
Abstract
Oklahoma has a high rate of chronic disease in comparison to other states in the U.S., currently ranking among the top five worst states for heart disease, chronic lower respiratory disease, cancer, diabetes, and maternal mortality. The purpose of this study was to evaluate the lifestyle medicine (LM) program at a local hospital system in Tulsa, Oklahoma, a health system that serves a patient population with notable health disparities. This mixed-methods evaluation assessed patient data from a representative sample of 63 patients across six distinct cohorts. Quantitative data included pre/post biometric data and pre/post-self-efficacy assessment. SPSS (V29) was used to analyze all quantitative data via descriptive statistics and paired t-tests. Qualitative data were gathered via interviews and focus groups; all interviews were audio-recorded and transcribed verbatim. MAXQDA was used to analyze qualitative data. Results reveal significant weight loss and significant increases in knowledge, self-efficacy, and health behavior change among patients. The findings of this study support the recommendation that Oklahomans should have increased access to LM interventions in hopes of experiencing significant shifts in improved health outcomes and reduced chronic disease risk factors for individuals and at the community level when such interventions are implemented at scale.
“Significant improvements were observed in patient-reported knowledge, attitudes, self-efficacy, and purpose in life through the use of the SHLA pre- and post-program.”
Background
Lifestyle Medicine (LM) is a rapidly growing field in the healthcare and public health sectors. 1 Aiming to prevent, treat, and even reverse chronic disease, the American College of Lifestyle Medicine (ACLM) takes an evidence-based approach to health and behavior modification for healthcare providers, patients, and communities. 2 In order to mitigate many chronic diseases such as obesity, cardiovascular disease, type 2 diabetes, chronic kidney disease, some forms of cancer, and other non-communicable diseases, many clinicians, hospital systems, and community programs have begun to take an upstream approach by implementing LM education and clinical care. 3 Focusing on the six pillars of ACLM (sleep, nutrition, physical activity, stress management, social connection, and avoidance of risky substances), many LM programs are seeing improved patient outcomes from a healthcare and public health perspective. 4
In alignment with these aforementioned efforts, the Saint Francis Health System (SFHS) in Tulsa, Oklahoma, has recently created and implemented a LM clinic and 8-week intervention program. 5 As one of the three states with the highest prevalence of obesity and ranking as the worst state for cardiac mortality, Oklahoma is in dire need of a program such as this. 6 Pioneered by Dr Ajay Joseph, a preventive cardiologist, this LM program is the first of its kind across the entire SFHS. 5 Beginning with a pilot program, expanding the program to SFHS employees, and recently opening the program to SFHS patients, an evaluation of this program is timely. Understanding the overall outcomes and impacts of this program will aid in the improvement and expansion of the SFHS LM program for the greater Tulsa community. 7
A thorough program evaluation can provide informative insights into the overall reach and impact of these unique factors associated with this particular program. It is ideal to have an informed understanding of how this program is affecting the health and well-being of program patients in the greater Tulsa, Oklahoma, area. Identifying beneficial features of this program will allow for improvement of the existing LM program, replication across SFHS and throughout other healthcare systems, and determining how programs such as this can combat challenges associated with health disparities and health inequities.
Oklahoma has a high rate of chronic disease in comparison to other states in the U.S., currently ranking among the top five worst states for heart disease, chronic lower respiratory disease, cancer, diabetes, and maternal mortality, all conditions that are significantly affected by lifestyle and health behavior factors. 6 The current body of knowledge reveals that LM and preventive care efforts are lacking and often inaccessible in areas where health disparities and inequities prevail. 2 As the largest hospital in Oklahoma, Saint Francis Health System is playing a critical role in increasing access to LM healthcare and improving health outcomes in a state that is riddled with obesity, chronic diseases, and associated poor health conditions. 6 The SFHS LM program is actively addressing health disparities and chronic disease conditions in Tulsa, Oklahoma by providing LM education, clinical care, cooking classes, and mindfulness sessions to patients with a past history and/or current diagnosis of obesity and other chronic diseases such as cardiovascular disease, diabetes, and fatty liver disease, among others. 5 Gaps in the current literature highlight important factors related to LM, such as self-efficacy, purpose in life, and barriers to LM behavior change, have not been well-researched or evaluated in relation to LM interventions and their overall effectiveness. Further exploring how LM program patient self-efficacy and sense of purpose in life influence patient health outcomes and adoption of LM behavior change will further inform the development, objectives, and implementation of LM interventions. 8 Additionally, learning more about LM program patients perceived barriers and perceived benefits associated with health behavior change is paramount to the overall improvement, outcomes, and expansion of LM interventions.
Purpose of the Study
The purpose of this study was to evaluate the LM program at a local hospital system in Tulsa, Oklahoma, to determine the program’s effectiveness in reducing chronic disease conditions, understand correlations associated with patient attitudes, knowledge, self-efficacy, purpose in life, and lifestyle behavior, and explore how perceived benefits and perceived barriers are influencing patient lifestyle behavior change.
Research Questions
(1) Is this new lifestyle medicine intervention program effectively reducing chronic disease risk factors among program patients? (2) What are the associations of this lifestyle medicine intervention program with patient attitudes, knowledge, self-efficacy, purpose in life, and lifestyle behaviors? (3) How do perceived benefits and perceived barriers influence the likelihood of lifestyle behavior change for program patients?
Existing Lifestyle Medicine Program Outcomes
There are many LM programs similar to the SFHS LM program intervention that have been implemented over the past decade. One article highlights the optimal dosage of intensive LM programs such as the Complete Health Improvement Program (CHIP), noting that the CHIP program is effective when provided in 8- and 16-sessions over a 4-week time period, ultimately stating that cutting the number of sessions in half could be equally as effective. 9 Another LM program serving low-income and uninsured patients in a safety-net healthcare setting can significantly improve patient-reported outcomes related to physical activity, adopting a plant-based diet, and other factors associated with the pillars of LM. 10 Furthermore, exploring provider perspectives and interprofessional efforts related to such LM interventions also provides valuable insights into the overall feasibility and effectiveness of such programs in a healthcare setting. Cheng, et al, (2024) note that healthcare providers significantly value interprofessional teams as a part of intensive LM programs, highlighting that successful interprofessional teams require “investment from all levels within a healthcare system.” 11
Oklahoma Health Disparities and Inequities
The state of Oklahoma continues to experience inordinately high rates of chronic disease, poor health outcomes, and uninsured patient populations. In comparison to other states in the U.S., the state of Oklahoma currently ranks as follows for the respective leading causes of death: first for heart disease, second for chronic lower respiratory disease, fourth for cancer and diabetes, and Oklahoma consistently ranks among the U.S. states with the highest rates of maternal mortality.6,12 The current body of knowledge informs us that LM and preventive care efforts are lacking and often inaccessible in areas where health disparities and inequities prevail. 2
As chronic disease conditions continue to persist and even worsen, implementing LM intervention programs at scale may be a valuable way to reduce healthcare costs, modify patient behavior, and ultimately reduce rates of chronic disease at the local, state, and even national levels over the long term. 13 Focusing on existing gaps related to patient self-efficacy, perceived benefits and barriers, having a sense of purpose in life, and systemic barriers to change will further inform the existing body of knowledge. Adding to the current literature may allow for the replication and expansion of more effective LM intervention programs, further support patients and healthcare providers in their lifestyle behavior change efforts, and ultimately advance the field of LM for the betterment of our nation’s health and the overall reduction of chronic disease.13,14
Methods
Theoretical Framework
This evaluation used the Centers for Disease Control and Prevention (CDC) Framework for Program Evaluation in Public Health as a guiding framework for the entire project.
15
The CDC Framework for Program Evaluation in Public Health consists of the following six steps: (a) describe the program; (b) focus the evaluation design; (c) gather credible evidence; (d) justify conclusions; (e) ensure use and share lessons; and (f) engage stakeholders.
16
The standards of this CDC evaluation framework are utility, feasibility, propriety, and accuracy.
