
Abstract
The relationship between family dynamics and health has been extensively studied, but the specific pathways involved are not yet fully understood. The role of intimate partner relationships in promoting and maintaining healthy lifestyle behaviors remains understudied, particularly in minority populations. This study addressed this gap by examining how frequent spousal and familial interactions affect healthy lifestyle behaviors in young Asian Americans. Survey data from Asian American adults aged 18 to 35, collected in March 2021, is used to compare two groups: one interacting most with an intimate partner and the other interacting most with other non-intimate family members. The results showed that young Asian Americans interact most with their spouses/partners and mothers. Participants who interacted most frequently with their spouses/partners reported a greater influence in maintaining a healthy lifestyle, particularly in the domains of exercise and sleep. Moreover, those who interacted more with their spouses/partners exhibited a greater sense of connectedness, which impacted spousal and personal influence on healthy lifestyle behaviors. The findings suggest that promoting interaction and fostering stronger spousal/partner relationships can positively influence the healthy lifestyle behaviors of young Asian Americans.
Keywords
“Promoting positive, appreciative, and frequent interactions between partners emerges as a key strategy to strengthen their relationship and facilitate the adoption of healthy lifestyle behaviors.”
Introduction
The health concerns of Asian Americans, one of the fastest-growing ethnic populations in the US, are gaining recognition. 1 Despite being labeled as a “model minority,” Asian Americans face unique health challenges, including a higher risk of diseases like cancer, heart disease, and mental illness. 2 Factors such as underutilization of health care services, cultural identity, racism, and health-compromising behaviors contribute to these conditions.2-4 It is crucial to recognize that these factors are interconnected, working in tandem rather than independently shaping health conditions in Asian American communities. Specifically, the amalgamation of Asian American identity and culture, coupled with the lack of culturally tailored and informed health care spaces, contributes to health care underutilization. 5 For instance, cultural aspects such as the emphasis on indirect communication, respect for authority, and the stigma surrounding certain health behaviors (e.g., substance use) can affect the way individuals express health concerns or seek medical information. 6 Also, the lack of mixed health care spaces, where traditional and alternative medicine practices are integrated, contributes to health care underutilization. 5 This dynamic reinforces the reliance of Asian Americans on family members for health-related conversations and family-based caregiving. This scenario underscores the importance of investigating the role of family interaction in shaping health behaviors among Asian Americans.
In the realm of public health, concerns also arise over the dietary habits of young Asian Americans, increasing the risk of obesity and chronic diseases as they become acculturated.7,8 Asians have a higher risk of metabolic syndrome, which increases the risk of diabetes and cardiovascular disease, even at the same BMI levels as their non-Hispanic white counterparts. 9 Lifestyle modifications and health behavior practices cannot be overstated in preventing and managing chronic diseases, yet sustaining healthier habits is challenging. Therefore, it is crucial to examine the factors shaping and maintaining a healthy lifestyle, particularly within the Asian American community. 10
In the Asian American community, marriage and family hold significant value, influencing the well-being and health behaviors of Asian Americans. However, research on how spousal/partner and other family relationships impact the health behavior of young Asian Americans remains limited. Research indicates that individuals tend to spend more time with their partners as they progress into adulthood, shifting social control to their partners. 11 Implementing interventions during young adulthood becomes crucial for preventing chronic diseases later in life.12,13 Surprisingly, the existing literature on social relationships and health has largely overlooked the healthy lifestyle choices of young AA. Recognizing this gap, this study aims to investigate how frequent interactions within intimate partnerships may influence lifestyle choices differently compared to other family relationships. The objective is to explore the nature of this influence and determine its extent within the context of young AA health behaviors.
The Impact of Relationship Quality and Frequent Interaction on Health Behavior
Intimate partners play a crucial in adopting, maintaining, and modifying health-related behaviors. The health of one partner can positively or negatively influence the health of the other through various pathways. Health behaviors play a vital role in this relationship, as romantic partners are often the primary source of support and social control in health behavior.12,14,15 Positive aspects, such as support and intimacy, and negative aspects, such as strain and conflict, can both influence health behaviors. 16 However, marriage or cohabiting can also result in health-compromising behaviors, such as substance use, as a coping strategy for stress and conflicts in the relationship.17,18 Family emotional climate can trigger health behaviors, which in turn can affect health outcomes. 17 A recent study also revealed that increased shared activities with families are positively associated with greater influence on Asian Americans’ healthy lifestyle behaviors. 10 Overall, spousal and familial interactions can have both positive and negative effects on health behaviors and the nature of these effects depends on the quality of the relationship.
Frequent interaction with a partner is important for establishing intimacy and enhancing family functioning.19,20 If frequent interaction is conducive to improving overall relationship quality, which affects health-related behaviors, relationship quality could at least partially account for the link between frequent interaction and maintaining a healthy lifestyle. Despite this, few studies have examined these relationships comprehensively.
