
Abstract
Purpose: This activity by the Expert Lifestyle Medicine Panel (ELMP) proposes a set of competencies for providers who specialize in the practice of lifestyle medicine (LM), focused on intensive therapeutic lifestyle change. Methods: ELMP invited a core consensus group consisting of 13 providers who specialize in LM and key stakeholders to develop, by consensus, a set of competencies for those specializing in the practice of LM based on the LM core competencies for primary care physicians published in 2010. Two ELMP members (JK and MCK) facilitated and moderated the consensus process conducted by email and teleconference. The competencies were emailed to the consensus group for comment and revision and, through an iterative process, full consensus was reached by the 13-member group. Competencies were organized into the 6 Accreditation Council for Graduate Medical Education and American Board of Medical Specialties (ACGME/ABMS) categories. Results: The final set of competencies consist of 34 competencies in the 6 ACGME/ABMS categories. Conclusion: This new set of competencies will provide guidance for the education, certification, and practice of lifestyle medicine by physicians and other health providers who specialize in the practice of intensive lifestyle medicine treatment.
Keywords
‘Physicians have cited inadequate confidence and lack of knowledge and skill as major barriers to counseling patients about lifestyle interventions.’
The leading causes of death for adults in the United States are related to lifestyle—tobacco use, poor diet, physical inactivity, and excessive alcohol consumption. 1 The enormous potential effects of health behavior change on mortality, morbidity, and health care costs provide ample motivation for the concept of lifestyle medicine (LM), that is, evidence-based practice of assisting individuals and families to adopt and sustain behaviors that can improve health and quality of life. Examples of target patient behaviors include, but are not limited to, eliminating tobacco use, improving diet quality, increasing physical activity, maintaining a healthy weight, addressing one’s mind-set and limiting alcohol consumption. 2
Effectively motivating patients to change behavior can be a frustrating and difficult challenge. Merely encouraging patients at the conclusion of an office visit to attempt such changes yields limited results. Success requires the development of specific healthy lifestyle action plans in partnership with patients and intentional follow-up in subsequent visits. For example, an intervention trial among sedentary adult patients (N = 255) demonstrated that when physicians provided structured counseling, followed by a health educator booster call, the total length of the weekly walking exercises increased by 5 times that of patients in the control group who received standard care. 3
Even though the most widely accepted, well-established chronic disease practice guidelines uniformly call for lifestyle change as the first line of therapy,4-12 physicians often do not follow these recommendations.13,14 For instance, obese patients are advised to lose weight only 36% of the time during regular examinations, a proportion that improves only slightly to 52% if a patient already has obesity-related comorbidities. 15 Physicians have cited inadequate confidence and lack of knowledge and skill as major barriers to counseling patients about lifestyle interventions. 16 Among the 620 respondents in a survey of family physicians, only 49% felt competent prescribing weight loss programs for obese patients. 17
To begin to address the gap in physicians’ knowledge and skills in LM, in 2009 a group of representatives from primary care medical specialties and other interested medical professional societies met and developed suggested LM competencies for primary care physicians. Those competencies were published in 2010. 18
The suggested competencies were developed largely to guide continuing medical education activities for primary care and preventive care physicians. However, many of these individual competencies have relevance for all specialties. Physician educators at both the undergraduate and graduate medical education levels are incorporating the relevant LM competencies into education and training programs. Each medical specialty is encouraged to review these competencies and adopt and adapt them as appropriate. This work has informed the development of curricula, training materials, evaluation, and system-based practice tools and performance measures to help physicians acquire the competencies and achieve practice goals. The American Board of Lifestyle Medicine (ABLM), established in 2015, is offering certification for primary care clinicians and professionals. The American College of Lifestyle Medicine (ACLM) offers the official Board Review Course. In conjunction with the American College of Preventive Medicine (ACPM), ACLM also offers the LM Core Competencies online course.
