mapping practices of spatial analysis and cartographic display have expanded in recent decades through Geographic Information Systems (GIS). Geographic Information Systems store, analyse and present geographic data and are particularly adept at visualising patterns within and between multiple digital inputs. In other words, GIS can create maps that overlay various layers of information, such as population health statistics, road networks and land use categories, permitting spatial analysis routines to run within and between layers.
GIS support decisions around planning and governing space, producing tangible impacts across numerous social, economic and health spheres. Epidemiology and public health have used maps and spatial thinking for hundreds of years to explain location-based relationships between population characteristics and health outcomes (Waller, 2017). Since GIS became widely available in the late 1990s, these fields have seen a rapid uptake of GIS capacity to understand and plan interventions for all manner of health issues, including infectious diseases, cancers and chronic conditions (Cromley & McLafferty, 2012). In the dementia context, Bagheri et al. (2017) deployed GIS to understand the concentration and forecasting of dementia diagnoses to support health service planning, with an eye to placing key dementia services in those communities with the highest need. From an outdoor mobility standpoint, Wettstein et al. (2015) used a combination of GPS tracking, GIS and multivariate statistics to create typologies of walking types amongst people with dementia.
The bulk of public health engagements with GIS fit within a spatial-analytic biomedical approach. That is, a reliance on spatial and statistical analysis routines suitable for modelling, forecasting and visualising disease clustering; mapping population attributes that can indicate spatial patterns of health risks; and uncovering the geography of health disparities and access to services (Cromley & McLafferty, 2012). However, interest is growing in deploying GIS as part of mixed methodological inquiries, where a plurality of methods can permit more nuanced understandings of a research problem over quantified GIS data and methods alone (Kwan & Knigge, 2006). This can be particularly helpful in research that seeks to illuminate the contextual role of place and neighbourhood on individual and small group health and wellbeing outcomes. Examples that have taken this approach include research on obesity in childhood (Wridt, 2010); illicit drug use by adolescents (Mennis et al., 2013); welfare dependency amongst low-income families (Matthews et al., 2005); experiences of place by the elderly (Milton et al., 2015) and experiences of wellbeing for supported workers employed by social enterprises (Farmer et al., 2020). These studies are beneficiaries of earlier epistemic debates (see Pavlovskaya, 2006; Cope & Elwood, 2009) as to the nature of GIS that have successfully decoupled the technology from its supposed quantitative roots.
Following trenchant critique of GIS as quantitative and unsuitable for social and qualitative researchers (see Pickles, 1995), critical GIS scholars saw potential rather than foreclosure, forging ahead with alternate and productive engagements with GIS. These included Feminist GIS for visualising gendered experiences of space and time (Kwan, 2002) and a broad array of participatory GIS practices that sought to involve marginalised communities or groups in map-making for their own ends and advocacy (Dunn, 2007; Elwood, 2008). Across the early 2000s, GIS began to be seen as a “critical visual method” that can assist understanding of the spatiality of social processes (Kwan & Knigge, 2006, p. 2001). This potential is increasingly being realised by qualitative researchers and projects that adopt a Qualitative GIS stance. Qualitative GIS can be thought of as a mixed methods framework that bridges between analytical mappings and diverse qualitative ways of knowing. Qualitative GIS recognises that all knowledge is partial, situated and complex (Cope & Elwood, 2009). Qualitative GIS thus welcomes a variety of data sources familiar to qualitative and ethnographic research (for example narrative text, audio, photo, video and sketches) into a GIS. Such data can be contrasted, triangulated or combined with quantitative data for subsequent spatial visualisation. The analytical and visualisation capacities of GIS open spaces of possibility for project-specific mixes of data types and epistemologies to collide, often in productive and unforeseen ways (Brown & Knopp, 2008; Gibson et al., 2010).
This growth in mixed methods GIS is at odds with the way that biomedical research has historically problematised the spatial experiences of people living with dementia. This has included a focus on the negative outcomes of getting lost behaviours (e.g. MacAndrew et al., 2018; Furumiya & Hashimoto, 2015); the need for tracking and monitoring to maintain safe outdoor participation (Ly et al., 2015; Mangini & Wick, 2017; Mckinstry & Sheikh, 2013); and even the institutionalisation and segregation of people with dementia, restricting free access to the outdoors (Steele et al., 2019). This has in some part been attributed to the impaired wayfinding capacities of people with dementia including reduced ability to remember routes, follow written instructions and difficulties using maps (Mitchell & Burton, 2010; Cushman et al., 2008). Yet like other capabilities, some map-reading capacities for some people may remain. We therefore caution against applying blanket definitions that all people living with dementia cannot comprehend Cartesian maps. As we seek to demonstrate, with scaffolds in place they can be useful research instruments for uncovering the everyday importance of place and space.
The social health model of dementia (Huber et al., 2011; Vernooij-Dassen & Jeon, 2016) recognises not only the contribution of individual capabilities but also the importance of space and place as mediators of wellbeing within the everyday lives of people with dementia. A number of methods have been used to understand the role of place and its contribution to social health including: quantitative auditing for the presence of dementia design principles within community buildings (Fleming et al., 2017) and neighbourhood precincts (Su, 2013); and qualitative methods such as interviewing and walking interviews (Mitchell & Burton, 2010). Some of these have engaged with mapping in a limited way. For example, in walk-around interviews as part of field notations (Ward et al., 2017), as an aide to communicating design principles which emerged as important to community mobility (Mitchell & Burton, 2010) or as a means for revealing important social networks across multiple scales (Clark et al., 2020). This work engages with geographic concepts when analysing, synthesising and presenting findings, with narrative approaches and textual representation dominating. While these modalities convey information about spatial relations, social health research is beginning to turn toward more explicit use of spatial technologies and rhetorically powerful cartographic images.
