
Abstract
Objective
The objective of this expert consensus process was to define performance measures that can be used to document remission or long-term progress following lifestyle medicine (LM) treatment.
Methods
Expert panel members with experience in intensive, therapeutic lifestyle change (ITLC) developed a list of performance measures for key disease states, using an established process for developing consensus statements adapted for the topic. Proposed performance measures were assessed for consensus using a modified Delphi process.
Results
After a series of meetings and an iterative Delphi process of voting and revision, a final set of 32 performance measures achieved consensus. These were grouped in 10 domains of diseases, conditions, or risk factors, including (1) Cardiac function, (2) Cardiac risk factors, (3) Cardiac medications and procedures, (4) Patient-centered cardiac health, (5) Hypertension, (6) Type 2 diabetes and prediabetes, (7) Metabolic syndrome, (8) Inflammatory conditions, (9) Inflammatory condition patient-centered measures, and (10) Chronic kidney disease.
Conclusion
These measures compose a set of performance standards that can be used to evaluate the effectiveness of LM treatment for these conditions.
Keywords
“The performance measures and remission criteria recommended by our panel provide a basis for quantitating the effectiveness of lifestyle interventions and LM treatment programs.”
Introduction
As the field of lifestyle medicine (LM) expands, 1 the need to define parameters that can be used to evaluate effectiveness of treatment grows. Many clinical practice guidelines do mention lifestyle and health behaviors as important to address in the treatment of chronic disease.2–4 However, no standards exist by which progress or long-term outcomes following lifestyle interventions can be evaluated. This gap poses a barrier to the evaluation of effectiveness of LM treatment, as well as the widespread integration of LM practice into healthcare. There is a need to provide guidance on the best selection of performance measures that can be used to assess LM treatment.
The objective of this expert consensus process was to identify performance measures that can be used to document remission or long-term progress following lifestyle medicine (LM) treatment, thus creating a set of standards that can be used to consistently evaluate the effectiveness and performance of LM treatment.
Methods
This consensus update of the competencies was based on an a priori protocol (previously developed by AAO-HNSF 5 and also used by ACLM 6 to develop expert consensus statements), modified to streamline the process. In this project, the following steps were completed (1) recruit the expert panel, (2) vet potential conflicts of interest among proposed development group members, (3) develop candidate performance measures for voting, (4) develop and implement modified Delphi Method surveys, (5) revise performance measures based on survey results, and (6) assemble performance measures that achieved consensus for presentation.
Choice of Lifestyle Medicine Performance Measures and Expert Panel Recruitment and Vetting
The development of a list of standardized performance measures to assess the effectiveness of LM treatment was a companion process to the expert consensus process undertaken to develop Competencies for LM Intensivists, the methods of which have been previously described. No direct conflicts of interest 7 existed for the chair or the majority of the participants.
Discussion of Performance Measures for Delphi Voting
The expert panel considered various domains of disease and health risk factors proposed by the chair, and approved those included in this document. As each domain was considered, the panel members used their expert opinion and stakeholder needs to identify potential performance measures.
Voting, editing, and revoting using five survey rounds were administered, following the modified Delphi method 8 with surveys distributed in an online survey platform (https://QuestionPro.com) to assess agreement among panel members. As previously described, questions in the survey were answered with a 9-point Likert scale, and established criteria for consensus 5 were used (see Supplemental Table S1). Each survey focused on one domain of disease or risk factors.
The final manuscript was drafted with participation and final review from each panelist, and reviewed and approved by ACLM.
