
Abstract
Objective: The objective of this expert consensus process was to identify the competencies that lifestyle medicine (LM) Intensivists should be expected to have within their skill set. Methods: Expert panel members with experience in intensive, therapeutic lifestyle change (ITLC) updated and expanded a previously published set of competencies for this intensive LM practice, using an established process for developing consensus statements adapted for the topic. The previously published set of competencies was discussed for possible revision and expansion. Proposed changes were assessed for consensus using a modified Delphi process. Results: The expert panel revised the original list of 34 competencies, maintaining the 6 initial proposed topics that were previously published as Specialist Competencies: (1) Practice-Based Learning and Improvement, (2) Patient Care and Procedural Skills (3) Systems-Based Practice, (4) Medical Knowledge, (5) Interpersonal and Communication Skills, and (6) Professionalism. After a series of meetings and an iterative Delphi process of voting and revision, a final set of 46 competency statements for LM Intensivists achieved consensus. Conclusion: These competencies define the scope of practice and desired skill set for LM Intensivists. Further, these competencies establish a standard for certification of LM Intensivists.
Keywords
“In addition to medical knowledge and other foundational skills of medical practice, a core element of all LM intervention is supporting health behavior changes in patients.”
Introduction
The practice of lifestyle medicine (LM) continues to grow as the number of certified practitioners increases 1 and the implementation of LM within both private practices and health systems gains traction. 2 As the reach of LM broadens, there is a need to provide guidance to maintain a clear definition of the expected scope of knowledge and skill set for qualified LM practitioners.
The clinical competencies required for LM Intensivists (then-called “Specialists”) were first formulated and published in 2020 by an expert panel commissioned by the American College of Lifestyle Medicine (ACLM). 3 Just as the core competencies for primary care LM 4 served to formalize the practice of LM in primary care and promote its development and use, extended competencies for those who specialize in intensive therapeutic lifestyle change (ITLC) were needed. The recognition and use of ITLC since this first publication has grown. The American Board of Lifestyle Medicine (ABLM) offers an advanced LM certification for physicians who specialize in intensive treatment, now known as “Intensivists.” (https://ablm.org/eligibility-scheduling/).
In lifestyle medicine, the clinical goal is health with no evidence of disease. Remission is the return to a state of non-disease as determined by the failure to meet the recognized criteria for diagnosing the disease. Remission does not necessarily equate to a state of no evidence of disease. For example, a return to glucose levels in the range of “prediabetes” are consistent with various definitions5,6 of remission of type 2 diabetes, but are not adequate to meet criteria for no evidence of disease. Reversal is the process of disease treatment with the clinical goal of health with no evidence of the disease. LM Intensivists are best poised to support patients in achieving optimal health and remission of disease, by engaging in reversal in the context of ITLC treatment. The rise of ITLC combined with rapid growth in the evidence base for LM suggests a need to reassess and update the existing competencies for physicians using a more formal expert consensus process with input from an international panel of experts.
The evidence-based practice of LM includes both therapeutic lifestyle change (TLC) and ITLC methods of treatment. ITLC can be defined as an intensive, total-immersion approach to change providing maximum therapeutic dosing, while more gradual, incremental change is typically utilized with lower dose TLC interventions. 7 TLC interventions are appropriate and adequate for many lifestyle-related conditions, especially for early treatment when symptoms are milder and less acute. 7 However, the more intensive dosing 8 that is used in ITLC is needed as lifestyle-related conditions progress and more serious symptoms develop. As in certain specific contexts such as weight loss, 9 it is important that active ITLC interventions be followed by appropriate ongoing TLC treatment and monitoring to maintain adequate dosing of lifestyle interventions. In some cases, just as with addiction medicine where “refresher” treatment is sometimes needed to address relapse, a course of ITLC dosing may need to be repeated.
The objective of this consensus statement is to identify and describe the set of competencies that encompass the expertise required of physicians to provide effective, evidence-based intensive LM treatment (ITLC), and to organize them into the 6 Accreditation Council for Graduate Medical Education and American Board of Medical Specialties (ACGME/ABMS) categories. 10 The goal was to use the existing competencies as a starting point for a more formal, expert consensus process that would validate, update, and bolster the ITLC competencies to best serve development of standards for Intensivists.
