
Abstract
Background
Cancer survivorship guidelines emphasize Lifestyle Medicine (LM) pillars, including physical activity, healthy eating, restorative sleep, stress management, and avoiding risky substance use. We describe the development and patient population of a multidisciplinary LM clinic in oncology.
Methods
The clinic launched virtually in 2020. Patients had same-day consultations with an oncologist/nurse practitioner, nutritionist, and psychologist. Patients completed a one-time online survey assessing demographics, quality of life, LM pillars, and mental health. Descriptive statistics were used to characterize the population.
Results
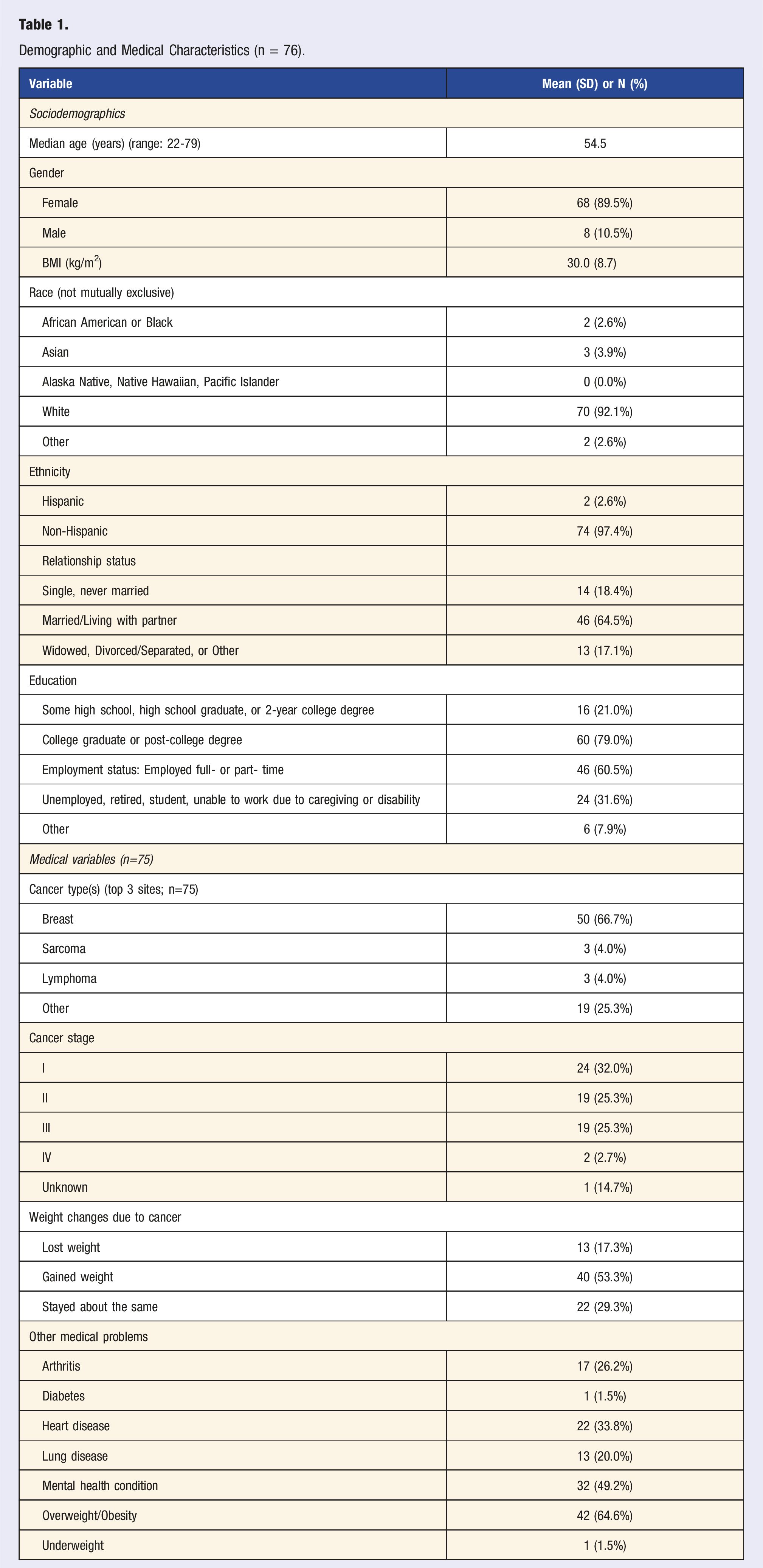
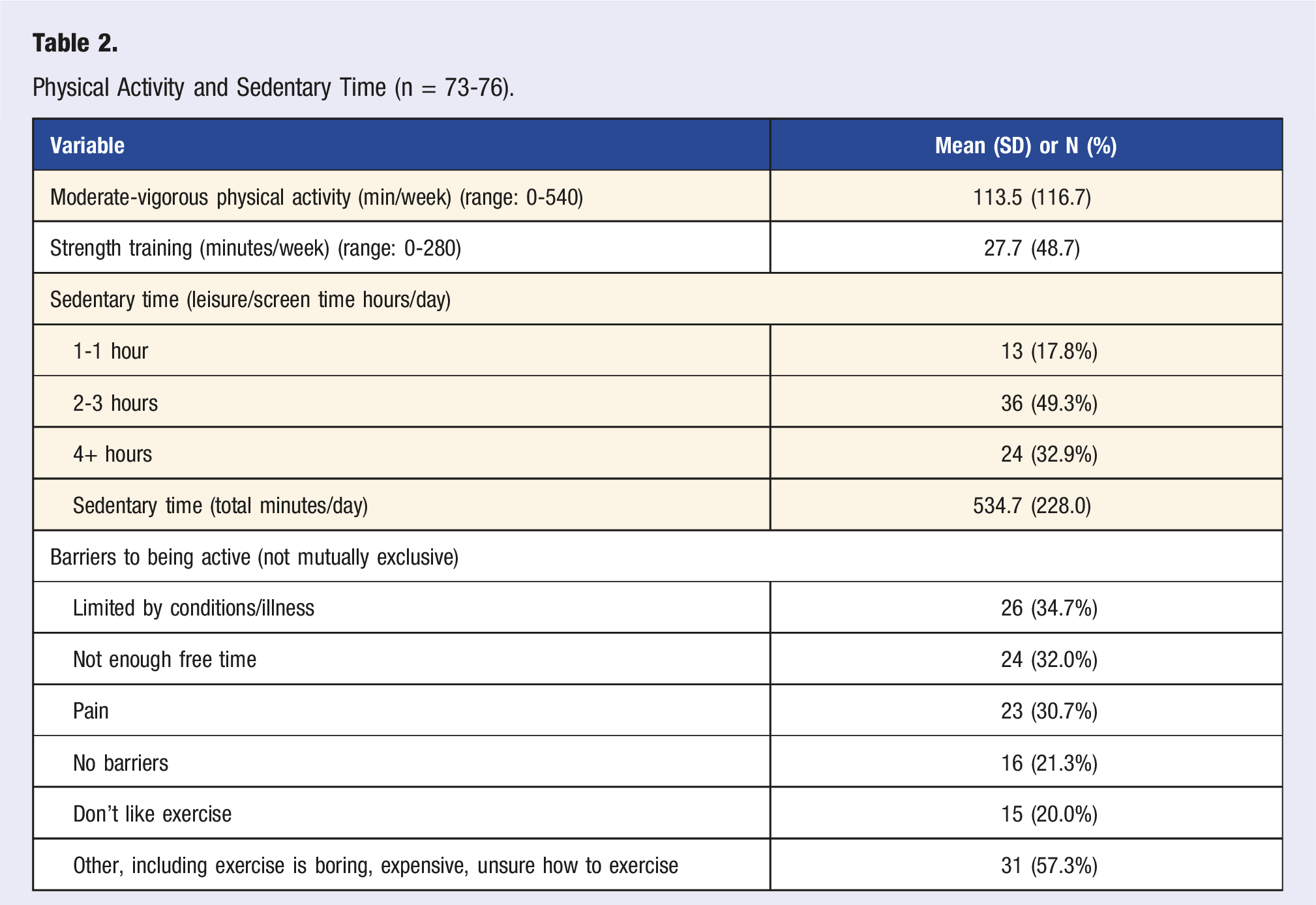
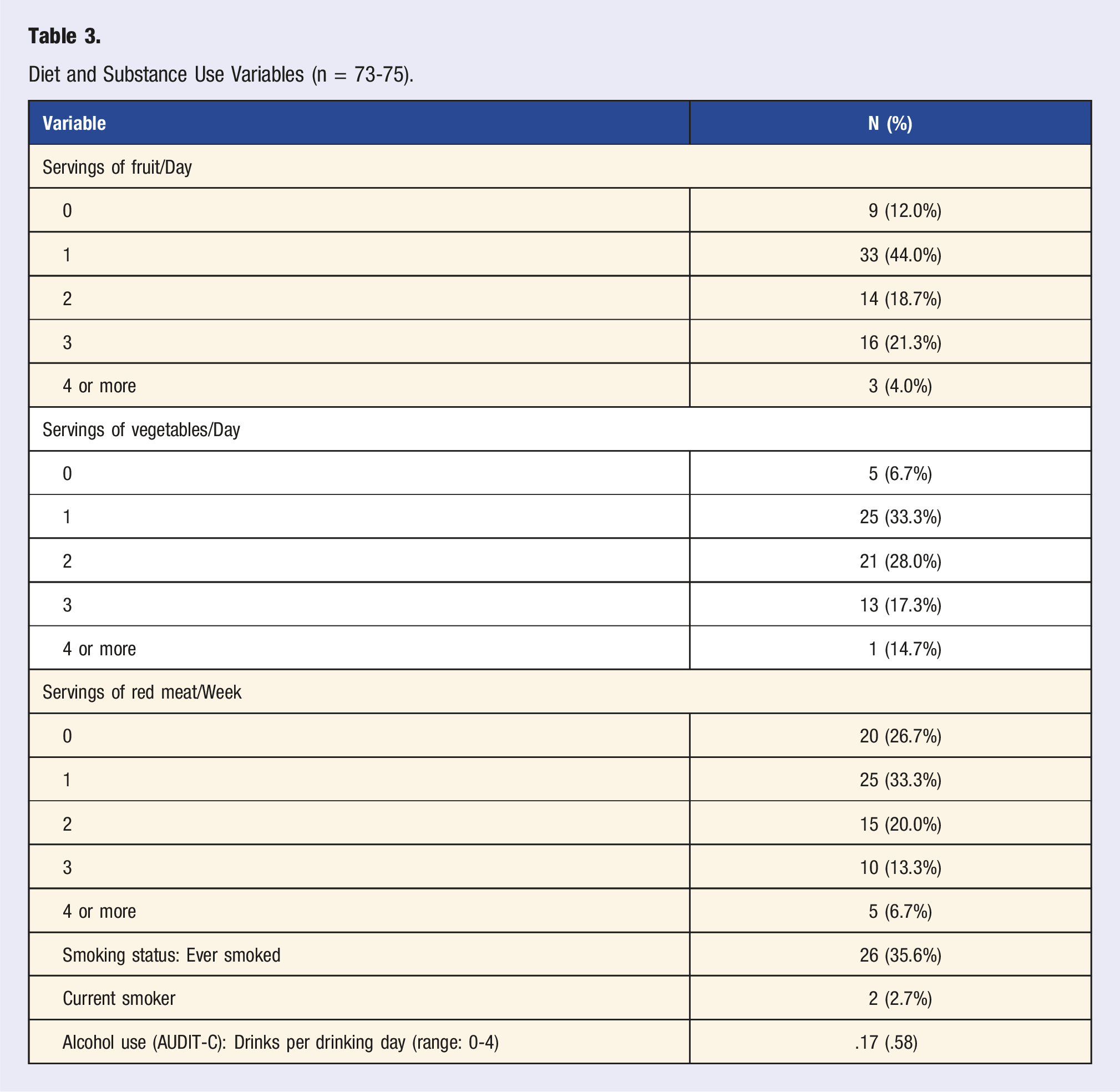
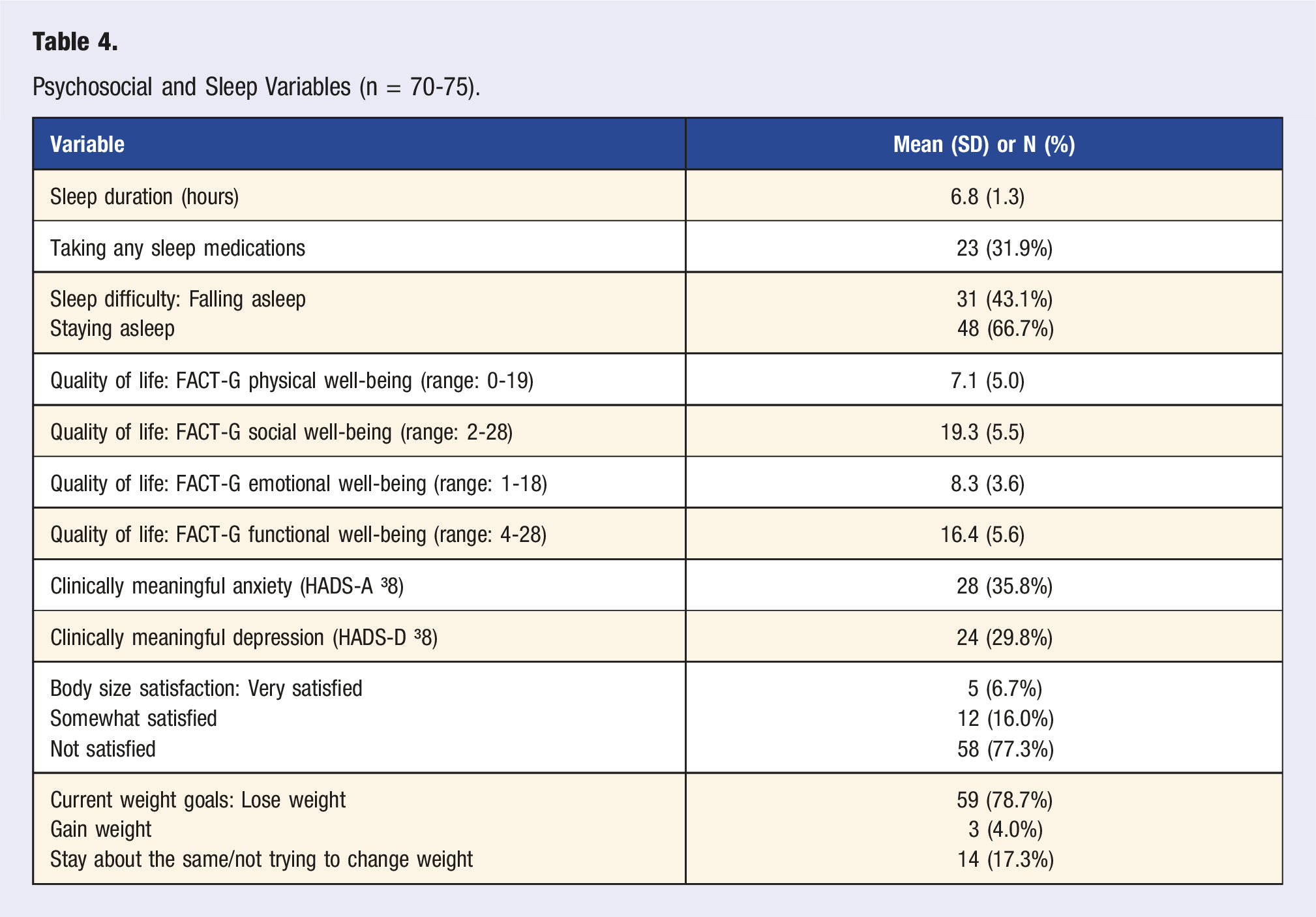
Seventy-six patients took the survey (July 2020-January 2023). Most were female, non-Hispanic White, with early-stage cancers. The mean BMI was 30 kg/m2. A minority of patients met aerobic physical activity (27.6%) and dietary (28.6%) recommendations. Two-thirds (67%) reported sleep difficulties, and 30%–36% reported elevated anxiety/depression. Over half (53.3%) gained weight due to cancer treatment and 78.7% were trying to lose weight.