16
Figure 1 provides a visual representation of the steps and standards of the CDC Framework for Program Evaluation in Public Health. CDC program evaluation framework.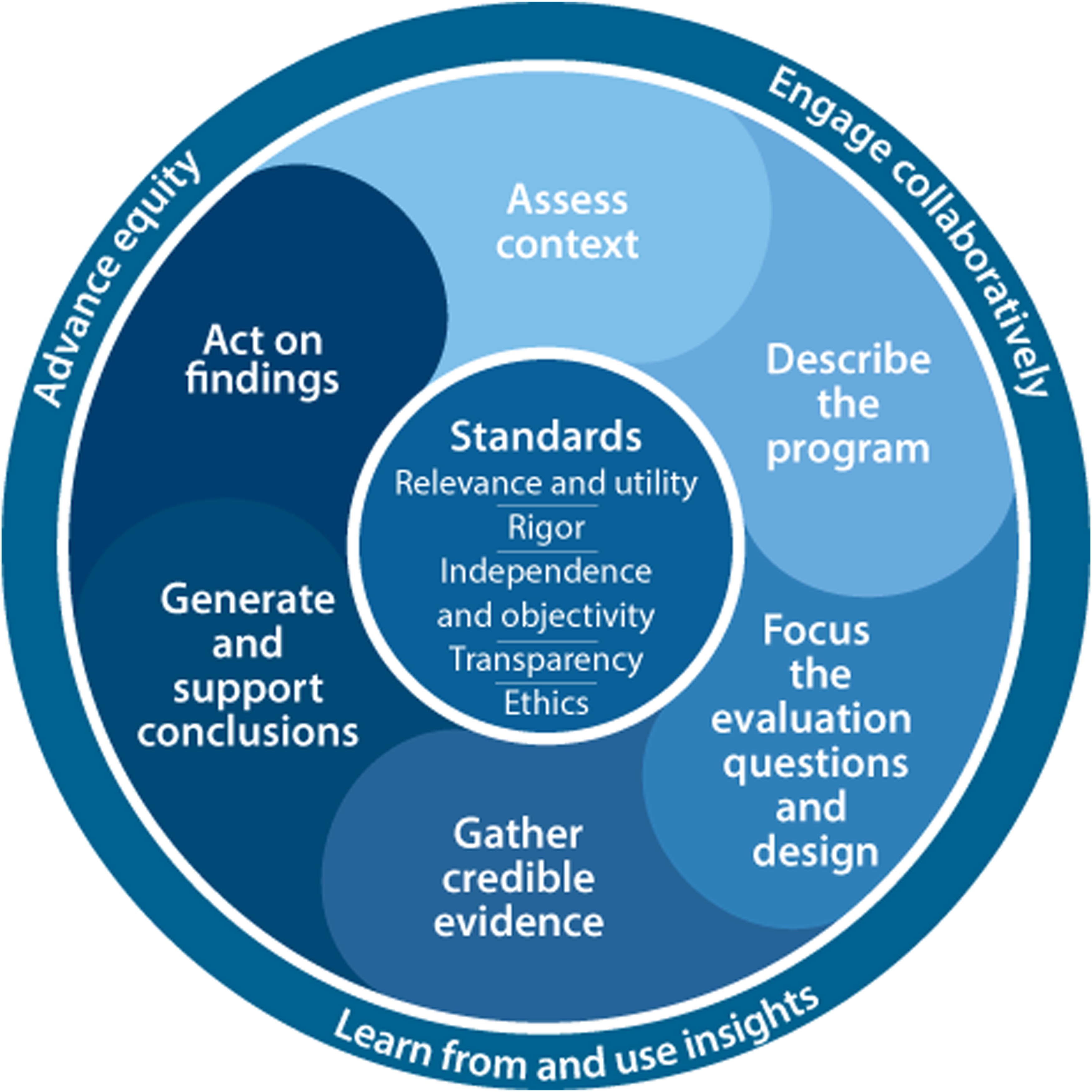
This program evaluation project was guided by the health belief model (HBM). The HBM is a theoretical framework often used as a guide for health promotion and disease prevention programs. 17 The HBM serves as a model to understand health behaviors and predict changes that may occur in health behavior. Key components of the HBM include perceived susceptibility, severity, benefits, and barriers, along with cues to action and self-efficacy. 18 These core aspects of the HBM make this framework ideal for the observance and measurement of patient health behavior and self-efficacy changes for this LM intervention program.
The Health Belief Model and Lifestyle Behavior Change
The HBM is a founded theoretical model that explains and predicts health-related behaviors by focusing on the attitudes and beliefs of individuals. 17 It is particularly useful in research studies such as this one that aim to better understand health behavior changes among patients, especially those dealing with chronic diseases. The constructs of the HBM help in understanding why some people take action to prevent or treat illness while others do not. 18 For the purpose of this study, the HBM constructs of perceived benefits and perceived barriers were the focal point.
Perceived Benefits
In the context of chronic disease prevention, treatment, and reversal, the perceived benefits refer to an individual’s assessment of the value or efficacy of engaging in a health-promoting behavior to decrease the risk of disease. 18 A research study on LM intervention, for example, might use the HBM to evaluate how perceptions of benefits affect a patient’s willingness to adopt a healthier lifestyle. Patients who recognize that changes in diet, exercise, and stress management can significantly reduce symptoms or progression of conditions like diabetes, heart disease, or hypertension are more likely to engage in these behaviors.
Perceived Barriers
Conversely, perceived barriers are the costs or obstacles that are viewed as outweighing the benefits of engaging in the behavior. 18 In chronic disease management, these barriers can be tangible, such as the cost of healthy foods or the lack of access to safe exercise environments, or psychological, such as the fear of injury or the belief that one’s disease is too far advanced to benefit from changes. Effective research into LM must, therefore, address these barriers directly. This can be achieved through designing interventions that not only educate patients about the manageable nature of these barriers, but also provide practical solutions, such as tailored exercise programs that are mindful of physical limitations or budget-friendly diet plans. 19 Understanding these perceived barriers allows researchers and healthcare providers to develop more targeted interventions that are better suited to the real-life contexts of patients’ lives, increasing the effectiveness of lifestyle interventions in chronic disease management. 20
In summary, the HBM serves as a robust framework in research studies focusing on health behavior change. By elucidating the role of perceived benefits and barriers, the HBM helps in designing, implementing, and evaluating interventions that are more likely to be effective in promoting healthy behaviors among patients with chronic diseases. This dual focus not only enhances the understanding of patient motivations and resistances but also guides the creation of supportive environments that facilitate the adoption and maintenance of health-enhancing behaviors, ultimately contributing to the prevention, treatment, and reversal of chronic diseases. 21
Program Intervention
SFHS is the leading healthcare system in Eastern Oklahoma. A new LM program was established and piloted through SFHS in 2023. 5 This LM program aims to prevent, treat, and reverse chronic disease conditions for SFHS patients through the six pillars of LM 4 as outlined by the ACLM. These six pillars include: (1) A whole foods plant-based diet; (2) Physical activity; (3) Sleep hygiene; (4) Avoidance of risky substances; (5) Positive social connections; and (6) Stress management.
This SFHS program focused on these six LM pillars over the duration of an 8-week cohort-style program with 10-12 patients per cohort. The SFHS LM healthcare team includes a preventive cardiologist, a registered nurse and health coach, a licensed therapist, a registered dietitian, a licensed chef, and a certified physical trainer. All patients developed specific, measurable, achievable, relevant, and time-bound (SMART) goals at the beginning of the 8-week program. Patients met in person at the SFHS Health Zone on a bi-weekly basis for a 3-hour in-person class session for a total of five sessions. At the beginning of each session, patient biometrics (height, weight, blood pressure, and heart rate) were measured and recorded. Patients then gathered as a group for a chef-led interactive whole food plant-based cooking session. During the cooking session, each patient individually met with the preventive cardiologist for 1:1 SMART goal check-ins. The culinary session was followed by a health education lecture and Q&A focused on the topics of cardiovascular disease, stroke, dementia, cancer, hypertension, diabetes, obesity, fatty liver disease, and gastrointestinal disorders. Each module was then closed out with a therapist-led group mindfulness exercise.
Program Duration & Pedagogical Approaches
The in-person LM program sessions took place every other week throughout the 8-week timeframe. All 5 sessions were approximately 2 ½ h long, including the following components: • Check-in, vitals, and biometrics (5-10 min) • Chef-led interactive, hands-on cooking session (60 min) • 1:1 doctor/patient SMART goal checking (5-10 min) • Health education lecture presentation with Q&A discussion (30-40 min) • Therapist-led group mindfulness session (20-30 min)
All program participants had access and were able to schedule consultations with the SFHS LM program staff for the duration of the program, which includes an LM-certified preventive cardiologist, a registered dietitian, a certified chef, a licensed therapist, a health coach, and a licensed personal trainer. Additional resources are provided to LM program participants, including, but not limited to: • A Full Plate Living Account • American Heart Association resources • Books, podcasts, and other free resources related to chronic disease and lifestyle medicine interventions.
Upon completion of the 8-week LM program, participants received follow-up LM care via the SFHS LM clinic. Depending on each participant’s individual needs and diagnoses, follow-up appointments are scheduled for 3- to 6-month post-LM program completion.
Program Goals & Objectives
(1) Increase awareness of LM interventions as an evidence-based approach to chronic disease prevention, reversal, and treatment throughout the SFHS. (a) Objective 1: Promote the SFHS LM clinic and program to SFHS personnel via Grand Rounds presentations at least twice per year. (b) Objective 2: Inform the general public within the greater Tulsa area of the SFHS LM clinic and program via local digital media and printed handouts across SFHS hospital and clinic locations. (2) Increase access to LM-certified healthcare providers and LM interventions for the Tulsa, Oklahoma community. (a) Objective 1: Increase the number of LM-certified healthcare providers in the SFHS LM clinic and program from 1 physician to at least 3 providers by January 2025. (b) Objective 2: Increase capacity for patients within the LM clinic by expanding LM clinic operations from 1 day per week to 3+ days per week by January 2025. (c) Objective 3: Increase capacity for patients within the LM program by expanding the number of LM program cohorts from 3 per year to 5+ per year by January 2025. (3) Empower patients to take control of their health and chronic disease conditions through the six LM pillars of the ACLM: plant-predominant diet, physical activity, stress management, sleep hygiene, positive social connection, and avoidance of risky substances for the purpose of chronic disease prevention, treatment, and reversal. (a) Objective 1: Increase patients’ sense of purpose to inspire optimistic adoption of LM practices. (b) Objective 2: Increase patients’ knowledge of mindfulness practices and self-efficacy to incorporate mindfulness into daily life. (4) Increase patient knowledge regarding chronic disease conditions and effective lifestyle medicine interventions to prevent, treat, and reverse chronic disease. (a) Objective 1: Distribute free resources to increase patient knowledge of how lifestyle behaviors influence chronic disease conditions. (b) Objective 2: Conduct 5 interactive sessions for patients to learn about chronic diseases and lifestyle behaviors that treat, prevent, and reverse these diseases through interactive lectures and Q&A-style sessions. (5) Increase patient self-efficacy specific to LM interventions and practices to increase long-term adoption and implementation of health behavior change. (a) Objective 1: Demonstrate examples of LM health behaviors with patients during each in-person module and share free practical resources that support day-to-day implementation of LM habits to increase participant confidence and self-efficacy (i.e., interactive cooking demonstrations, mindfulness practices, SMART Goals etc.). (b) Objective 2: Increase knowledge and awareness of self-compassion and support groups to LM participants to help them be kind to themselves if/when they do not uphold new LM health behaviors and have the resources to re-implement healthy habits and actions.
