
Abstract
Changes in disease patterns from predominantly infectious to predominantly chronic diseases in Australia, in line with economic development throughout the developed world, have led to the need for changes in conventional health practice. This has resulted in a movement toward an evidence-based discipline of lifestyle medicine incorporating aspects of both public health and clinical medicine, aimed at moderating lifestyle and environmentally based etiologies. A professional association, postgraduate and continuing professional development training, working text, interactive Web site, and annual conference, as described here, are designed to complement conventional medical knowledge and practices. Changes to the Australian health system, which operates on a dual public/private model have made this approach more feasible and continue to be adapted to allow a more comprehensive approach to lifestyle-related health problems.
As with other advanced countries, the obesity epidemic began in the late 1970s and early 1980s in Australia, signaling the end of a “sweet spot” in human advancement.
Introduction
Once called “The Lucky Country,” 1 there’s little doubt that Australia, a relatively “new” colony, after little more than 2 centuries of European settlement, punches above its weight in the health stakes. With a longevity among the highest in the world, a highly performing health system, and a notable absence of the life-threatening communicable diseases that plague countries in the vicinity, 2 Australia can count its blessings.
But as with many postindustrial economies, future portents are less encouraging. The rise in chronic diseases and potential increase in disability-adjusted life years (DALYs) accompanying this 3 are causing experts to question whether early predictions that morbidity would be compressed into the latter years of an extended lifetime with advanced economic development 4 may have been premature.