GPS tracking is one such spatial technology. Despite being deployed earlier as a biomedical tracking tool for understanding and intervening in wandering behaviours (e.g. Wettstein et al. (2015)), combining these locative media with qualitative methods has yielded new insights. For example, Sturge et al. (2020) take a qualitative GIS approach, combining GPS-tracking, travel diaries and subsequent interviews with people living with dementia in a dense Dutch city, revealing routine and occasional activity spaces and the degree to which social supports were required to access the latter. Similarly, Biglieri and Dean (2022) utilised GPS tracking while accompanying participants living with dementia on walking interviews to investigate their wayfinding strategies in the dispersed suburbs of Waterloo, Canada. Similar to Mitchell and Burton’s seminal work (2010), they uncovered that important landmarks were also present in car-dominated suburbia, advocating for more nuanced understandings of how long-time residents living with dementia remain active pedestrians in places often portrayed as monotonous and unwalkable. These examples demonstrate that crucial further context about the lived experience of navigation when living with dementia can be gathered with mixed method research, above and beyond just recording movement patterns with GPS.
Even without the added analysis benefits of GPS, go-alongs have been used repeatedly with people living with dementia to break free of the, at times, clinical and decontextualized setting of the sit-down interview, enhancing participant recall as interviewers accompany participants in real time, multisensorial journeys (Mitchell & Burton, 2010; Odzakovic et al., 2020). Indeed, Jones and Evans (2012) have found that accompanying participants on walks yields a much greater frequency of place-based discussion to occur than during a standard sit-down interview. However, when go-alongs are augmented with GPS and become a ‘spatial go-along’ (Jones & Evans, 2012), the spatial technology is only used in a passive mode. That is, map representations of the GPS trail are not engaged with as a prompt while on a walk. The spatial data (tracks or waypoints) collected by the GPS tend only to be used for subsequent GIS analysis and visualisation in parallel with interview or diary transcripts. While not as multisensorial as a spatial go-along, our approach sought to investigate whether Cartesian maps might animate place-based discussions in the static research setting. If brought front and centre, might they act as prompts for generating spatial narratives about everyday activities and barriers to maintaining social connection?
Our decision to pursue mapping as an alternative to spatial go-alongs was also inflected by concerns related to safety, practicality and ethics (Adekoya & Guse, 2020). For some participants with restricted mobility or during inclement weather, walking might not be the most practical option. For these contexts, a sit-down mapping activity was worth exploring. Furthermore, we were buoyed by the value of introducing sketching and other visual artefacts into interviews with people living with dementia (Phillipson & Hammond, 2018). Broadening the range of interview prompts can enliven otherwise staid and challenging interview settings (Smith & Phillipson, 2021; Dooley et al., 2021).
The ‘Dementia Friendly Kiama’ Project
This paper reports on an Australian study undertaken in Kiama, a regional local government municipality with a population of over 21,000 people (Australian Bureau of Statistics, 2022). The town itself consists of a small downtown area with low-density suburbs of freestanding homes stretching north and south along the coastline. To the west are productive dairy farms and nature reserves of the densely wooded Illawarra Escarpment. Kiama is a quintessential Australian ‘sea-change’ town, popular with retirees with an attractive coastal location, village atmosphere and rail access to nearby Wollongong and Sydney. The larger Kiama State Electorate has a population of 79,000 people (Australian Bureau of Statistics, 2022). Due to the region’s ageing demographic profile, the number of people living with dementia in the State Electorate is projected to increase from an estimated 1200 in 2012 to almost 4000 by 2050 (Australian Bureau of Statistics, 2012).
The Dementia Friendly Kiama project, which commenced as a partnership between the University of Wollongong, Dementia Australia and the local Kiama municipal council (Phillipson & Hall, 2020), was guided by its use of a Community Based Participatory Action Research framework (Israel et al., 1998). In the early stages of the project two governance groups were formed: a Dementia Advisory Group (consisting of people living with dementia and their carers); and a Dementia Alliance (including members of the Advisory Group, representatives from partner and other organisations, and interested individuals). Both groups have participated in the various cycles of formative and evaluative research and taken actions in response to create local change. These included increasing community awareness about dementia and local services, promoting understanding of the lived experience of dementia (in particular, how they moved about and utilised community environments), reducing the stigma of dementia and improving the accessibility of the local environment (Phillipson et al., 2019).