Theoretical Background
In conjunction with empirical evidence, the Biobehavioral Family Model (BBFM) posits that family emotional climates interact with biobehavioral reactivity, affecting the health outcomes of individual family members.21,22 The family emotional climate in the BBFM encompasses relational factors such as familial and intimate partner relationship quality. 21 Biobehavioral reactivity, as conceptualized in the model, refers to the biological, shared health behaviors, and psychophysiological pathways through which an individual family member responds to the family’s emotional climate. 23 Previous empirical research has demonstrated that depression and anxiety as emotional factors and allostatic load as physiological components mediate the link between emotional climate and disease activity.21,22
While limited, a recent study explored health behavior as an operationalization of the pathways in the BBFM in response to marital dysfunction. This study revealed that health behaviors, specifically diet and exercise, are prompted by the emotional influence of marital issues, establishing the connection between marital relationships and health outcomes. 17
In the present study, our focus centers on frequent interactions, relationship quality, and their association with the influence on lifestyle behaviors. In light of the BBFM framework, frequent interaction denotes the regularity and consistency of interpersonal exchange within the family unit, encompassing communication patterns, shared activities, and overall engagement. 19 This dynamic contributes to cultivating a supportive and cohesive family environment, nurturing positive emotional climates.19,20 The outcome variable in this study is the perceived familial and spousal/partner influence on lifestyle behaviors, which pertains to the extent to which family dynamics and frequent interactions shape an individual’s lifestyle behaviors. It is important to note that this study does not undertake a comprehensive testing of all theoretical constructs within the BBFM. Rather, we utilize the BBFM as a guiding theoretical lens to investigate how family and frequent spousal interactions influence the capacity of young Asian American adults to maintain lifestyle behaviors.
Present Study
The present study examines the impact of frequent interaction and relationship quality on the ability to maintain a healthy lifestyle among 18–35-year-old Asian Americans. It also investigates the indirect impact of frequent interaction on health behavior through the quality of marital and non-marital family relationships. Comparisons are made between the perceived influence of intimate partners and other family members on young AAs’ ability to maintain a healthy lifestyle. Additionally, the study explores the link between perceived influence and connectedness in romantic relationships. Two hypotheses guide the study: Firstly, we anticipate a positive association between frequent interaction and positive relationship quality, leading to an increased perceived influence on health behaviors. Secondly, positive relationship quality will help elucidate the link between frequent interaction with family members and the perceived influence on health behavior.
Methods
Data
The data for this study came from the online survey, administered in March 2021 using the Qualtrics platform. Details on data collection methods have been described elsewhere. 10 Briefly, to be eligible for participation in the study, individuals had to self-identify as Asian Americans and be between the ages of 18 and 35, with at least one family member residing in the U.S. A total of 900 participants were recruited through various online platforms, with the majority of participants being East Asian (44.1%, n = 397)), followed by Southeast Asian (24.1%, n = 217) and South Asian (23.7%, n = 213), and then mixed (8.1%, n = 73). Slightly over half of the sample (51.2%, n = 461) identified as female and the participants had a mean age of 25.0 (SD = 4.94). It should be noted that the study is not nationally representative, and the results of inferential statistics should be interpreted with caution. However, this dataset represents one of the first and only large, comprehensive, and (importantly) disaggregated samples of Asian American young adults, and findings can provide valuable insights into the family interactions and lifestyle behaviors of young AAs. All participants provided online informed consent, and the study protocol was approved by the institutional review boards of New York University. 10
Measures
Participants were asked to rate the extent to which the highest ranked family member they interacted with most frequently influenced their healthy lifestyle behaviors, and to what extent they themselves influenced the family member’s lifestyle behaviors, on a 6-point scale ranging from 1 (no influence) to 6 (significant influence). These lifestyle behaviors encompass 6 domains: eating a healthy diet, increasing physical activity, improving one’s sleep, forming and maintaining relationships with people, developing strategies to manage stress, and avoiding risky substances. 24 Responses of “don’t know” were coded as “0” in the analysis. The influence ratings were dichotomized into low (1-3) and high (4-6) perceived influence on each domain, with overall perceived influence calculated by summing the 6 domains. This study examined both the influence of spouses/partners and family members on an individual’s ability to maintain a healthy lifestyle, as well as the individual’s own influence on their spouse/partner or family member’s ability to maintain a healthy lifestyle.
Frequent interaction with a spouse/partner vs other family members was determined by asking participants to rank which types of US-based family members they interacted with most frequently, from 1 (most frequently) to 8 (least frequently). For this study, the most frequent interaction with a spouse/partner was coded as “1” and all other types of familial interaction as “0” to facilitate analysis.
The perceived quality of the family members participants interact with most frequently was measured using a 5-item scale that assessed connectedness. 25 Each item was rated on a five-point Likert scale ranging from 1 (not at all) to 5 (very much). Sample items included “They care about you they care about your feelings,” “They understand you,” and “They respect your privacy.” The measure of connectedness was obtained by calculating the mean score across the 5 items, with higher scores indicating greater levels of connectedness (Cronbach’s alpha = .88).
In addition, the Family Interaction Quality Assessment scale, consisting of 28 items, was used to measure positive (e.g., “when spending time with a family member, I look for more ways to do it”), negative (e.g., “when spending time with a family member, I feel pressured to do it”) and appreciative interaction quality (e.g., “when spending time with a family member”).
Covariates in the study included age (in years), gender (1 = female, 0 = male), marital status (1 = married/partners, 0 = widowed/divorced/separated), educational attainment (some college or less, bachelor’s, master’s or more), specific Asian American ethnic subgroup (East Asian, South Asian, Southeast Asian, Mixed), religion, household size (1, 2-3, 4 or more), work status (currently working), nativity (being born in the U.S.), and acculturation, which was measured using the 4-item Short Acculturation Scale was also included. 26
Statistical Analyses
To begin the analysis, descriptive statistics for all study variables were presented for the full sample, as well as by the type of family member with whom respondents interacted most frequently (i.e., spouse/partner and other family members). The differences between these 2 groups were also tested using Chi-square and t test. Following this, a series of regression models were conducted to estimate the influence on lifestyle behaviors, including eating a healthy diet, increasing physical activity, improving one’s sleep, forming and maintaining relationships with people, developing strategies to manage stress, and avoiding risky substances.
