
Abstract
Most adults do not adhere to established aerobic physical activity (PA) guidelines due in part to various barriers. PA snacks, or periodic short bouts of activity (<10 minutes) offer a potential strategy to overcoming such barriers and increasing PA. Previous efforts have been focused on eliciting the health benefits of PA and exercise snacks, yet adherence to this concept has not been examined. The purpose of this review is to summarize the current literature assessing adherence to PA snacks and health-related outcomes associated with PA snacks. PubMed, CINAHL, and SPORTDiscus were searched for literature published between January 2018-September 2023. Studies investigating adherence and/or the health-related outcomes of PA snacks were included. Of 4201 articles identified, 12 studies were included in the review. Most of the studies were randomized (n = 10), focused on adults with a chronic disease/life-long condition or exhibited a sedentary lifestyle (n = 8), and reported positive health outcomes (n = 12; e.g., improvements in cardiometabolic markers and body composition). Five studies reported adherence to supervised and unsupervised PA snack interventions, with high rates ≥92%. This review supports and extends the previously reported health-related benefits of PA snacks. It also shows promise for increasing overall PA and adherence to the PA guidelines.
“The health outcomes assessed support prescribing or recommending multiple short bouts of activity to adults as positive.”
Introduction
The prevalence of chronic disease (e.g., heart disease, stroke, Type II diabetes) among adults in the U.S. continues to increase with six in 10 adults having at least one, and four in 10 having two or more chronic diseases. 1 Among the key modifiable lifestyle risk factors for chronic disease is lack of physical activity (PA) or insufficient activity. Evidence-based aerobic PA guidelines for adults (150 minutes/week of moderate-intensity aerobic activity and OR 75 minutes/week of vigorous-intensity aerobic activity OR an equivalent combination) have been established to provide guidelines for the improvement and/or maintenance of activity and related health-related outcomes including chronic disease onset. 2 However, the majority of adults (≥75%) do not adhere to these guidelines 3 which has been attributed to common barriers (e.g., lack of time, lack of social support, lack of motivation, high costs and lack of facilities). 4 Increased efforts in PA promotion that address these challenges are much needed. Therefore, an appealing, novel approach, PA snacks, or periodic short bouts (<10 minutes) of activity offers a potential strategy to increasing PA adherence.
A recent systematic review conducted by Jakicic et al. (2019) highlighted the health-related benefits of accumulated short bouts of PA (<10 minutes) which included positive impacts on body weight or body composition, blood pressure, blood lipids, glucose/insulin, multimorbidity, and all-cause mortality. 5 This review informed the recent modifications to the second edition of the Physical Activity Guidelines (removing the requirement of 10 minute-bouts to count toward the minimal aerobic activity), and has introduced more of an emphasis on how PA is promoted. 6 The “PA snack” concept or engaging in multiple short bouts (<10 minutes) of moderate-to-vigorous intensity aerobic physical activities has gained traction as a more appealing way for individuals to increase activity and adherence to PA guidelines.7-10 Example activities include (but not limited to) short, brisk walks at lunchtime, taking the stairs instead of elevator, and marching in spot while brewing coffee. A recent scoping review conducted by Jones et al. focused on a similar concept “exercise snacks” (note: exercise is a subcategory of PA), or brief, high intensity, structured and planned aerobic (e.g., stair sprinting), strength (circuits of bodyweight exercises), balance, and combinations of these three activities. 11 Results from this review show that exercise snacks produce improvements in cardiorespiratory fitness with equivocal findings for physical function, mood, quality of life, blood markers (e.g., glucose, triglycerides), and feasible, acceptable, and adherence to intervention rates were high. 11 Despite the health enhancing effects of PA snacks and the promising adherence rates for exercise snacks, it remains unknown whether the accumulated approach for PA influences engagement in PA in comparison to traditional approaches such as one bout of 30 minutes or breaking up PA in multiple bouts ranging from 10-15 minutes. 12 An understanding of the relationship between PA snack and adherence and how PA snacks can serve as a potentially effective strategy for improving PA adherence warrants further examination, shedding light on the development of future PA interventions.
Although Jakicic et al. reported the health-related outcomes of engaging in PA snacks, 5 to our knowledge, there are no reviews registered in the PROSPERO international prospective register examining the relationship between short bouts (<10 minutes) of PA and adherence to intervention among adults. The purpose of this rapid review, or streamlined process to a systematic review is to summarize the current literature assessing adherence to PA snacks and health-related outcomes associated with PA snacks We hypothesize that prescribing short bouts of PA will be related to better adherence to PA interventions and increases in overall minutes of PA.