Session Topics
Session 1: Cardiovascular Disease Session 2: Strokes & Dementia Session 3: Cancers Session 4: Hypertension, Diabetes & Obesity Session 5: Fatty Liver & Gastrointestinal Health
Program Evaluation Overview
This program evaluation involves process and impact evaluation methods. A program evaluation planning period was conducted for the Saint Francis Health System (SFHS) Lifestyle Medicine (LM) program in 2023, and a formal program evaluation began in January 2024. This evaluation further informs the process of this LM program, the impact the program is having on patients, and aims to prepare for an outcome evaluation after the program has been in operation for 18 months. Program processes and impact data from January 2024 to December 2024 were evaluated, and the pilot program was excluded from the SFHS LM program evaluation.
For the process evaluation, data collection focused on program implementation, patient engagement, and participant satisfaction. Process data sources included patient feedback surveys administered at the conclusion of each program cohort and patient feedback provided via interviews and focus groups. In addition to numerical satisfaction ratings, the surveys included open-ended questions that provided suggestions for program improvement. Feedback surveys were distributed and analyzed using SurveyMonkey (Momentive SurveyMonkey Platform, San Mateo, CA), and all responses were anonymous.
Impact evaluation components included patient knowledge, self-efficacy, purpose in life, and behaviors related to the six pillars of LM (sleep, nutrition, physical activity, stress management, social connection, and avoidance of risky substances), changes in biometric data and lab values, and shifts in lifestyle health behaviors and self-efficacy. Ensuring that this LM program is meeting its intended goals, objectives, outputs, and outcomes will aid in the growth, expansion, and overall reach of the program now and in the future.
All quantitative data have been captured through existing SFHS LM program processes involving the Epic electronic health record (EHR) system and served as one source of data for the first phase of this program evaluation. The St. Francis Health System Institutional Research Ethics Board (IREB) has determined that this project does not qualify as human subjects research as defined in 45 CFR 46.102(d) and (f) and is not subject to further oversight by the SFHS IREB, as noted in the determination letter for IREB #2368-24. Existing data collection methods included patient intake forms, biometric data measurement (weight, body mass index, blood pressure, hemoglobin (HbA1c), blood glucose, and total cholesterol), and self-report survey responses from pre- and post-LM programs.
Analysis of lab results includes pre- and post-program lab measures for as many patients as possible. Due to existing processes of the SFHS LM clinic and 8-week program, patient lab tests were ordered and received by primary care providers (PCPs), not the SFHS LM clinic healthcare providers. These existing processes resulted in limited availability of patient biometric data and lab results. All relevant patient data were exported from Epic or collected via paper surveys and de-identified prior to analysis. In order to conduct a thorough analysis of all quantitative data, SPSS software (IBM SPSS, Inc., Version 29, Armonk, NY) was used to analyze all data from the patient intake forms, biometric measurements, and the pre/post-assessment survey. 22
Data for the second phase of the evaluation were obtained through key informant interviews (KIIs) and focus groups conducted by the external program evaluator. Eight KIIs were conducted in November 2024 until saturation 23 was met; five patients and three staff members were interviewed. All KIIs were conducted online via Zoom. Three focus groups were offered in December 2024 until saturation was met; 1 in-person focus group for cohorts 3 and 4 (n = 8), 1 in-person focus group for cohorts 5 and 6 (n = 6), and 1 online focus group for cohorts 5 and 6 (n = 5). A focus group was offered for cohorts 1 and 2, but only one patient expressed interest in participating. All focus group patients were recruited via convenience sampling. KIIs and focus groups were audio-recorded and transcribed verbatim using MAXQDA version 24. 24 All data remain confidential, and all program patients signed consent forms. MAXQDA was used to conduct a thorough analysis of all KIIs and focus groups to determine thematic codes across all qualitative data.
Program Evaluation Planning Stage
During the pilot phase of the SFHS LM program, a dedicated evaluation planning period was initiated. This early planning stage identified the need for improved processes to include pre- and post-program assessments rather than relying on post-program feedback alone. Establishing baseline measures was deemed critical for accurately detecting changes attributable to the intervention. The program evaluator also emphasized the importance of the consistency of evaluation instruments to be used in all SFHS LM program processes. Though different pre- and post-program survey tools were initially used, limiting the direct comparisons of program outcomes, LM program processes were updated to include the same tool for pre-program assessment as the tool used for post-program assessment. As a result, the protocol was refined so that the SHLA was administered at both the beginning and end of the program for all subsequent cohorts, ensuring comparability of pre- vs post-program data.
Additionally, the program evaluator recommended integrating module-specific evaluations and biometric tracking to monitor progress in greater detail. Brief feedback surveys were designed for each core module (e.g., nutrition, exercise, stress management) to capture immediate participant feedback on those sessions; however, this recommendation was not implemented for the 2024 LM cohorts due to limitations with time and personnel. The planning period also highlighted the importance of digitizing data collection (in place of paper surveys) to streamline analysis and improve data quality. Though these recommendations were not implemented in time for the 2024 LM cohorts, the program has since transitioned from paper to electronic surveys, making it easier to aggregate and review results in real-time. The recommendations have also led the SFHS LM team to explore and begin the process for the future integration of a mobile health platform to facilitate real-time data capture and enhance participant engagement.
Patient Demographics and Sampling
All LM patients were residents of the greater Tulsa, Oklahoma area who were current patients of the SFHS LM Clinic. In order to participate in the SFHS LM program, individuals must have had a history or current diagnosis of at least one of the following conditions: obesity, fatty liver disease, high blood pressure, stroke, coronary disease, high cholesterol, diabetes, or heart disease. 5
LM a Program Patient Population Demographics (N = 63).
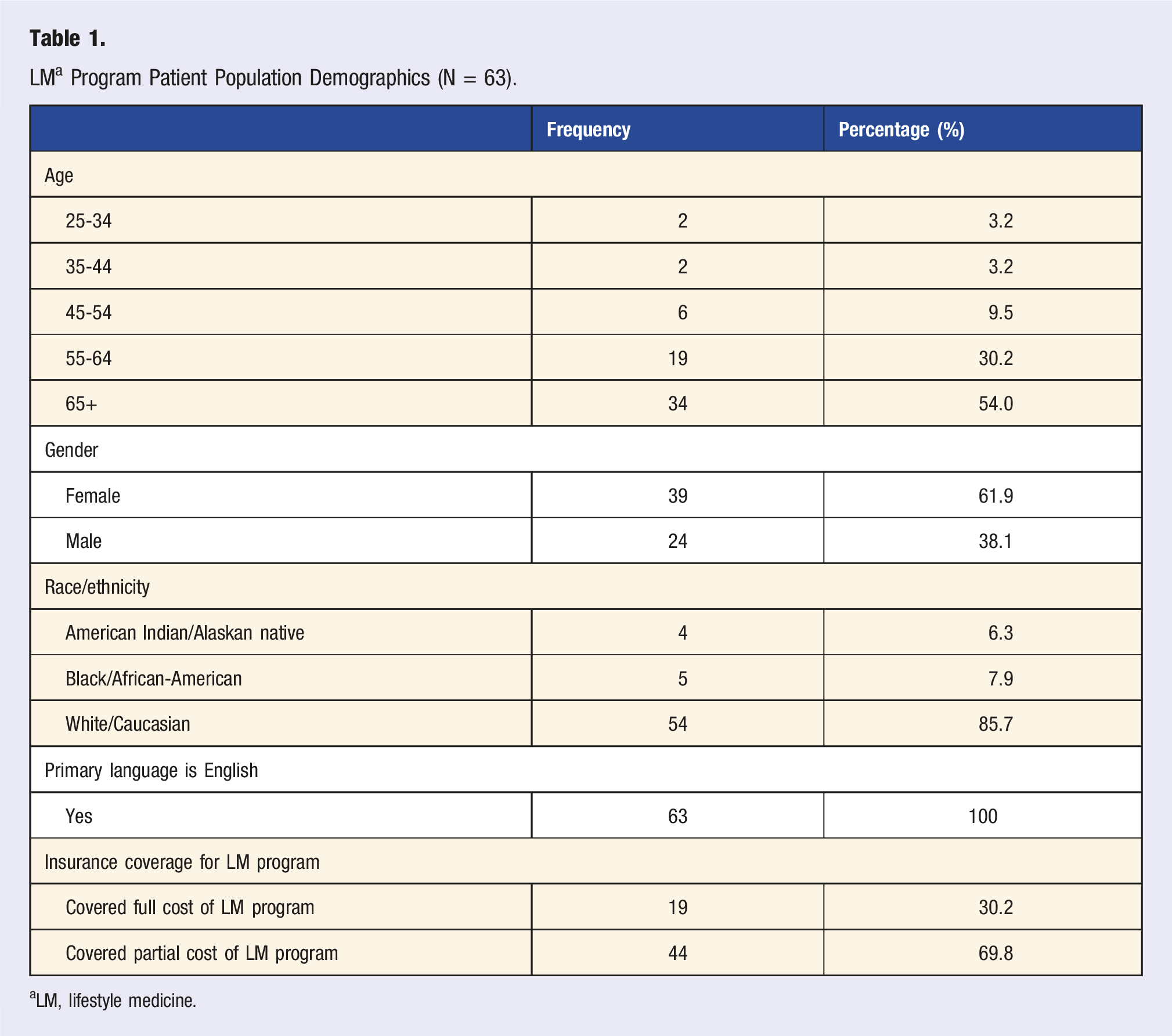
aLM, lifestyle medicine.