Results
Lifestyle Medicine Clinical Performance Measures for Cardiovascular Health. a
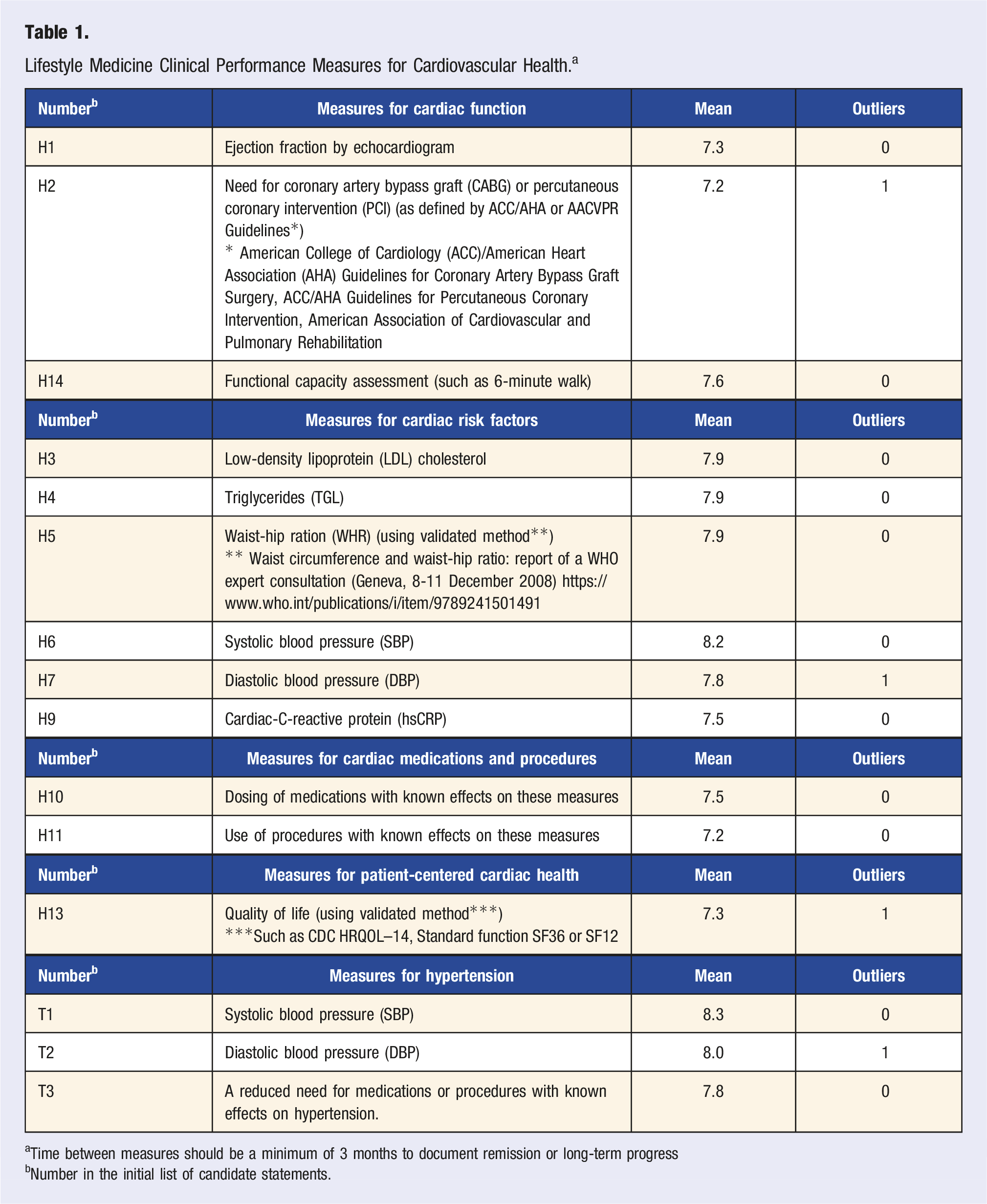
aTime between measures should be a minimum of 3 months to document remission or long-term progress
bNumber in the initial list of candidate statements.