The first regression model examined the differences between AAs interacting most with their spouses/partners vs other family members in terms of perceived influence on lifestyle, while adjusting for other covariates. The second regression model included connectedness to examine whether connectedness is associated with perceived influence and to account for potential differences in perceived influence between types of family members. To assess whether connectedness explains the potential association between the type of family member that respondents interacted with most frequently and the perceived influence on lifestyle behaviors, a mediation analysis using the KHB (Karlson -Holm-Breen) method was performed. 27 For the supplementary analysis, 3 measures of interaction quality were individually entered into a separate model due to their strong correlations with each other and with connectedness. Linear regression was used to estimate overall influence, while logistic regression was used to estimate each lifestyle behavioral outcome. All analyses were conducted in Stata version 16. 28
Results
Descriptive Analyses
Descriptive Statistics by the Family Members With Whom Participants Interact Most Frequently.
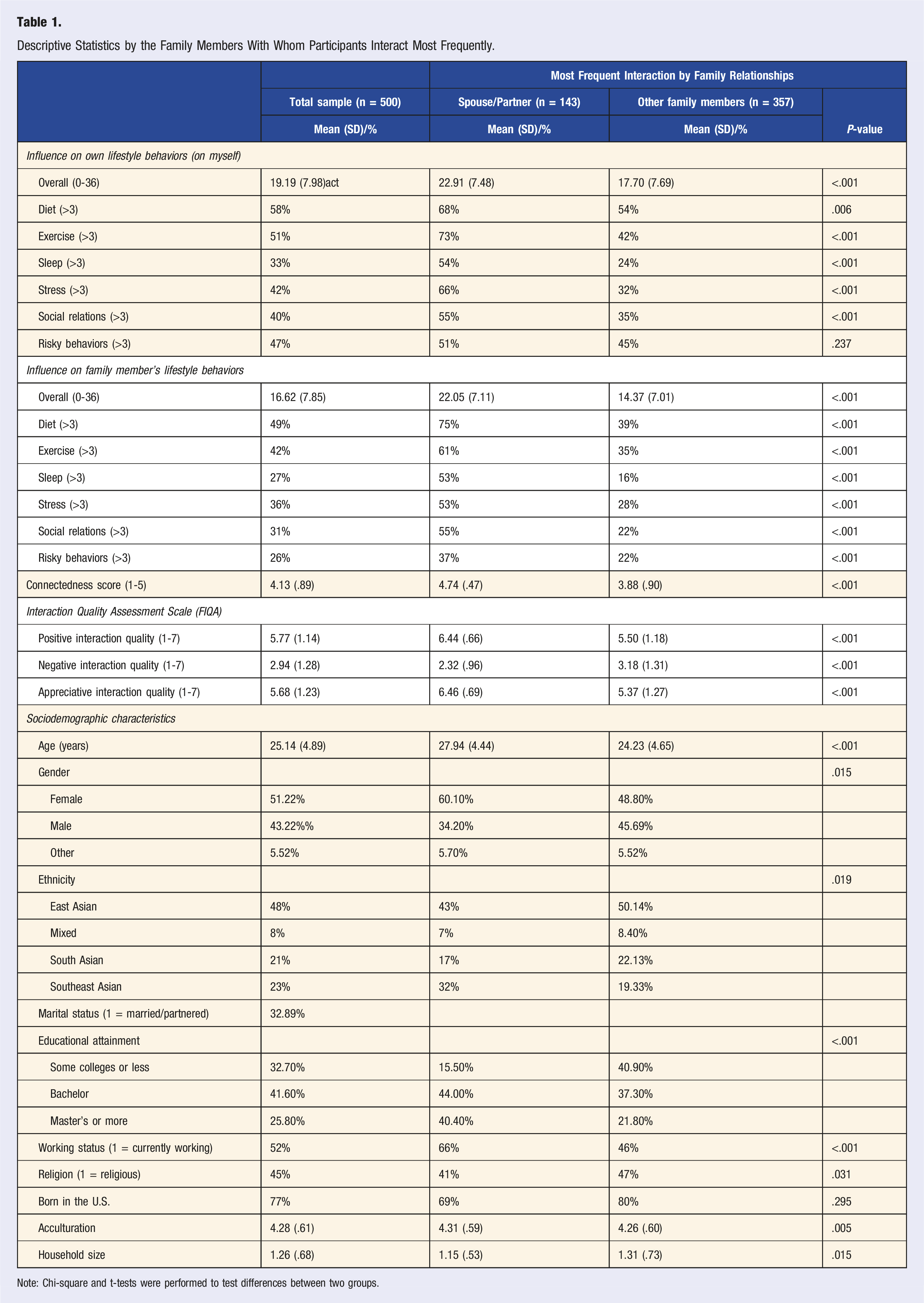
Note: Chi-square and t-tests were performed to test differences between two groups.
Main Analyses
Regression Estimates Predicting Perceived Spousal and Familial Influence on Own Healthy Lifestyle Behaviors.
