
Abstract
Group medical visits (GMVs) are effective in addressing care gaps for chronic diseases and patient education on healthy lifestyle interventions. This quality improvement project modified a previously piloted sleep and stress management GMV program, implemented the enhanced program, then evaluated its efficacy through pre- and post-surveys. Patients self-identified or were identified by a provider as having poor stress management skills, generalized anxiety disorders, insomnia, and/or poor sleep habits. The virtual GMV series compromised four 90-minute, biweekly visits from April to May 2024. Sleep was measured via the Pittsburgh Sleep Quality Index (PSQI) and stress with the Perceived Stress Scale (PSS). Twenty-two patients were initially enrolled, eight dropped out, four did not attend any visits, and one attended only one visit without completing surveys. Surveys included demographic questions, the PSQI, the PSS, and were completed before the first visit and after the last visit. The final sample included ten participants, and the majority (90%) attended 3 or 4 GMVs. The mean age (SD) was 53.10 (17.36) years, the majority were female (90%), and worked full-time (60%). Participants who attended 2-4 GMVs experienced a statistically significant increase in sleep quality; however, there was no significant improvement in perceived stress.
Keywords
“Past literature has shown a decrease in stress when addressed alone, as opposed to being combined with sleep quality.”
Introduction
Group medical visits (GMVs), also called shared medical appointments, are utilized to address chronic diseases and gaps in patient education, particularly regarding healthy lifestyle interventions. Group care models have been shown to have no adverse effects, increase the quality of care, and have lowered the cost of some health conditions. 1 Poor sleep and increased stress are two of the most prevalent issues in primary care.2-4 As high as 50% of the general population experiences insomnia symptoms, and 5%-20% are diagnosed with an insomnia disorder. 4 Seventy-six percent of American adults report their health was negatively impacted in the past month due to stress, 35% report stress is completely overwhelming most days, and 30% report their daily stress is so high they feel numb. 5 Sleep is an independent risk factor for mental health difficulties, regardless of severity or comorbidity. 6
Poor sleep quality and heightened stress have been successfully treated with GMVs.7-9 Mirsky et al conducted a study demonstrating the success of virtual group medical visits in educating patients on healthy lifestyle interventions. The study revealed that individuals who attended five or more GMVs focused on healthy lifestyle changes reported maintaining “some” or “a lot” of these changes in 89% of cases, in particular healthier eating, increasing physical activity, weight loss, and stress reduction 10 . A six-session weekly virtual GMV sleep behavior program for older adults significantly enhanced sleep quality, diminish maladaptive sleep hygiene behaviors, and reduced daytime sleepiness when compared to a control group who received no interventions. Each session lasted 30 minutes and was dedicated to teaching various aspects of sleep hygiene such as stimulus control, mindfulness, relaxation techniques, the relationship between sleep and physical activity, common sleep myths, and recommended sleep duration guidelines. Participants were actively engaged by setting goals during each session, sharing their progress with the group, and discussing barriers they encountered. 9
At present, little is known about the benefit of combining the topics of sleep quality and stress management into a four-session GMV series. This quality improvement project aimed to develop four 90-minute visits, utilizing previously developed sleep and stress management GMV content, to educate patients about sleep and stress, as well as evidence-based management tools and techniques; implement the enhanced sleep and stress GMV series, then evaluate the impact of the enhanced GMV program on patients’ perceived stress and sleep quality.
Methods
Setting
The group medical visits were delivered virtually through the electronic medical record (EMR) video platform, Vidyo. There were a total of four biweekly visits, which took place on Wednesday nights from 6 p.m. to 7:30 pm, from April 2024 to May 2024. All participants were patients of a primary care practice, located 70 miles north of Pittsburgh, Pennsylvania. This practice is part of a large healthcare organization. The GMVs were delivered through the organization’s lifestyle medicine program. Personnel involved in day-to-day activities include the product lead, site representative, and Lifestyle Medicine Project Manager (LMPM).