Lifestyle Medicine Performance Measures for Type 2 Diabetes and Prediabetes. a
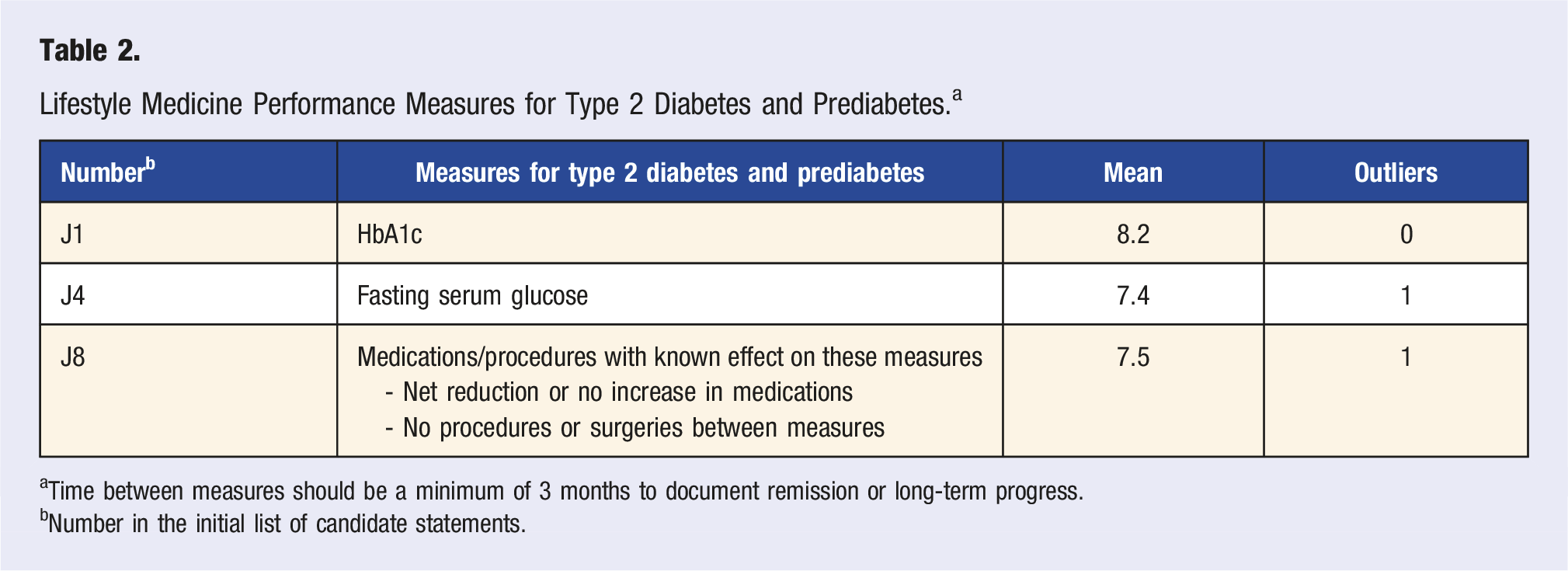
aTime between measures should be a minimum of 3 months to document remission or long-term progress.
bNumber in the initial list of candidate statements.
Lifestyle Medicine Performance Measures for Metabolic Syndrome. a