Conclusion
This paper details the baseline LM needs of cancer survivors seeking lifestyle consultation and describes the development of the clinic to address these concerns. Patients were open to evaluation and treatment in an oncology-focused LM clinic. This clinic model has potential to improve quality of life for survivors.
“The survivor population was largely composed of people with early-stage cancers, with the most common cancer type being breast cancer.”
Introduction
There are currently over 18 million cancer survivors in the United States, with survivorship projected to increase by 25% by 2032. 1 Treatments for cancer can include surgery, radiation, and systemic chemotherapy, which can lead to unintentional weight loss or gain, depending on cancer type and site. 2 Cancer survivorship is often a time of heightened worry about cancer recurrence, 3 and increasing healthy lifestyle behaviors can improve quality of life (QOL), as well as reduce the risk of recurrence and the development of additional chronic diseases.4-8 The six pillars of lifestyle medicine (LM): physical activity, a plant predominant diet, restorative sleep, stress management, avoiding risky substances, and social connections, are important for cancer treatment and survivorship.5,9-13 Authoritative bodies such as the American College of Lifestyle Medicine (ACLM), the American Cancer Society (ACS), the US Centers for Disease Control and Prevention (CDC), and the American College of Sports Medicine (ACSM) recommend incorporating LM education and practice into the continuum of cancer care to improve QOL and physical functioning.10,14 For instance, physical activity guidelines from authoritative bodies such as ACS, 15 NCCN, 16 and ACSM 14 recommend that cancer survivors engage in at least 150-300 minutes of at least moderate intensity aerobic activity and 2 strength training sessions per week. Despite the demonstrated benefits and decisive recommendations of LM interventions in survivorship, few services are established to address the domains of LM for patients with cancer and other populations. 17 Accordingly, our team of oncologists and supportive oncology clinicians developed a multidisciplinary LM clinic for patients with cancer. This paper describes the origin and development of the clinic and the characteristics of its patients.
This multidisciplinary LM clinic was the first known of its kind within supportive oncology. This clinic began in 2016 as a single-provider, single consultation clinic with a LM-trained medical oncologist. Based on the initial experience and the referral patterns of patients seen, the LM clinic evolved into a multidisciplinary consult clinic adding a nutritionist and a psychologist focused on health behavior change to the consultation. This multidisciplinary clinic was launched on a virtual platform due to the COVID-19 pandemic in 2020. Due to demand, a second clinic was opened by an ACLM-certified nurse practitioner and nutritionist who later began a virtual group visit program based on the six pillars of LM. The group visits were born out of the recognition that patients needed and were seeking ongoing education and skills for lifestyle education and behavior change.
The six pillars of LM were used as a foundational structure for the individualized consultations. Patients were encouraged to identify the survivorship topics within LM that were most important to them as the focus of the consultation (e.g., exercise limitations or recommendations).
In the multidisciplinary format, the first appointment was with the medical oncology provider (MD or NP). During this visit, a comprehensive medical history was taken, and patients were screened for limitations on physical activity using the Physical Activity Readiness Questionnaire.18,19 The nutritionist then conducted a comprehensive dietary assessment, and personalized recommendations were given. Additional resources, such as referrals to obesity medicine or individual follow-ups, were made as needed. Finally, the behavioral psychologist screened for psychosocial concerns, stressors, and helped patients create a behavior change plan to successfully implement their LM recommendations gained throughout their clinic day. Though the model was initially set-up as a one-time consultation, longitudinal follow-ups with nutrition, LM NP, and psychology were available as indicated. Further, virtual group visits were established in 2022 to offer a structured, longitudinal LM model that would increase access for patients seeking LM support and education. The curriculum for the group visits was based on the established PAVING The Path to Wellness curriculum.20,21 Group visits were conducted over zoom and the program includes a total of six visits based on the six pillars of LM. Each visit was 75 minutes in duration. The topics for the program include Exercise for Wellness and Recovery, Nutrition in Cancer Care, Start and Sticking with Healthy Habits, Better Sleep More Energy, Stress Management Tips and Tools, Making Meaning: Social Connections and Purpose. The curriculum is offered on a rolling basis and participants were encouraged to attend all 6 visits.
