
Abstract
Introduction. Lifestyle-focused rehabilitation plans need to become part of the standard system of care for the treatment of chronic diseases. To achieve this goal, the KAP of rehabilitation professionals toward lifestyle medicine needs to be understood. This study investigated the niche of orthopedic manual physical therapy and is purposed as a foundational model for continued research. Method. A survey instrument was designed to investigate the KAP of orthopedic manual physical therapists toward lifestyle screening and education. Results. There were 155 participants of which 58.1-72.3% reported frequently talking to their patients about lifestyle topics, while 78.1-80.6% felt highly confident and competent while doing so. Additionally, 92.9-94.8% thought that lifestyle screening and education was important and that physical therapists should be doing it. Participants discussed exercise most frequently with their patients (96.1%) and alcohol the least (12.9%). Participants with advanced degrees (ie, PhD or DSc) had significantly higher Practice (MΔ= −3.755, P = .001) and Knowledge (MΔ= −4.14904, P = .020) ratings than those with entry-level physical therapy degrees. Conclusion. There was strong acceptance of lifestyle screening and education in orthopedic manual physical therapy with an emphasis on exercise. This study provides a foundational basis for continued research.
Knowledge, Attitude, and Practice of Orthopedic Manual Physical Therapists Toward Lifestyle Screening and Education: A Descriptive Study a foundational study design to investigate the KAP of physical therapists in a specific setting and specialty
Introduction
Medical advancement in the early 20th century brought about effective solutions to common diseases such as smallpox, cholera, diphtheria, polio, measles, hepatitis, and more; conditions that devastated populations as late as the 19th and even early 20th centuries are now rare or nonexistent. 1 Advancements in biochemistry, biophysics, physical chemistry, virology, and immunology brought about these celebrated medical victories. 1 Yet, as the prevalence of certain diseases decreased in the latter half of the 20th century, that of chronic diseases such as heart disease, cancer, and stroke increased. 2
Efforts to mitigate the risks of chronic diseases were made at the end of the 20th century. In 1999, the United States Centers for Disease Control and Prevention reported that public health efforts in the late 20th century had identified several lifestyle-related risk factors contributing to chronic diseases and intervened to reduce mortality.2,3 Yet, in 2014, the leading causes of death were mostly unchanged, and a percentage of these deaths was reported as preventable through lifestyle change: diseases of the heart (30% preventable), cancer (15% preventable), unintentional injuries (43% preventable), chronic lower respiratory disease (36% preventable), and stroke (28% preventable). 3
Therefore, in 2014, the Centers for Disease Control and Prevention continued its efforts to manage the chronic disease burden by implementing the following strategies: epidemiology and surveillance to monitor trends and inform programs; environmental approaches that promote health and support healthy behaviors; health system interventions to improve the effective use of clinical and other preventive services; and community resources linked to clinical services that sustain improved management of chronic conditions. 4
Despite these efforts, the successful decline of chronic conditions was minimal as evidenced by a report from 2017, which showed that 74% of deaths in the United States were still caused by heart disease, cancer, unintentional injuries, chronic lower respiratory disease, stroke, Alzheimer’s disease, diabetes, influenza and pneumonia, kidney disease, and suicide. In fact, the prevalence of 7 of these 10 conditions actually increased from 2016 to 2017; cancer was the only condition the prevalence of which decreased by 2.1%, that of heart disease and kidney disease did not change, and the prevalence of all other conditions increased. 5
To date, efforts to decrease the prevalence of chronic diseases have been largely ineffective, but these preventive efforts have successfully identified metabolic risk factors, such as obesity, high blood pressure, and high blood sugar, as the most powerful predictors of chronic diseases.6-10
Further, certain lifestyle behaviors have been associated with metabolic risk factors, chronic diseases, or both. The primary lifestyle behaviors found to influence chronic diseases are as follows: diet,9-34 exercise,8-10,29-34 cigarette smoking,2,3,12,27,29,30,35-40 alcohol consumption,8,11,18,27,31,36,40-44 water consumption,2,8-10,28 rest and sleep,8,44-46 and perceived stress levels.10,43,45,46
Additionally, many of these risk factors also correlated with other chronic diseases—such as arthritis29,35 and osteoporosis 29 —that can greatly decrease an individual’s independence and overall quality of life. Research from 2008 and 2010 named osteoarthritis as the most common and persistent cause of mobility dependency and disability in the world with a prevalence of over 250 million affected people, which is approximately 3.6% of the world’s population.47,48 Obesity is the most modifiable risk factor for knee osteoarthritis. 35
Although it is now well established that there is a strong association between lifestyle behaviors and chronic diseases—from here forward referred to as lifestyle-related chronic diseases (LRCD)—initiatives to facilitate behavior change have been grossly unsuccessful. Factors attributed as barriers to public behavior change are (1) conflicting research leading to debate on the most effective recommendations for certain lifestyle behaviors, such as diet17-19; (2) lifestyle behavior change initiatives conflicting with commercial interests13,14,30; and (3) low utilization of nonpharmaceutical alternatives by medical professionals for managing LRCD. 35
Based on conflicting reports in the literature, dietary recommendations for preventing LRCD are discrepant. It has been speculated that competing interests in the commercial weight-loss and diet market have led to partial, biased, or misleading research on best dietary practices.13,14,49 However, in-depth investigation of the research revealed one primary trend that is universal for preventing LRCD—the whole food and plant-based diet.13-27,30 Some feel it is too extreme to expect people to shift from an animal-based to a plant-based diet and instead advocate for simply recommending an increased intake of fruits and vegetables.13,14,25,29,50 Yet, even with this more “achievable” goal, the majority of American adults do not meet the minimal dietary guidelines. 50
It has to be illustrated that whole food and plant-based dietary practices are effective for the prevention of LRCD.13,14,49 However, even within the plant-based realm, whole food practices are resisted. Several investigators have proposed that commercial interests are served better by foods with a high profit margin, that is, processed foods with a long shelf life that are easily transported around the globe and marketed; however, these have been shown to contribute to LRCD.7,13,14 It has been suggested that dietary behavior changes cannot be fully effective when competing with corporate interest and that public health advocates need to seek out mutual interest with food corporations.7,13,14
Despite the debates on best practices for certain lifestyle behaviors or competing interests with the commercial market, there is considerable research showing that community programs and individual action plans can be effective for facilitating lifestyle behavior change and ultimately reducing the risk factors associated with LRCD.34-36,43,47 However, the underutilization of nonpharmacological interventions for the management of LRCD is thought to be a primary contributor to unsuccessful mitigation of these conditions. 35 Based on the evidence, it could be stated that lifestyle behavior change needs to be recognized as part of the standard system of care for LRCD.