Sample
Participants were either self- or provider-identified as having poor stress management skills, generalized anxiety disorders, insomnia, and/or poor sleep habits. Inclusion criteria included English speaking, and the ability to use a smart device to access the mobile phone application. Exclusion criteria included those with severe medical disorders that would interfere with participation.
Intervention
This was a quality improvement project that utilized a pre- and post-implementation design. After patients were identified, the provider notified the LMPM, who reached out to patients. The LMPM then verified the patient was available at the scheduled GMV times, and obtained consent for participation in the GMVs. The patients were then assigned the GMV appointments, which appeared as a virtual medical visit in their phone application.
GMV Titles and Topics.
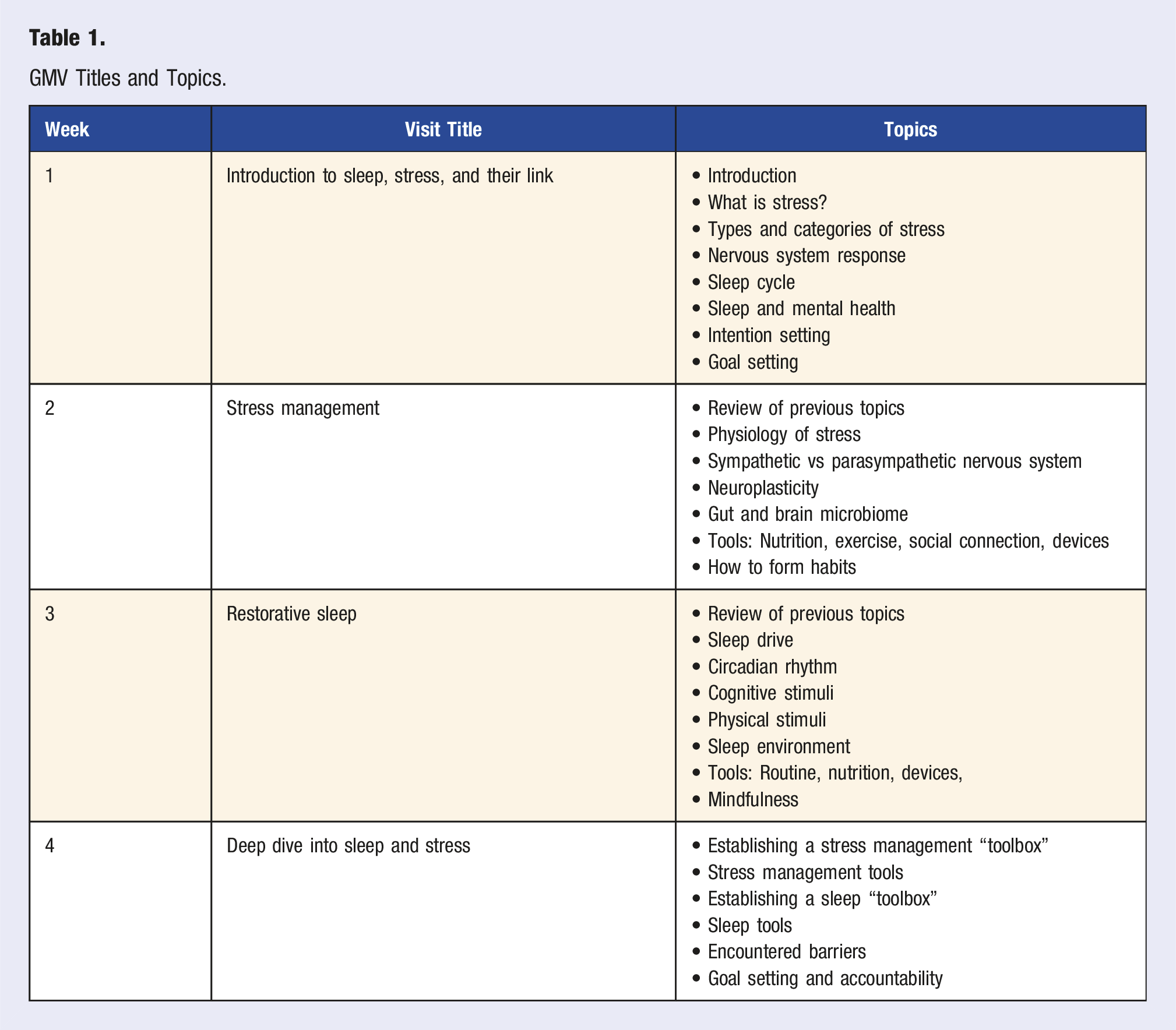
Following each visit, patients were provided with the utilized PowerPoint slides, notes, and links to resources in the Patient Education section of their After Visit Summary. An After Visit Summary document is created after each visit in this healthcare organization, and providers can add content to the Patient Education section. The document is then available through the patient’s portal.