Forewarning of this has come through the big rise in obesity in recent years. 5 As with other advanced countries, the obesity epidemic began in the late 1970s and early 1980s in Australia, signaling the end of a “sweet spot” 6 in human advancement. This is shown cross-sectionally in a range of countries by the rapid rise in healthy weight with increased income up to a BMI of ~25 kg/cm2, then a leveling off beyond this (Figure 1). Until that time, increases in consumption required to fuel the growth model of economics driving the postdepression world had benignly increased mean body weight within a healthy range (ie, BMI = 19-25). Beyond this point, however, increased consumption (of energy-dense foods and effort-saving technology) has resulted in a net positive energy balance pushing the national mean BMI in Australia to an unprecedented 26.7 kg/cm2—among the highest in the world. 7
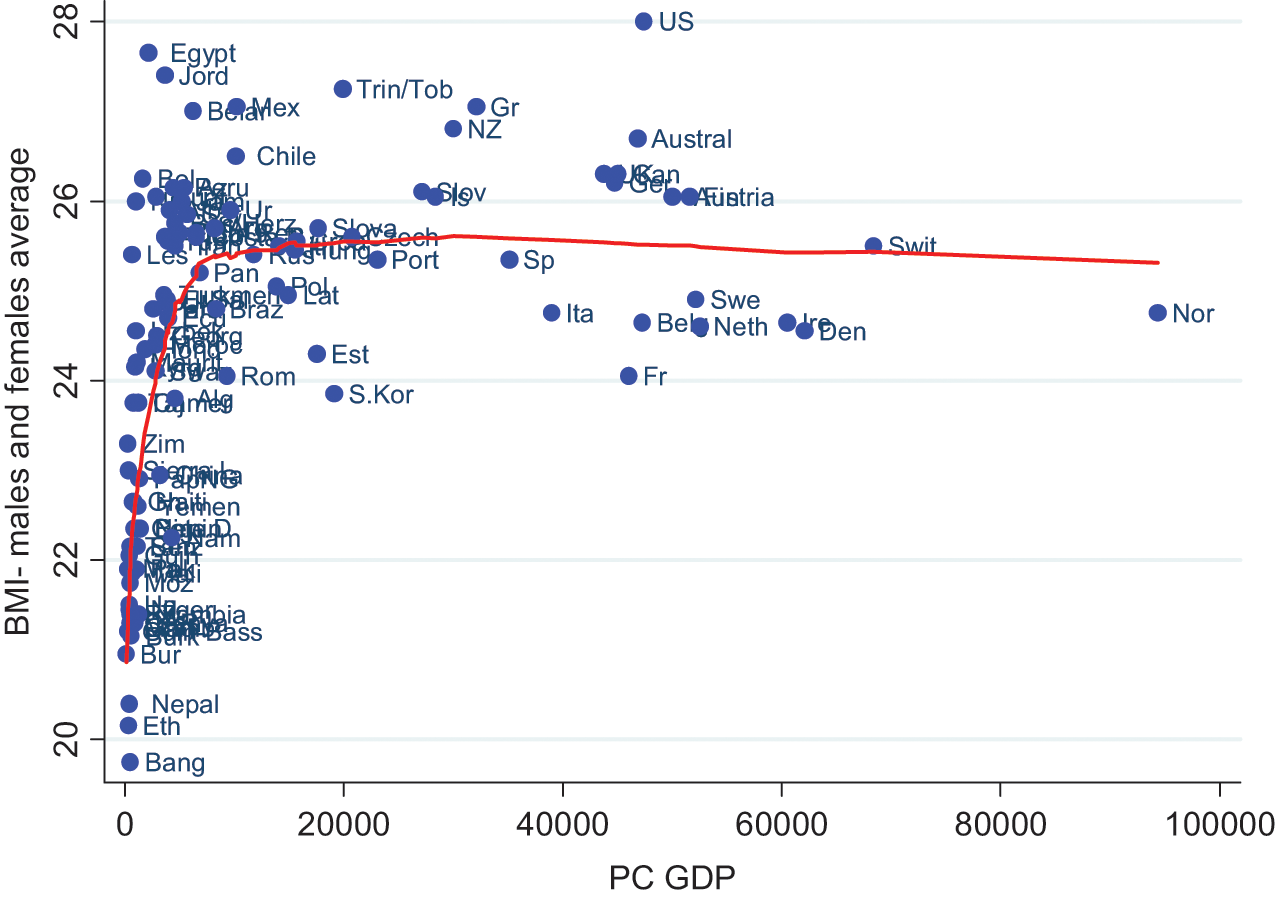
Average BMI by Economic Growth (GDP) With Lowess Smoothing Curve for 180 Countries in 2007.
Changing Patterns of Disease
With obesity has come a rise in the relative importance of chronic, or noninfectious, compared with acute, or infectious, diseases. 8 Although the death rates from heart disease, cancer, and chronic obstructive pulmonary disease continue to decline and deaths from infectious diseases have plummeted to a negligible level, the burden of these diseases (DALYs) as well as that from diabetes, mental disorders, injuries, and musculoskeletal problems remains high, and in many cases (eg, diabetes) is increasing dramatically. 3 Indigenous health is also a problem, with longevity being some 17 years less than that for the nonindigenous population and DALYs from all causes much higher. 2 The socioeconomic gradient in chronic disease prevalence also remains a concern and exceeds that of more egalitarian societies such as the Scandinavian countries, Japan, and Northern Europe. 9
Despite the successes, this changing pattern of diseases has led to an increase in health costs across the board. Hospital admissions in Australia have grown by 37% over the past decade, and GP visits are also on the rise. Elective surgery waiting lists have blown out from an average of 28 to 34 days in the past 5 years. 3 In this regard, Australia is not unique and reflects the experiences of countries developing past the “epidemiological transition,” 10 where the prevalence of lifestyle and environmentally related chronic diseases begins to surpass that associated with microbial infection.