All healthcare professionals and public health advocates can play a role in educating patients and the public on the connection between lifestyle behaviors and chronic diseases. However, rehabilitation professionals, such as physical therapists and occupational therapists, may be uniquely positioned to provide nonpharmacological alternatives for the rehabilitation of those with LRCD. Several models of care have proposed that physical therapists are particularly well placed to incorporate lifestyle behavior change into their practices.36,43,45,51-55
Elizabeth Dean reported that physical therapists are in a “preeminent position” to focus on the prevention, management, and, in some cases, cure of chronic conditions and that physical therapists need to include “assessment of smoking and smoking cessation (or at least its initiation), basic nutritional assessment and counseling, recommendations for physical activity and exercise, stress assessment, and basic stress reduction recommendations, and sleep assessment and basic sleep hygiene recommendations.”36,43,51,55 Further, the first Physical Therapy Summit on Global Health held in 2007 concluded, “Contemporary definitions of physical therapy support that the profession has a leading role in preventing, reversing, as well as managing lifestyle-related conditions.” 51
The American Physical Therapy Association also advocated for lifestyle management as a part of the physical therapist’s practice and reports, “It is within the professional scope of physical therapy practice to screen for and provide information on diet and nutritional issues to patients, clients, and the community.”56-60 Research by Lein et al 52 found that an interdisciplinary group of healthcare professionals believes that physical therapy practice should include lifestyle-focused care; the researchers presented the Health-Focused Physical Therapy Model as one method through which physical therapists can integrate lifestyle screening into practice.
It is evident that physical therapists may be uniquely positioned to incorporate lifestyle behavior change into patient care. Still, the questions remain, do physical therapists feel confident and competent enough to provide lifestyle-centered patient care plans, if so, how do they feel about implementing lifestyle medicine into practice, and are any physical therapists already addressing lifestyle behavior change with patients? To answer these questions, the full spectrum of physical therapists, in all practice settings and specialties, needs to be considered. Thus, the purpose of this study was to establish a foundational study design to investigate the knowledge, attitude, and practice (KAP) of physical therapists in a specific setting and specialty that can be replicated for future research across a variety of settings and specialties. The niche investigated in this study was that of orthopedic manual physical therapy (OMPT) in the outpatient setting. The investigators selected this niche based on the lead investigator’s focus of study at the time.
Methodology
Study Design and Participant Selection
The study used a descriptive design with purposive sampling and utilized a KAP survey instrument. To be included in the study, participants had to self-report that they were currently practicing physical therapy. Participants were recruited from OMPT programs accredited through the American Association of OMPT and the American Board of Physical Therapy Residency and Fellowship Education; of these 35 programs, 9 participated in the study. Additionally, participants were recruited from outpatient orthopedic clinics using a pass-along approach—the survey was allowed to be forwarded only by participants to other physical therapists. The survey was digitally formatted in Google Forms and emailed to participants as a hyperlink. Informed consent was obtained from participants, as required for protection of human participants.
Sample Size Calculation
To determine the sample size needed to strongly represent the OMPT population, the total population of physical therapists within OMPT was estimated based on reports from the 9 participating OMPT programs; the sum of all reported was 1213 persons. Assuming that this represented 26% of the population (ie, 9 of 35 OMPT programs), it was estimated that the total population of OMPT was 4665 persons. Based on the author’s preliminary interview of physical therapists within OMPT, it was assumed that 70% of the OMPT population provided some level of lifestyle screening and education to their patients. Using the following formula, it was determined that a sample size of 303 subjects was needed to strongly represent this population. The formula used was n = (Z2 × P[1 – P])/e2 where “Z” is the value from standard normal distribution corresponding to desired confidence level (Z = 1.96 for 95% CI); “P” is expected true proportion (P = .70); “e” is the desired precision (half-desired CI width).
Operational Definitions
Constructs
1. Knowledge: The participant’s perceived level of confidence and competence in talking to their patients about lifestyle topics. 2. Attitude: The participant’s beliefs about the relevance and importance of lifestyle screening and education in health care and physical therapy. 3. Practice: The participant’s frequency of providing lifestyle screening and education to their patients.
Variables
1. Lifestyle Behaviors: Those elements of a person’s daily behavior that are proven to influence chronic diseases. Exercise: The topic of habitual exercise as it pertains to the treatment and prevention of LRCD. Diet: The topic of habitual food intake as it pertains to the treatment and prevention of LRCD. Smoking: The topic of habitual cigarette smoking and how it pertains to the treatment and prevention of LRCD. Alcohol: The topic of habitual alcohol consumption and how it pertains to the treatment and prevention of LRCD. Water: The topic of habitual water intake and how it pertains to the treatment and prevention of LRCD. Sleep: The topic of the habitual amount of sleep received and how it pertains to the treatment and prevention of LRCD. Stress: The topic of a person’s perceived level of stress and how it pertains to the treatment and prevention of LRCD. 2. Practice Total Score: The variable created by combining all the responses for individual lifestyle topics related to the construct Practice. 3. Knowledge Total Score: The variable created by combining all the responses for individual lifestyle topics related to the construct Knowledge. 4. Professional Demographics: Denotes the participant’s self-reported professional characteristics. PT Degree: Denotes the self-reported highest physical therapy degree earned—Bachelor’s (BPT), Master’s (MPT), or Doctorate (DPT). Practice Status: Denotes the self-reported information on whether or not a person is currently practicing physical therapy. Years in Practice: Denotes the self-reported range of years spent practicing physical therapy to date— <1, 1-3, 4-10, 11+ years. Practice Setting: Denotes the self-reported setting where a person practiced physical therapy—outpatient, inpatient, home-health, or other. Patient Population: Denotes the self-reported primary patient population seen while practicing physical therapy—pediatrics, adults, geriatrics, or other. Advanced Degrees: Denotes the self-reported advanced degrees earned in addition to a physical therapy degree—PhD, DSc, or other. PT Certifications: Denotes the self-reported PT-related certifications earned—Certified Manual Physical Therapist (CMPT), Certified Orthopedic Manipulative Therapist (COMT), Fellow of the American Academy of OMPT (FAAOMPT), Orthopedic Clinical Specialist (OCS), or other.