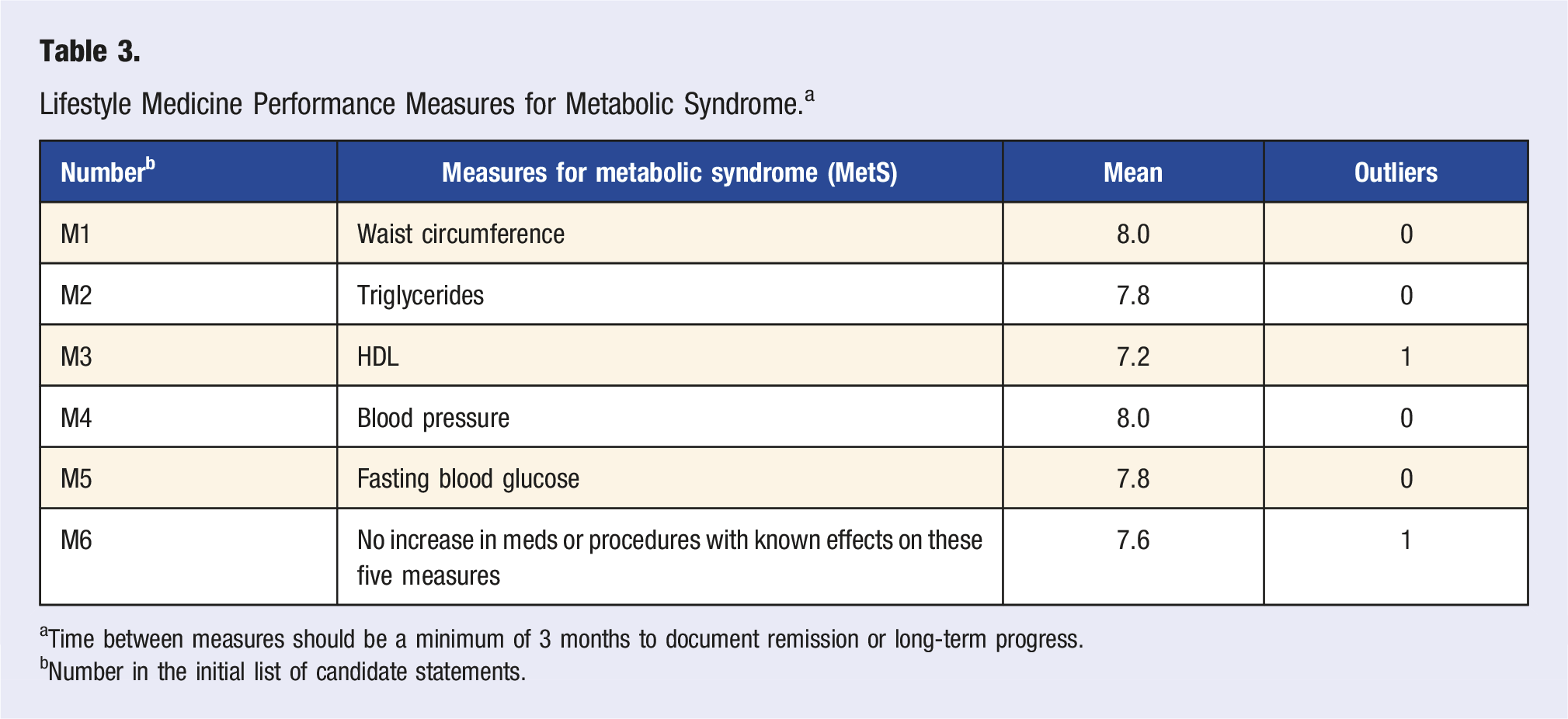
aTime between measures should be a minimum of 3 months to document remission or long-term progress.
bNumber in the initial list of candidate statements.
Lifestyle Medicine Performance Measures for Inflammatory Conditions. a
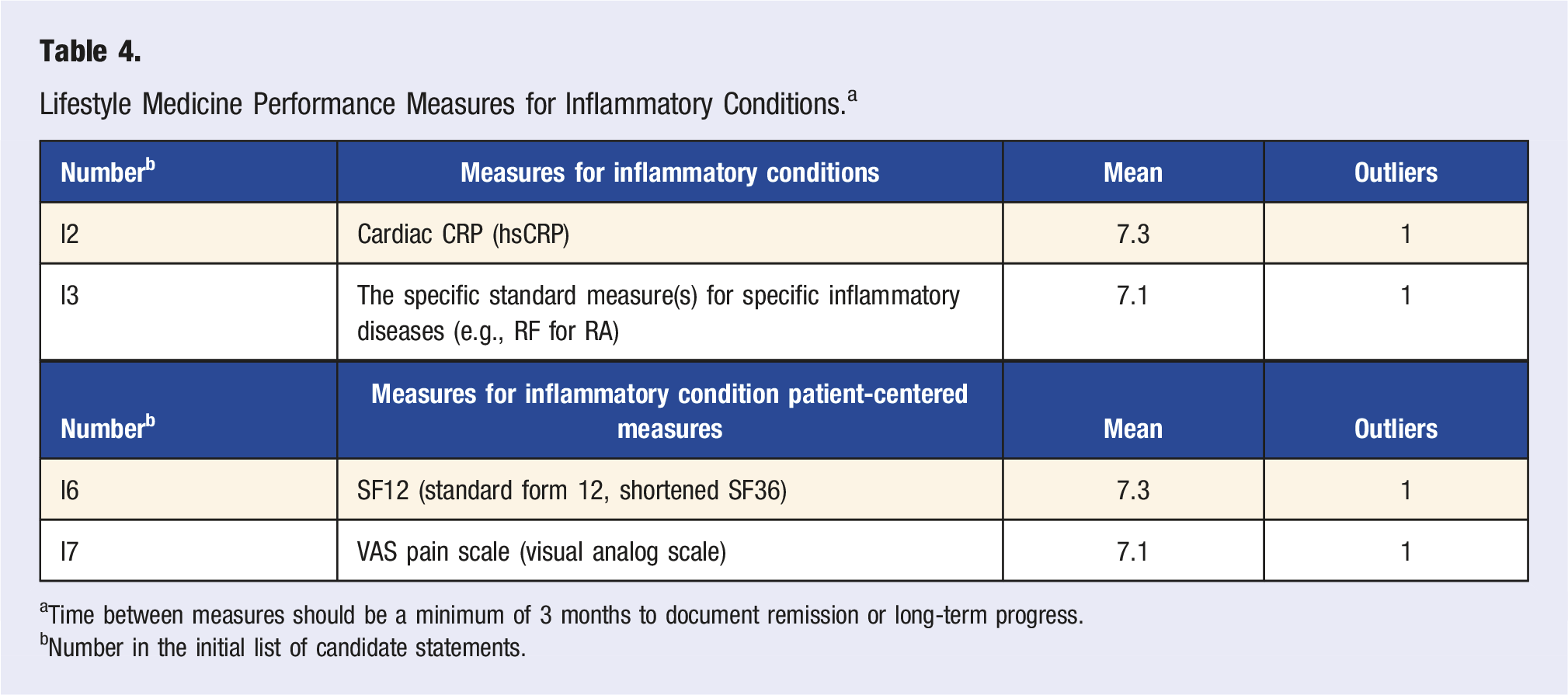
aTime between measures should be a minimum of 3 months to document remission or long-term progress.