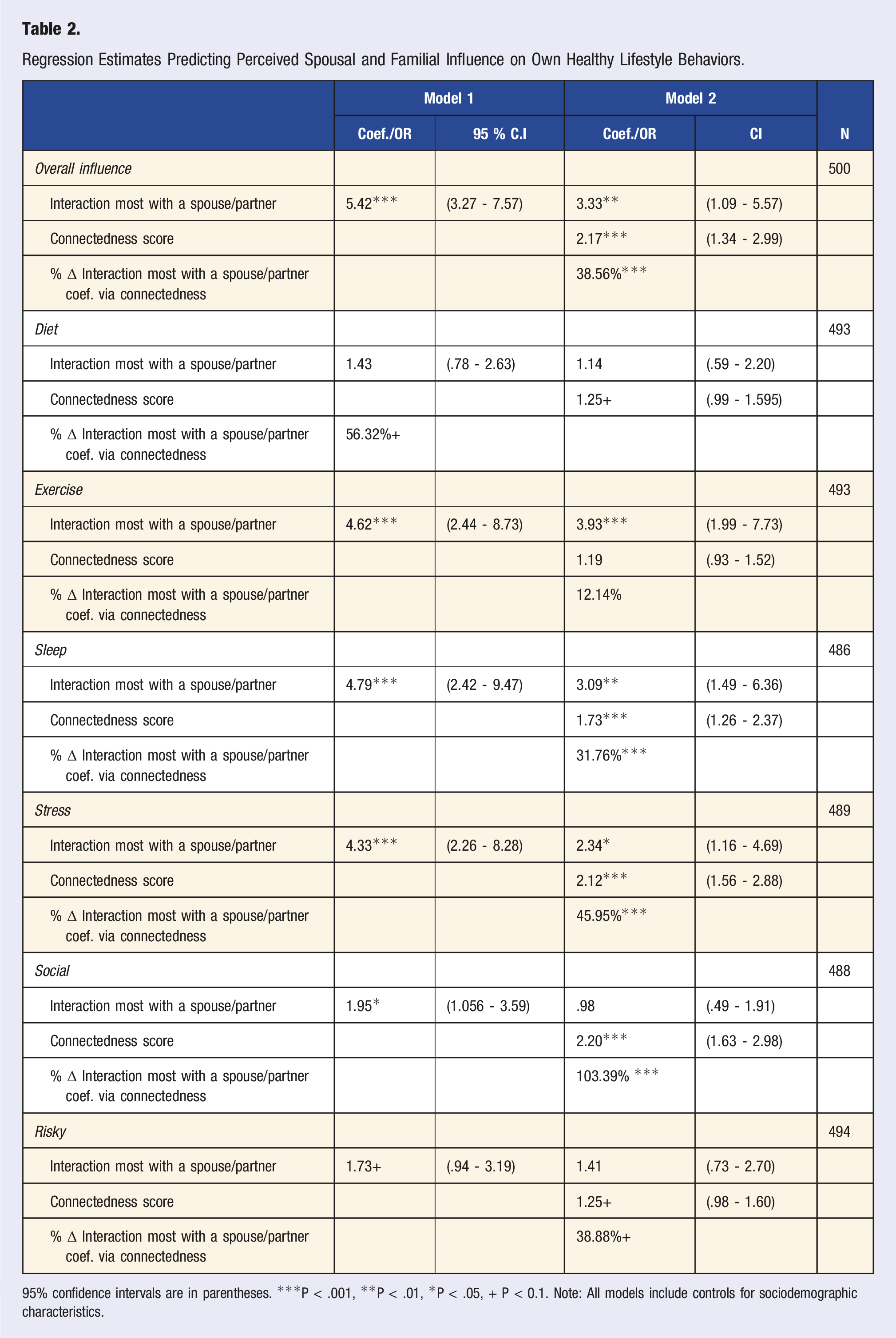
95% confidence intervals are in parentheses. ***P < .001, **P < .01, *P < .05, + P < 0.1. Note: All models include controls for sociodemographic characteristics.
Regression Estimates Predicting Perceived Personal Influence on Spouse and Family Members’ Healthy Lifestyle Behaviors.
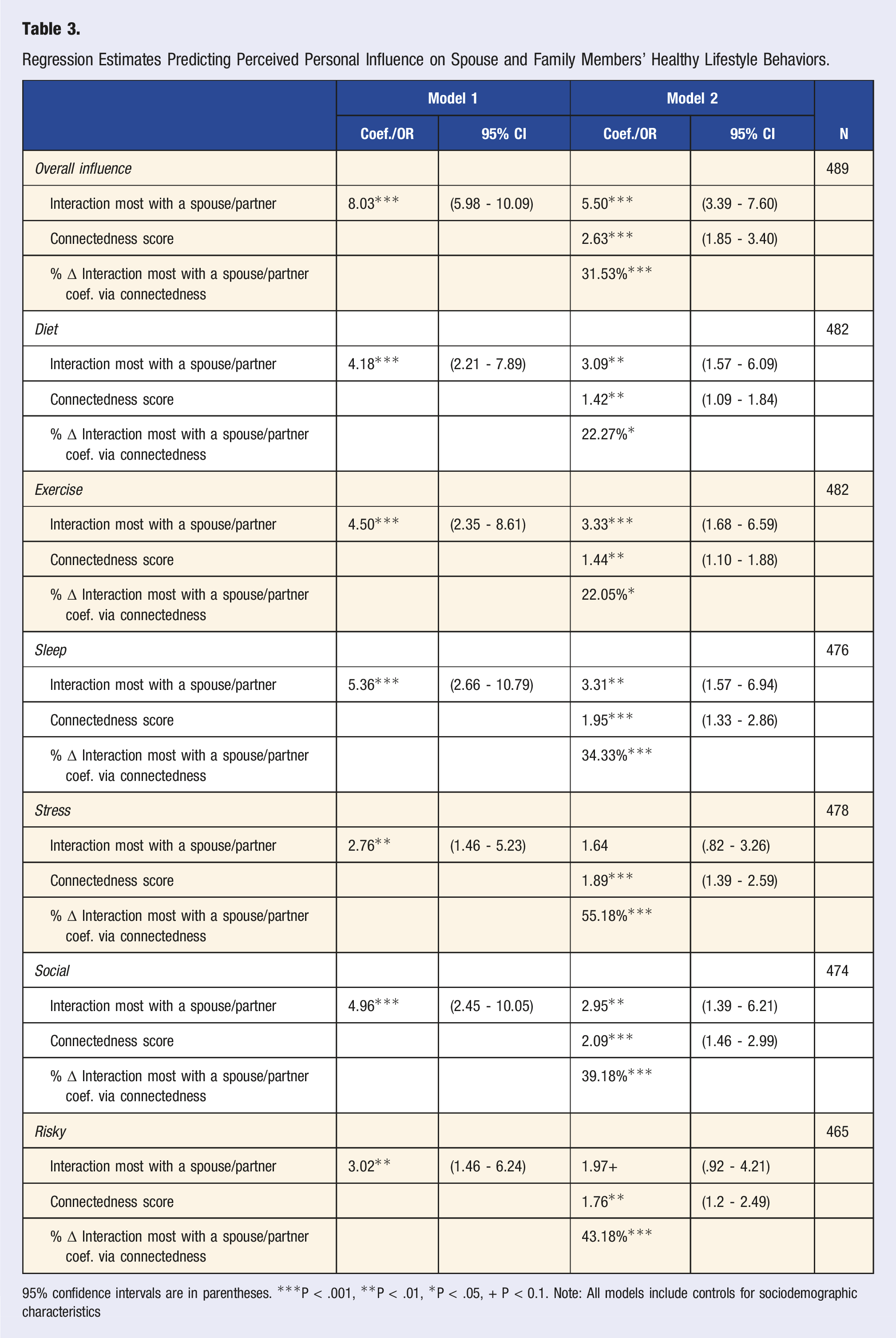
95% confidence intervals are in parentheses. ***P < .001, **P < .01, *P < .05, + P < 0.1. Note: All models include controls for sociodemographic characteristics
Table 2 illustrates that spousal influence on lifestyle behaviors appeared to be greater than other familial influence on lifestyle behaviors (b = 5.42, P < .001). It is significantly associated with greater odds of high influence in increasing physical activity (OR = 4.62, 95% CI 2.44, 8.73), improving sleep (OR = 4.78, 95% CI 2.41, 9.47), forming and maintaining relationships with people (OR = 1.94, 95% CI 1.056, 3.586), developing strategies to manage stress (OR = 4.33, 95% CI 2.26, 8.28), and avoid risky substances (1.73, 95% CI .94-3.19). However, it has no significant association with the influence on the ability to eat a healthy diet.
In Model 2, when connectedness was added, the coefficients for the most frequent interactions with a spouse/partner remained statistically significant in estimating overall perceived influence and the odds of reporting high level of perceived influence on exercise, sleep and stress management. However, these coefficients were no longer significant in predicting perceived influence on social relationships and risky substances. Also, greater connectedness with the family members with whom a participant interacts most frequently was positively associated with perceived influence on most of the lifestyle outcomes with the exception of exercise. To provide a better understanding of these findings, predicted probabilities were generated and displayed in Figure 1. For instance, the predicted probability of reporting high spousal/partner influence on one’s own sleep was .48, while the predicted probability for non-spousal/partner influence on sleep was .23.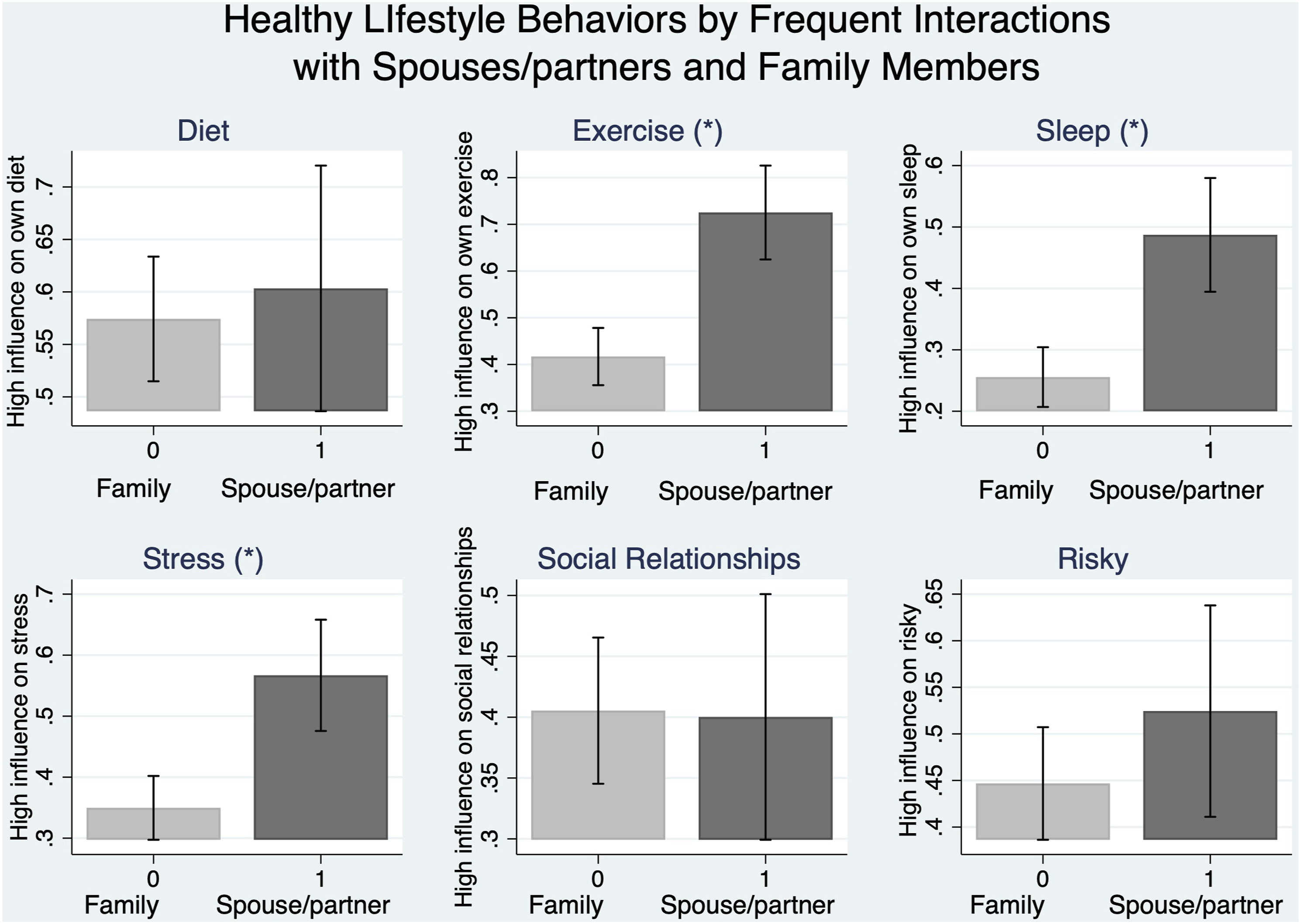
Given the pattern of the findings, the mediating contribution of connectedness was tested. Frequent interaction within the context of marriage and family has the potential to impact lifestyle behavior through various routes, one of which is relationship quality or connectedness, which the present study examined. Ancillary analysis revealed that AAs who frequently interacted with their spouses exhibited greater connectedness than those who had other frequent familial interactions (b = .96, P < .001) (now shown). Additionally, as demonstrated in the third row of each lifestyle behavioral outcome, connectedness