Methods
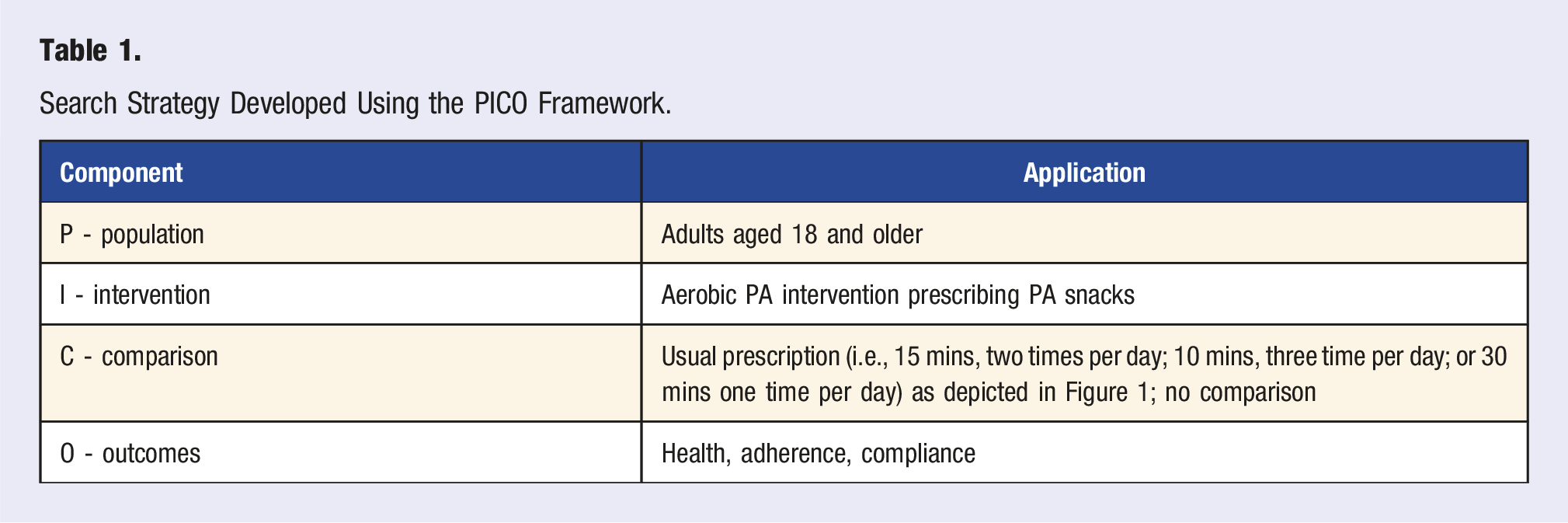
Search Strategy
Search Strategy Developed Using the PICO Framework.
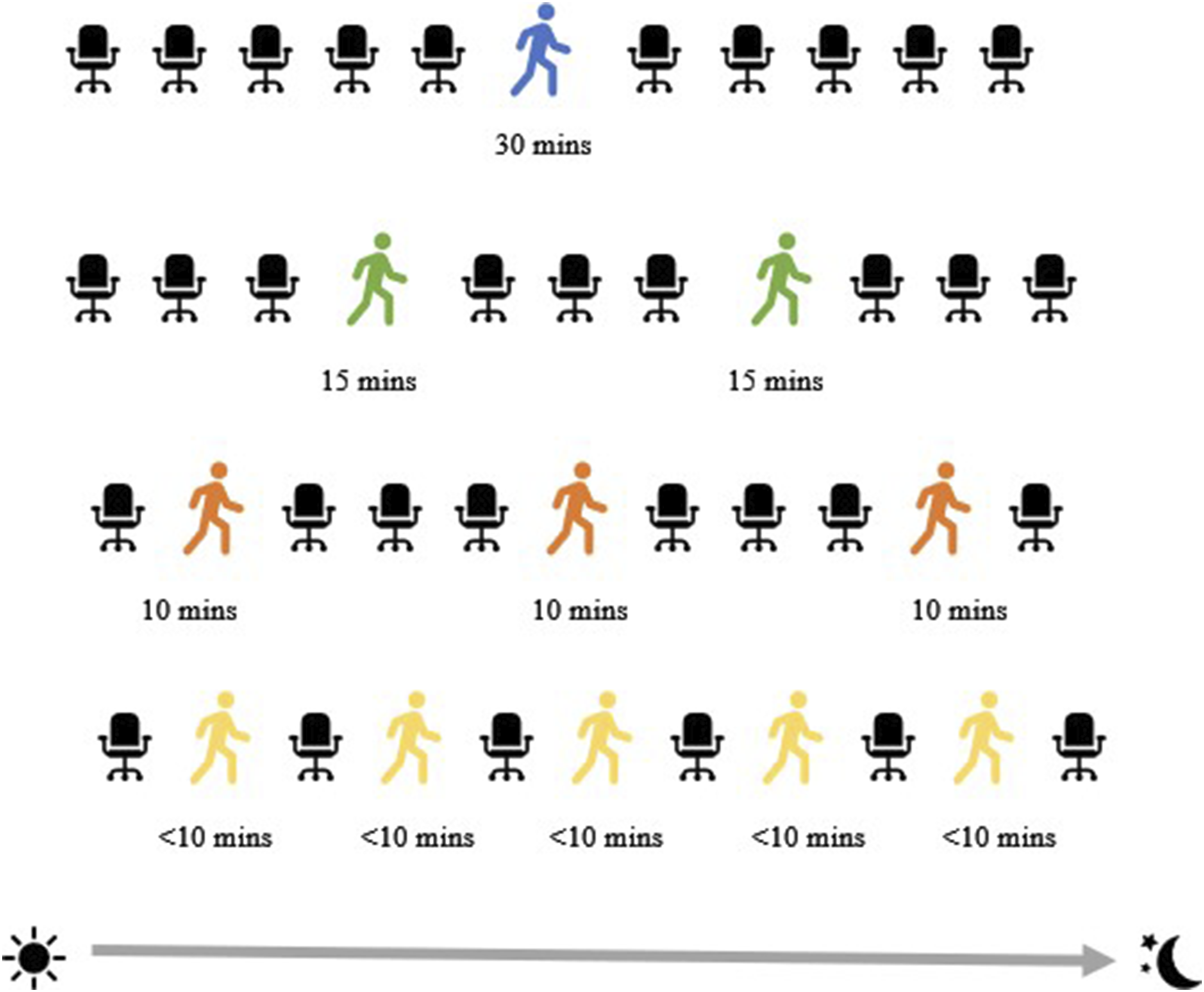
Common PA prescriptions or recommendations versus PA snacks.