bNumber in the initial list of candidate statements.
Lifestyle Medicine Performance Measures for Chronic Kidney Disease. a
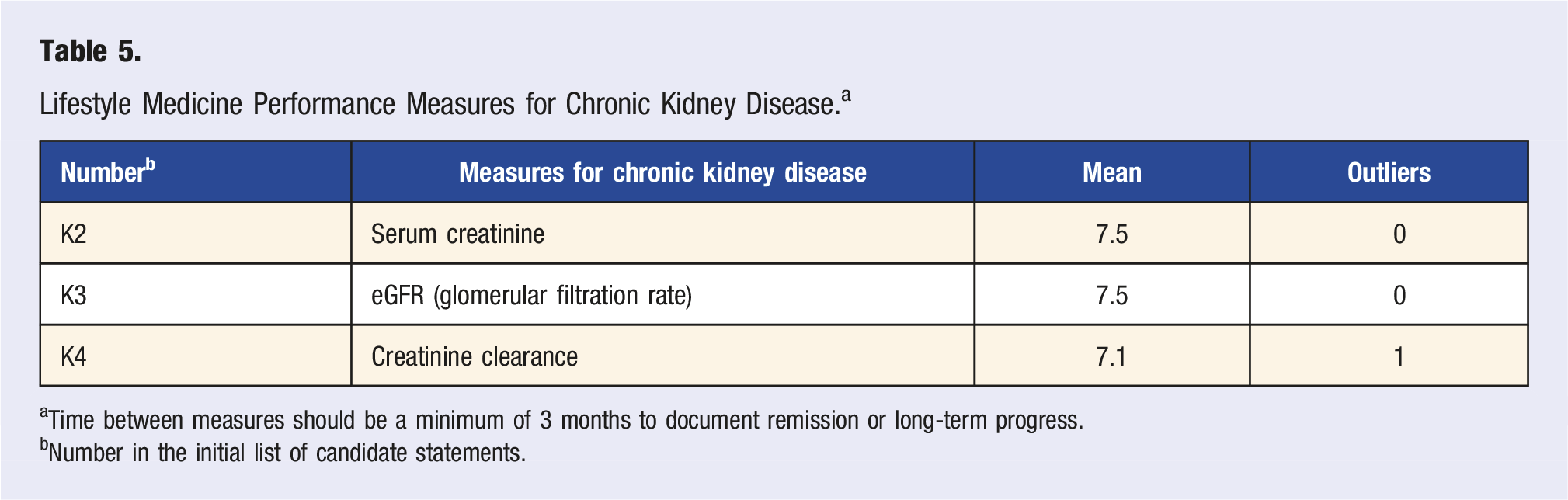
aTime between measures should be a minimum of 3 months to document remission or long-term progress.
bNumber in the initial list of candidate statements.