Generative Sketching
Our trialling of static spatial methods with people living with dementia began first with sketch maps: paper maps of a study area for participants to sketch and draw upon while answering questions about that place (Boschmann & Cubbon, 2014). The sketching technique emerged from the mental map tradition that is carried out on a blank page, permitting an individual’s cognitive map and sense of place to emerge through drawings of their favourite landmarks, ways and nodes (Lynch, 1960; Gieseking, 2013). Sketch maps extend upon mental mapping because the base map, instead of a blank page, has landscape features already drawn upon it. This has a two-fold impact on the resulting data. First, regarding elicitation, sketch maps encourage deep engagement with the base map, permitting participant and researcher to effectively place themselves in it, by orienting themselves against any map features (for example via the street network or by using the names or symbols representing physical or built landscape features). Second, the base map encourages relatively spatially accurate markings to be made in an additive fashion, often via drawing with different coloured pens in response to spatial questions during an interview. Later conversion with a GIS can ‘lift’ and separate any markings made by participants from the underlying base map.
A review article by Curtis (2016) demonstrates that since the early 2000s, research combining sketch maps with GIS is on the increase. Importantly for social health researchers, sketch mapping has been deployed successfully and repeatedly with marginalised groups otherwise excluded from official spatial data. Through sketch mapping, their lived experience is transformed into authoritative spatial data. In our research, we wanted to see just how helpful sketch mapping might be for uncovering the hidden geography of life with dementia in a community setting. Due to the previous barriers to the use of this method with people with dementia, we also wanted to understand the type of scaffolds needed to support their engagement with both the sketch and crowdsourced maps. The concept of ‘scaffolding’ has been usefully employed to describe how carers and service providers create supports for people with dementia in their daily lives (McCabe et al., 2018). However, it is novel to apply it to an understanding of the supports that people with dementia may need to engage with the ‘doing’ of qualitative research. In this case, we apply it here as method to highlight the specific actions that qualitative researchers can take to support the engagement of people with dementia in qualitative GIS research.
Local Kiama residents living with dementia and their care partners were recruited to take part in dyadic sketch mapping interviews to explore their daily experiences of activities undertaken ‘at home’ and ‘out and about’ in the community. Participants were recruited through local council and community service groups. Prior to commencing interviews, all participants were provided with a written Participation Information Sheet. The details of the study were also verbally explained with opportunities for people to ask direct questions to promote informed consent from the people with dementia. Written consent was obtained from both the person with dementia and their supporter/carer. Researchers also attended to verbal and behavioural indicators throughout to monitor the willingness and engagement of participants (Dewing, 2008). Ethical approval for both was provided by the University Human Ethics Committee HE14/065.
Twelve interview dyads – each including a participant with dementia and their care partner – were successfully recruited. Participants with dementia were aged between 60 – 84 years. Two had younger onset dementia. Seven of our participants living with dementia were female and five were male. All spoke English at home, and the majority lived in their own private homes or apartments with an informal care partner. Most (7/12) of the care partners were in a married or close personal relationship with the person with dementia, one was a friend and two were adult children of the person with dementia. Ten out of 12 recalled they had been given a formal diagnosis of dementia and all of these had been diagnosed within the previous 2 years. Most could walk more than 500m without assistance and eight out of 12 rated their overall quality of life as either good or very good.
Scaffolding for Generative Sketch Mapping with People with Dementia
All except one of the mapping interviews were conducted face-to-face in the participants’ homes – the exception taking place in a local cafe. This approach promoted familiarity and comfort, avoided connotations of a clinical interview, and made use of environmental cues (Cridland, Phillipson et al., 2016). The majority were conducted by two researchers. One acted as the primary interviewer of the person with dementia, with the second often interviewing the carer separately or taking notes or providing additional context to support more meaningful engagement of the person with dementia and the map. Interviews were audio recorded for later transcription. Along with the traditional semi-structured interview technique, we produced two individual sketch maps as a visual stimulus for each participant (Figure 1). We first represented their immediate local neighbourhood to scaffold maximal engagement for each participant with dementia. The second map represented the Kiama town centre (or high street). Extending on the general principles of familiarity and comfort promoted by Cridland et al. (2016), use of these tailored scaffolds promoted more opportunities to reflect and engage with a familiar and visual backdrop to the places and experiences that people were describing. Example sketch maps from one interview dyad. Their home village (Gerringong) shown left and Kiama town on the right. Interviewer notes helped for added context during the interview and subsequent GIS analysis. Base maps produced using www.fieldpapers.org.
When presenting the sketch maps for the first time, we would use visual, physical and narrative scaffolds to support engagement with the maps. First, physical and visual orientation of participants was achieved by marking the map with a cross to identify the location of the person’s home (which in all but one case was also the location of the interview). Participants were then given physical ‘ownership’ of the map, being allowed and encouraged to rotate the map in whichever direction was most helpful. Finally, we used ‘narrative’ scaffolding, encouraging the interview dyad to orient themselves further, by identifying local places of interest or significance on the map and talking about them. Conversation and storytelling then proceeded, and participants were encouraged to respond by providing a narrative to their activities whilst also drawing with different coloured pens in response to any questions with a spatial inflection. Sample questions from the semi-structured interview guide included: • What sort of things do you get up to during a typical week when you are ‘out and about’? • Where are the places you like to go? Are there any places you don’t like to go? • How does the environment support you to maintain the activities/roles you are interested in? Where? By who? What type of support? • Is there anything that could be done to support you in getting ‘out and about’ that would improve your quality of life?