Inclusion and Exclusion Criteria
Included studies must have: (1) focused on adults aged 18 and older, (2) been an intervention (e.g., randomized, pre-post), mixed methods, or cross-sectional, (3) focused on aerobic PA and/or exercise engaged in multiple bouts (<10 minutes), (4) reported health and/or intervention protocol adherence or compliance outcomes and (5) been published after 2018 (i.e., when the PA guidelines changed omitting requirement of bouts lasting >10 minutes to count toward meeting PA guidelines). For this review, adherence is defined as the extent to which participants complete prescribed supervised and unsupervised PA/exercise. Supervised activities are completed in controlled, research facilities (e.g., exercise laboratories) under the supervision of research staff whereas unsupervised activities are conducted freely outside of a controlled setting without any supervision. Studies with the following criteria were excluded from the review: (1) intervention protocol descriptions and purely qualitative studies; (2) meeting and conference abstracts; and (3) those focused on high-intensity interval training (HIIT) and high-intensity interval training exercise (HIIE). HIIT and HIIE are forms of interval training comprised of alternating intensities of short periods of alternating maximum-effort exercise and recovery periods. 6 The Physical Activity Guidelines Advisory Committee Scientific Report 6 separates HIIT from aerobic PA, and for this review, HIIT and HIIE are excluded as these types of PA differ and deviate from our primary focus on aerobic PA. This review was registered in the PROSPERO registry (CRD42023464374).
Data Extraction
After conducting searches in databases, all resulting references were imported to EndNote reference management software, duplicates were removed, and recorded by one reviewer (NIB). From EndNote, remaining references were exported to Microsoft Excel for screening. The following publication data were included: primary author, publication year, title, and abstract. First, two reviewers (NIB and