Data Collection
The primary means of data collection was the patient-reported surveys. Before the first appointment, the LMPM sent patients the pre-survey link through the EMR’s patient portal via the secure messaging feature. This message could then be accessed by patients on a desktop or smart device. After the fourth appointment, the LMPM sent patients the post-survey link through the same secure messaging portal. The utilized survey platform was Microsoft Forms, which was hosted on the healthcare organization’s secure network.
Demographic information was also collected via pre- and post-surveys. The pre-survey collected age, sex, employment status, presence of chronic illness, asked if they were currently taking any medications for stress, anxiety, depression, and/or sleep issues, and if they were currently seeing a therapist or counselor. The post-survey collected employment status, asked if they were currently taking any medications for stress, anxiety, depression, and/or sleep issues, and if they were currently seeing a therapist or counselor. Measurements of stress and sleep quality were also collected via pre- and post-survey. Stress was evaluated by the Perceived Stress Scale, and sleep quality was evaluated by the Pittsburgh Sleep Quality Index (PSQI).12,13
The Perceived Stress Scale (PSS) was designed to quantify the degree of stress caused by situations in individuals’ lives over the past month. The PSS assesses three central components of the experience of stress—the degree to which respondents found their lives unpredictable, uncontrollable, and overloading. It was designed for use in a community sample with at least a junior high school level of education. 14 The original PSS consisted of 14 items, which was later revised to 10 items. Scores are calculated by summing all 10 items, 0 to 4. Items 4, 5, 6, 7, and 8 were scored by reversing the response. For example, an answer of 0 would receive a score of 4, a 1 would receive a score of 3, and a 2 still receives a score of 2. The PSS scores can range from 0 to 40, with a higher score indicating increased perceived stress. 15 This measurement is not a diagnostic instrument, so categories to establish scores as high, medium, or low do not exist. Comparisons can only be drawn from population studies and individual samples. 16 For reference, the PSS was administered to 2000 adults in 2009. The PSS sample mean for men was 15.52 (SD 7.44) and 16.14 (SD 7.54) for women. Individuals who worked full-time scored a mean of 16.23 (SD 7.31) while those who worked part-time scored 15.32 (SD 7.28). 14 Scores correlate with depression and physical symptomatology, life-event scores, utilization of health services, social anxiety, and smoking-reduction maintenance. 13
The Pittsburgh Sleep Quality Index is a reliable and valid tool created to measure sleep quality, discriminate between “good” and “poor” sleepers, and assess for a variety of sleep disturbances that could affect sleep quality. The PSQI has seven domains that assess a variety of factors related to sleep quality. These domains are subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medications, and daytime dysfunction. Each item is weighted 0-3 on a scale. The sum of the scores for the seven domains produces one global score. A global PSQI score >5 indicates the individual is a “poor” sleeper with a sensitivity of 89.6% and a specificity of 86.5%. A global PSQI score of ≤4 indicates the individual is a “good” sleeper. 12
Due to this being a quality improvement project, an exempt protocol was approved by the University’s Human Research Protection Office (HRPO) on April 15, 2024, and the healthcare organization’s quality improvement committee granted this project approval on March 29, 2024.