Metrics
1. Combined High Scores (CHS): The combination of participants’ responses on the 2 higher ratings on the 5-point Likert scale; 2. Neutral Scores (NS): The middle rating on the 5-point Likert scale; 3. Combined Low Scores (CLS): The combination of participants’ responses on the 2 lower ratings on the 5-point Likert scale; 4. Average CHS (ACHS): The average of all the CHS for all participants on the 7 individual lifestyle topics; 5. Average NS: The average of all the NS for participants on the 7 individual lifestyle topics; and 6. Average CLS (ACLS): The average of all the CLS for all participants on the 7 individual lifestyle topics.
Measurement Methods and Data Collection
Instrument Design
This study utilized a KAP survey instrument created by the investigators to investigate the subjects’ KAP toward lifestyle screening and education. The survey instrument comprised questions that were primarily measured using a modified Likert Scale. The questions (8 items) pertaining to Practice asked the participant to indicate “how much” they talked to their patients about lifestyle topics in general and each lifestyle topic individually (eg, Exercise, Diet, Smoking, Alcohol, Water, Sleep, and Stress). Similarly, the questions (8 items) pertaining to Knowledge asked the participant to indicate their level of confidence and competence in talking to their patients about lifestyle topics in general and each lifestyle topic individually. There were 4 additional questions pertaining to Knowledge that asked the participant to indicate how much their professional education—both in physical therapy school and after—had covered lifestyle topics in general and Diet specifically. There were 2 questions pertaining to Attitude that asked the participants to indicate how important they felt lifestyle screening was and if physical therapists should perform lifestyle screening. There were 8 demographic questions that did not utilize the Likert scale.
Instrument Validation
Content and face validity of the survey instrument were established through a literature review, which determined the primary lifestyle behaviors that contribute to LRCD. Additionally, pilot testing was done with a panel of orthopedic manual physical therapists (n = 7) who took the survey and provided feedback. The pilot testers rated the survey in 6 different categories (eg, first impression, writing tone, terminology and vocabulary, clarity of writing, survey length/time needed, and content) on a 5-point Likert scale. All participants either rated the instrument as “Good” or “Very Good” in each category. Participants also provided open-ended feedback. Based on the open-ended feedback, the instrument was adjusted to use only the 5-point Likert scale for all KAP questions; the suggested length of time to take the survey, which was mentioned in the introduction of the survey, was adjusted to less than 8 minutes, and, the purpose of the study was clarified in the introduction.