plays a role in differences in overall perceived influence and influence on sleep, stress management, and social relationships between spousal and non-spousal frequent interactions. Using sleep as an example, over 30% of the total effect of interacting most with a spouse/partner (vs other family members) on perceived influence on own sleep came from connectedness. Similar findings were obtained for stress and social relationship. It is worth reiterating that the outcome was related to the influence of the highest ranked family members on one’s lifestyle, and thus frequency of interaction was inherently controlled for in the analysis. Therefore, the mediation percentage, which showed that more than 30% of the differences in spousal/partner influence and other non-spousal family members could be attributed to differential connectedness, was particularly meaningful.
Table 3 displays the results of the linear and logistic regression models of overall perceived personal influence on a spouse/partner and family member’s lifestyle behaviors. As shown in Model 1 of Table 3, the perceived own influence on a spouse/partner’s lifestyle was found to be greater compared to personal influence on other family members. In Model 2, connectedness was included, and the coefficient for frequent interaction with a spouse/partner decreased but remained statistically significant, except for the association with stress. To provide context, predicted probabilities were generated based on Model 2, and the estimated overall perceived own influence and predicted probabilities for each domain of lifestyle were displayed in Figure 2. Using sleep as an example, the predicted probability of reporting high personal influence on a spouse/partner’s sleep and family members’ sleep was .39 and .16, respectively. Lastly, the mediation percentage indicated that over 20% of the total effect of interacting most with spouses/partners (vs other family members) on personal influence on their lifestyle behaviors was linked to connectedness. This finding suggests that there was a mediated effect, with connectedness accounting for some of the differences in the perceived personal influence on spouses/partners’ lifestyle and other family members’ lifestyle behaviors while controlling for the interaction frequency.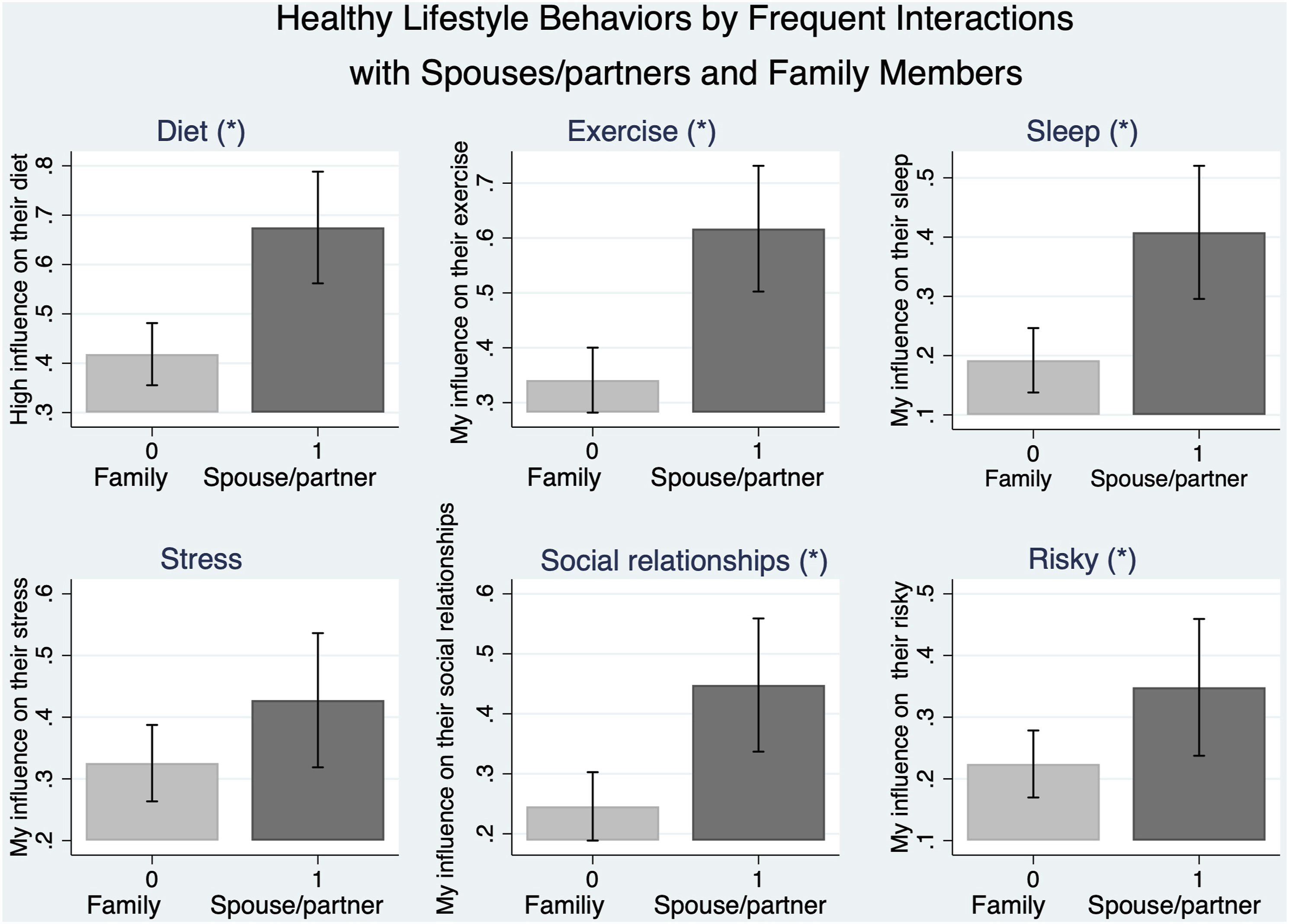
Supplementary Appendix Table 1 presents the results of the model predicting outcomes using 3 separate measures of interaction quality: positive interaction quality, negative interaction quality, and appreciative interaction quality. When controlling for the quality of interaction, those who interacted most with their spouses/partners exhibited a greater influence on healthy lifestyle behaviors compared to those who interacted most with other family members. Moreover, positive and appreciative interaction was positively associated with a greater influence on lifestyle behaviors, while negative interaction was not significantly associated with perceived influence.