In spite of the tremendous progress in bringing LM competencies to primary care, a key piece of evidence-based LM continues to be underutilized, namely, intensive therapeutic lifestyle change (ITLC). 19 The vast majority of studies of LM in the reversal of chronic disease included an intensive induction phase of treatment.20-23 The induction phase both educates and demonstrates—patients not only learn what to do, but they also personally experience the power of lifestyle change to transform even advanced disease into vibrant health. An intensive induction phase potentiates motivational interviewing and lifestyle coaching, increasing the degree of change that can be achieved by inducing the patient to select bolder personal goals for change.
This important induction phase can be provided in a variety of ways, including residential and outpatient settings. Regardless of the setting, optimal treatment effectiveness requires specialized knowledge and skill in providing ITLC care. The more intensive the treatment the more dramatic the changes and the more closely medications and treatment must be managed. The specialized knowledge and skills required to effect disease reversal (ie, cessation of symptoms of chronic disease, reduction or elimination in medication) have not been defined or well described, though there is general agreement such expertise exists and is possessed by those who specialize in intensive LM treatment. This activity aimed to identify and describe the set of competencies that encompass the expertise required to provide effective, evidence-based intensive LM treatment (ITLC), and to organize them into the 6 Accreditation Council for Graduate Medical Education and American Board of Medical Specialties (ACGME/ABMS) categories. 24
These competencies aim to guide the education, clinical training, and board certification of an intensivist category of physicians who specialize in LM versus a generalist category of practice, via the ABLM. While a formal specialty of LM via the ABMS has not been established, leaders in LM are exploring options for advancing the LM field as a type of formal specialization based on the foundation created by the ABLM.
Methods
A small group of 3 LM experts, all diplomates of the ABLM, expanded the core competencies for primary care physicians 16 to include advanced expertise in LM.
The consensus group of 13 LM experts and stakeholders shared descriptions of expertise and competencies required and/or desired in the practice of intensive LM. The expanded competencies were revised to incorporate the expertise, knowledge and skills agreed upon by the consensus group.
The process included group emails and a telephone conference. The moderators sought to generalize and restate the key concepts in comments by the consensus group, subject to approval by the group members who made the comments. There were some differences in perspective and opinions, but with back-and-forth dialog these were resolved and incorporated into the competencies. Finally, the list of competencies was reorganized into the 6 ACGME/ABMS categories. The timeline for the discussion and consensus-building process spanned 3 months.