Construct reliability was determined using a Cronbach’s alpha analysis for each construct—KAP. The results revealed high internal consistency for all constructs: Knowledge (α = .845), Attitude (α = .894), and Practice (α = .853).
Data Analysis
Data analysis was done using IBM SPSS Statistic 27 software. Descriptive statistics were used to report on the frequencies. Comparative statistics were used to determine if certain group characteristics affected participants’ responses. Nonparametric comparison tests (Kruskal Wallis and the Mann–Whitney U) were used for ordinal and nominal data. Parametric comparison tests (one-way ANOVA and a Tukey’s post hoc) were used for continuous data.
Results
Descriptive Statistics
Demographics
There were 155 responses to the survey, and one participant did not complete any part of the survey. Of the 154 completed surveys, all participants reported that they were currently practicing physical therapy. The sample size calculated as needed to strongly represent this population was 303 persons; thus, the collected sample size of 155 participants was considered of moderate statistical strength.
Participant Demographics, n = 155.
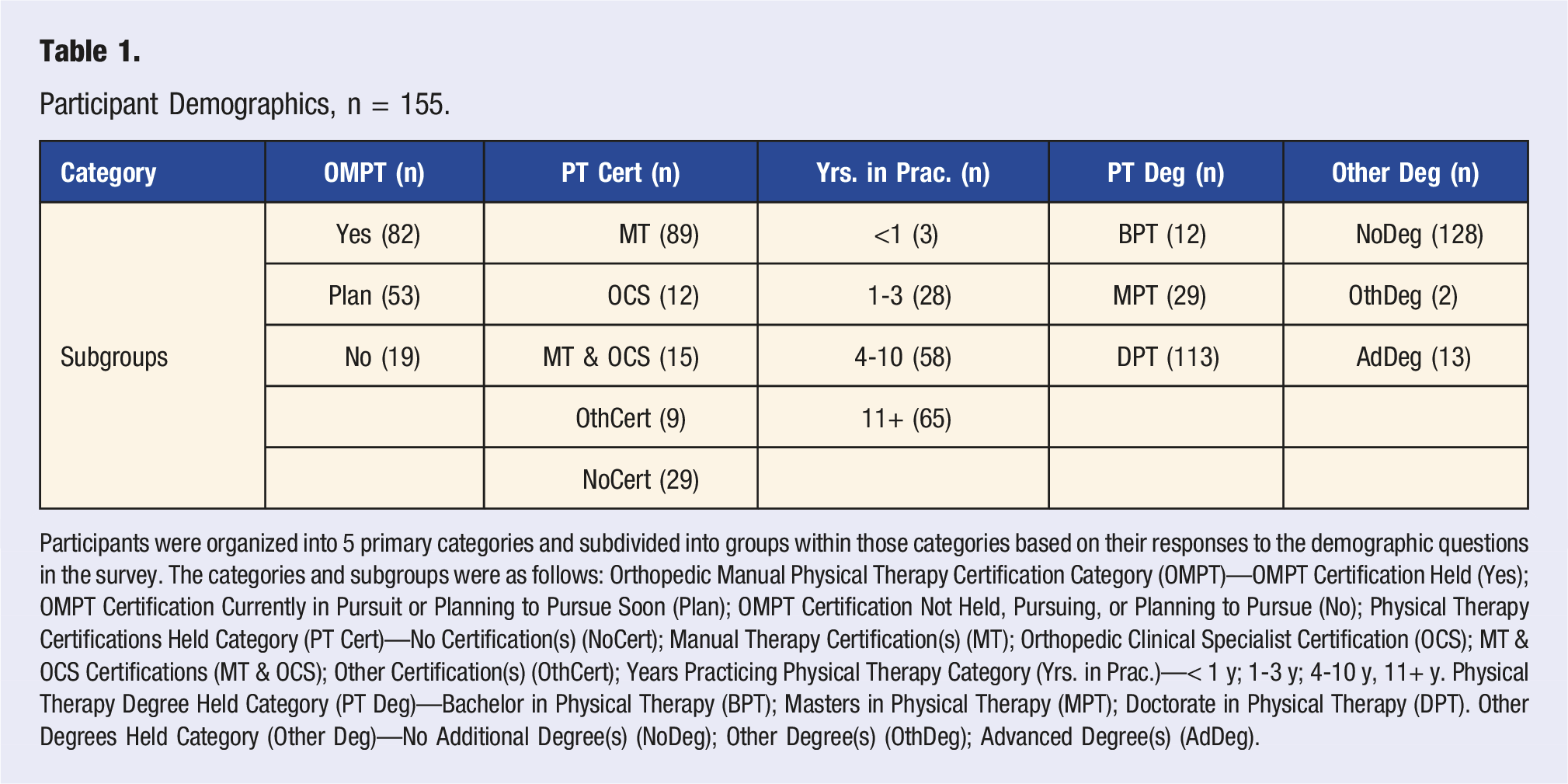
Participants were organized into 5 primary categories and subdivided into groups within those categories based on their responses to the demographic questions in the survey. The categories and subgroups were as follows: Orthopedic Manual Physical Therapy Certification Category (OMPT)—OMPT Certification Held (Yes); OMPT Certification Currently in Pursuit or Planning to Pursue Soon (Plan); OMPT Certification Not Held, Pursuing, or Planning to Pursue (No); Physical Therapy Certifications Held Category (PT Cert)—No Certification(s) (NoCert); Manual Therapy Certification(s) (MT); Orthopedic Clinical Specialist Certification (OCS); MT & OCS Certifications (MT & OCS); Other Certification(s) (OthCert); Years Practicing Physical Therapy Category (Yrs. in Prac.)—< 1 y; 1-3 y; 4-10 y, 11+ y. Physical Therapy Degree Held Category (PT Deg)—Bachelor in Physical Therapy (BPT); Masters in Physical Therapy (MPT); Doctorate in Physical Therapy (DPT). Other Degrees Held Category (Other Deg)—No Additional Degree(s) (NoDeg); Other Degree(s) (OthDeg); Advanced Degree(s) (AdDeg).
KAP Frequencies
Practice: Participants Self-Reported Frequency of Talking to Patients about Lifestyle Topics, n = 155.
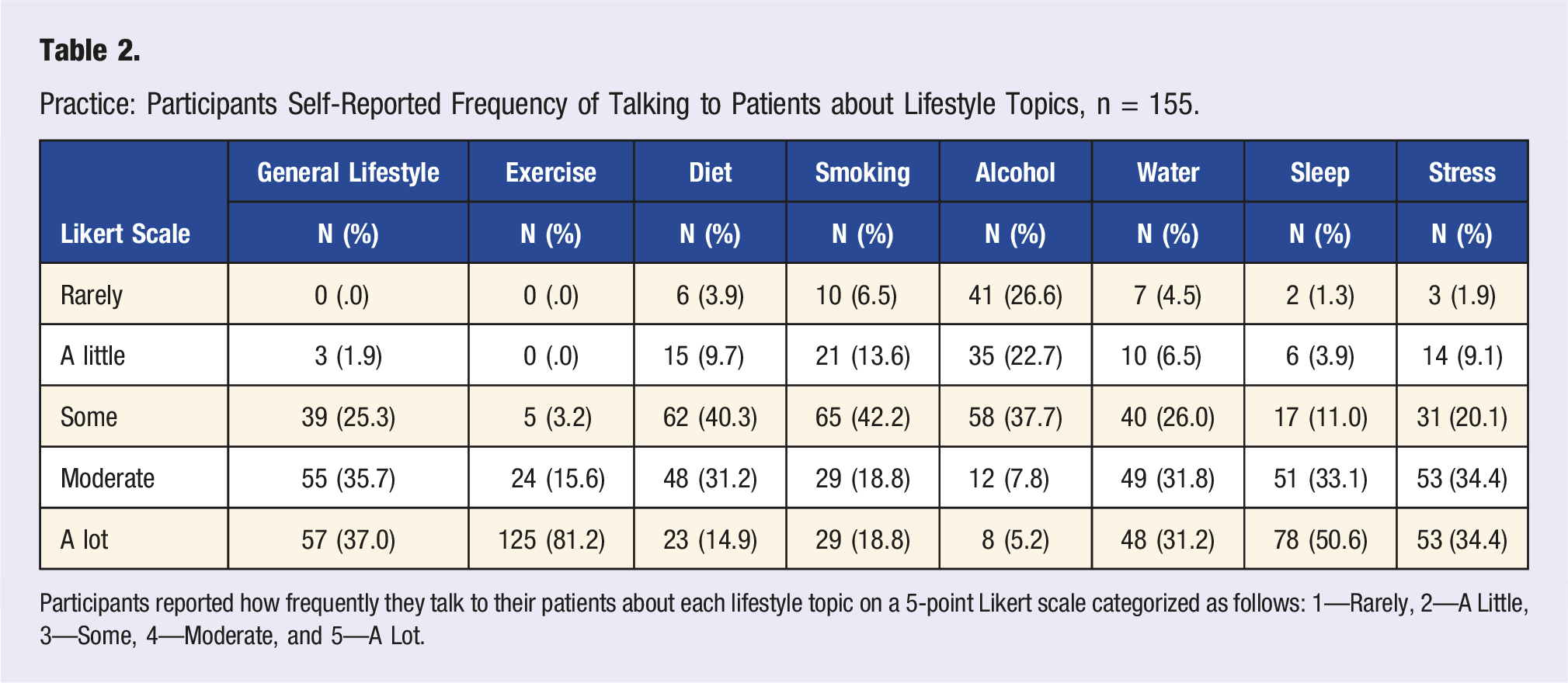
Participants reported how frequently they talk to their patients about each lifestyle topic on a 5-point Likert scale categorized as follows: 1—Rarely, 2—A Little, 3—Some, 4—Moderate, and 5—A Lot.