Demographics for Patient Interviews (N = 5) & Focus Groups (N = 17).
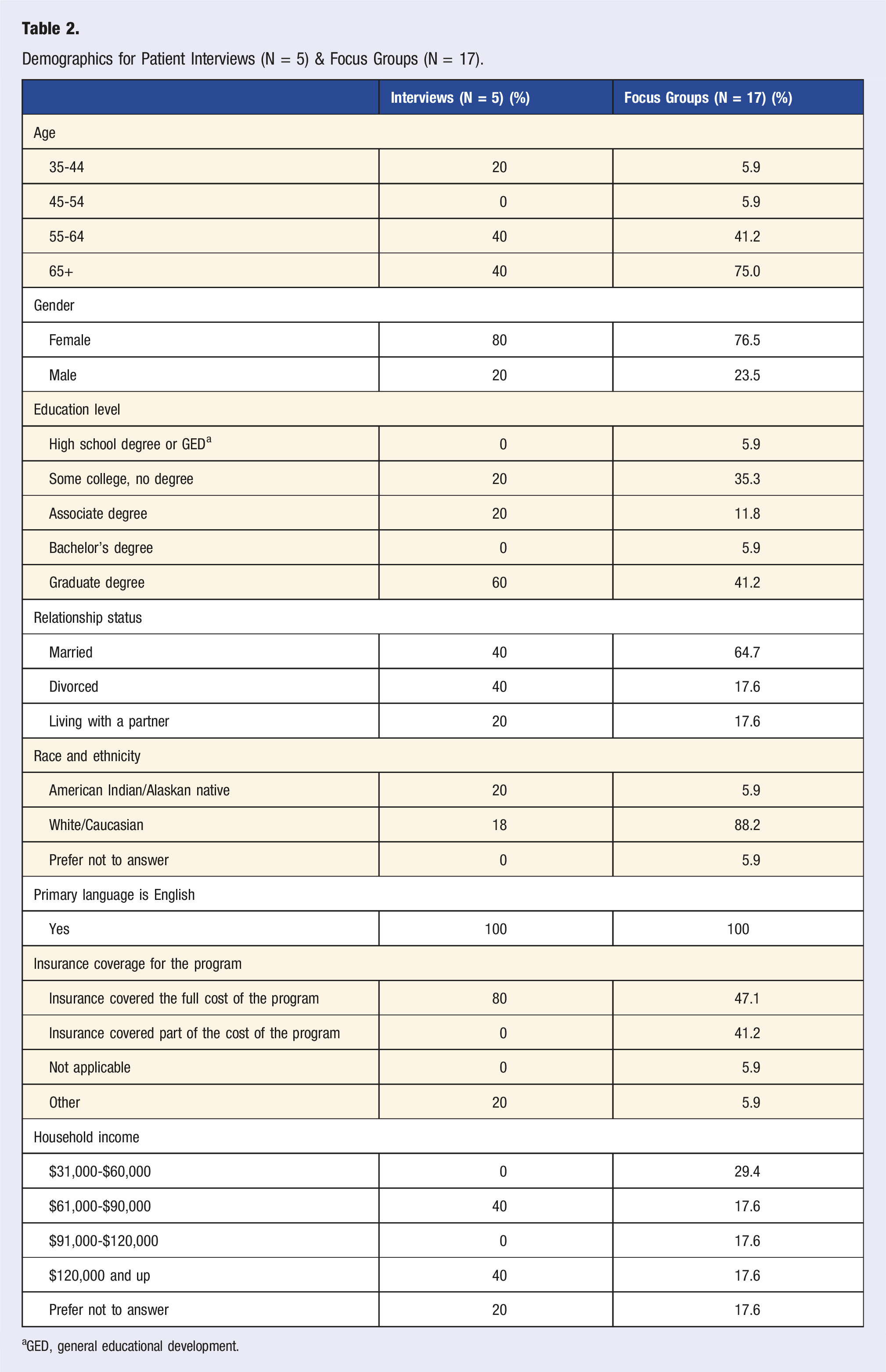
aGED, general educational development.
Procedures
LM program patients were informed of the SFHS LM 8-week intervention program through the SFHS LM clinic. Patients of the SFHS LM clinic were provided the opportunity to participate in the more intensive LM program if interested. All quantitative data for each LM patient were captured and stored through the SFHS Epic EHR system; these quantitative data were de-identified before provided to the external program evaluator. All quantitative data served as a source of secondary data for this program evaluation.
Qualitative data were gathered via KIIs and focus groups and served as a primary data source for the use of this program evaluation to further explore SFHS LM patients’ perceived benefits and perceived barriers related to their personal experiences associated with lifestyle behavior change. All KIIs and focus groups were conducted by the external program evaluator. KII question and focus group question guides and scripts were created by the external program evaluator and reviewed and approved by the primary investigator of this study, a program and process evaluation expert. MAXQDA version 24 was used to transcribe all audio recordings and conduct thematic analysis and content analysis via an inductive coding approach. 24 The convenience sampling technique was used to notify LM patients of the key informant interviews and focus groups. All qualitative data were audio-recorded and transcribed verbatim using MAXQDA version 24. After transcription of the interviews and focus groups, MAXQDA was used to conduct a thematic analysis of all qualitative data to formulate codes and identify recurring themes.
Lifestyle behavior change was measured by calculating the post-minus pre-difference of the lifestyle behavior index that was created over the course of the SFHS LM program intervention. The Simple Health Lifestyle Assessment tool (explained below) was used to measure patient pre- and post-LM program lifestyle behavior scores.
Instrumentation and Measurement
Only one quantitative assessment tool was initially intended to be used for this program evaluation; however, a second assessment tool was used only for the pre-program assessment of cohort 1 and 2 patients. The Simple Health Lifestyle Assessment (SHLA) created by Western Wisconsin Health (WWH) was used as a pre- and post-program assessment for cohorts 3, 4, 5, and 6. The SHLA was also used for the post-program assessment of cohorts 1 and 2, while the ACLM Lifestyle Assessment Short Form (LASF) was used for the pre-program assessment of cohorts 1 and 2. Both assessment tools can be viewed in Appendix A and B.
Simple Health Lifestyle Assessment (SHLA)
The SHLA was created by public health and LM experts at WWH in 2023. 8 Verma A, Mehta S, & Patyal A. Knowledge, attitude and practices toward health behavior and cardiovascular disease risk factors among the patients of metabolic syndrome in a teaching hospital in India. Journal of Family Medicine and Primary Care 2019;8(1):178-183. DOI: 10.4103/jfmpc.jfmpc_257_18. The SHLA was provided to patients at the beginning of Module 1 upon check-in at the SFHS Health Zone and at the end of Module 5 upon check-out at the SFHS Health Zone to measure patient pre- and post-LM program lifestyle behavior scores. This assessment tool has been created to specifically focus on the ACLM’s six pillars of LM and measures patient knowledge, attitudes, behaviors, self-efficacy, and purpose in life related to LM interventions and health behavior change. This 21-question 4-level Likert-type scale was founded on interpersonal discussion and self-efficacy in knowledge, attitude, and practice models presented by Chatterjee et al. 8 All 21 questions were measured on a scale ranging from one to four; strongly disagree (code = 1), somewhat disagree (code = 2), somewhat agree (code = 3), and strongly agree (code = 4). The SHLA was given to SFHS LM patients pre- and post-LM intervention to measure shifts in patient knowledge, attitudes, behaviors, self-efficacy, and purpose in life.
Data Analyses and Management
To analyze how effectively this new LM intervention program is reducing chronic disease risk factors among LM patients, secondary quantitative data that were captured through the SFHS LM program process were analyzed via SPSS. Descriptive statistics and paired t-tests were conducted to compare patient lab results and biometric data from pre- to post-LM intervention. All quantitative data served as secondary data for this program evaluation. All data were cleaned, sorted, and de-identified prior to inputting the data into Microsoft Excel and ultimately to an analytical SPSS save file. Descriptive statistics and paired t-tests were conducted to compare patient knowledge, attitudes, self-efficacy, purpose in life, and lifestyle behavior from pre- to post-LM intervention.