Results
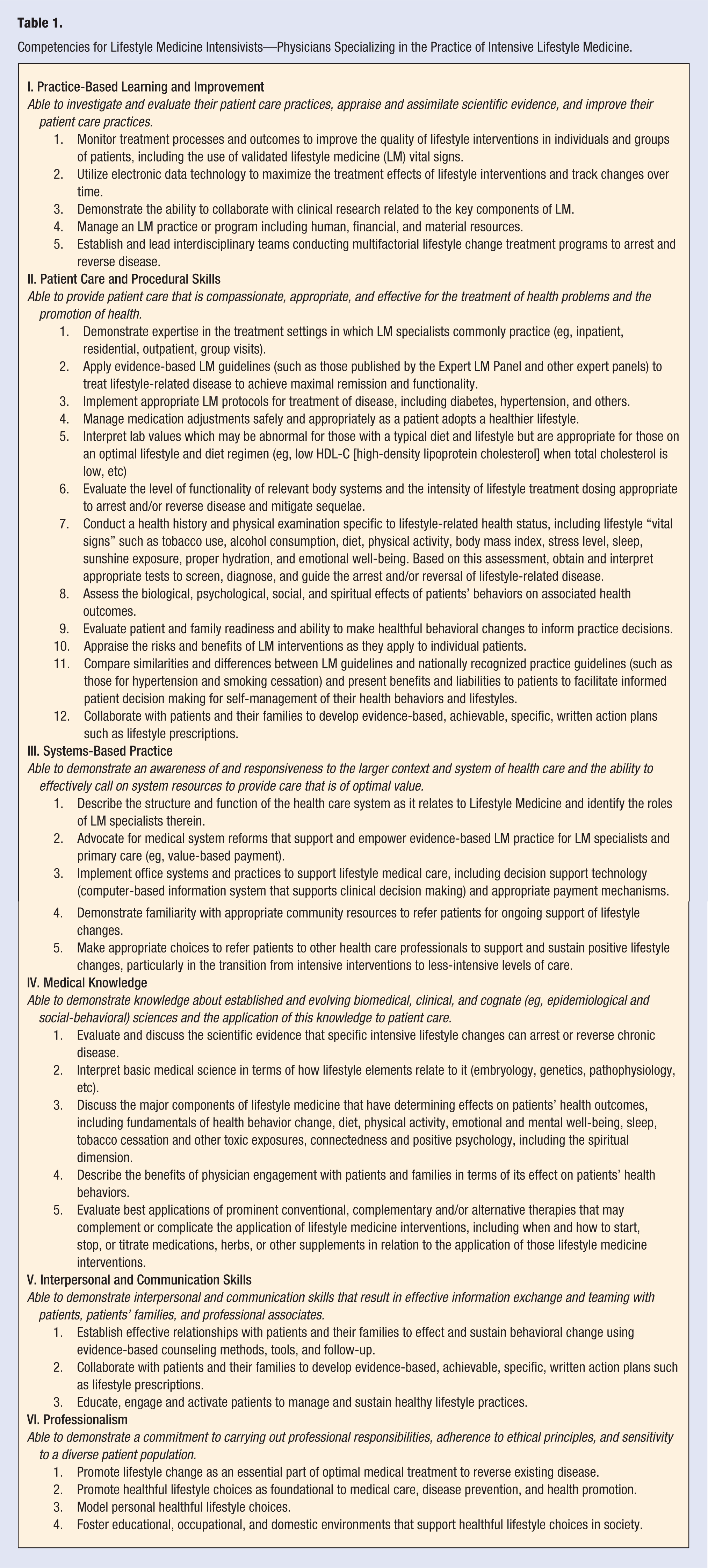
Consensus competencies are listed in Table 1 under the 6 ACGME/ABMS categories into which the competencies are organized. 21 All LM physicians who practice intensive lifestyle medicine should possess and demonstrate by their practice the General Physician Competencies at the expert level. 25 Lifestyle medicine intensivists should also possess the competencies listed in Table 1 in each of the 6 ACGME/ABMS categories.
Competencies for Lifestyle Medicine Intensivists—Physicians Specializing in the Practice of Intensive Lifestyle Medicine.
Discussion
The Expert LM Panel expects to build on this set of competencies for physicians who specialize in intensive LM in future expert practice guidelines. These competencies, adapted and expanded from the core competencies for primary care physicians, will provide a similar basis for developing the education, training and certification of physicians who specialize in the practice of intensive LM that the core competencies provided for primary care physicians. Whereas the core competencies were developed by a consensus group of primary care physicians and stakeholders, these LM intensivist competencies have been developed by a consensus group of LM experts and stakeholders, most of whom specialize in the practice of intensive LM. The group came to a unanimous consensus on the final set of competencies.
ACLM and ABLM anticipate incorporating this set of competencies into their activities and model for maximally effective, evidence-based treatment of chronic disease. It is hoped these competencies will be utilized to establish appropriate clinical fellowships to educate and train a cadre of physicians to specialize in intensive LM who can lead and expand the field of clinical LM treatment, education and research.
Footnotes
Acknowledgements
The authors and the Expert LM Panel want to thank the members of the consensus group for their time and expertise: Wayne Dysinger, MD, MPH; Caldwell Esselstyn, MD; Joel Fuhrman, MD; George Guthrie, MD, MPH; Zeno Charles-Marcel, MD; Michael Greger, MD; John McDougall, MD; Dean Ornish, MD; Jim Peters, MD, DrPH, RRT, RD; Brenda Rea, MD, DrPH, DPT, RD; James Rippe, MD; Mark Sandoval, MD; Scott Stoll, MD.
Author Contributions
Conception and design of the work: JK and MK; Group facilitation and moderating: JK and MK; drafting the article: JK, MK; critical revision of the article: LL; and final approval of the version to be published: all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by volunteers through the Expert Lifestyle Medicine Panel and the American College of Lifestyle Medicine.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.