Knowledge: Participants Self-Reported Confidence and Competence Talking to Patients about Lifestyle Topics, n = 155.
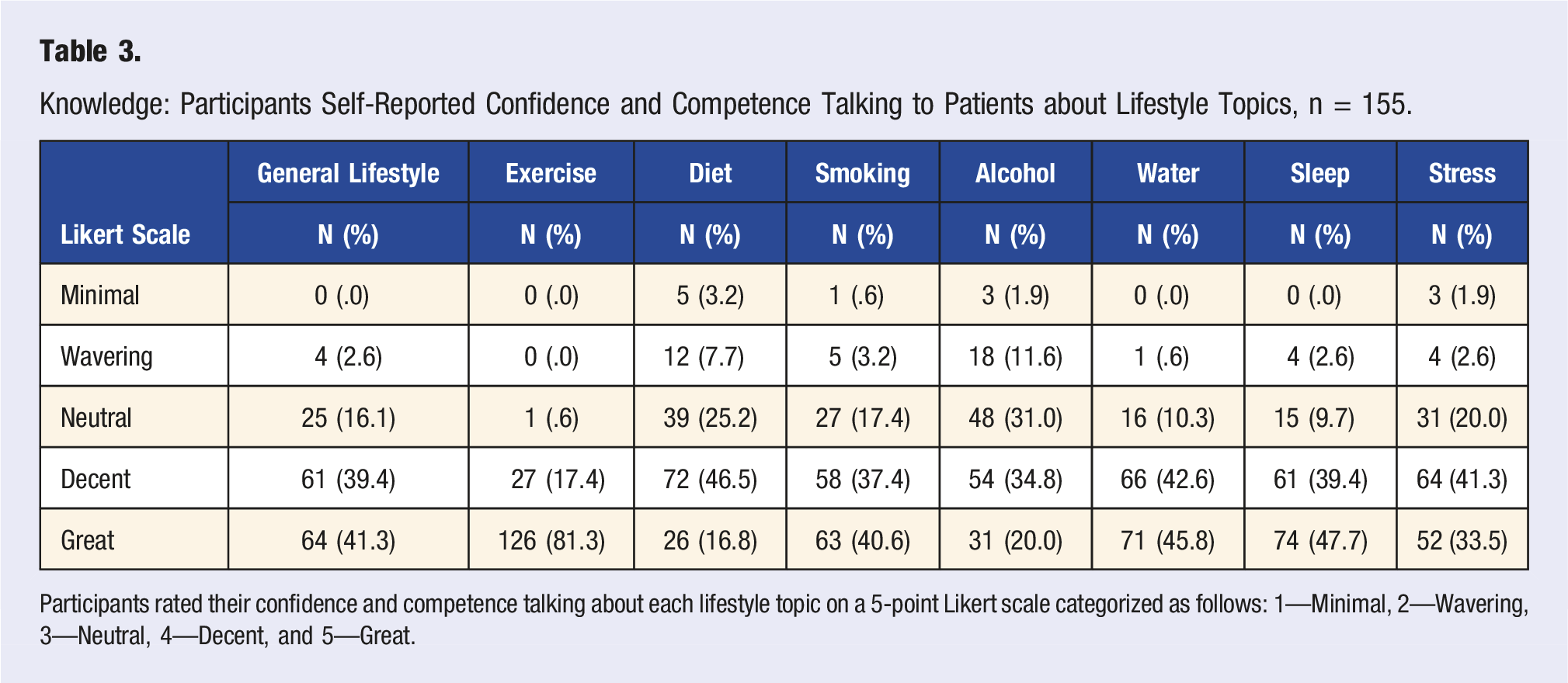
Participants rated their confidence and competence talking about each lifestyle topic on a 5-point Likert scale categorized as follows: 1—Minimal, 2—Wavering, 3—Neutral, 4—Decent, and 5—Great.
In fact, no individual lifestyle topic had Knowledge CHS (Table 3) lower than its Practice CHS. In general, Knowledge CHS were high (no lower than 55.0%) and the Knowledge ACHS for all individual lifestyle topics was 78.1% (n = 121), which was quite a bit higher than the previously mentioned Practice ACHS (n = 90, 58.1%).
As may be expected, Diet (n = 21, 13.5%), Smoking (n = 31, 20.0%), and Alcohol (n = 76, 49.0%) had the highest Practice CLS. However, Diet (n = 62, 40.0%) and Smoking (n = 65, 41.9%) had fairly high Practice NS, while Alcohol stood out with the highest Practice CLS (n = 76, 49.0%) by a notable margin, making the low Practice of Alcohol screening and education an outstanding finding of this study.
Sleep (P: n = 129, 83.2%; K: n = 135, 87.1%), Stress (P: n = 106, 68.4%; K: n = 116, 74.8%), and Water (P: n = 97, 62.6%; K: n = 137, 88.4%) all had fairly high Practice and Knowledge CHS. However, Water showed a notable disparity between its Practice (n = 97, 62.6%) and Knowledge (n = 137, 88.4%) scores, indicating that potentially, this topic was under-discussed with patients based on the clinician’s knowledge of the topic.
There was not much disparity between the CHS (n = 55, 35.5%), NS (n = 58, 37.4%), and CLS (n = 41, 26.5%) for physical therapy school coverage of lifestyle topics in general (Table 3). However, physical therapy school coverage of Diet showed notably higher NS (n = 58, 37%) and CLS (n = 73, 47.1%) than CHS (n = 28, 18.1%), indicating that participants did not perceive receiving much education on Diet while they were in physical therapy school.
Knowledge and Attitude: Participants Self-Reported Education and Attitude Towards Lifestyle Topics, n = 155.