JH) conducted a pilot screening of titles and abstract. NIB screened all titles and abstracts, and JH then screened a smaller sample (20%) of the titles and abstracts. Full-text screening was independently conducted by one reviewer (NIB) and one reviewer (JH) screened 20% of the articles. No disagreements were found.
Study Quality Assessment
Study quality was assessed independently by two reviewers (NB and JH) using the National Heart, Lung, and Blood Institute Study Quality Assessment Tools (i.e., controlled intervention studies and observational cohort studies). 14 The 14-item Quality Assessment of Controlled Intervention Studies was used to assess the quality of randomized studies. The 14-item Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies was used to evaluate the quality of observational studies. The response options to each item/criterion of tool consists of “yes,” “no,” or “cannot determine/not reported/not applicable.” Responses of “yes” were assigned a score of 1 and responses of “no” or “cannot determine/not reported/not applicable” were assigned a score of “0.” Total scores were summed across the 14 items. Study quality was rated based on the following ranges: poor (0-4 “yes” responses), fair (5-10 “yes” responses), or “good” (11-14 “yes” responses).
Results
A total of 4201 articles were retrieved from searching PubMed, CINAHL, and SPORTDiscus. After duplicates and retracted articles were removed (n = 1518), titles and abstracts were screened (n = 2683) with 2638 exclusions. The full text of 43 articles were screened and 31 were excluded, with 12 studies meeting the eligibility criteria for inclusion. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart is shown in Figure 2. PRISMA Flow Chart.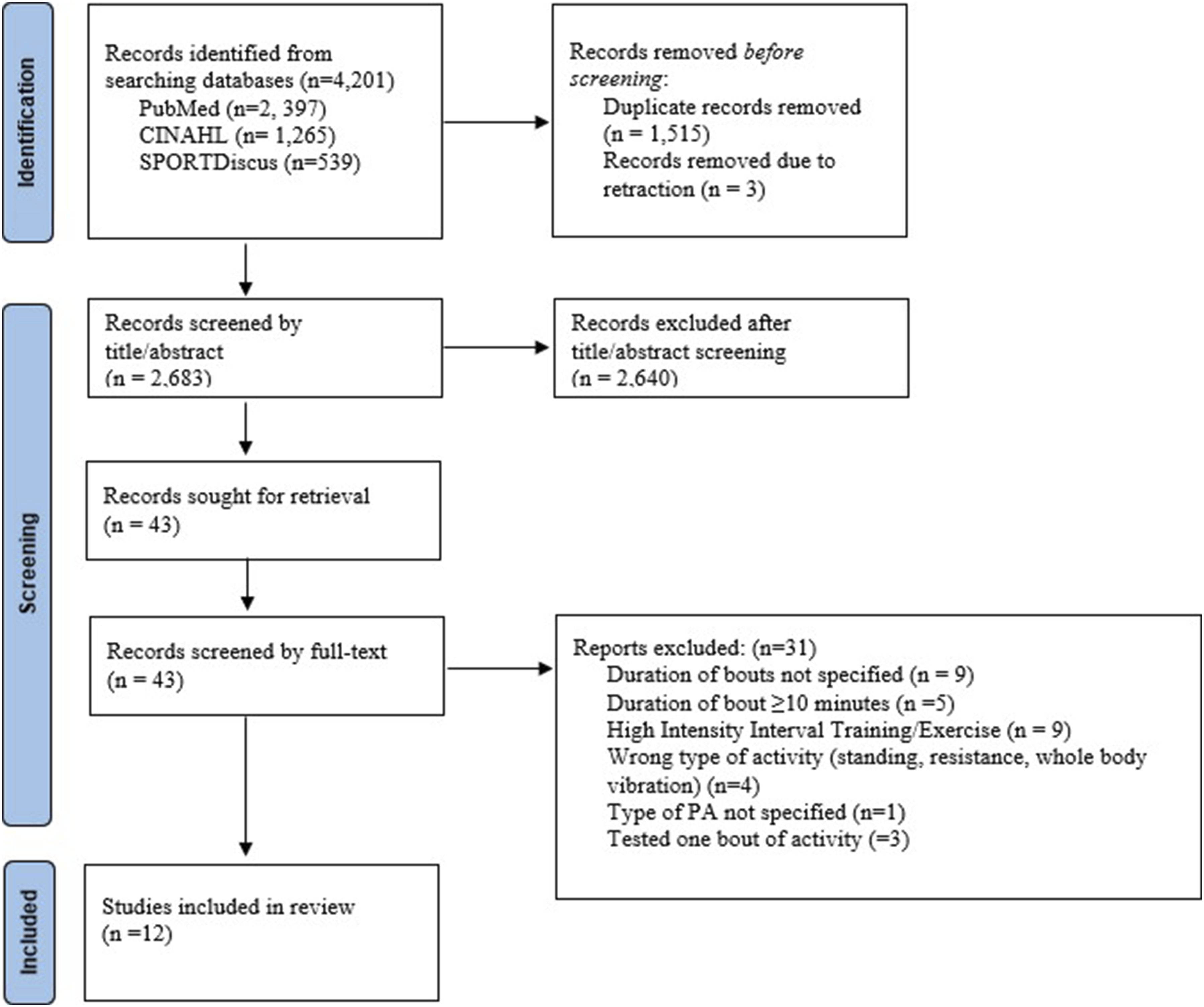
Study Characteristics
Overview of Included Studies.
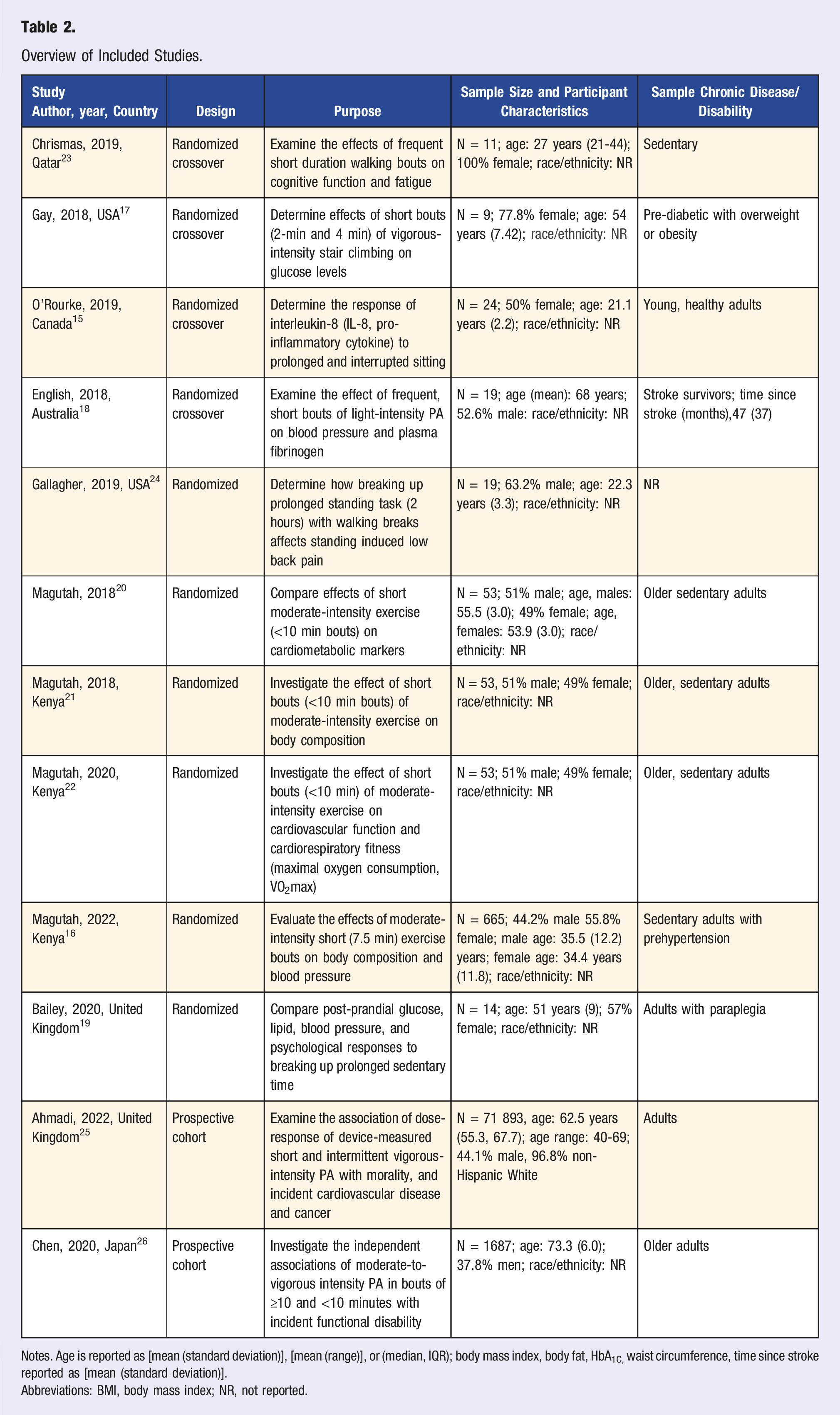
Notes. Age is reported as [mean (standard deviation)], [mean (range)], or (median, IQR); body mass index, body fat, HbA1C, waist circumference, time since stroke reported as [mean (standard deviation)].