Results
Demographics
Demographics of Participants.
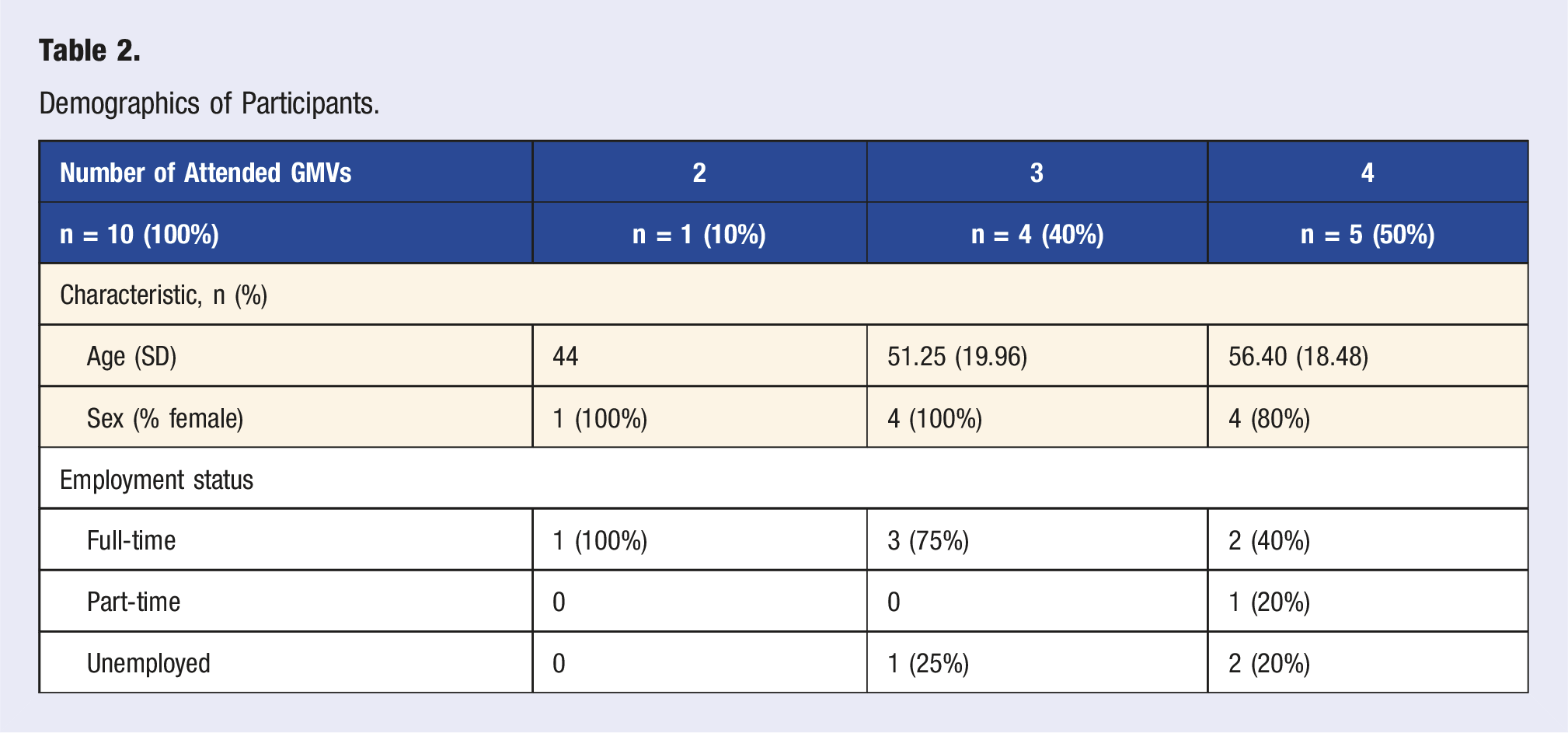
Of the 10 individuals who attended two, three, or four visits, the mean age (SD) was 53.10 (17.36), and they were predominantly female (90%). Six participants (60%) worked full-time, one (10%) worked part-time, and three (30%) were unemployed. Before the intervention, six (60%) participants reported the presence of one or more chronic illnesses, with the average number of chronic diseases being 1.4 (SD 1.35). After the intervention, 5 (55.6%) reported the presence of one or more chronic illnesses, with an average number of 2 (SD 2.06) chronic illnesses per participant. Before and after the intervention, three participants (30% before the intervention, 33% after the intervention) reported taking medications for depression, anxiety, and/or sleep, as well as being seen by a therapist or counselor.