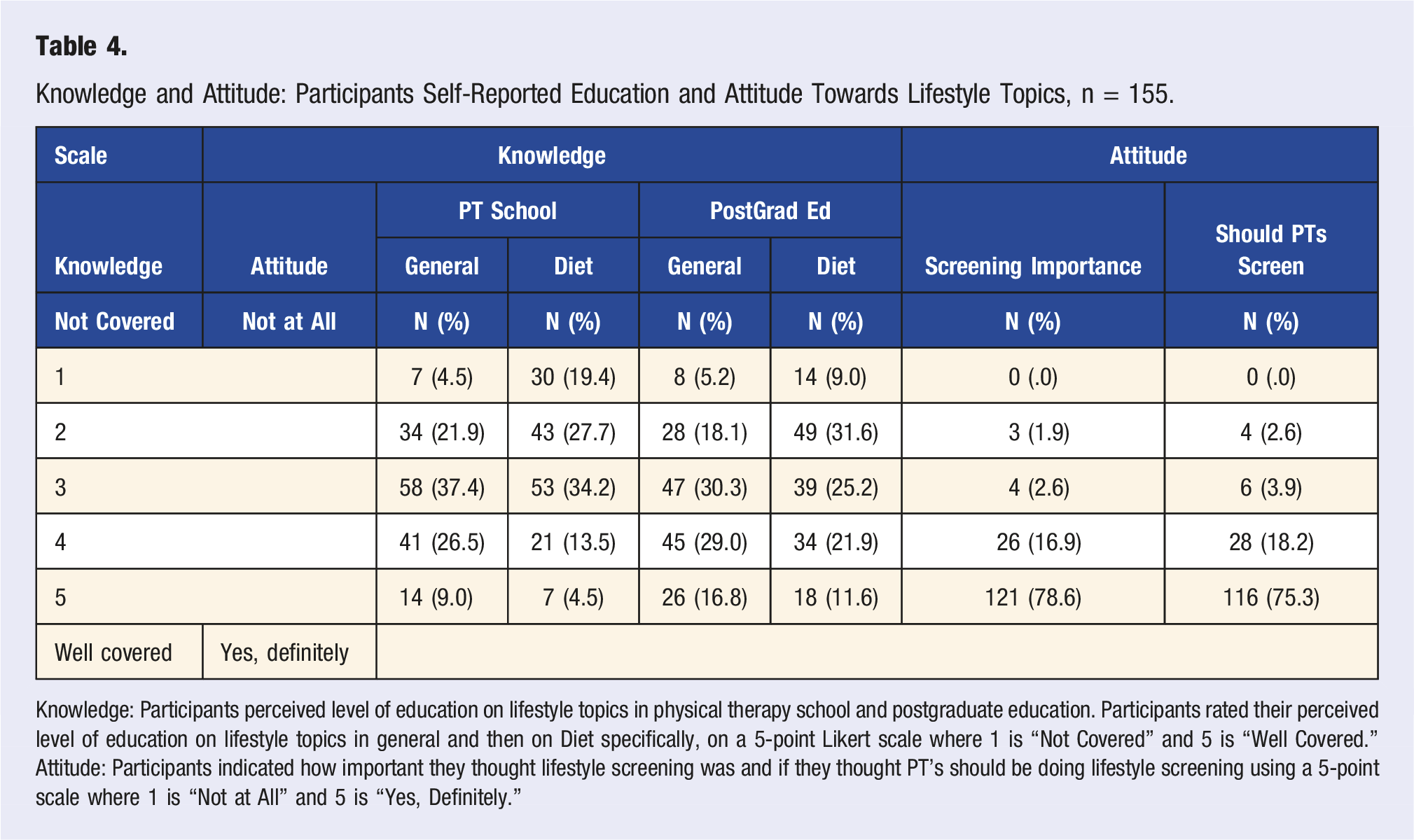
Knowledge: Participants perceived level of education on lifestyle topics in physical therapy school and postgraduate education. Participants rated their perceived level of education on lifestyle topics in general and then on Diet specifically, on a 5-point Likert scale where 1 is “Not Covered” and 5 is “Well Covered.”
Attitude: Participants indicated how important they thought lifestyle screening was and if they thought PT’s should be doing lifestyle screening using a 5-point scale where 1 is “Not at All” and 5 is “Yes, Definitely.”
The physical therapists represented in this study had a notably positive Attitude in favor of lifestyle screening and education (Table 4). The majority of participants believed that lifestyle screening and education was important (n = 147, 94.8%, CHS) and that physical therapists should be doing it (n = 144, 92.9%, CHS). This nearly unanimous positive Attitude did not seem to be supported by the Practice ACHS (n = 90, 58.1%) nor the Knowledge ACHS (n = 121, 78.1%). Instead, there seemed to be a slowly dissolving idealism, as Attitude exceeded Knowledge and Knowledge exceeded Practice.
Between Subgroup Comparisons
Multiple Comparisons: Mann–Whitney U Tests, n = 155.