Discussion
We successfully used an expert consensus process to create a recommended list of LM performance measures, which can serve to set standards for measuring and evaluating the effectiveness of LM treatment. LM generally addresses the underlying harmful lifestyle behaviors that precipitate disease. Since most medications and medical procedures are used to ameliorate the negative effects of disease, it is inevitable that as unhealthful practices are replaced by healthful ones, changes will take place in the measures used to quantitate the need for these medications and procedures. The degree or amount of change in these measures can be used to identify the effectiveness of LM interventions. This is particularly important because of the variability in lifestyle interventions and in the physiologic response of individuals receiving lifestyle interventions.
For example, poor diet and lack of exercise with resulting excess weight often lead to elevated blood pressure and hypertension. This condition is typically treated with antihypertensive medications. In extreme cases, treatment may include bariatric surgery to reduce obesity. Measures of blood pressure and weight are used to help determine when medications and surgery should be prescribed. When lifestyle interventions are used to treat the underlying causes of the condition, the effectiveness of the LM treatment can and should be measured and quantitated using these same measures of blood pressure and weight. Unless these measures improve, the treatment should be considered ineffective.
When the LM treatment is effective and these measures improve, it becomes necessary to reduce the dosing of treatments prescribed to ameliorate the negative effects, 9 which are being reduced by LM treatment. As this process continues and efficacious LM treatment fully reverses 10 the ill-effects of the condition, the negative effects disappear and it becomes necessary to deprescribe other treatments to avoid causing negative effects from inappropriate dosing. This state of non-disease as determined by the failure to meet the recognized criteria for diagnosing the disease constitutes “remission.” as previously defined by this panel. 10 Since the resumption of unhealthful lifestyle practices may produce the same condition, with perhaps even worse negative effects than before, remission is not considered an absolute “cure,” but rather the result of reversing the condition to a point of not meeting these recognized criteria. 10
Therefore, the recommended measures of LM treatment effectiveness include the generally recognized measures of disease/condition severity, such as BP and weight, but also measures of medication dosing and the use of procedures or devices known to affect these measures, such as surgery. In addition to identifying these recommended measures, including the dosage of other treatments affecting the target diseases/conditions, our panel further recommends that LM disease remission generally be defined as not only reducing the disease measures below the threshold for diagnosing the target disease/condition but that this happens with an absence of medications or procedures known to affect those measures.
It should be noted that LM performance is based upon improvements in objective, quantitative measures of disease, not upon measures of treatment processes. LM-effectiveness is based upon disease outcomes resulting from LM treatment, independent of other treatments. This is accomplished by measuring the dosing of other treatments used simultaneously with LM interventions. When improvements occur without an increase in non-LM treatment dosing, it is reasonable to credit the improvement to the LM treatment. Relying on objective and/or validated self-reported metrics to determine the effectiveness of treatment distinguishes LM as a field of medical practice that can be evaluated on equal footing with conventional treatment that may be pharmaceutical, procedural, or surgical, without requiring expensive testing paid of out-of-pocket. Adopting these measures establishes that LM does not rely on unconventional tests for treatment and assessment of patients but instead follows accepted measures of disease status and severity.
It is possible for non-LM treatment dosing to increase in parallel with LM dosing, raising questions about the effectiveness of the LM treatment. At this time no reliable method is known to the authors for quantitating the relative treatment effects of multiple distinct treatments on the same disease, such as medication and surgery, or medication and lifestyle change, besides conducting multi-arm randomized controlled trials. It is only possible to know with certainty that LM treatment is effective in the absence of non-LM treatment, or in cases where there is no increase in non-LM treatment dosing. When other treatments are stopped or remain unchanged, it is reasonable to attribute improvements to the new or added treatment; in this case, LM interventions. As more research is conducted and outcomes evaluated with clear and valid measures such as those listed here, the capacity of lifestyle treatments, and the characteristics needed for effective interventions, will be further clarified. Similarly, as more research on chronic disease states and novel metrics is conducted, the list of performance measures suitable to quantifying LM-effectiveness may expand. Among this panel, some members felt that C-reactive protein (CRP) could be used as an alternative measure to hs-CRP, based on recent research comparing the two measures’ ability to predict cardiovascular disease. 11 Future updates of this ECS will address the evolving research.