Outcomes
PSS and PSQI Results.
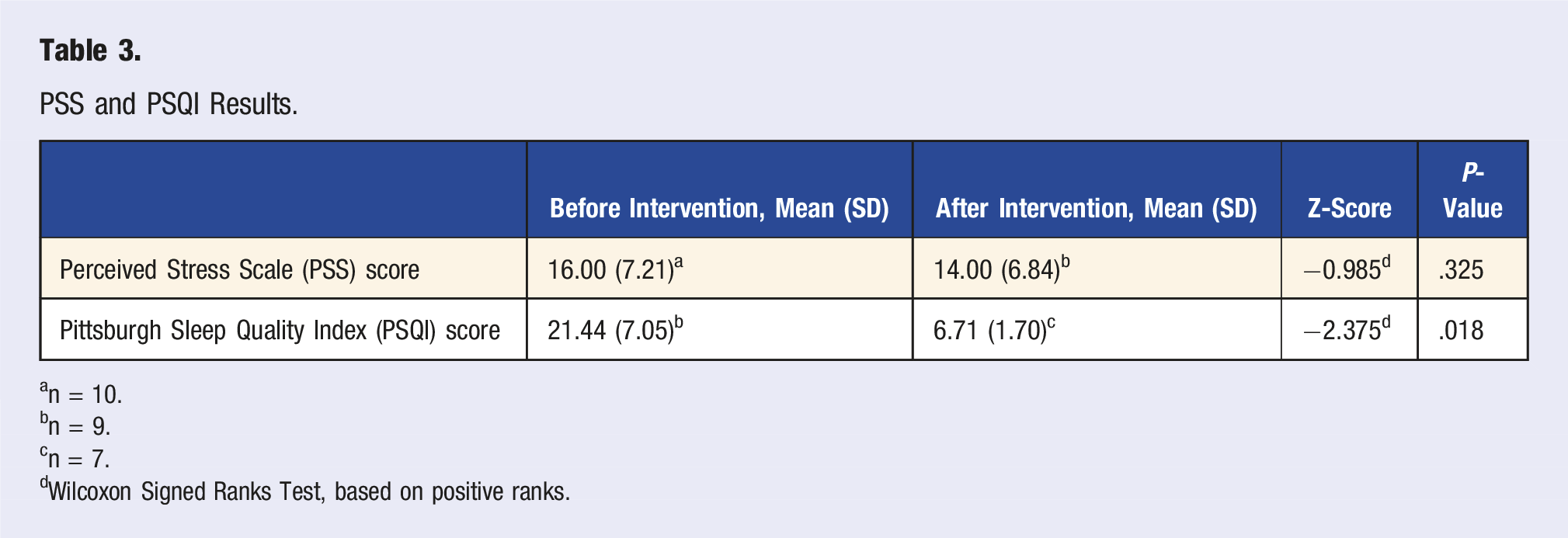
an = 10.
bn = 9.
cn = 7.
dWilcoxon Signed Ranks Test, based on positive ranks.