Shifts in Disease Management
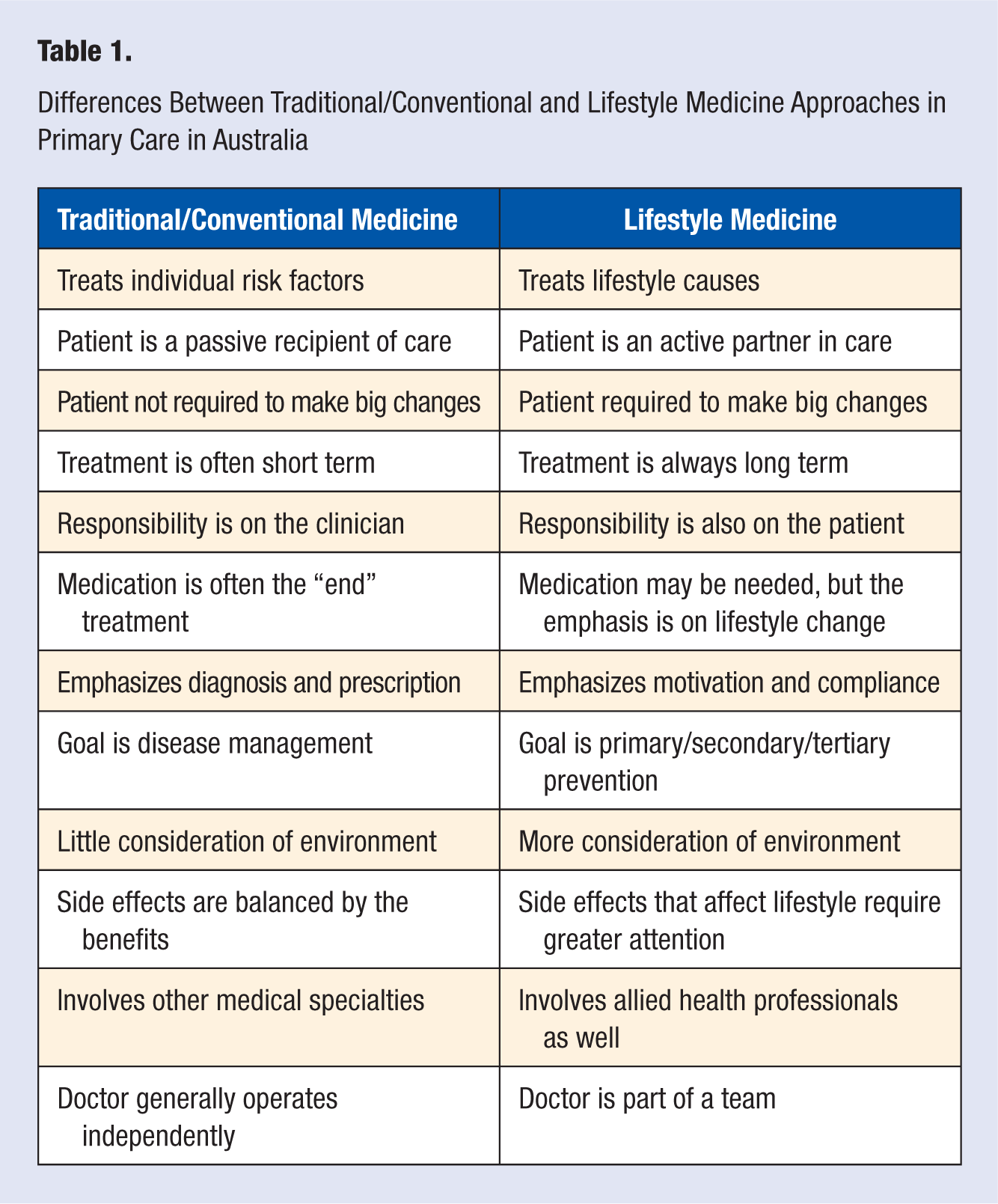
The transition from infectious to chronic diseases in developed countries like Australia has led to a need for a reassessment of the medical model for managing these problems. The need for a greater emphasis on lifestyle, and the environment driving this, means neither clinical nor public health approaches alone are sufficient, and hence, an approach integrating both becomes more appealing. Lifestyle medicine is a new way of doing this, incorporating in particular a greater emphasis on self-care and self-management, and this involves the patient as an active partner, applying his or her knowledge continuously to the care process. To this end, we have defined Lifestyle Medicine as “the application of environmental, behavioural, medical and motivational principles to the management, including self care and self management, of lifestyle-related health problems in a clinical and/or public health setting (p. 1).” 11 Differences between this and the conventional medical approach, while acknowledging that both are complementary rather than competitive, are summarized in Table 1.
Differences Between Traditional/Conventional and Lifestyle Medicine Approaches in Primary Care in Australia
An epidemiological approach to chronic disease, that is, identifying the cause of the causes, 12 shows the need for a multilevel approach such as shown in Figure 2. It should be clear from this, that lifestyle medicine requires a broad palette of tactics from environmental action to individual behavior change. At the distal end of causality, issues that are as apparently unrelated as economic growth need to be considered. 13 Growth for growth’s sake, resulting in consumption beyond a point of need, is an obvious cause of obesity (and thus chronic disease) as also accompanying environmental factors such as climate change. 14 And although individual approaches to obesity and the chronic diseases spawned from this are vital, a lifestyle medicine approach should see the limitations of these within the broader context.