Abbreviations: BMI, body mass index; NR, not reported.
Intervention Characteristics
Intervention Characteristics and Findings of Included Studies.
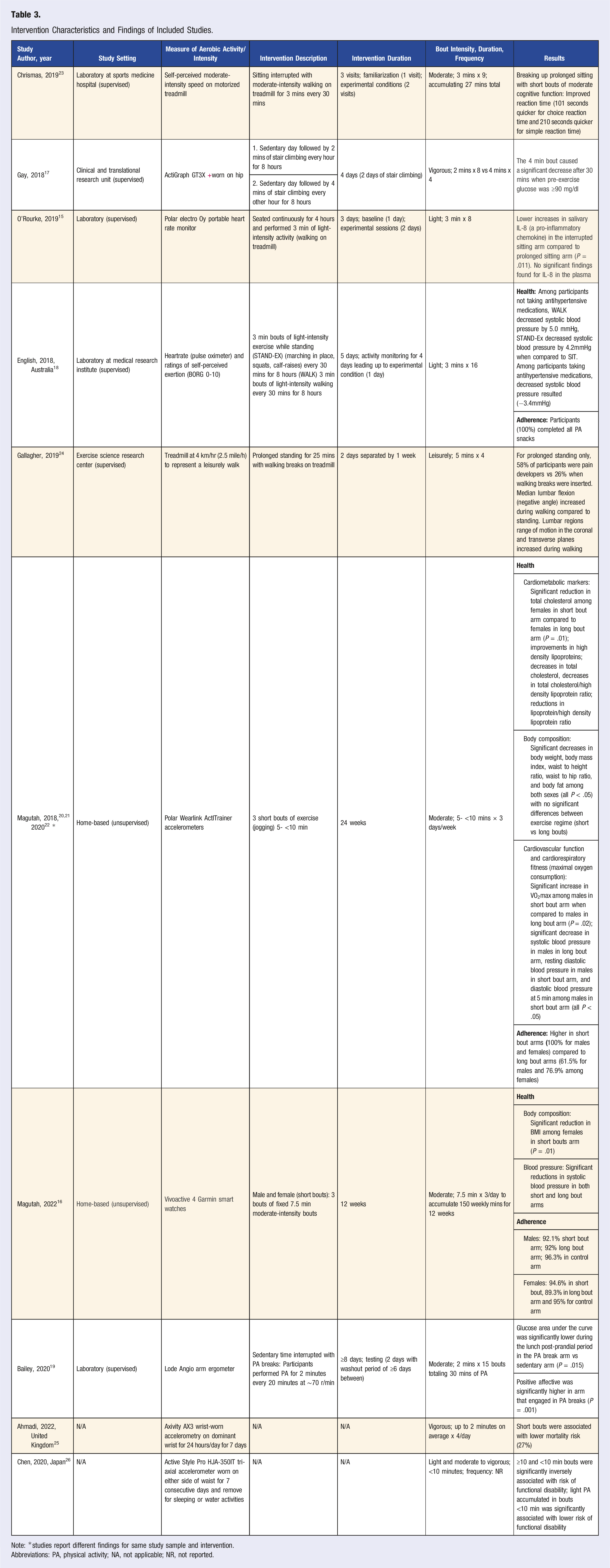
Note: *studies report different findings for same study sample and intervention.
Abbreviations: PA, physical activity; NA, not applicable; NR, not reported.