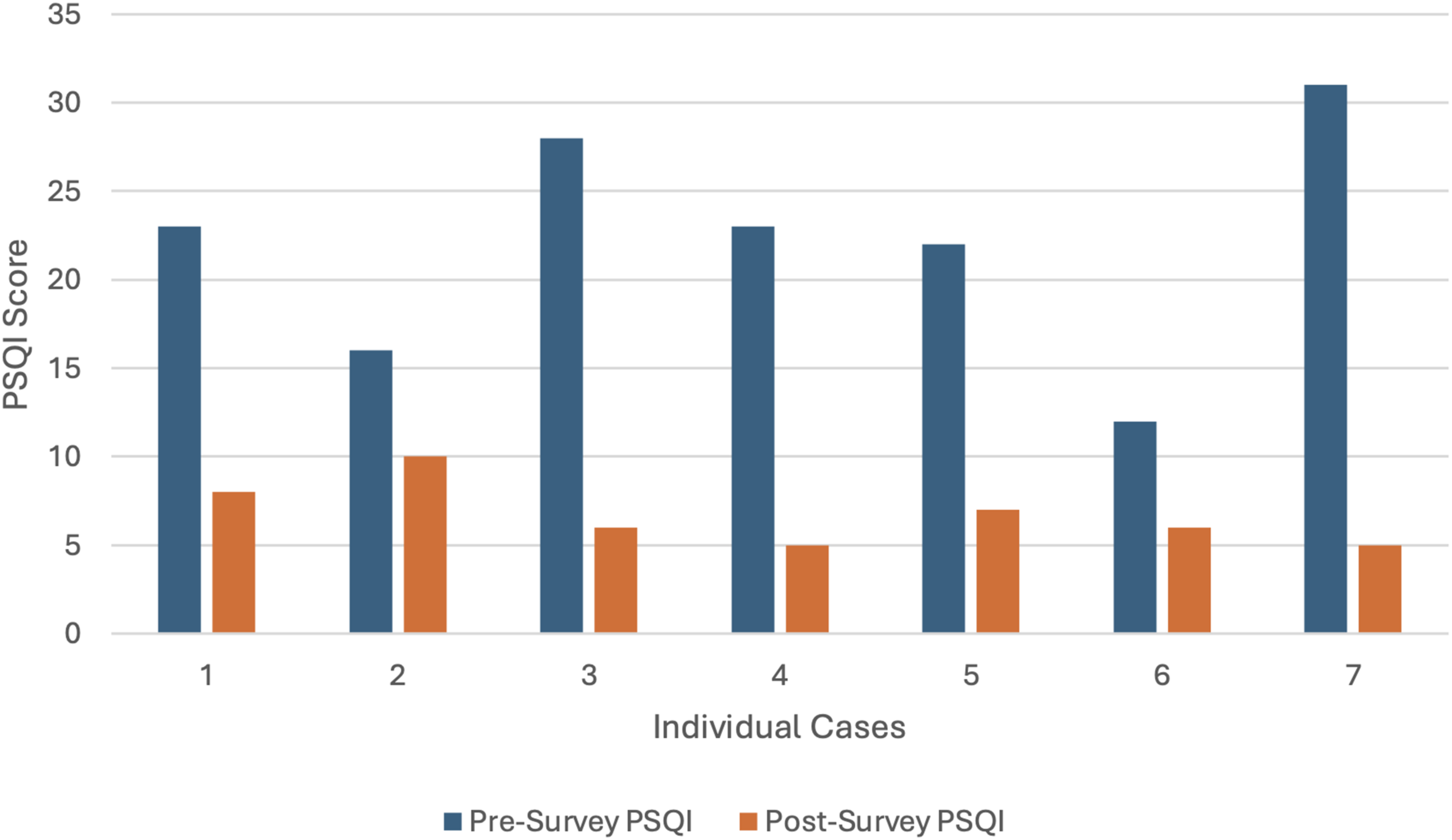
PSQI scores before and after the GMV series.