To ensure the robustness of the study’s findings and address the issue of a large amount of missing data, particularly on the dependent variables and connectedness variable, multiple imputation by chained equation was performed. The imputed data were analyzed, and the results were found to be consistent with the original substantive findings (not shown here).
Discussion
The present study aims to expand on this topic by investigating the impact of intimate partner interactions vs non-intimate family interactions on healthy lifestyle behaviors among young Asian American adults. Furthermore, the study explores how the level of connectedness may influence the association between frequent interaction and its impact on healthy lifestyle choices.
The results of the descriptive analysis indicate that among young Asian American adults, their spouse/partner and mother were the most frequent sources of interaction in the family. This is particularly noteworthy as previous research has consistently reported that social support from these two sources is linked to better health and healthier lifestyle choices among Asian and Asian American families.29,30 Thus, these findings reinforce the crucial role of spouse/partner and mother as primary sources of social support for young Asian Americans in maintaining healthy lifestyles.
By comparing frequent interaction with intimate partners vs non-intimate family members, the study found that frequent interaction with a spouse or partner has the greatest impact on both one’s own and their partner’s healthy lifestyle behaviors. In particular, frequent interaction with a spouse/partner was significantly associated with greater perceived influence on the ability to maintain physical exercise, improve sleep, and develop strategies to manage stress. One possible explanation for the significant effect of frequent intimate partner interactions on healthy lifestyle behaviors is the potential for mutual accountability and support between partners. When both partners share a commitment to a healthy lifestyle, they can work together to motivate each other and hold each other accountable for their behavior. Additionally, partners may be more likely to engage in healthy behavior together, which can further reinforce healthy habits as the literature supports the idea of concordance of behavior changes.31,32