To guide assessment within the clinic, all participants presenting for individual consultation were offered a self-administered survey addressing baseline LM domains that was completed prior to their clinic visit. Patients provided information about their sociodemographic, medical, health behavior, and well-being characteristics. Seventy-six patients completed the intake survey between 2020-2023. We present the baseline data collected to demonstrate the types of LM issues and their prevalence reported by patients seeking LM care at a tertiary academic center and provide details of the clinic to help inform LM and cancer survivorship professionals of the options and challenges of building this program for cancer centers and patients.
Methods
Patient Population
Eligible patients included any patients over the age of 18 who had a history of cancer or who were currently undergoing treatment for cancer. All patients were seen at our hospital, but the clinic was open to cancer patients who had been or were undergoing treatment at different institutions. The inclusion criteria were that patients had to have been referred by an oncology provider or self-referred to the clinic, scheduled a visit, and willing to take the survey. There were no exclusion criteria.
Clinic Development and Launch
The multidisciplinary LM clinic launched during the COVID-19 pandemic as a virtual (online) clinic. Patients had same-day sequential consultations with a medical provider (MD or NP), nutritionist (RD), and a behavior change psychologist (PhD) over the course of 2 hours. During the virtual visits, patients’ needs were evaluated, and LM recommendations were made with a particular focus on their LM priority areas.
A goal of the clinic was to provide broad access to consultation and LM resources. Patients were billed and received a co-pay for the MD/NP consultation and group visits, but consultation with nutrition and psychology was not billed to the patient. The cost for the nutritionist was covered within the hospital’s operating budget and behavioral psychologist through philanthropy. In addition, the LM clinic providers, in partnership with physical therapy and physical medicine and rehabilitation specialists, developed 8 free, web-based exercise videos designed for cancer survivor use 22 ). In addition to the individual consultations, patients could opt into the virtual group visits, which were based on a 6-part rolling curriculum, corresponding to the LM pillars. Patients were also referred to additional supportive care programs available at our cancer center or in the community. Patients’ insurance was billed for a follow-up visit for each virtual group session and patients were responsible for the co-pay. In 2023, the clinic returned to a single (MD) or dual (NP/RN) provider model, which was largely due to a lack of ongoing funding.
Survey Development and Administration
Prior to attending the clinic, patients were sent an online self-report survey assessing all domains of LM, demographics, quality of life, and cancer-specific items (e.g., site, time of diagnosis). The survey was optional, and their care at the clinic was not contingent upon survey completion.
Data in the present sample were collected from July 2020 through January 2023. All responses to each survey item were used to calculate the scores, such that respondents with missing data were still included when they supplied any data (pairwise deletion). Study data were collected and managed using REDCap electronic data capture tools hosted through our healthcare system.23,24 REDCap (Research Electronic Data Capture) is a secure, web-based software platform designed to support data capture for research studies. All survey procedures were IRB approved.
Survey Development and Measures
The online survey was developed by a multidisciplinary team of physicians, nurses, psychologists, and research staff. It was designed to take a comprehensive approach to assessing the pillars of LM and related constructs for this patient population. When appropriate, validated and cancer-specific surveys were included. When validated measures were not available, items were created specifically to gather information about lifestyle behaviors of clinical relevance to the planned LM visit. The details of each measure are described below.
Demographics
Participants reported their date of birth (from which age was calculated based on survey response date), gender, race, ethnicity, education, employment, and marital status.