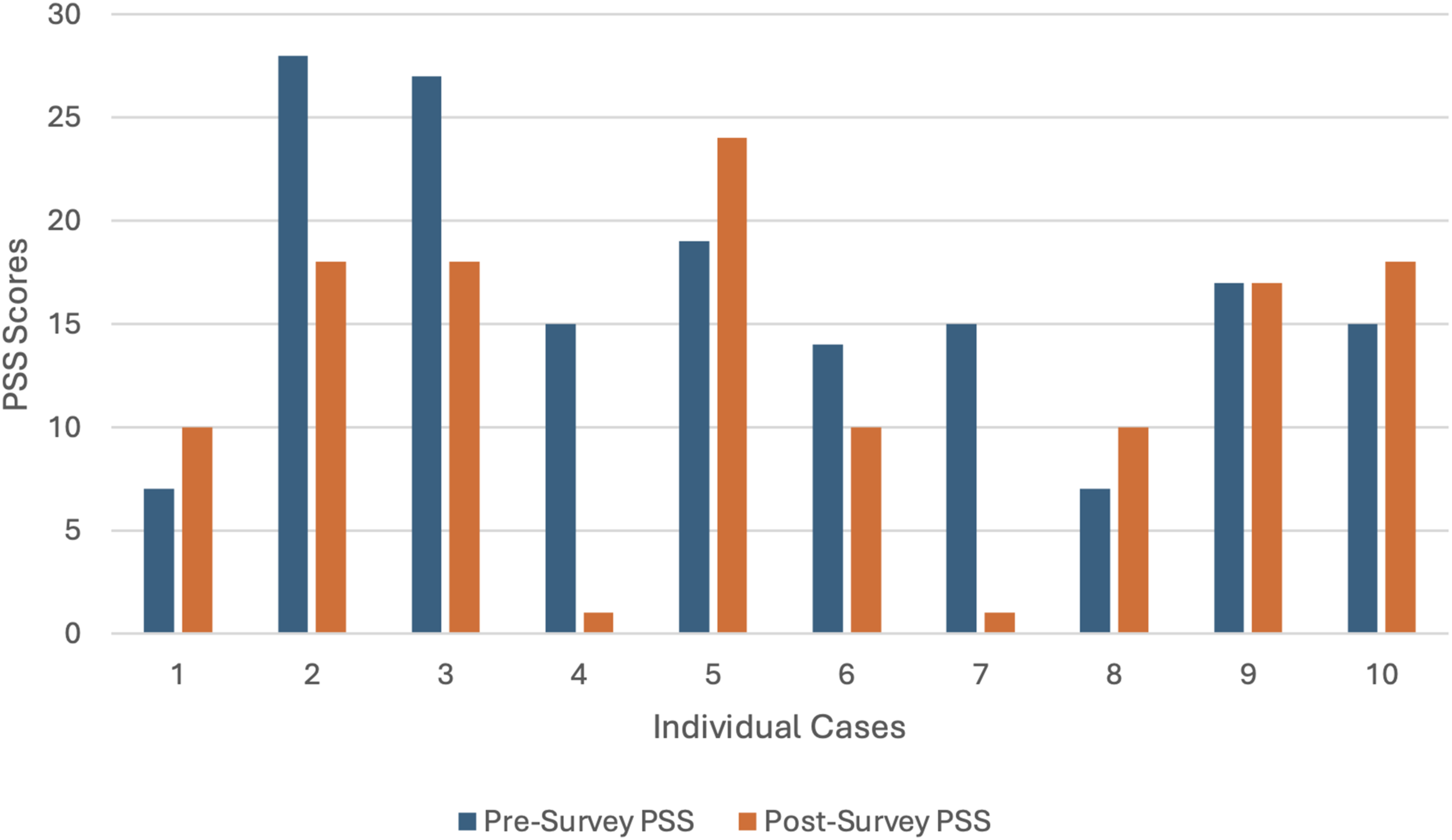
PSS scores before and after the GMV series.