As can be seen from the above discussion, the generally accepted measures of disease status or severity recommended for determining LM treatment performance are the same as those identified and used by the relevant disease specialists in their guidance documents, including cardiology,12,13 endocrinology, 14 or nephrology. 15 There is no attempt or intent by our panel to change or replace these generally recognized measures of disease status, progression or remission.
The performance measures and remission criteria recommended by our panel provide a basis for quantitating the effectiveness of lifestyle interventions and LM treatment programs. We encourage these measures to be rigorously recorded, analyzed and reported for all LM endeavors, including research, clinical practice, and educational programming. We recommend that LM certification incorporate the use of these measures in determining the minimum LM proficiency to be certified as diplomates. This would be especially appropriate for advanced certification as a LM Intensivist.
Strengths and Limitations
Strengths of this ECS include the systematic consensus process and expertise of the panel members as previously identified. With their unique experience, they brought critical knowledge and perspective to the development of this list of performance measures. Additionally, using the Delphi methods as a foundation for to find consensus added methodological rigor to the development of the list of performance measures. Limitations of this ECS included the smaller size and make-up of the expert panel, being mostly US based. The number of panelists was limited to the small group of experts skilled in ITLC treatment. In addition, only performance measures for a specific list of common chronic conditions were addressed; all chronic conditions were not. Future work should continue this development to identify performance measures for additional conditions, especially as research continues to develop on the capacity of lifestyle changes to improve them.
Conclusions
These measures compose a set of performance standards that can be used to evaluate the effectiveness of LM treatment. Future work should use these measures in data collection to standardize LM treatment effectiveness and performance. LM certification should make use of these measures in determining minimum proficiency for certification.
Supplemental Material
Supplemental Material - Lifestyle Medicine Performance Measures: An Expert Consensus Statement Defining Metrics to Identify Remission or Long-Term Progress Following Lifestyle Medicine Treatment
Supplemental Material for Lifestyle Medicine Performance Measures: An Expert Consensus Statement Defining Metrics to Identify Remission or Long-Term Progress Following Lifestyle Medicine Treatment by John H. Kelly, MD, MPH, DipABLM, FACLM, Liana Lianov, MD, MPH, FACLM, FACPM, DipABLM, Dexter Shurney, MD, MBA, MPH, FACLM, DipABLM, Sley Tanigawa Guimarães, MD, DipIBLM, Mechelle Palma, MD, MMHA, DipIBLM, FACLM, Caldwell Esselstyn, MD, FACLM, Scott Stoll, MD, FABPMR, Padmaja Patel, MD, FACLM, DipABLM, Brenda Rea, MD, DrPH, PT, RD, FACLM, Koushik Reddy, MD, FACC, FACLM, DipABLM, George Guthrie, MD, MPH, CDCES, CNS, FAAFP, FACLM, Michelle Reiss, MBChB, LMCC, CCFP, FRACGP, FASLM, and Micaela C. Karlsen, PhD, MSPH in American Journal of Lifestyle Medicine.
Footnotes
Acknowledgments
The authors wish to thank the leadership of the American College of Lifestyle Medicine.
Declaration of Conflicting Interests
John H. Kelly: Receives consulting payments from the American College of Lifestyle Medicine; Brenda Rea: Program Director of the Lifestyle Medicine Intensivist Fellowship at Loma Linda University Health; Board Member, American Board of Lifestyle Medicine, employed as Medical Director of Education, American College of Lifestyle Medicine; Liana Lianov: Receives consulting payments from the American College of Lifestyle Medicine; Micaela C. Karlsen: Employed by the American College of Lifestyle Medicine.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This Project was Funded by the American College of Lifestyle Medicine.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.