Medical Variables
Participants were asked to report their height, weight, cancer type, stage, and treatment, and additional medical diagnoses.
Physical Activity, Diet, and Sleep
To assess physical activity, participants completed PACE measures, 4 reporting the number of minutes of aerobic and strength physical activity, as well as sedentary time, per day and week. Sedentary activities included time spent commuting, on screens, phones, reading, and hobbies. To assess dietary quality, participants were asked to report the number of servings of fruit, vegetables, and red meat they ate each day and week. Sleep was assessed using 6 items created by our team for this survey, including items on difficulty falling asleep, staying asleep, and sleep duration.
Weight and Body Image
Participants were asked to rate three items created by our team for this survey assessing how they felt about their body size, if they were trying to lose weight, and if their weight changed because of cancer treatment.
Substance Use
Participants completed the 3-item AUDIT-C to assess alcohol use. 25 One item from the AUDIT-C was used to assess adherence to alcohol recommendations (e.g., less than 2 drinks/day for men and 1/day for women): “How many standard drinks containing alcohol do you have on a typical day? (One drink is defined as 12 oz beer, 5 oz wine, or 1.5 oz liquor (e.g., vodka).)” Adherence to tobacco recommendations was assessed using 6 items about current and historical tobacco use, and interest in quitting smoking if applicable, based on the National Comprehensive Cancer Network’s (NCCN) survivorship guidelines. 26
Quality of Life
The 27-item Functional Assessment of Cancer Therapy-General (FACT-G) was used to assess cancer-specific physical, social, emotional, and functional well-being. 27 The FACT-G contains four sub-scales for physical (7 items), social/family (7 items), emotional (6 items), and functional (7 items) well-being. These self-reported measures possess strong psychometric properties and have been validated for patients with cancer. Higher total and subscale scores indicate better QOL.
Anxiety and Depression
The 20-item Hospital Anxiety and Depression questionnaire (HADS) 28 is a well-validated tool used in many studies with medical patients, which derives scale scores for anxiety and depression. Scores on each subscale range from 0 to 21, with a cutoff of 8 or greater denoting clinically meaningful anxiety or depression. The measure has good psychometric properties in patients with cancer [19, 20].
Data analysis
Stata 17.0 was used to calculate descriptive statistics of the patient population and survey measures.
Results
Demographic and Medical Characteristics (n = 76).
Physical Activity and Sedentary Time
Physical Activity and Sedentary Time (n = 73-76).
Diet and Substance Use
Diet and Substance Use Variables (n = 73-75).
Sleep, Quality of Life, and Mental Health
Psychosocial and Sleep Variables (n = 70-75).
Discussion
This paper highlights the characteristics, concerns, and needs of cancer survivors seeking LM consultation in a newly developed multidisciplinary LM clinic from 2020-2023. Most importantly, this paper demonstrates major lifestyle health concerns among patients with cancer and a willingness of patients to seek care within a dedicated LM clinic to address these needs. The survivor population was largely composed of people with early-stage cancers, with the most common cancer type being breast cancer. We found that most patients did not meet physical activity and diet (fruit and vegetable) recommendations for cancer survivors,9-13,29 which LM interventions can address. This study also shows poor sleep quality, low physical and emotional cancer-specific QoL, prevalent body size dissatisfaction, and weight loss intentions among this population. Cancer survivorship clinics, such as this one, can play an important role in the cancer care trajectory to improve the many mental and physical health concerns following treatment.8,25
Meeting physical activity recommendations is associated with reduced risk of cancer recurrence30,31 and mortality32-34 in cancer survivors. In addition, physical activity is associated with reduced rates of lymphedema, 35 fatigue, 36 cardiovascular disease, 18 and depression, 37 all of which can be debilitating side effects of cancer treatment. This study found that cancer survivors in the LM clinic engaged in an average of 113.6 minutes of moderate-to-vigorous intensity aerobic exercise and 27.7 minutes of strength training per week, though number of bouts of strength training was not assessed. The most reported barriers to exercise were physical and time limitations. A clear gap between physical activity recommendations (e.g., 150 minutes of moderate-vigorous activity/week) and patients’ experiences and abilities to engage in physical activity is demonstrated in these findings. While many patients were engaging in regular activity, the self-reported averages in this study do not meet national-level recommendations. By providing guidance and education around physical activity, clinicians, such as those in the LM clinic, may help patients come closer to meeting recommendations, thereby increasing the likelihood of positive oncologic outcomes while mitigating side effects of treatment. Further, specific, focused consultations with behavior change specialists, such as psychologists and health coaches, may help patients overcome their barriers to initiating and sustaining physical activity.