Discussion
The results of this quality improvement project provide data to support further development of this GMV series as improvements in sleep quality, but not perceived stress were found. This was the first set of data collected on this series, so overt conclusions cannot be drawn.
These results are consistent with current literature showing insomnia being efficiently managed with virtual care. A 2022 comprehensive systematic review and meta-analysis showed virtual treatment of insomnia not only accelerates access to sleep services, but also can improve the efficiency of health services in terms of time, cost, and therapeutic effects. 17 Another piloted group-based program focused on sleep behavior change for older adults and observed a significant increase in sleep quality. 9 Virtual group medical visits were also found to effectively increase sleep quality in postmenopausal women with insomnia. 7
The resulting insignificant decrease in stress does not align with the current literature. Lower anxiety and depression, usually scored via GAD-9 and PHQ-9, respectively, are typically seen as results of group medical visits treating stress. GMVs that have successfully treated stress note the exact mechanism of decreased stress is difficult to judge, as there are multiple reasons stress via the GAD-9, PHQ-9, or PSS might be decreased after a GMV series. Several hypothesized reasons include mindfulness-based interventions, education, or group support. 2 Further research is needed to explore this cause, which will likely explain why this GMV series was unsuccessful in decreasing stress.
Research on GMVs lack homogeneity, therefore one series is difficult to compare to another. The length of visits, number of visits, frequency of visits, target populations, and measurement tools are different amongst each group medical visit. For this particular series, future research should perform follow-up measurements for an extended amount of time after the final GMV. It would be in the healthcare organization’s best interest to gather PSQI and PSS results in 1 month, 3 months, and 6 months after the intervention to analyze the lasting benefits of this series. Data should also be collected from the EMR to observe for secondary benefits such as decreased blood pressure, and metabolic changes such as decreased A1C, weight loss, or improved thyroid function. Future research should also address barriers to this GMV controlling stress. Past literature has shown a decrease in stress when addressed alone, as opposed to being combined with sleep quality.8,10 Barriers to attendance, as well as drop-out rates, should also be investigated. Patient polling should be considered to find the time that works best for the target population.
Limitations
Important limitations of this quality improvement project are the potential for historical bias, the Hawthorne effect, and the small sample size. The COVID-19 pandemic resulted in heightened rates of anxiety in all populations. This new heightened anxiety baseline might result in participants reporting higher levels of stress than they would have before the pandemic. The Hawthorne effect is also a possible explanation for the decrease in the PSQI score. Participants were aware their survey responses were being used for quality improvement, and might have reported higher sleep quality to appease the providers. The small sample size is also a limitation, as it doesn’t allow for generalizability.
Strengths
A strength of this study is the measurement tools, the PSQI and PSS. These are both widely recognized as reliable and valid instruments to evaluate sleep quality and perceived stress.12,13 Both tools have also been used to evaluate the efficacy of group medical visits in previous literature.7-9
Conclusion
This 90-minute, four-course program was successfully developed, enhanced, and evaluated for its effects on perceived stress and sleep quality. A statistically significant increase in sleep quality was observed, and stress was not significantly impacted. This GMV series serves as the first, to our knowledge, to treat sleep and stress together. In our clinic, these results suggest that for our patients this GMV series might improve sleep quality and may not improve heightened stress. This GMV series framework could serve as a valuable template for future series or other quality improvement projects to teach patients lifestyle modifications, as well as at other clinics. This program is easily sustainable in a large healthcare system, but might not be appropriate where resources are limited.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr. Melissa Kerr, FNCP, PT, DPT, and Dr. Paul Scott, PhD, for their contributions to this quality improvement project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.