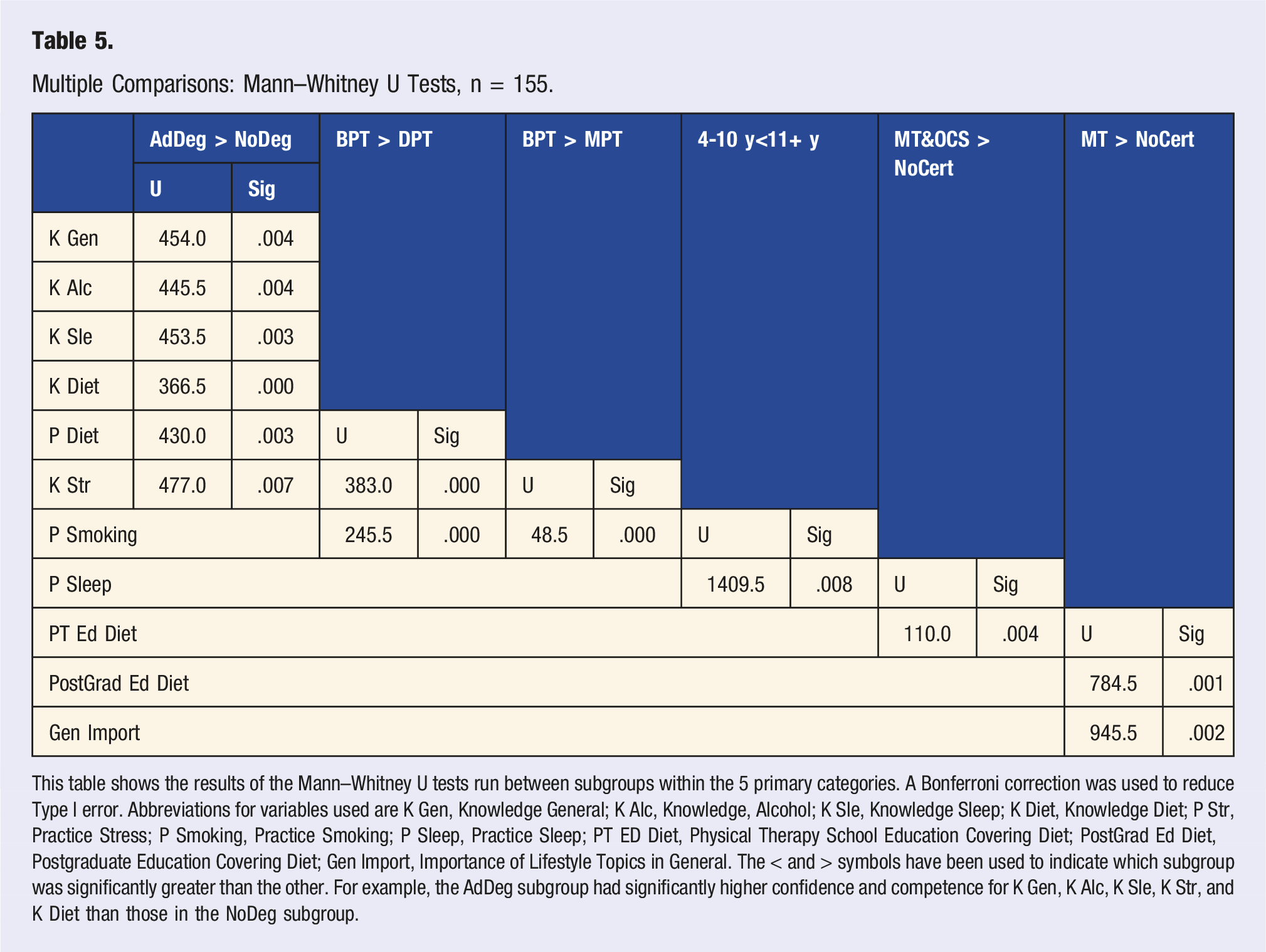
This table shows the results of the Mann–Whitney U tests run between subgroups within the 5 primary categories. A Bonferroni correction was used to reduce Type I error. Abbreviations for variables used are K Gen, Knowledge General; K Alc, Knowledge, Alcohol; K Sle, Knowledge Sleep; K Diet, Knowledge Diet; P Str, Practice Stress; P Smoking, Practice Smoking; P Sleep, Practice Sleep; PT ED Diet, Physical Therapy School Education Covering Diet; PostGrad Ed Diet, Postgraduate Education Covering Diet; Gen Import, Importance of Lifestyle Topics in General. The < and > symbols have been used to indicate which subgroup was significantly greater than the other. For example, the AdDeg subgroup had significantly higher confidence and competence for K Gen, K Alc, K Sle, K Str, and K Diet than those in the NoDeg subgroup.
Multiple Comparisons: One-Way ANOVA Tukey’s Post Hoc Test, n = 155.
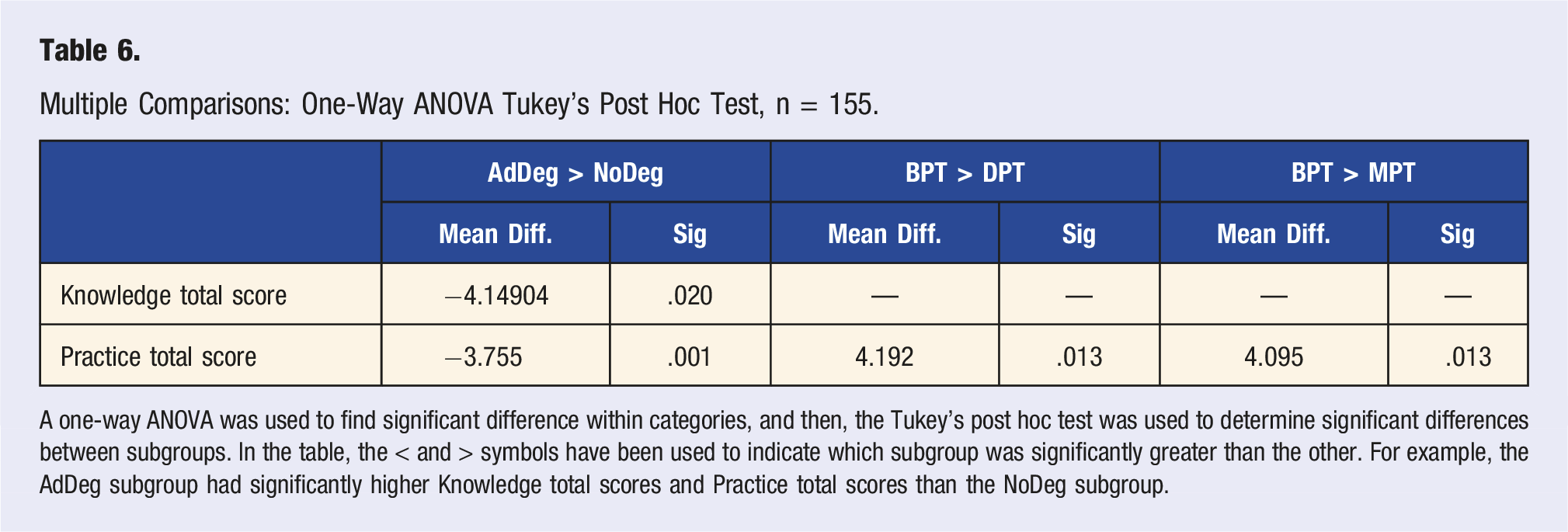
A one-way ANOVA was used to find significant difference within categories, and then, the Tukey’s post hoc test was used to determine significant differences between subgroups. In the table, the < and > symbols have been used to indicate which subgroup was significantly greater than the other. For example, the AdDeg subgroup had significantly higher Knowledge total scores and Practice total scores than the NoDeg subgroup.