Methods
This consensus update of the competencies was based on an a priori protocol (previously developed by AAO-HNSF 11 and also used by ACLM 5 to develop expert consensus statements), modified to streamline the process. In this project, the following steps were completed (1) define the scope of updating these competencies (2) recruit the expert panel, (3) vet potential conflicts of interest among proposed development group members, (4) perform a systematic literature search (5) discuss edits to the previous competencies statements to develop new competencies for voting, (6) develop and implement modified Delphi Method surveys, (7) revise the competencies based on survey results, and (8) assemble final statements for presentation.
Choice of Lifestyle Medicine Intensivist Competencies and Expert Panel Recruitment and Vetting
Competencies for LM Intensivists was proposed for a consensus statement by the Founding President of ACLM and approved by the ACLM Board of Directors. Expert panel membership was strategically developed to ensure appropriate representation of physicians from within the field of lifestyle medicine who have experience in delivering ITLC interventions, who come from a geographically diverse set of countries and continents, and who have unique perspectives on implementing ITLC interventions in a variety of practice settings. The ECS expert panel included representatives selected by the American College of Lifestyle Medicine (ACLM) and the American Board of Lifestyle Medicine (ABLM). Supplementary Table S1 presents a summary of panelist qualifications.
Once the expert panel was assembled, complete disclosure of potential conflicts of interest were reported and vetted. No direct conflicts of interest 12 existed for the chair or the majority of the participants. The project chair led the development of the consensus statements and the Delphi process with administrative support from an ACLM staff liaison, who also served as a non-clinician expert panel member.
Literature Review and Scope of the Consensus Statement
A literature review was performed in PubMed by ACLM staff, using keywords selected to identify current evidence on lifestyle medicine intervention and ITLC. The search was run through 9/28/21 and updated 9/6/22 and included publications in English. The following terms were used in the search: ((intens*[Title/Abstract] OR therapeutic[Title/Abstract]) AND (lifestyle[Title])) AND (change[Title/Abstract] OR program[Title/Abstract] OR intervention[Title/Abstract] OR treatment[Title/Abstract]) Filters applied: Case Reports, Clinical Trial, Guideline, Meta-Analysis, Observational Study, Practice Guideline, Randomized Controlled Trial, Systematic Review. (no reviews)
The primary target audience of this consensus statement was defined as physicians practicing lifestyle medicine, either already practicing ITLC interventions or interested in doing so. The secondary target audience was defined as the professional entities organizing and advancing the field of lifestyle medicine. The target population was defined as all patients of LM physicians. Search results were screened by the chair and used to inform the discussions and refinement of edits to the competencies.
Discussion and Competencies Editing for Delphi Voting
Once the target population and scope of practice were determined, the expert panel used the results of the literature reviews, combined with their expert opinion and stakeholder needs, to propose edits to updating the competencies in 6 topic areas, which were previously published as Specialist Competencies in 2020. 3
Each statement from the previously published document was discussed in meetings. Edits to improve and refine them were proposed for voting. As needed, competencies were edited, combined, deleted, or new statements were created. Competencies were developed or modified to follow best educational practices in developing learning objectives, using a strong action verb to begin each statement. A modified Delphi survey method 13 was implemented to assess consensus for the edited competencies, 11 with multiple surveys completed to address proposed edits that arose through further discussion. Prior to dissemination to the expert panel, the Delphi surveys were created by the chair, reviewed, and revised by ACLM staff liaison as needed with oversight from the chair. An online survey platform (www.QuestionPro.com) was used to administer the surveys to expert panel members.
Questions in the survey were answered with a 9-point Likert scale, with anchors of 1 = strongly disagree, 3 = disagree, 5 = neutral, 7 = agree, and 9 = strongly agree. The surveys were distributed, and responses were analyzed and presented in the next expert panel meeting. Statements or edits that achieved near consensus were discussed further and revised for re-voting.
The final draft of the expanded competencies was reviewed for completeness by the expert panel, with further editing by the chair and 1 panel member. These additional, final edits to the competencies were approved with 2 last rounds of Delphi voting. The expanded competencies were then reviewed and approved by the ACLM and ABLM Board of Directors.