Of six domains of healthy lifestyle behaviors, spousal influence has a notable impact on maintaining exercise, improving sleep and managing stress. The personal influence was also significant for diet, exercise, sleep and social relationships. We utilized the Suest test to compare spousal and personal influence on each domain of lifestyle behaviors and found no significant differences, except for dietary behavior. The two domains with the strongest impact from both spousal and personal influence were sleep and physical activity. We speculate that the reason behind this could be that, unlike other family members, people in relationships tend to sleep together with their partners and spouses. Previous research on sleep has demonstrated that sharing a bed or co-sleeping has numerous benefits for sleep health and can lead to the synchronization of sleep patterns between partners. 33 Sharing a bed as a couple creates a close proximity that can facilitate the influence of one partner’s sleep on the other. This finding is particularly intriguing as previous research on familial influence on health behaviors, which did not specifically examine spousal influence, found a low impact of non-intimate family members on sleep. 10 Additionally, exercise was found to be a significant domain where spousal influence was stronger than other familial influences. This could be attributed to the shared resource hypothesis, where greater spousal influence than familial influence on exercise is related to the sharing of physical and social environments and access to resources such as time and gym facilities.
We also found that there were no significant differences in spousal and familial influence on the ability to maintain a healthy diet. These findings support a recent analysis of Asian American young adult dietary behaviors which observed that living with a partner was not associated with significant differences in dietary healthfulness. 34 Previous research has shown that mothers have the greatest influence on dietary behavior, and this may be attributed to cultural norms and traditions. 10 Further, couples may share similar dietary behavior and preferences according to the assortative mating theory, which could explain the lack of differences in spousal and familial influence on diet. As for the greater influence on their partner’s diet compared to their family members, it is possible that young Asian Americans may have more control over their partner’s diet. In the family context, young adults are often in a position to receive care, especially in food choices, which are usually led by mothers. 35 In a romantic/marital relationship, on the other hand, they may perceive themselves to have power to influence or negotiate their partner’s dietary habits. The finding suggests that young couples are possibly in a transitional phase where they are undergoing changes and modifications in their dietary habits outside of the influence of their parents.