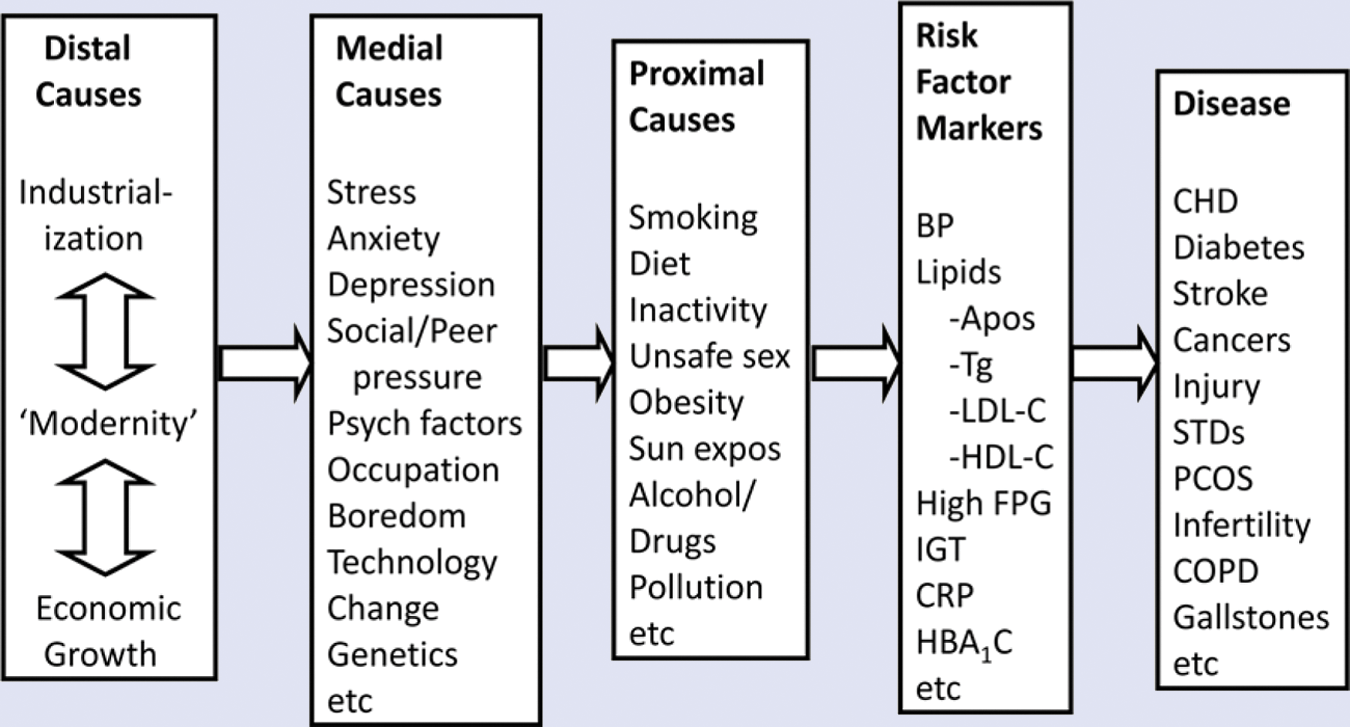
An Epidemiological Approach to the Hierarchy of Causality in Modern Chronic Diseases.
At the more medial point of causality, lifestyle medicine, through appropriate disciplines, both medical and nonmedical, needs to deal with the facilitating causes of health-related behavior, such as stress management, peer pressure, inequality, and so on. Wilkinson and Pickett, 9 for example, show a clear link between inequality in a country, as expressed by the ratio between the top and bottom 20% of income earners, and a wide range of health and social problems. And while these may mediate more proximal causes such as overeating, inactivity, and so on (as shown in Figure 2), which are typically the core of a lifestyle-change program, these medial causes also need to be considered if lifestyle medicine is to play more than just a superficial role in disease management.
At the more proximal level, risk factors and markers still need to be addressed using the existing arsenal of primary care practitioners, from pharmacotherapy to behavior modification. Add to this the role for secondary and tertiary prevention, and lifestyle medicine covers a broad and diverse canvas.
A text written for Australian lifestyle medicine practitioners in 2008 11 was initially intended to cover just the proximal areas of chronic disease causality with chapters originally planned mainly on exercise, nutrition, and weight control. With contributions from around the Australian health community, however, this expanded to 22 chapters in the first edition and now to 26 in a revised second edition. Research findings, as well as new thinking in the interim have expanded the scope of the lifestyle medicine brief. The discovery, for example, of a low-grade form of systemic inflammation (“metaflammation”) 15 associated with most, if not all modern lifestyle-related chronic disease, has changed the focus of lifestyle and environmentally related etiology. Our understanding of gastrointestinal disorders, sexual problems, dental health, and auditory function as lifestyle-related and environmentally related health issues have all led to an expansion of the field and the need for the development of practice guidelines for lifestyle medicine. As these require formal acknowledgment and development at the national level, however, the Australian Lifestyle Medicine Association (ALMA) has developed a draft set of practice principles in the interim (see Table 2). Alternative processes such as the use of cartoons (Figure 3) are also being utilized as part of the professional and patient education process. An interactive Web site with professional tools (www.lifestylemedicine.com.au) is also available for members.