Reflecting on the scaffolded sketch mapping process, we noticed both opportunities and drawbacks. Prior research has indicated that drawing and sketching during interviews can sometimes break down power relationships between researcher and participants, particularly for those less adept with expressing themselves verbally (Bagnoli, 2009; Brennan-Horley et al., 2010). However, in our interviews, participants sometimes found it challenging to draw upon sketch maps. Here we were confronted directly by those well-rehearsed difficulties that some people living with dementia have with map reading. Importantly though, we were not treating the interview as a test of their spatial comprehension. Rather, we adapted as required to suit their capabilities and keep the conversation flowing. For example, we did provide support around comprehending the maps when necessary, pointing, questioning further or drawing at the direction of participants. As a result of this active scaffolding, some of the sketch map data is very much co-created by researcher and person living with dementia, or person living with dementia and their carer. Taking this approach ensured their place-based experiences and narratives were captured and included on the map.
Overall, the sketch maps grounded discussions about the everyday activity space of our participants – broadly, documenting and discussing places they travelled to and any underlying experiences of everyday mobilities. As is regularly the case with sketch mapping research, the map became an active agent in the interview (Brennan-Horley & Gibson, 2009), drawing everyone into it as we gathered around to discuss living in Kiama and surrounds.
The map acted as an ‘aide memoire’ for particular interviewees living with dementia, assisting to record their quotidian activities:
“Well most of the places, we either go up to the main street by car, or we walk around. But most of the things up there we only go to IGA [supermarket], shopping, chemist or the doctors.”
Occasionally the map helped spark productive conversational tangents. For example, one interviewee living with dementia used the map to pick out a walking trail back into town:
“And when you look down here, there’s a lagoon. You can only do it when the tides out, you can walk across with your shoes off and the other side they’ve got a walkway from there right through to Kiama”
This exchange dovetailed from prior map-based discussion about how a particular headland was an excellent site for watching whales on their seasonal migration. Discussion about these important elements of the natural environment that contributed to their social health flowed by enrolling a map into the interview.
The value of the sketch mapping to uncover the geographies of dementia
We turn now to outcomes generated during the scaffolded sketch map exercise. In keeping with a mixed method stance, the qualitative GIS analysis that follows relies on co-presentation of quantitative and qualitative data (Elwood, 2010). Spatial analysis of sketch map data utilises the quantitative visio-spatial capabilities of a GIS, providing understanding about collective usage patterns in public space. To add further meaning to those patterns, we intersperse quotes and comments from select participants gathered during the mapping activity. Co-presenting quantitative and qualitative data sources in this way enhances the explanatory power of both data types, providing a more integrated perspective of how our participants negotiated their everyday activity space.
Figure 2 presents responses collated and coded in three ways: First as locations and zones they regularly travelled to, then a subset of those places that held special meaning (and by extension might already be ‘dementia-friendly’), and finally places or zones they avoided or found difficult. In each frame, the darker shades denote where multiple spatial responses lined up across the 12 interviews. A four panel map detailing places of everyday travel, meaningful sites, spaces of difficulty and overlaps.
Perhaps most starkly, these results illustrate participants maintaining a collective physical footprint in Kiama. Contrary to narratives of a shrinking life-world (Duggan et al., 2008) and ‘prescribed disengagement’ (Swaffer, 2015) our participants regularly visit sites across the entirety of the commercial zone. Concentrations emerged as they moved between key sites located predominantly within Kiama’s town centre, adjacent public green space and dispersing out into coastal areas. Kiama’s small, compact and walkable commercial zone maximised opportunities for social health, with sites for everyday travel either co-located or only a short distance apart.
When read alongside accompanying narratives from interviews, we were able to comprehend the multiple layers of meaning that maintaining mobility achieved for our participants. As was relayed to us by one participant living with dementia:
“I love to go over the Centro [shopping centre] here and, and it’s, everybody’s very friendly and you can have a nice cup of coffee and that’s what we did this afternoon. We met and we had a nice coffee there… you go into Centro and they all say hello to you whether they know you or not. You know what I mean, and you can start up a few words like a beautiful day or something like that and you come home and think oh, I met so and so today.”
Instrumental travel to the local grocery store was equally a chance to maintain important social connections. Active engagement and exercising of personal agency through interactions with shopkeepers, health professionals and the broader community meant our participants contributed to their social health, simply by participating in the everyday social life of Kiama.
Resonating with much other research about living with dementia in the community, the sketch map results also revealed the daily challenges of contending with the material environment. Difficult places were often couched in terms relating to problems with physical accessibility: “It’s very, very hilly, so you’re coming out of the park there and it’s quite a wide road, so even for a person to cross that road, you’ve got to have a spring in your step” (Carer)
The steep topography leading into Kiama’s two main commercial streets, difficulties with car parking and busy road crossings all appeared in Figure 2. Negotiating these spaces was achieved via a range of supports including travelling with others or avoiding difficult places especially at busy times like weekends and public holidays: “....planning not to go in there during Christmas, it’s murder. And after school holidays” (Carer)
However, many of the places where our participants experienced access difficulties were also en route to their most meaningful and important sites: “I feel that area’s very difficult. But you see you’ve got a doctor’s surgery there on the corner, a dentist, so you’ve got two essential services there” (Carer)
Continuing to traverse the downtown area to get to meaningful places remained a priority, even though the journey presented risk. The usefulness of composite visualisation of sketch map data was how it enabled us to see, in one frame, how these contradictory spatial narratives intersected.