Another notable finding is the positive and direct effect of connectedness on healthy lifestyle behaviors. This finding is consistent with a number of studies that have highlighted the importance of positive relationship quality in promoting healthy behaviors in romantic relationships. 31 Moreover, the Biobehavioral Family Model (BBFM) has also emphasized the role of a supportive family climate in promoting healthy behaviors and better health outcomes. 17 Therefore, among young AAs, it appears that fostering supportive and connected relationships with romantic partners can be an effective way to promote healthy lifestyle behaviors.
The study also found a mediated effect, with connectedness accounting for some of the differences in the perceived influence on spouses/partners’ lifestyle and other family members’ lifestyle. The finding implies that young AAs who interact frequently with their partners are more likely to build a greater connection, which, in turn, promotes a greater likelihood of engaging in healthy behaviors. This positive cycle between frequent interaction, connectedness, and healthy lifestyle choices can have significant long-term health outcomes, underscoring the importance of fostering positive and connected relationships with intimate partners in promoting healthy lifestyle behaviors among young AAs. In light of social control theory, partners may exert social control over each other’s behavior through mechanisms like positive reinforcement, punishment, or monitoring.12,31 Thus, regarding health behaviors, frequent interaction between partners forms closer connectedness, allowing partners to hold each other accountable for behavior change without creating too much conflict or strain.
Although interaction quality was not the primary variable of interest in the present study, the study found that positive and appreciative interaction had a significant positive association with greater influence on healthy lifestyle behaviors. Conversely, negative interaction did not show any significant association with the influence on healthy lifestyle behaviors. These findings suggest that cultivating positive and appreciative interactions in relationships may contribute to the promotion of healthy behaviors. It is important to consider the quality of the interaction in the context of couple and family when trying to make positive lifestyle changes.
The study has limitations that should be acknowledged. First, the data used in this study is not couple-level data, meaning that the results may not fully capture the dynamics of the couple’s interactions. To address this limitation, future research could use couple-level data with an actor-partner interdependence model, which would allow for a closer examination of the couple dynamics and disentangle the actor’s and partner’s perceived influence on health behaviors. Another constraint lies in the study’s reliance on cross-sectional data, which limits our ability to draw causal conclusions about the relationship between frequent interaction, connectedness and influence on the ability to maintain healthy lifestyle choices. To address this constraint, future research should consider longitudinal data to examine actual health behavioral change within the context of a couple. Furthermore, the study lacked potentially important information on the characteristics of spousal and family relationships, such as the length of the marriage or relationship, sleeping and living arrangement, whether the marriage or relationship is interracial, whether there are children present, and other factors that could have an impact on and explain the results obtained. It is important to note that the results of this study are based on self-reported data, introducing the possibility of a disparity between perceived and actual influences on behaviors. This is particularly pertinent in the context of health stigma within the Asian American community. Stigma, acting as a substantial barrier to accurate reporting, may lead participants to underreport information, particularly regarding sensitive health conditions or behaviors like the use of risky substances. The emphasis on privacy and maintaining a positive image in Asian culture, often referred to as the Asian American model minority myth, discourages participants from fully disclosing their health behaviors, even in an anonymous survey. 6 Cultural norms within the community further compound this limitation, sharing an individual’s perception of socially acceptable or desirable health behaviors. Stigma may consequently influence participants to conform to these norms, potentially resulting in biased self-reporting that aligns more with societal expectations than actual behaviors. Finally, the absence of geographic information about participants in the data poses a limitation. Subsequent research endeavors could benefit from including state-specific data to gain a more nuanced understanding of health care services for Asian American families and couples.
Conclusions
This study highlights the significance of intimate partner interactions in promoting healthy lifestyle behaviors among young AAs, underscoring the need for health care professionals, community leaders, and policymakers to recognize this role. The implications for behavioral medicine suggest a shift towards interventions targeting healthy lifestyle behaviors in young AA couples, with a focus on treating couples as a unit rather than individual partners. Promoting positive, appreciative, and frequent interactions between partners emerges as a key strategy to strengthen their relationship and facilitate the adoption of healthy lifestyle behaviors. Moreover, the results point towards the effectiveness of interventions accounting for the influence of family members, particularly spouses or partners and mothers, in instilling health behavior change in young Asian Americans. This insight can guide community leaders in designing interventions that recognize the role of family members, especially within intimate relationships. Such tailored interventions stand a better chance of instigating positive health behavior changes within the community. Additionally, the data used in this study represents the first national dataset exclusively focusing on young Asian American adults, providing comprehensive information about family interactions and health behaviors. 10 By delving into the details provided by the data, community leaders can discern patterns and dynamics within Asian American families that significantly influence healthy lifestyles. They can then organize family-centric initiatives that focus on strengthening family connections and providing tools for families to collectively adopt and sustain healthy habits. In conclusion, the integration of the findings into community initiatives can contribute to more targeted and culturally relevant programs to improve health and well-being of the young Asian American adults.
Supplemental Material
Supplemental Material - Comparing the Influences of Spouses or Partners With Other Family Members in the Ability of Young Asian Americans to Maintain a Healthy Lifestyle
Supplemental Material for Comparing the Influences of Spouses or Partners With Other Family Members in the Ability of Young Asian Americans to Maintain a Healthy Lifestyle by Soyoung Kwon, Shamir H. Ali, and Ralph J. DiClemente in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
The project described in this paper relies on data from survey(s) administered by the New York University South Asian Health and Research Group (SAHARA). The content of this paper is solely the responsibility of the author and does not necessarily represent the official views of NYU-SAHARA. The NYU IRB approved the parent study protocol.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data for this study is supported by the NYU South Asian Health and Research Group (SAHARA). The content in this study is solely the responsibility of the author and do not necessarily represent the official view of the NYU-SAHARA.
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.