Setting
Half of the studies (n = 6) were conducted in a supervised laboratory or research unit.15,17-19,23,24 The other half were home-based studies (n = 6).16,20-22,25,26
PA Snacks
Bout duration, frequency, and intensity varied for PA snacks. The bouts ranged from less than 2 minutes up to no more than 10 minutes. The majority of the interventions or studies assessed (n = 7) bouts lasting 5 minutes or less.15,17-19,23-25 One study instructed participants to engage in multiple fixed bouts of 7.5 minutes, three times per day each week to meet the PA guidelines of 150 minutes per week. 16 A total of four studies did not impose a fixed duration time but prescribed or assessed a range or maximum of activity minutes.20-22,26 Specifically, three of these studies prescribed bouts of activity lasting between 5 minutes but less than 10 minutes three times per day on a daily basis.20-22 The other study assessed bouts that were less than 10 minutes in duration per day. 26
Intensities for PA snacks ranged from light to vigorous. Half of the included studies (n = 6) prescribed or assessed moderate-intensity bouts of activity.16,19-23 Three studies assessed the effects of light intensity or leisure activity,15,18,24 and two examined vigorous-intensity bouts.17,25 One study examined the associations of bouts with multiple intensities (i.e., light and moderate to vigorous). 26
PA Measurement
There was variability among the studies with regard to the devices used to measure and assess PA. Accelerometer-based activity monitors (i.e., Actigraph, Axivity, Garmin Vivoactive smartwatch, and Active Style Pro) were used in the majority of the studies (n = 7) to objectively measure activity and intensity.16,17,20-22,25,26 Heart rate monitors (i.e., Polar and pulse oximeters) were used to assess intensity of activity in two studies.15,18 Two studies used self-perceived intensity 23 and exertion (i.e., using the BORG 0-10) 18 to measure intensity of activity. One study used two methods (i.e., objective and subjective) to measure intensity (i.e., pulse oximeter and self-perceived exertion BORG 0-10). One study used miles per hour to represent the intensity of a leisure walk. 24 Specific equipment such as treadmills23,24 and arm ergometers 19 were used in three studies.
Health-Related Outcomes
All 12 of the included studies reported health-related outcomes as shown in Table 3. Two studies reported significant reductions in body composition (e.g., body weight, body mass index, and body fat).21,22 Cardiometabolic markers were assessed in half of the studies (n = 6)16-20,22 with reports of significant decreases in glucose,17,19 total cholesterol, 20 and blood pressure.16,18,22 Response of pro-inflammatory cytokines (i.e., salivary and plasma interleukin-8 (IL-8)) was examined in one study 15 and results showed significantly lower increases in salivary IL-8. One study reported reduction in low back pain reports. 24 Cognitive function (i.e., attention and executive function) and fatigue outcomes were assessed in one study 23 and findings consisted of significantly improved reaction time, yet no effects on fatigue. Two studies examined the mortality risk and risk of functional disability 26 showing decreased risk for both outcomes. Five of the included studies reported health-related outcomes for comparison arms (i.e., traditional PA prescriptions of 30 min bouts and controls).16,20-22 Four of these studies reported similar positive health outcomes consisting of improvements in cardiometabolic markers (e.g., increases in high density lipoproteins, decreases in total cholesterol, decreases in total cholesterol/high density lipoprotein ratio), 20 body composition (e.g., body weight, BMI, and percent body fat), 21 and cardiovascular function (systolic and diastolic blood pressure) and cardiorespiratory fitness (i.e., maximal oxygen consumption,VO2max). 22 Another study 26 reported that MVPA in bouts of ≥10 mins was independently associated with a lower risk of functional disability.
Adherence Outcomes
Adherence outcomes are shown in Table 3. Adherence to intervention protocol (i.e., supervised and unsupervised) was applicable for 10 of the 12 included studies. Three of the four studies (i.e., three using the same sample of participants) used home-based assessed adherence via written exercise logs kept by participants and activity monitors. These studies reported that 100% of participants in the short bout arms adhered to the 24-week exercise prescription while 61.5% of males and 76.9% of females in the long bout arm adhered.20-22 Furthermore, the weekly cumulative minutes of exercise were similar in both the short and long bout arms by sex (males: short vs long bout: 161.8 ± 7.2 mins vs 162.56 ± 6.1 mins, respectively; females: short vs long bout: 158.3 ± 3.6 mins vs 156.05 ± 2.7 mins, respectively). One study measured adherence based on activity monitors and written exercise logs and reported similar levels of adherence by sex and study arm (i.e., short bouts, long bouts) with levels ranging from 89.3% to 92.1%. 16 Activity monitor data from this study also showed similar weekly total minutes of exercise for the short and long bouts (155.6 ± 2.9 mins vs 154.5 ± 2 mins, respectively) for male participants and 154.6 + 3.1 vs 154.7 + 3.1 for females. 16 Adherence to PA intervention while supervised at a laboratory was applicable for six of the included studies with only one study 18 reporting that 100% of participants adhered to the protocol. A total of four studies (i.e., three reporting on the same sample) reported adherence for comparison groups (e.g., PA bouts ≥10 mins).16,20-22 Overall, adherences rates among the comparison groups were lower, with levels ranging from 61.5% to 89.3% and variance in levels between sexes.
Study Quality Assessment
Study Quality Assessment.