Discussion
It is well established that lifestyle behavior change must be utilized in the prevention, management, and treatment LRCD.8-52,61 Yet, the gap between what is known in the literature and what is being done in healthcare practice needs to be understood.35,45 One study shows the percentage of physicians who self-reported counseling at least 75.0% or more of their patients on Smoking was 78.7%, Physical Activity was 54.0%, Diet was 54.6%, and Alcohol was 44.8%. 62 However, several other studies have found that only a small percentage (5.0-34.0%) of patients reported receiving any lifestyle screening and education from physicians.63-69 Interestingly, in both a physician-reported 62 and a patient-reported 65 study, alcohol counseling was provided the least, which is consistent with the findings of this study where only 12.9% of physical therapists reported talking to their patients about alcohol frequently, making alcohol the most disregarded lifestyle topic over several studies.
However, the work of motivating lifestyle behavior change does not fall to physicians alone. In fact, although physician support is crucial for patient buy-in, physicians may not be best-placed to facilitate lifestyle behavior change programs. One report demonstrated that physicians use brief lifestyle education with their patients and feel that the individualized plans that some patients want are outside the role of the physician. 66 Another study showed that 54.0% of physicians feel they do not have adequate time to provide behavior change education. 70 In contrast, the profession of physical therapy is well placed to facilitate lifestyle behavior change.36,43,51–61,71 The existing treatment approach in physical therapy allows a significant amount of patient contact time and physical therapists already provide individualized care plans that emphasizes behavior change through exercise prescription and activity modification.45,63 Moreover, the findings of this study indicate that some physical therapists are already providing a certain amount of lifestyle screening and education.
Admittedly, there are limitations to the findings of this study. The purpose of this study was to provide a foundational study design for continued investigation of the KAP of rehabilitation professionals toward lifestyle medicine across a variety of settings, specialties, and professions. Thus, the population sample of this study is narrow leading to poor generalizability of these results.
Further, a notable percentage of participants held or were pursuing advanced certifications and specialties, advanced degrees, or both (n = 148, 95.5%). This bias toward advanced education might have created a bias in favor of lifestyle screening and education. Certainly, the results of this study suggested that holding an advanced degree increases the Knowledge and Practice of these subjects toward lifestyle screening and education. This is also supported in other research showing that continued education improves the knowledge and confidence of physicians toward providing patient education on lifestyle topics.72,73 Therefore, to gain a broader understanding of the KAP of physical therapists toward lifestyle screening and education, a less biased and more heterogeneous sample needs to be pursued through future research.
Moreover, there are many questions about the findings of this study that are yet to be answered, such as what barriers may have kept participants from providing lifestyle screening and education. Other researchers have proposed that the barriers faced by physicians in regard to lifestyle counseling include the following: insufficient training, knowledge, and skills67,68; low motivation due to personal habits67,70,74,75; lack of time64,70; and low confidence.67-69,73,75
The findings of this study did not support the idea that low confidence was a barrier for these subjects. However, it could be speculated that barriers related to the construct Attitude, such as personal lifestyle habits, were at play in cases where the Knowledge CHS were notably higher than the Practice CHS, such as in the case of Alcohol (n = 65, disparity between scores) and Smoking (n = 63, disparity between scores). Many studies have shown that providers were less likely to counsel patients on lifestyle topics if they themselves were not practicing certain lifestyle behaviors.66,70,74,75 Unfortunately, participants in this study were not given the opportunity to demonstrate their Attitude toward individual lifestyle topics or their personal lifestyle practices—any future research should correct for this.
Continued research on this topic could be taken in many directions which include but are not limited to a replication study to investigate a different niche or more heterogeneous population, or a new design with the purpose of discovering the barriers that keep physical therapists and other rehabilitation professionals from implementing lifestyle medicine into practice.
Conclusion
The KAP of rehabilitation professionals toward lifestyle screening and education should be considered as important if lifestyle-focused rehabilitation plans are to become part of the standard system of care for the treatment of LRCD. This study demonstrated a strong acceptance of lifestyle screening and education within the niche of OMPT and provides a foundational design for further investigation of the KAP of other rehabilitation professionals. Given the prevalence of lifestyle-related chronic diseases, it could be argued that all healthcare professionals should have a greater understanding of lifestyle medicine. Thus, this study model could be modified to investigate a variety of other healthcare professions as well.
As evidenced by disease prevalence studies, the prevention, treatment, and management of LRCD are presently the greatest rehabilitation need of society. Yet, no single rehabilitation profession as a whole has attempted to address this need through lifestyle medicine. It has been observed that physical therapy is well placed to expand further into lifestyle medicine. However, historically physical therapy has focused primarily on exercise prescription and activity modification and has placed little emphasis on the other aspects of lifestyle. It is the hope of the investigators that physical therapists will expand their perspective and be viewed as more than just exercise and movement specialists, but rather as prevention and recovery specialists who use exercise, movement, and all aspects of lifestyle to help prevent disease, guide healing, and restore health.
Supplemental Material
sj-pdf-1-ajl-10.1177_15598276211028557 – Supplemental Material for Knowledge, Attitude, and Practice of Orthopedic Manual Physical Therapists Toward Lifestyle Screening and Education: A Descriptive Study
Supplemental Material, sj-pdf-1-ajl-10.1177_15598276211028557 for Knowledge, Attitude, and Practice of Orthopedic Manual Physical Therapists Toward Lifestyle Screening and Education: A Descriptive Study by Jillian M. Zollinger and Sozina D. Katuli in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
The investigators appreciate the input, support, and encouragement of all the faculty and staff from the School of Rehabilitation Sciences at Andrews University and the participation of the nine OMPT programs in addition to all who helped disseminated the survey instrument.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
IRB: Andrews University; Address: 8488 E Campus Circle Dr Room 234 – Berrien Springs, MI 49104-0355; Tel: (269) 471-6361; Email:
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.