Scaling up through Crowdsourced Web Mapping
To scale the affordances of sketch mapping up to a wider cohort beyond our interviewees we also investigated the utility of a crowdsourced web map into our data collection. In a crowdsourced model, the power of the crowd is harnessed to gather geospatial information through a distributed web map interface (Sui et al., 2013). One of the most predominant means for gathering location information is to encourage participants to place pins upon sites of interest. Such mappings form an important part of Public Participation GIS, informing academic understandings of place attachment across multiple domains including landscape values, development preferences and spatial experiences (Brown & Kyttä, 2014). NGOs have also begun leveraging crowdsourcing capacities to collect spatial and narrative data (e.g. Plan International, 2022). Activist spatial crowdsourcing platforms can potentially generate substantial public by-in, and in the case of Plan International’s ‘free to be’ project, substantive positive change to the planning and policing of public space for women and girls’ safety resulted (Kalms, 2017). More recently, crowdsourced pin maps have become almost mundane public engagement tools, evidenced in their increasing uptake by local authorities seeking spatially oriented input into planning processes. We again were interested in highlighting the scaffolds needed to engage people with dementia in this type of qualitative research activity.
Scaffolding Crowdsourced Mapping with People with Dementia
A crowdsourced web map was created on www.socialpinpoint.com (one of a slew of providers that now service the growing market for crowdsourced mapping) and placed upon a project webpage we dubbed ‘Our Place’. Ethical clearance for this public-facing phase was granted by University Human Ethics Committee HE15/165. This crowdsourced mapping phase occurred after preliminary analysis of the sketch mapping interviews. Indeed, it was prompted directly by members of the Kiama Dementia Advisory Group, who upon seeing the collective cartographic results of the sketch map interviews (refer to Figure 2) saw the potential in continuing to map their town with the aim of affecting change through sharing geospatial information among themselves and with government representatives. Unlike the sketch map interviews, which targeted people living with dementia and their care partners or family, the Our Place Kiama map invited public contributions from anyone with internet access and an interest in the dementia friendly issue, but still inclusive of those with dementia and their care partners.
Figure 3 shows a screen capture of the interface in action. Importantly, the interface of the web map, the instructions and appearance were co-designed with people with dementia and their care partners as much as possible to support the clarity of purpose and potential engagement of users who may be living with dementia, or other aged-related disabilities. Users could either access the crowdsourced map from a desktop computer or mobile device. Two different types of pins were available to the user to place upon the map. A blue pin for places they ‘liked’ or considered ‘dementia friendly’ and a yellow pin indicating ‘ideas for action’ or positive change. Once a pin was dropped a comment bubble permitted textual input alongside an option to add a photo. Users could also choose to not add data and just review other responses by either clicking on existing pins or reviewing an interactive list of textual responses via a side panel. Clicking on a response in the list would highlight it on the map, and vice versa. Therefore, users could interactively explore the likes and ideas of others in their spatial context, and potentially respond or rate those submissions with a thumbs up or down. The our place map interface in action.
Based on feedback from the Dementia Alliance members, and on the experience of the use of simple sketch maps, the background layer from google maps was chosen to include aerial imagery overlain with roads and prominent place names. As opposed to the ‘cleaner’ standard google maps background designed for car-based navigation, aerial imagery provided extra visual orientation cues such as prominent buildings, tree-lined boulevards and car parks which were identified as important during user testing. Upon accessing the site, the map was centred on Kiama town centre. Standard web map capabilities of zooming and panning were available for subsequent navigation to a point of interest, or via address searching.
To maximise participation, the interface was pilot tested by Kiama Dementia Advisory Group members – including those living with dementia – who suggested improvements to textual instructions and design elements. Where possible some alterations were attended to, within the confines of the Social Pinpoint platform. It does permit changes to text, but not more systemic alterations to the user experience (e.g. positioning and sizing of particular webpage elements) that might make a website more legible for people living with dementia. Upon dropping a ‘like’ or ‘idea’ pin users were prompted to leave a comment and then click a checkbox against one of four status options: ‘Community member living with dementia’, ‘Family carer or friend of someone living with dementia’, ‘support worker’, or ‘other’. In contrast to the sketch mapping interviews, where further discussion was generated as spatial data was collected, the crowdsourced map was very much a hands-off research and engagement tool. As we were not present during most of the data production, we lack any further context about the pins beyond what participants chose to write in the online form and provided as their status.
Finally, training and support was provided for potential users of the website to place their pins during community group meetings, Dementia Alliance meetings and public events. This support was in recognition of low digital literacy and potentially minimal prior engagement with webmaps amongst the target audience. At these, researchers were present with either a laptop or tablet device running the Our Place map and were able to answer questions, model the haptic process of engaging with the webmap, or help place pins and type written responses at a participant’s request. This in-person support for participation thus became an important scaffold, making the crowdsourced mapping process more manageable.