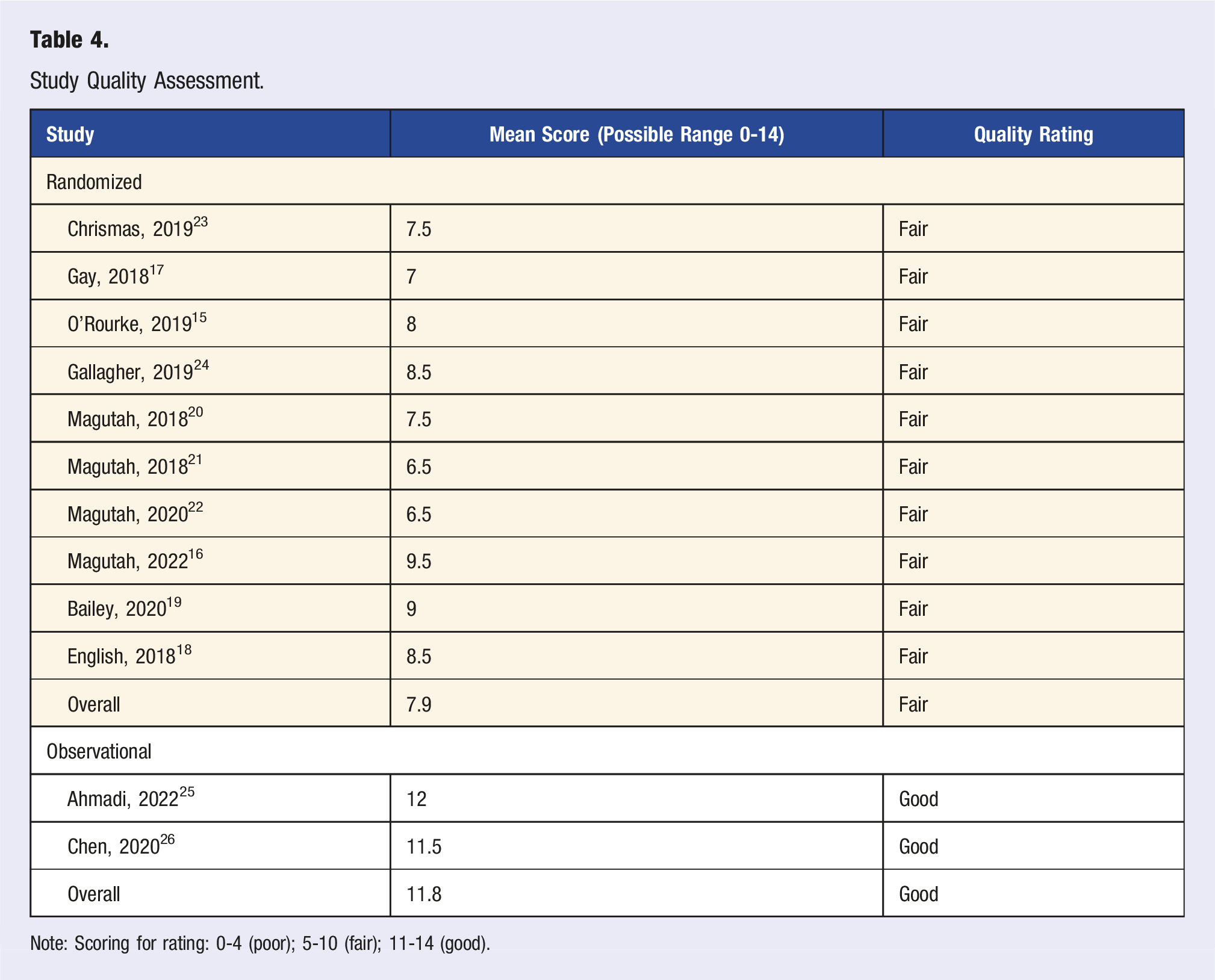
Note: Scoring for rating: 0-4 (poor); 5-10 (fair); 11-14 (good).
Discussion
We identified 12 studies assessing the health impacts and/or adherence related to prescribing or recommending PA snacks among adults. Most studies were conducted among adults that exhibited sedentary behavioral patterns and/or had a chronic disease. Overall, the health outcomes assessed support prescribing or recommending multiple short bouts of activity to adults as positive. Significant effects were observed for body composition, glucose, pain, cardiometabolic markers and cardiovascular function. As for evaluation of adherence to short bouts and PA intervention, the results were limited, yet promising as participants generally adhered to the prescribed short bouts and significantly increased their levels of PA. Based on the use of the NHLBI Study Quality Assessment Tool, the majority of studies (n = 10; 83.3%) were rated as fair. The quality assessment criteria for RCTs criteria were more rigorous corresponding with lower ratings (i.e., fair) in comparison to the prospective cohort studies with good ratings. Findings presented in this review have implications for various groups including researchers, health care providers, and allied health professionals working with adults to increase engagement in PA and adherence to established PA guidelines.
Health Outcomes
The second edition of the Physical Activity Guidelines for Americans 6 eliminated the requirement of PA bouts lasting at least 10 minutes to count toward meeting guidelines as it has been recognized that bouts of any length, specifically moderate-to-vigorous intensity PA, are beneficial. A previous review highlighted the health-related impacts of short bouts of PA (<10 minutes) among adults. 5 Jakicic and colleagues conducted a systematic review to determine whether there were health-related benefits of engaging in multiple short bouts of PA for <10 minutes vs >10 minutes. 5 Overall, health-related effects on weight or body composition, blood pressure, lipids, glycemic control, metabolic syndrome, c-reactive protein, cardiovascular disease risk score, frailty, multimorbidity, and all-cause mortality were observed regardless of bout duration (<10 minutes vs ≥ 10 minutes). 5 Similar to this previous review, we found health-related benefits for body composition, cardiometabolic markers and mortality risk for bouts <10 minutes. Additionally, we also found significant benefits related to cognitive function, protein (i.e., related to inflammation), pain, cardiovascular function, and cardiorespiratory fitness (i.e., maximal oxygen uptake, VO2max), and functional disability. The recent review focused on exercise snacks (i.e., higher intensity, vigorous exercise) also reported modest improvements in cardiorespiratory fitness. 11 When comparing the health outcomes of longer bouts of traditionally recommended PA bouts ≥10 minutes (i.e., 10 mins – 3 times per day, 15 mins – 2 times per day, or 30 mins – once a day), we found similar positive findings for the previously mentioned health outcomes. Taken together, the health benefits observed from engaging in multiple short bouts of PA were shown to produce equally or similar health outcomes as longer bouts further highlighting the advantages of prescribing activity in shorter bouts.