To determine the associations of this LM intervention program with patient attitudes, knowledge, self-efficacy, purpose in life, and lifestyle behavior, analyses of the pre- and post-program SHLA results were conducted. Cohorts 1 and 2 were analyzed separately from cohorts 3, 4, 5, and 6. The ACLM LASF was used as the pre-program assessment for cohorts 1 and 2, while the WWH SHLA was used for the post-program assessment of cohorts 1 and 2. The WWH SHLA was used for the pre- and post-program assessment of cohorts 3, 4, 5, and 6. Pre- and post-program SHLA results were analyzed for cohorts 3, 4, 5, and 6 to determine shifts in patient attitudes, knowledge, self-efficacy, and purpose in life related to lifestyle behavior change. A total of 46 pre-program SHLA forms were analyzed, and 36 post-program SHLA forms were analyzed for cohorts 3-6. A SHLA summary index score was created by summing responses to all 21 SHLA items for each participant response from cohorts 3-6. Each item used a 4-point Likert scale (1 = strongly disagree to 4 = strongly agree), with higher scores indicating more favorable lifestyle and coping behaviors. Summary index scores were calculated for all available pre-intervention responses (n = 46) and all available post-intervention responses (n = 36). Because the pre- and post-intervention samples differed in size and contained different participants, a Welch’s t-test was used to compare mean SHLA index scores across time points.
All KIIs and focus groups were conducted by the external program evaluator. KII question and focus group question guides and scripts were created by the external program evaluator and reviewed and approved by the primary investigator of this study, a program and process evaluation expert. All qualitative data were captured via audio recording and transcribed verbatim using MAXQDA version 24. 24 MAXQDA version 24 was used to transcribe all audio recordings and conduct thematic analysis and content analysis via an inductive coding approach.
As part of the process evaluation, a post-program patient feedback survey was administered to gauge participant satisfaction and gather suggestions. A total of 26 program participants responded to the survey, with an average overall satisfaction rating of 4.67 out of 5, indicating a very high level of approval. Qualitative comments from the survey highlighted what participants found most valuable about the program.
Ethical Considerations
This LM program evaluation adheres to ethical standards to protect the rights and well-being of all patients. Human subjects’ concerns are paramount. This evaluation has been designed to maximize benefits while minimizing risks. 15 Patients in the program can expect to gain significant health benefits through evidence-based lifestyle interventions, including improved physical and mental well-being. However, it is also acknowledged that there may be minimal risks, such as discomfort from dietary changes or increased physical activity. These risks were addressed by providing patients with comprehensive support throughout the program. 5 In order to protect all patients and adhere to research ethics and standards, Institutional Review Board (IRB) applications were approved through the Saint Francis Hospital System (IERB #2368-24) and Loma Linda University (IRB #5240374) for the purpose of this program evaluation.
To ensure the confidentiality of patient data, rigorous procedures were put in place. All personal information collected during the program were securely stored and accessible only to authorized personnel involved in the evaluation. Patient information was kept anonymous and de-identified during analysis to prevent the identification of any individual participating in the LM program. Additionally, informed consent was obtained from all patients, clearly outlining the purpose of the evaluation, the procedures involved, and their right to withdraw at any time without any negative consequences. By prioritizing these ethical considerations, the evaluation sought to uphold the highest standards of integrity and respect for patients’ rights and privacy.
Results
Quantitative Results
Reducing Chronic Disease Risk Factors
Pre- and Post-Program Biometric Values.
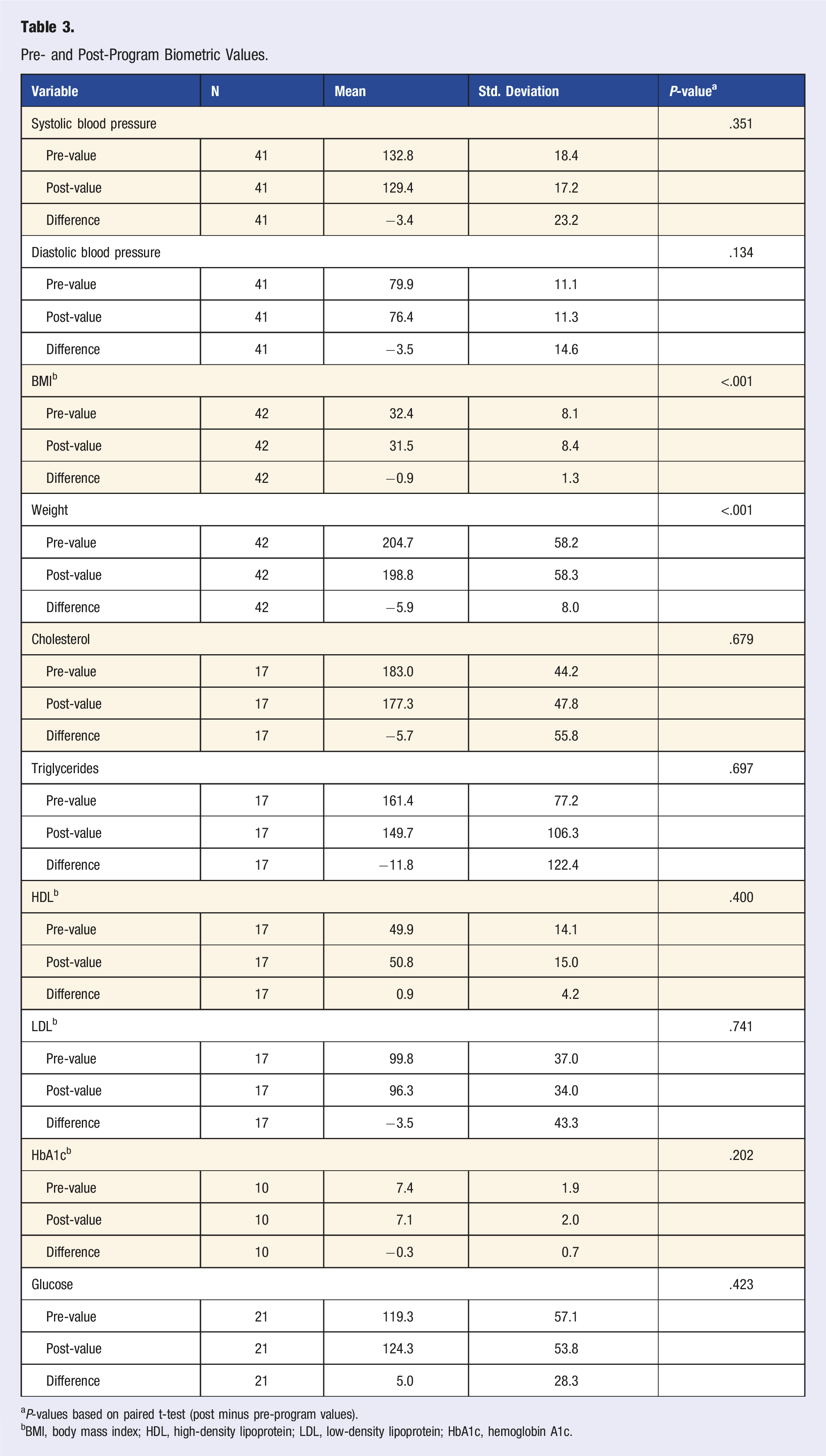
aP-values based on paired t-test (post minus pre-program values).
bBMI, body mass index; HDL, high-density lipoprotein; LDL, low-density lipoprotein; HbA1c, hemoglobin A1c.
Patient Attitudes, Knowledge, Self-Efficacy, Purpose in Life and Lifestyle Behavior Change
Cohorts 1 and 2 Pre-Program LASF and Post-Program SHLA Results.