The Value of Crowdsourced Mapping to Understand the Geographies of Dementia
Figure 4 displays the spread of ‘like’ and ‘idea’ spots as clusters across Kiama as well as a breakdown by user type. During its 6 months of active promotion 30 pins were added, nearly all located in the commercial zone, with approximately two-thirds of these highlighting dementia friendly businesses and locations, including hotel and restaurant suggestions to favoured cafes and shops. These blue pins were more likely to be suggested by carers and support workers. As evidenced in a selection of written comments that accompanied these pins (Table 1), contributors were signalling about qualities of the places that might help others living with dementia to enjoy being ‘out and about’ in Kiama. These included tips on helpful material elements related to mobility, alongside positive visual and auditory elements. Also evident were examples of social supports provided by the actions of staff that made for a dementia friendly experience. Public education campaigns were a key plank of the Dementia Friendly Kiama project, specifically designed and evaluated to reduce stigma and raise understanding amongst the general public, including local businesses (Phillipson et al., 2019). Here the map was potentially recording some of those education outcomes, directing any locals or visitors living with dementia toward locations where they might more easily continue active community engagement. Crowdsourced ‘like’ and ‘idea’ spots. A Selection of Comment Pins by User Type.
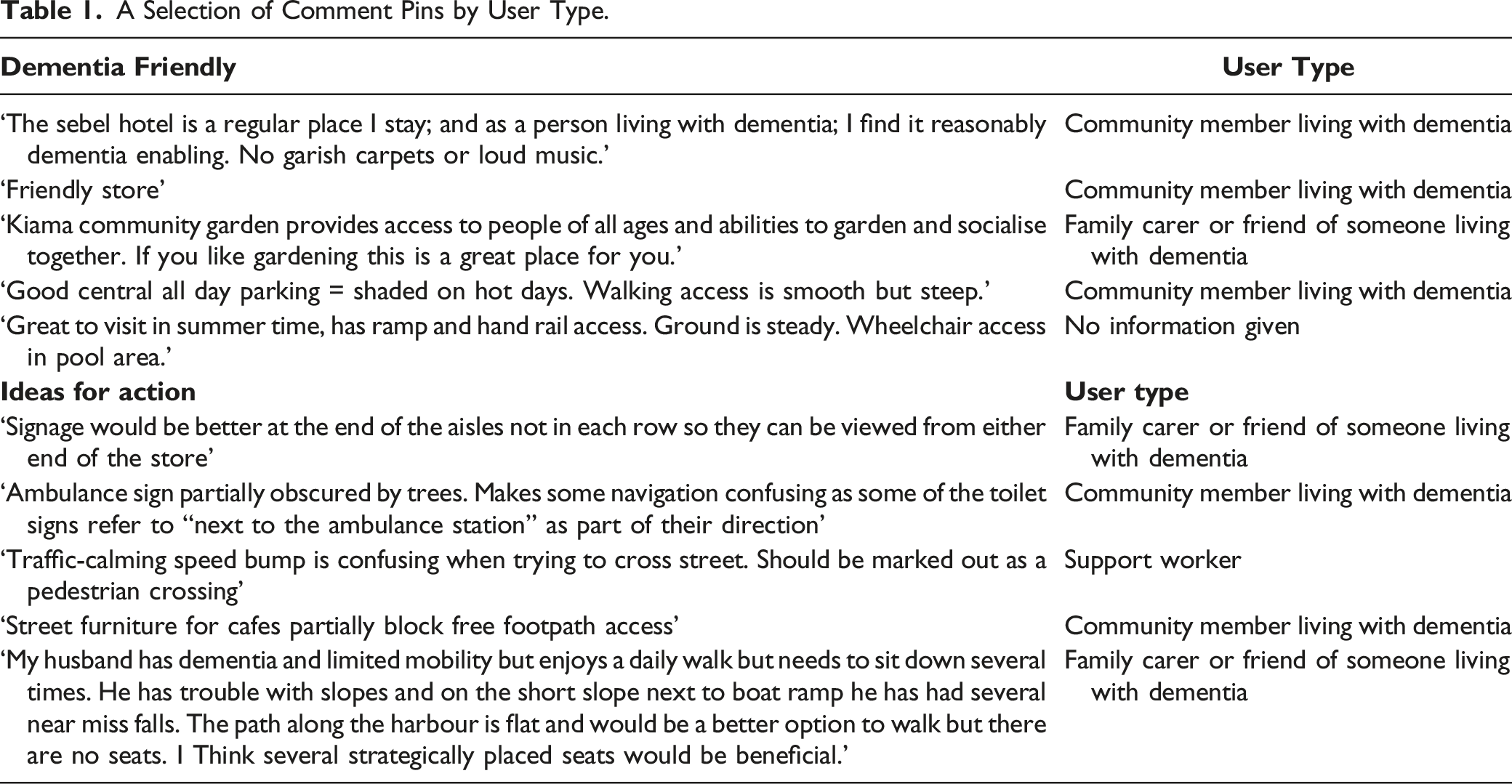
Of all the pins, just over one third (37%) contained ‘Ideas for action’, with most of these contributed to the map directly by people living with dementia. The majority promoted ideas for improvements to footpaths, kerbsides, pedestrian crossings, improved signage, car parking, and public toilets. While the general focus of these issues may have been expected and lined up with what we already knew from the sketch mapping interviews, what was not anticipated was that being able to identify specific places for action empowered the members of the Kiama Dementia Alliance. As part of the Kiama Dementia Alliance regular monthly meetings, postings from the Our Place Kiama web map were reviewed. This map aided the transformation from a general discussion about ‘how to make Kiama more dementia friendly’ to discussions that were grounded in accountabilities and support for making the places that had been pinned better. Rather than face the impossible task of ‘improving all environments’, council officials were instead enabled to raise specific and manageable work orders with the relevant departments to fix specific instances of, for example, signage for public toilets, kerb repairs and extra seating along certain footpaths. The web map grounded participants’ pins and comments in tangible elements of the built environment that caused issue, while simultaneously acting as a conduit, communicating the lived experience of people with dementia to decision makers.