Adherence
Adherence to supervised and unsupervised short bout PA intervention protocols was explicitly reported in five studies (i.e., three conducted among same sample).16,18,20-22 Four of these studies were home-based and used objective and subjective measures to assess adherence to intervention, with reports of high adherence to short bouts at 12 weeks (94.6% among females and 92.1% among males) and 24 weeks (100% for both females and males) follow-up. One study conducted in a supervised laboratory reported 100% adherence to the intervention protocol. 18 These findings are comparable to the adherence rates (80%–100%) for studies included in the Jones et al. review focused on exercise snacks. 11 Several supervised studies were conducted in a laboratory, but adherence was not reported. Thus, it is unclear to what extent participants adhered with the protocol. However, it could be implied that the participants within these studies adhered fully as they were supervised within controlled environments. Despite the reporting from the few studies, there is need for better reporting for future studies.
Four studies16,20-22 had the goal of increasing PA and increasing adherence to the PA guidelines. Three of these studies (i.e., two conducted using the same sample) reported cumulative minutes of PA/exercise at follow-up.20-22 Among sedentary adults with prehypertension, cumulative moderate-intensity exercise minutes were similar (>150 minutes) for both interventional groups at 24 weeks. 16 Similarly, in another study, cumulative minutes of moderate-intensity exercise was >150 minutes at 12-week follow-up. 16 Both of these findings are noteworthy as this sheds light on prescribing short bouts of aerobic physical activity to successfully increase levels of activity and adherence to established PA guidelines, especially given the extremely low rates of PA and prevalence of meeting the guidelines.
Directions for Future Research
Prescribing or recommending short bouts (<10 minutes) of varying intensity activity was effective for reducing and/or improving several health-related outcomes and increasing levels of PA. Further, studies that compared short bouts (<10 minutes) and longer bouts (≥10 minutes) showed that positive health outcomes were produced regardless of the bout duration. For researchers, when developing future PA interventions among adult populations (i.e., healthy, sedentary, have a chronic disease or disability), short bouts should be considered in addition to the traditional recommendations. While the activities in this review included common activities such as walking, jogging, and stair climbing, other daily activities that can serve as PA snacks (e.g., marching in place while coffee brews, quick household chores) should be considered. For health care providers who provide PA counseling or recommendations, it is important to address the frequently reported PA barriers with PA snacks. Based on the high adherence to prescribed PA snacks, health care providers should consider recommending PA snacks instead of longer bouts of activity. Providing examples of activities that can be completed in short bouts can be more palatable for patients. Addressing the common barriers of time, high costs of facilities/resources, lack of social support are pertinent to increasing PA.
Strengths and Limitations
No review (to our knowledge) has examined the impact on adherence to the prescription of short bouts, a main focus for this review. While this review was systematic, it was a rapid review conducted for literature published between January 2018 and September 2023. Further, race and ethnicity were not reported for most of the included studies, with only one study reporting a predominately non-Hispanic White sample of adults (96.8%). Generalizability of these findings to other racial and ethnic groups, as well as to individuals without chronic conditions, may be limited suggesting areas warranting further research.
Conclusions
This review both supports and extends health-related benefits from recent reviews focused on PA and exercise snacks and provides preliminary insights in relation to adherence. The findings suggest that promoting PA snacks in comparison to longer bouts ≥10 minutes to adults could be a promising approach for increasing levels of PA and adherence to established PA guidelines.
Footnotes
Acknowledgments
We would like to thank Allison Howard, a librarian at the University of South Florida for her efforts in helping with the search strategy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Nashira I. Brown’s work was funded by the National Cancer Institute while postdoctoral fellow at H. Lee Moffitt Cancer Center and Research Institute (T32CA090314; MPIs: S. T. Vadaparampil and V.N. Simmons).
Search Strategy.
Database
Search Strategy
PubMed
((“Intermittent activity” [tiab] OR “intermittent exercise” [tiab] OR “accumulated activity” [tiab] OR bouts [tiab]) AND (“physical activity” [tiab] OR “Exercise” (mh) OR “Exercise” [tiab]))
NOT (“Animals” [Mesh] NOT (“Animals” [Mesh] AND “Humans” [Mesh])) filters: years: 2018-2023
Limit: English language
CINAHL
S2 (((MH “Animals+”) OR (MH “Animal studies”) OR (TI “animal model*”)) NOT (MH “human”))
S1 (“intermittent activity” OR “intermittent exercise” OR “accumulated activity” OR bouts) ) AND (“physical activity” OR (MH “physical activity”) OR exercise OR (MH “exercise”))
S1 NOT S2
Filters: years: 2018-2023
English language
Peer reviewed
Exclude MEDLINE records
SPORTDiscus
((DE “PHYSICAL activity”) OR (DE “EXERCISE”)) AND ((DE “INTERVAL training”) OR “intermittent activity” OR “intermittent exercise” OR “accumulated activity” OR bouts) filter: Published date: 20180101-20231231; peer reviewed; language: English; document type: Article