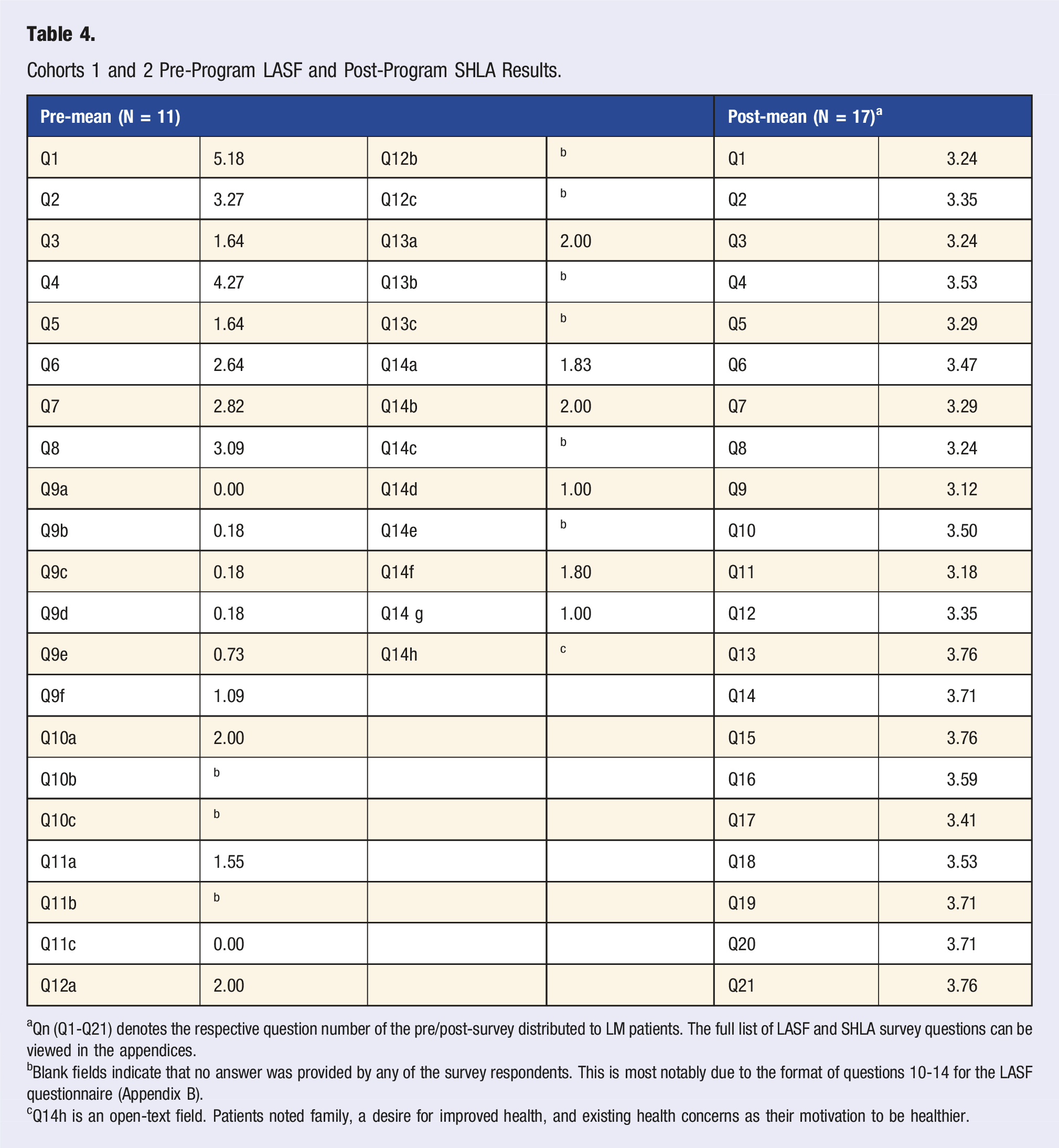
aQn (Q1-Q21) denotes the respective question number of the pre/post-survey distributed to LM patients. The full list of LASF and SHLA survey questions can be viewed in the appendices.
bBlank fields indicate that no answer was provided by any of the survey respondents. This is most notably due to the format of questions 10-14 for the LASF questionnaire (Appendix B).
cQ14h is an open-text field. Patients noted family, a desire for improved health, and existing health concerns as their motivation to be healthier.
Cohorts 3, 4, 5, and 6 Pre-and Post-Program WWH SHLA Results.
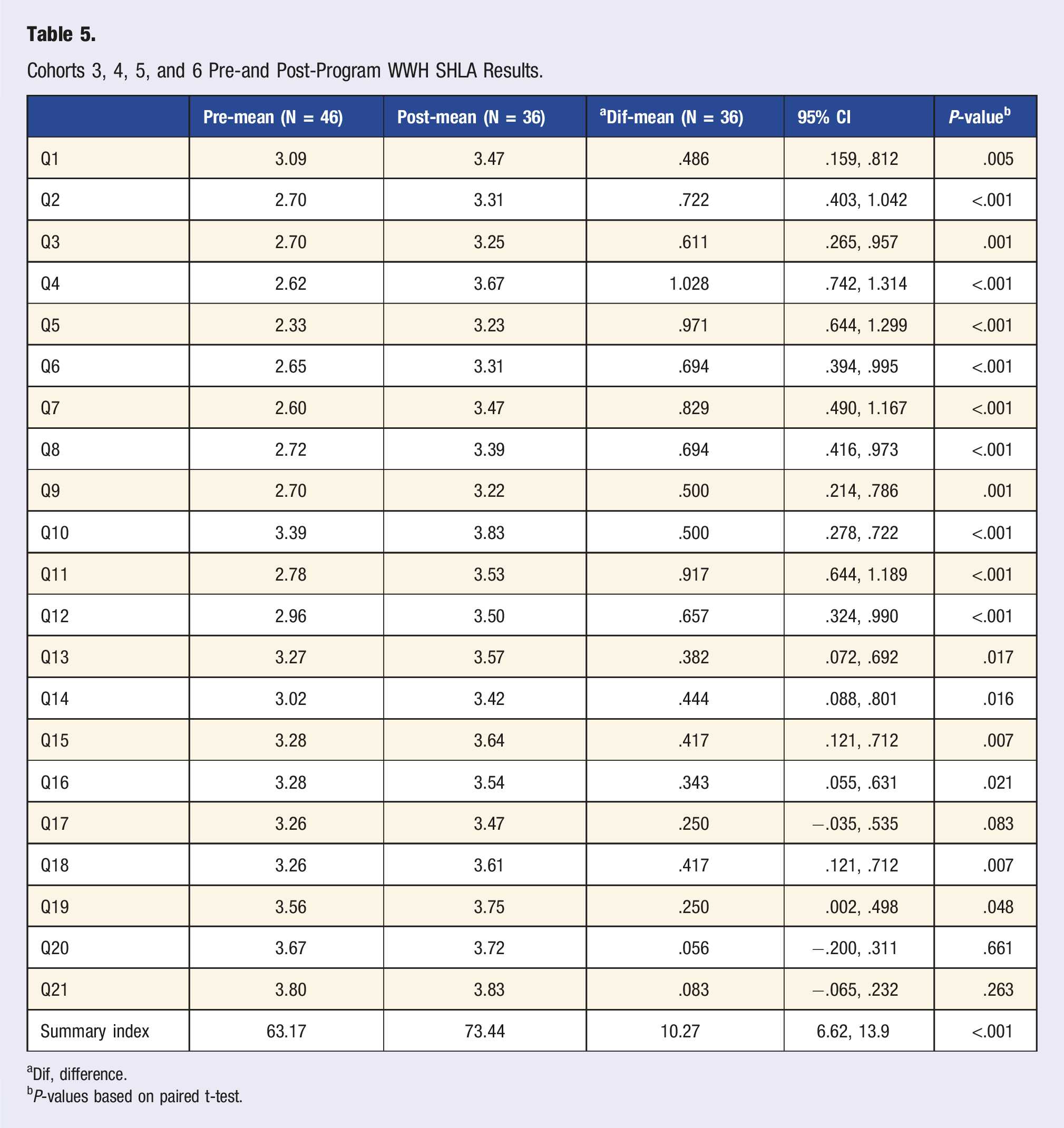
aDif, difference.
bP-values based on paired t-test.
Qualitative Results
Perceived Benefits and Perceived Barriers of Lifestyle Behavior Change
Qualitative Results From Key Informant Interviews (KII) and Focus Groups.
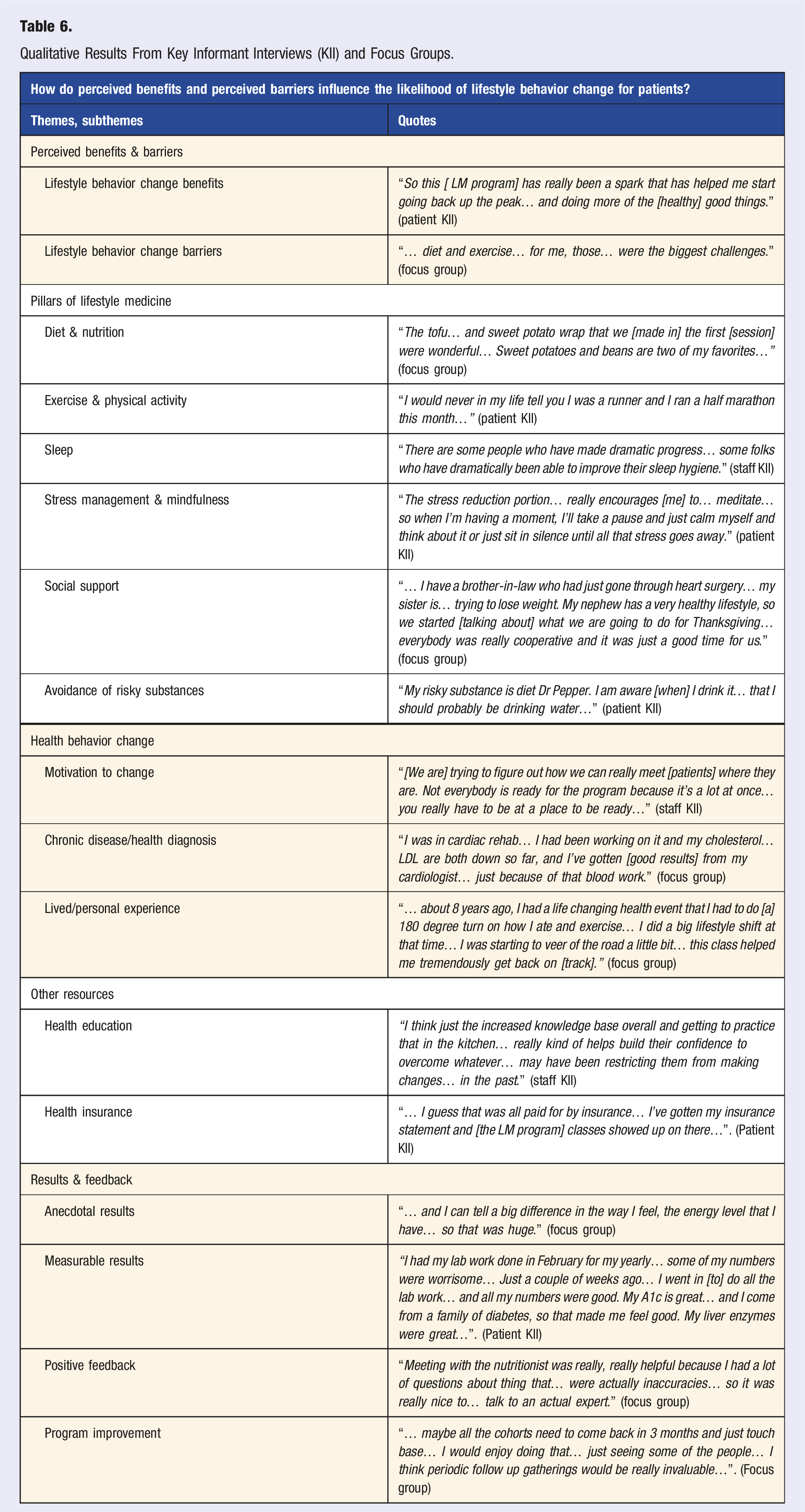
The key theme, “perceived benefits and barriers” occurred 157 times across all patient interviews, 93 times across all staff interviews, and 88 times across all focus groups. The following subthemes emerged from the perceived benefits and barriers themes: lifestyle behavior change benefits and lifestyle behavior change barriers.