Discussion
Previous research suggests that people with dementia may struggle with map-reading (Mitchell & Burton, 2010) and so the use of maps within qualitative place-based research has been minimal. However, our findings highlight that the use of dedicated scaffolds can support people with dementia to participate meaningfully in both sketch mapping of their neighbourhood engagement as well as crowdsourced mapping of dementia friendly places and spaces.
Research Scaffolding for Sketch Mapping
Scaffolds for Engaged Sketch Mapping with People with Dementia.

Narrative and relational scaffolding by both the care partner and the researcher were also important to populate the sketch maps which were ultimately a co-produced artefact representing neighbourhood engagement and stories. The role of the researcher and the degree to which assistance should be rendered when conducting sketch map interviews remains unresolved (Curtis, 2016). In our study, we quickly realised that while sketch mapping was achievable for those with less advanced dementia symptoms, getting this method to ‘fit’ for others meant enacting social supports either from researchers, or more often, allies working alongside them. Allies involved in our dyads were keenly aware of the collective impacts dementia has on their daily lives and might be able to better grapple with drawing on a map more effectively. There is a growing awareness of the benefits of the perspective of the dyad (the person with dementia with their care partner) in dementia research, as well as in the benefits of dyadic therapeutic interventions (Orsulic-Jeras, Whitlatch et al., 2020). We likewise emphasise that sketch mapping in our study benefitted from being treated as co-produced, due to the inclusivity that emerged from those social supports and prompts offered by care partners within interviews.
Research Scaffolding for Crowdsourced Mapping
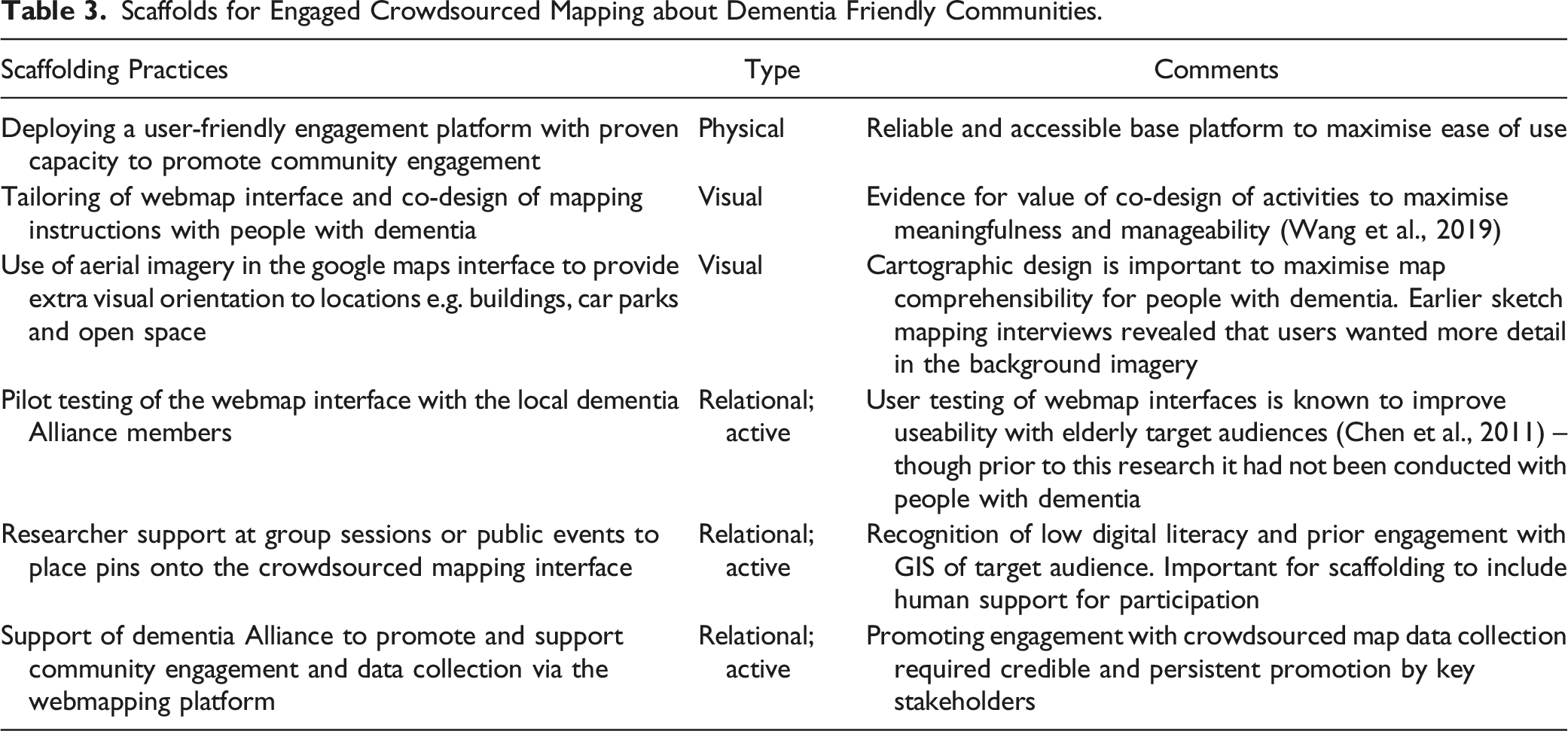
Scaffolds for Engaged Crowdsourced Mapping about Dementia Friendly Communities.