Criteria for Consensus Were Established a Priori as Follows
• • •
Each survey focused on 1 or more topic areas. All expert panelists present completed the survey items, and absentee panelists were encouraged to review the minutes and recorded meetings and complete the survey. The competency statements that did not meet consensus were discussed to determine if wording or specific language was pivotal in the item not reaching consensus. Each topic area was addressed with 1-3 Delphi rounds. The factors leading to the remaining items not reaching consensus were not attributed to wording or other modifiable factors, but rather a genuine lack of consensus. However, the group discussions allowed ample opportunity to engage in the iterative nature of the voting process and propose revisions for revote. For methodological transparency, results from each specific round of voting with mean agreement and number of outliers are presented in Supplementary Tables S2-S8.
The final manuscript was drafted with participation and final review from each panelist, and reviewed and approved by ACLM and ABLM.
Results
Practice-Based Learning and Improvement.
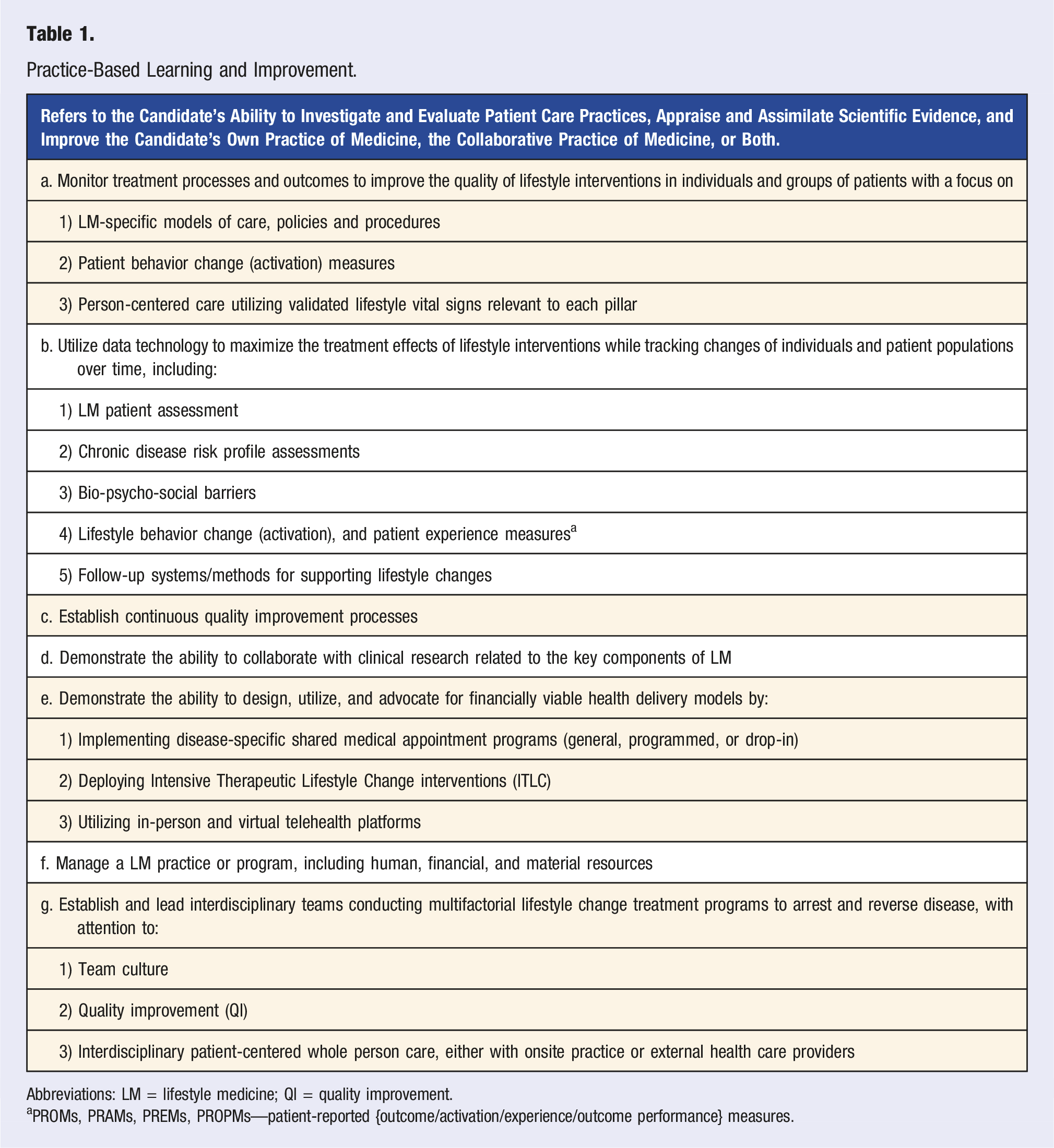
Abbreviations: LM = lifestyle medicine; QI = quality improvement.
aPROMs, PRAMs, PREMs, PROPMs—patient-reported {outcome/activation/experience/outcome performance} measures.