One patient responded: “I could say [this program has] benefited me… all in a really well-rounded way. I was already eating close to a whole food plant-based diet… the sessions in the kitchen expanded my scope considerably.”
In a separate interview, one staff member responded: “… the transformation in some of these people’s lives, even in such a short window… we have a patient right now who in six weeks has absolutely changed [their] body in a way that… everything is just different about [them] in six weeks’ time… it’s just so fun to be a part of this kind of narrative.”
The key theme, “pillars of lifestyle medicine” occurred 241 times across all patient interviews, 132 times across all staff interviews, and 261 times across all focus groups. The following subthemes emerged from the pillars of lifestyle medicine theme: diet and nutrition, exercise and physical activity, sleep, stress management, social support, and avoidance of risky substances. The subtheme of diet/nutrition and exercise/physical activity emerged most frequently across all KIIs and focus groups, while the subthemes of sleep, stress, and avoidance of risky substances emerged very infrequently.
One patient responded: “I have really improved my balance… but I have been faithful with my exercise, coming to the Health Zone at least 3 or 4 times a week…”.
In a separate interview, one staff member responded: “The peer support that you get in the… group setting where you see [what other] people are going through, and we’re all going through our own struggles… that peer support, that camaraderie within the group is… really critical.”
The key theme, “health behavior change” occurred 161 times across all patient KIIs, 130 times across all staff interviews, and 192 times across all focus groups. The following subthemes emerged from the health behavior change theme: motivation to change, confidence and self-efficacy, chronic disease/health diagnosis, and lived/personal experience.
One staff member responded: “Ozempic… If you look at the package itself, it says when in combination with diet and exercise and lifestyle change… that [is on] the package insert. The company itself says [this], so we need to make sure that [these lifestyle factors are] addressed.”
In a separate interview, one patient responded: “… in the past few years I was diagnosed with diabetes, and… they really encourage you to eat a lot of protein and low carb with that [diagnosis], and I hated it. So the diet part [of this program] has helped me… I just think back to the habits that it teaches you to form… and looking at all aspects of your life to try to benefit and improve and grow.”
The key theme, “other resources” occurred 36 times across all patient KIIs, 74 times across all staff interviews, and 87 times across all focus groups. The following subthemes emerged from the health education theme: health education and health insurance.
One patient responded: “[The therapist], the things she taught us during some of our classes about relaxation and meditation and how to meditate and relax to go to sleep have really changed my life. So I really value that… I am using [this] now just habitually… when I’m working on something and a thought comes to mind that I shouldn’t be dealing with [right] now, I say ‘hey, I see you there, [but] I’m not dealing with you now… [and I] go back to what I was doing… so I feel like that has made me more confident, that… I can handle this stress because I know how to manage… thanks to [the therapist] from this program.”
The key theme, “results and feedback” occurred 66 times across all patient KIIs, 43 times across all staff interviews, and 121 times across all focus groups. The following subthemes emerged from the results and feedback theme: anecdotal results, measurable results, positive feedback, and program improvement.
One patient responded: “I’m on insulin, and we’ve cut [my dosage] almost in half… I have little spikes here and there, but overall, it’s about half what it was… I saw my primary care [provider] in October, [and] my blood work was better than it [has] looked in several years.”
Process Evaluation Results
Lifestyle Medicine Patient Feedback Survey
Patients especially appreciated the interactive cooking sessions; they reported enjoying the educational aspect of these classes, the opportunity to try new healthy foods, and the chance to learn practical cooking skills (such as using a variety of spices to prepare flavorful plant-based meals). One participant said: “I enjoyed actually cooking meals so I could see how easy it was to prepare. I also liked having the recipes included in our notebooks. I really didn’t find anything missing in the cooking sessions.”
The one-on-one consultations with the registered dietitian were highly rated, with participants noting that the personalized nutritional advice and concrete diet suggestions were particularly helpful. Similarly, sessions with the personal trainer were praised for providing tailored exercise guidance and motivation, which helped participants build confidence in physical activity routines. The educational lecture presentations covering various LM topics were generally described as informative and engaging, although a few respondents mentioned that the text on some slides was difficult to read due to a small font size. The group meditation and stress management practices at the end of each session were widely seen as beneficial for introducing mindfulness techniques and helping attendees reduce stress; several participants suggested allocating more time to these group mindfulness sessions in future cohorts. One participant noted: “The material was very understandable and when we did have questions [the LM staff] explained in a way that was easy to understand. I really appreciate all [they] have done to get this started to help people like me!”
Beyond the core sessions, participants also gave feedback on program logistics and support elements. Many appreciated the regular email communications from the LM staff, which reinforced key lessons and provided encouragement between meetings. The SFHS LM program notebooks were also mentioned as useful tools that helped participants stay organized. Some respondents proposed a minor scheduling adjustment—preferring a slightly later start time for the bi-weekly sessions to better accommodate work and family schedules. A few participants felt that certain classes were somewhat rushed or packed with too much material, indicating that a slightly slower pace (or additional sessions) might improve content absorption.
Finally, there was strong interest in maintaining the supportive community formed during the program: participants expressed enthusiasm for post-program reunions or follow-up gatherings, which would allow alumni to reconnect with peers and facilitators, share updates on their progress, and sustain motivation after completing the 8-week intervention.
Program Feedback From Interviews & Focus Groups
Feedback from participants during interviews and focus groups echoed the feedback survey findings and offered additional suggestions for enhancing the program. Ongoing community support was a prominent theme—many participants expressed a desire to stay connected with one another after the 8-week program concluded. For example, some recommended creating a private Facebook group or an email newsletter for program alumni to stay in touch, exchange healthy recipes, and support one another’s lifestyle changes. Consistent with the feedback survey, participants were also enthusiastic about periodic reunion events after program completion (e.g., monthly or quarterly gatherings) as an opportunity to celebrate milestones, reinforce healthy habits, and continue the supportive network developed during the program.
Participants additionally suggested a few modifications to the in-person sessions to improve engagement and social support during the program itself. To foster more interaction during the classes, some participants proposed rotating cooking partners each week so individuals could collaborate with different peers and build a broader sense of camaraderie. There were also calls for better integration of group physical activity into the class meetings; for instance, incorporating brief group exercise segments or demonstrations to reinforce the exercise pillar of lifestyle medicine alongside the individual physical activity guidance provided by the personal trainer.
Discussion
Summary of Key Findings
The quantitative analysis of the SFHS LM program results demonstrates significant improvements in patient biometric health outcomes, particularly reductions in weight and BMI, while changes in other chronic disease risk factors (i.e., blood pressure and lab values) also shifted in a desirable direction from pre- to post-program. This evaluation included pre- and post-program biometric and lab data for a subset of this program evaluation patient population (N = 63); BMI, weight, blood pressure, cholesterol, triglycerides, HDL, LDL, HbA1c, and blood glucose were analyzed. Although there was a desirable downward trend in total cholesterol, triglycerides, LDL, and HbA1c levels, and a desirable increase in HDL, these pre- to post-program shifts were not statistically significant, perhaps partially due to the small sample size. However, the positive biometric and lab result trends suggest potential benefits of the LM intervention in managing chronic disease risk factors. Additionally, significant improvements were observed in patient-reported knowledge, attitudes, self-efficacy, and purpose in life through the use of the SHLA pre- and post-program. These SHLA results indicate a meaningful impact of the LM program on patients’ perceptions and confidence in making lifestyle changes.