The Value of Qualitative GIS to Place-Based Research about Life with Dementia
Whilst go-alongs and walk-arounds are being increasingly promoted as useful in place-based dementia research (e.g. Odzakovic et al., 2020), our experience highlights that with dedicated scaffolding, sketch mapping interviews also have utility to uncover collective and otherwise hidden geographies of dementia. For example, when simple questions about travel and accessibility were explored through the prism of a printed map, they helped us to see and understand how each participant maintained an activity space, in spite of and in reaction to particular pinch points or spaces of difficulty. When combined across interviews, the data came alive even further, demonstrating and providing visual evidence of the ongoing civic participation of people with dementia. When responses were overlaid one on top of the other in the GIS, the resulting visualisation clearly demonstrated a collective footprint of people with dementia as citizens with agency in civic spaces.
We contend that putting their data ‘on the map’ visually intervenes in the politics of social inclusion for people with dementia by pointing to a worldview where they are still present in the material shared spaces (shops, parks, streets and so on) of community life. The sketch map results can thus be read as performative acts, documenting and presenting a collective spatial achievement that directly counters ‘shrinking world’ narratives (Duggan et al., 2008). These spatial results are a further line of evidence for arguments about the need for urban planning to hear the voice of people with dementia and contend with their specific needs so they can continue as active participants in those spaces (Mitchell & Burton, 2010). Like other social groups, people with dementia should have a voice in those debates.
Importantly, the distributed crowdsource map gave people living with dementia and their allies a tool which supported their communication about how their local public spaces should be planned or adjusted to support their participation. While producing less complex or rich spatial information than the sketch maps (which tended to show how and where people living with dementia engaged), the crowdsourced map produced a more actionable dataset based upon the outcomes of their spatial engagement. Maintaining the ability to move beyond home and interact socially with others in community settings is central to social health (Dröes et al., 2017). In this way, our crowdsourced map provided exact locations where problematic features could be addressed to make them more manageable and accessible. Crowdsourced map data thus supported advocacy by people living with dementia and their engagements with the public realm, offering new possibilities for dialogue between our research participants, and the decision makers and managers of the urban environment, and supporting their capacity to take their place with other groups who have engaged in neighbourhood activism through local campaigns and attempts at empowerment (Horak & Blokland, 2012).
Whilst overall engagement with the crowdsourced map was not particularly high, there were many positives to this method. First, this was not just a passive data collection tool. The interactive and public nature of an online crowdsourced map provided numerous opportunities for ongoing engagement, including responding and rating other posts, and if accessed via a mobile device, interacting with that information in real time and in situ. In much the same way that recommendation websites like TripAdvisor draw attention to favoured places, attention can be drawn via a location-based interface toward other proximate dementia friendly facilities as well as point out potential hazards along the way. In this way, the Our Place crowdsourced map also promoted access to essential ‘communication and information’ for local people with dementia, which has been highlighted as a central domain to address in the creation of aged and dementia friendly cities (WHO, 2007). Finally, people living with dementia were able to contribute spatial and qualitative data to a crowdsourced interface in their own time, outside of the performative and potentially stressful confines of the interview setting. The capacity of the crowdsourced map to promote ongoing, flexible interaction and opportunities for engagement in a public conversation highlights yet another potential benefit of online technologies in dementia care and healthy aging (Shu & Woo, 2021).
Overall, it was our general experience that sketch mapping acted as a ‘provocation to imagination’, generating place-based conversations which might have not otherwise materialised if we pursued only a question-and-answer discussion. To this end, Cartesian maps of a participant’s general activity space should be considered for inclusion in the interviewer’s toolkit, much like other participatory visual methods that focus on inclusion and flexibility (Phillipson & Hammond, 2018; Cridland et al., 2016). In the context where maps are perhaps not so useful for the participant living with dementia, our experience attests to the fact that engaging support through the dyad can assist in collecting what may turn out to be politically important data. Spatial data, either that collected by sketching or dropping a pin, has been shown in this research to potentially play an important advocacy role, supporting their continued engagement and free movement in public space.
To conclude, we return to Stea et al.’s (1996) proposition that mapping is a shared cultural universal: a communicative language that humans use to tell stories about places. These devices can also bring communities together, to think collectively and plan for the shared spaces they all inhabit (Young & Gilmore, 2013). If people living with dementia are excluded from mapping – from engaging in that continuing storytelling practice – then we may inadvertently bypass their involvement and continue to sideline their voices and perspectives from future spatial planning. Actively scaffolding people with dementia into qualitative mapping practices is not only productive for understanding their lived experience of traversing and being in community spaces, but also a constructive medium to advocate for meaningful change.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Australian Research Council [DE130101436]; UOW Global Challenges Program; Dementia Australia Research Foundation [DGP14-84].