Dietary guidelines for cancer survivors all emphasize consuming a variety of plants and plant-based foods, limiting red and processed meat, limiting sugar intake, and eating whole grains.38-41 Adhering to these guidelines in survivorship has been associated with reduced risk of all-cause and cancer-specific mortality,42-44 reduced obesity,45,46 and improved quality of life.47-49 Specifically, with respect to the present findings, guidelines support consuming at least five servings of fruits or vegetables per day, and eating no more than three servings of red meat per week. 29 Data from the present study indicated that patients consumed a mean of 3.6 servings of fruits or vegetables per day, and 1.4 servings of red meat per week. Patients appear to be meeting the recommendation to lower red meat consumption, but they are not meeting the recommendations for fruits or vegetables. Assisting patients in incorporating more fruits or vegetables into their diets is a clinical and public health priority that a clinic such as this one can promote. Referrals to—or an embedded—nutritional consultation are a key to LM clinics’ abilities to meet patients’ needs for nutrition education, advice, and targeted dietary change recommendations.
In terms of sleep, substance use, and stress, we found that patients reported poor sleep quality, low sleep duration, very limited use of alcohol and cigarettes, and rates of anxiety and depression symptoms higher than those of the general population. As sleep has restorative properties that can improve survivors’ QoL, it is an important area of targeted interventions. Cognitive Behavioral Therapy for Insomnia (CBT-I) is an evidence-based non-pharmacological treatment for several sleep problem areas 50 and should be considered as a strong referral option for LM providers, given its efficacy for cancer patients and survivors. 51 It is encouraging that this patient population engages in very little use of harmful substances, though anyone who smokes or uses alcohol excessively would benefit from collaborations with smoking cessation and psychology resources. By intervening in cases of risky substance use, our providers may assist patients in promoting positive outcomes and preventing the development of further illnesses. In the US adult population, the prevalence of anxiety symptoms was 8.1% and depression symptoms was 6.5%, 52 whereas our clinic population reported elevated anxiety (35.8%) and elevated depressive symptoms (29.8%). The HADS is not a clinical diagnostic tool, however, these findings indicate elevated mental health and stress concerns among the cancer survivors presenting to this clinic. Close referral sources to mental health specialists are encouraged for any LM clinic.
As this is primarily a descriptive study, there are inherent limitations. First, the clinic population was based on referrals, so the patients seen reflect the referring oncology specialties (e.g., predominantly breast cancer). If there had been more outreach and advertisement to other specialties, there may have been more patients presenting for sleep, substance use, or other LM pillars. This clinical sample was largely white, female, well-educated, and employed. Thus, it is not yet clear if these results would generalize to other populations, indicating a need to expand this clinic and survey over time and in new clinical settings or hospitals. Future research will include pre-post clinic evaluations to assess for change over time related to these LM interventions. Moving forward, we aim to collect additional survey data on patient experiences with the LM clinic to complement the existing demographic and descriptive statistics. Such surveys could inform program development, for example, what an optimal number of group and individual sessions might be for patients to attain long-term benefits. Patient satisfaction with the LM clinic, overall quality of life, and attitudes towards ongoing medical care are also important metrics to consider as this clinic continues to grow. Self-reported data on what topics in LM the patients found most useful and where they have experienced the most growth would allow the LM team to adapt the group curriculum and individual sessions to best meet patient needs. This paper summarizes the successful development of a LM clinic to meet the many needs of cancer survivors to improve their overall health and well-being. This clinical model may encourage more providers and healthcare systems to offer LM services for cancer survivors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.