Qualitative analysis results further reinforced the effectiveness of the program by highlighting patients’ perceived benefits and barriers to lifestyle behavior change. Key themes emerging from interviews and focus groups included improved diet and exercise habits, enhanced confidence, self-efficacy, and motivation to change, and positive health outcomes such as weight loss and reduced medication (i.e., insulin and statins) reliance. Patients frequently noted the pillars of LM, with nutrition and physical activity as the most impactful aspects of the program, whereas sleep and avoidance of risky substances were mentioned much less frequently. Barriers to change included social norms and influences, time constraints, and motivation to change. Patients also emphasized the value of health education and support from healthcare providers in sustaining long-term lifestyle changes. Overall, the SFHS LM program was perceived as highly beneficial in promoting positive health behaviors, though ongoing support and strategies to overcome barriers may further enhance the impact and outcomes of the program over the long-term.25–27
The biometric trends observed in this evaluation are consistent with outcomes from similar lifestyle medicine programs such as CHIP and other intensive LM interventions, which typically report significant improvements in weight, blood pressure, and lipid profiles following program participation.9,10 Although some laboratory outcomes in our evaluation did not reach statistical significance, the direction of change mirrors findings of prior studies and suggests that even shorter LM interventions (such as this 8-week, bi-weekly model) may generate meaningful shifts in chronic disease risk factors. Comparable evaluations of lifestyle medicine programs show meaningful improvements in knowledge, diet, activity, and quality of life (e.g., patient-reported outcomes in a plant-based program in a safety-net system. 10 Furthermore, a recent digital LM intervention among emerging adults achieved >3% weight loss across intervention arms, illustrating the adaptability of LM models across age groups. 28 The findings of this LM program evaluation in Oklahoma align with the broader evidence base and extend it by focusing on a sample in a high-burden state context. Additionally, the field is moving toward consensus metrics and implementation frameworks,29,30 and the findings of this LM program evaluation contribute new data from an integrated health system in a region riddled with chronic disease burden.
The significant improvements in knowledge, self-efficacy, and lifestyle-related attitudes and behaviors observed in the SHLA align with prior LM studies demonstrating that psychosocial confidence and perceived ability to change are key mechanisms driving adoption of LM behaviors.8,10 The findings of this study contribute new evidence supporting the role of purpose in life as an important and understudied construct associated with lifestyle behavior engagement. In contrast to most existing LM evaluations, which have been conducted in academic medical centers or safety-net settings, this study represents one of the first mixed-methods LM evaluations conducted within a large integrated health system in the Oklahoma, a state with some of the highest chronic disease burdens nationally. This context underscores the potential population-level impact of LM interventions in regions with high disease prevalence and limited access to preventive care.
Implications of This Program Evaluation
Practical & Applied Implications
The findings of this evaluation highlight the effectiveness of the SFHS LM program in improving patient health outcomes, emphasizing the need for its integration and replication into clinical and community health settings.27,31,32 Clinicians can use these insights to enhance patient education and counseling, incorporating lifestyle medicine principles into routine care. Educators and practitioners can develop targeted interventions to address patient-reported barriers, such as time constraints and social influences, to foster sustainable behavior change. 27
Additionally, securing funding is essential for program expansion and sustainability. As a result of this program evaluation, the SFHS LM program has had the data and measurable results to be able to apply for and secure various grants to support its implementation and scalability, ensuring that more patients can access these beneficial services, and additional healthcare providers can be hired to expand the LM care team capacity. Furthermore, barriers related to data capture and analysis for this program evaluation and patient feedback related to social support have led to the exploration of the Health Motivate Engage App. 33 This platform is a tool that will help the SFHS LM care team collect real-time behavior change data and allow for patient group chat features, providing SFHS LM clinicians, researchers, and evaluators with up-to-date feedback on patient progress and adherence. Implementing such digital tools can enhance patient engagement, motivation, and long-term lifestyle behavior modification as well as lead to improved LM program processes and implementation strategies. 34
Policy Implications
The results of this evaluation underscore the importance of integrating LM into health policy and insurance reimbursement models. Given the significant improvements in patient weight, BMI, knowledge, and self-efficacy, policymakers should advocate for lifestyle intervention programs as reimbursable services under preventive and chronic disease management care. Expanding access to LM programs through policy changes can reduce healthcare costs by preventing, treating, and reversing leading chronic disease conditions and associated risk factors such as obesity, diabetes, hypertension, and cardiovascular disease, among others.27,32 Additionally, policies supporting workplace wellness initiatives and community-based lifestyle interventions can further enhance public health outcomes at the community level. 35
Implications for Future Research
Future research should focus on long-term outcomes and larger sample sizes to further validate the effectiveness of similar LM intervention programs. Studies incorporating randomized controlled trials would provide stronger causal evidence of the program’s impact on chronic disease risk reduction. Additionally, future research should explore personalized interventions tailored to more diverse populations, addressing cultural and socioeconomic barriers to the initial involvement in a program such as this and the associated lifestyle behavior change and improved health outcomes. Integrating real-time tracking through mobile applications and wearable technology could provide valuable insights into adherence and sustained behavior change over time.33,34
Broader Impact
The broader societal impact of the SFHS LM program extends beyond individual health improvements, contributing to population-level health advancements. The adoption of lifestyle medicine principles in clinical practice and public health initiatives can reduce healthcare expenditures, improve workplace productivity, and enhance quality of life.32,35 Technological innovations, such as mobile health applications and telemedicine, can further facilitate behavior change, making lifestyle interventions more accessible and personalized. Additionally, increasing public awareness of the benefits of lifestyle medicine can shift societal norms toward healthier living, ultimately reducing the burden of chronic diseases on healthcare systems at large. 27
Strengths and Limitations
This evaluation benefits from several strengths that bolster the credibility and relevance of its findings. The LM program at SFHS was grounded in strong evidence-based support from well-established sources, including similar successful programs,36-39 guidelines from the ACLM,2,40 and recommended frameworks from the CDC. 9 These affiliations provide a robust framework for the program, ensuring that its interventions are scientifically sound and align with best practices in the field of LM. Furthermore, this program evaluation process was based on evidence-based approaches provided by Rossi et al and the CDC program evaluation in the public health framework.15,41
Several limitations should be considered when interpreting the findings of this evaluation. Although the mixed-methods design strengthens the credibility of the results, both the quantitative and qualitative components contain important constraints that may affect generalizability and internal validity. First, the quantitative sample size was relatively small (N = 63), and not all participants had complete pre- and post-program biometric or laboratory data. Missing data reduced the statistical power to detect significant changes and may underestimate the program’s true impact. Self-report measures, including the SHLA, are subject to recall and social desirability bias, especially in a program emphasizing positive behavior change and close rapport with program staff.
Limitations also exist within the qualitative component. Although a total of eight key informant interviews and three focus groups were conducted and thematic saturation was achieved, the sample likely reflects perspectives of more engaged, motivated, or satisfied participants. Recruitment relied on convenience sampling and voluntary participation, which may have introduced selection bias. Individuals who were less satisfied with the program, faced more substantial barriers, or disengaged early may not be represented in the qualitative findings.
Contextual factors related to the state of Oklahoma should also be acknowledged. As a state with exceptionally high rates of chronic disease, limited access to preventive care, and substantial health disparities, Oklahoma represents a high-need, high-burden environment. While this context underscores the importance and relevance of the SFHS LM program, it may limit the transferability of findings to regions with different healthcare infrastructures, socioeconomic conditions, and baseline health status.
Finally, the LM program itself was evolving during the evaluation period. Program processes, including assessment tool use, data capture procedures, and aspects of program delivery. For example, early cohorts used two different program assessment tools (ACLM LASF vs SHLA), which limited comparability of pre/post findings across all 63 participants. Variations in implementation may have introduced inconsistencies that affect the reliability of the outcome measures. As the program continues to mature and standardize its evaluation tools and processes, future assessments may yield more consistent and comparable data.
Conclusion
The SFHS LM program demonstrated significant improvements in patient biometric outcomes, knowledge, attitude, behavior, and confidence/self-efficacy from pre- to post-LM program, reinforcing the value of lifestyle interventions in preventing, treating, and reversing chronic disease conditions and associated risk factors. While some lab value reductions were nonsignificant, the overall trend of patient biometric and lab results suggests a positive impact on health outcomes and reduction in chronic disease risk factors. The qualitative findings further highlight the program’s effectiveness in fostering motivation, self-efficacy, and lifestyle behavior change. Addressing barriers such as social influences and time constraints can enhance the program’s long-term success. Policy integration and technological advancements, including real-time behavior tracking, can further support patient engagement and adherence. Moving forward, expanding the program’s reach and refining strategies based on patient feedback will be crucial in maximizing its impact.
Supplemental Material
Supplemental Material - Improving Health Outcomes for Oklahomans: A Mixed-Methods Evaluation of a Lifestyle Medicine Intervention Program
Supplemental Material for Improving Health Outcomes for Oklahomans: A Mixed-Methods Evaluation of a Lifestyle Medicine Intervention Program by Lauren E. Vanderpool, R. Patti Herring, W. Lawrence Beeson, Anna Nelson, Ajay Joseph in American Journal of Lifestyle Medicine
Footnotes
Ethical Considerations
This study was conducted in accordance with ethical guidelines and approved by the Loma Linda University Health Institutional Review Board under approval number 5240374 and the Saint Francis Health System Institutional Research Ethics Board under approval number 2368-24.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.