Practice Principles for Lifestyle Medicine of the Australian Lifestyle Medicine Association (ALMA) a
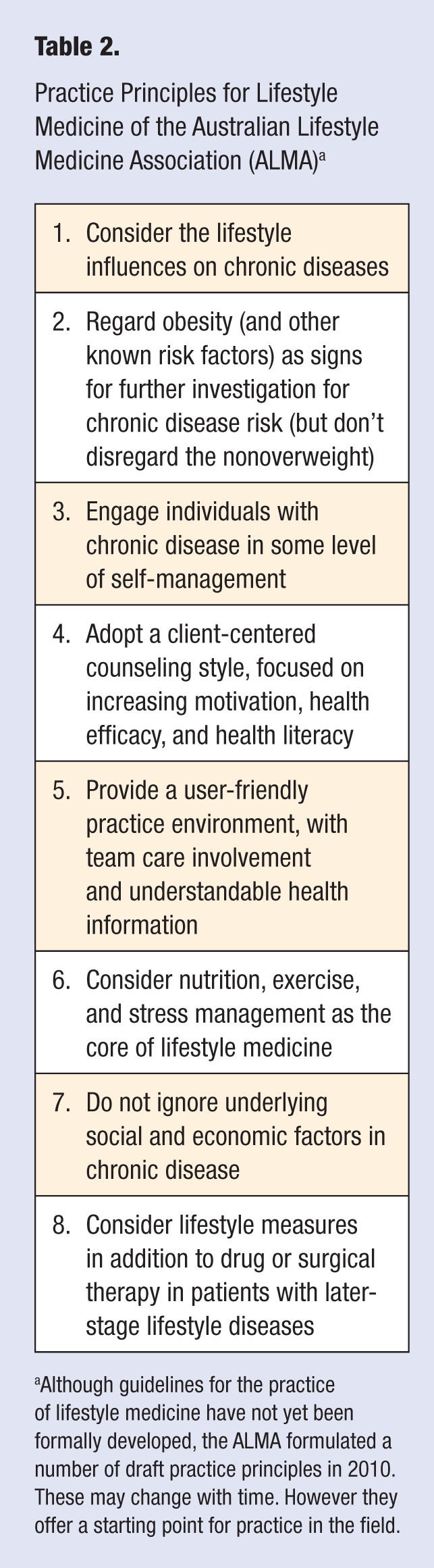
Although guidelines for the practice of lifestyle medicine have not yet been formally developed, the ALMA formulated a number of draft practice principles in 2010. These may change with time. However they offer a starting point for practice in the field.
Cartoons as a Means of Raising Awareness in Lifestyle Medicine.
The health care system in Australia currently enables publicly funded care plans and team care arrangements incorporating medical and allied health professionals. This allows the greater flexibility required for a more time-consuming lifestyle medicine approach in clinical practice. But a streamlining of the bureaucracy and expansion of modes of function is now necessary to keep up with the demands of exploding chronic disease care. To meet this, the annual ALMA conference, which was first convened in Sydney in 2008, involves a reversion to former times—no concurrent sessions, so all disciplines have to interact—and short “tales from the trenches,” giving practical examples of evidence-based treatments on lifestyle management. Certified Professional Development (CPD) training for GPs and other primary care workers is also available around the country, with more than 25% of the country’s practicing GPs having attended at least 1 of the current 6 levels on offer. An academic connection, with multidisciplinary online postgraduate training in lifestyle medicine is available through Southern Cross University on the North coast of New South Wales (see www.scu.edu.au [search on ‘lifestyle medicine’]) with students from around the world.
As it evolves, the practice of lifestyle medicine will no doubt change. It was never intended that this should take over from the practices of modern conventional medicine and public health but rather that it should contribute to them. How it does this in the future will (hopefully) remain fluid, based on changing needs and cognizant of the dynamic nature of health in the modern world.