Patient Care and Procedural Skills.
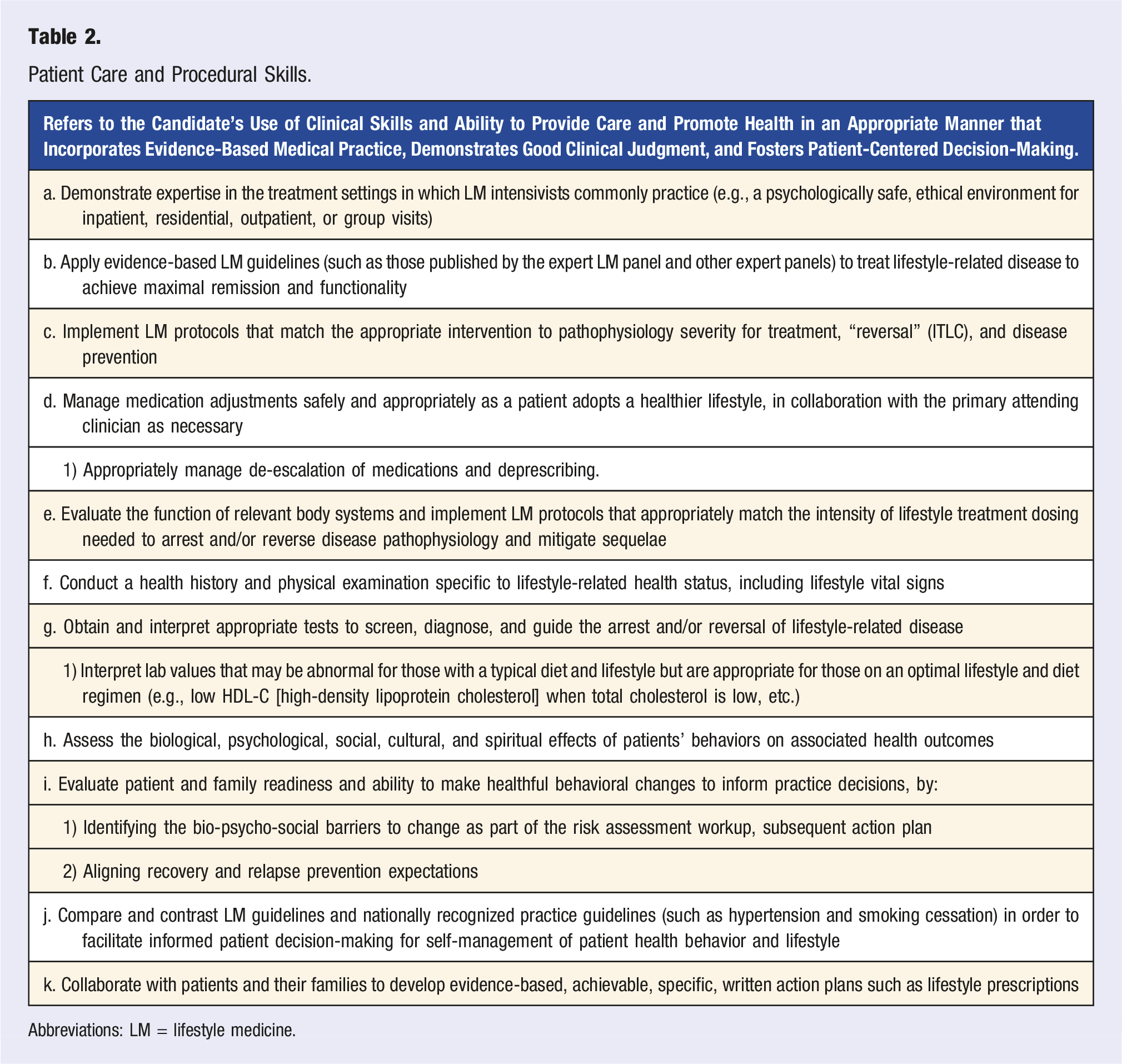
Abbreviations: LM = lifestyle medicine.
Systems-Based Practice.
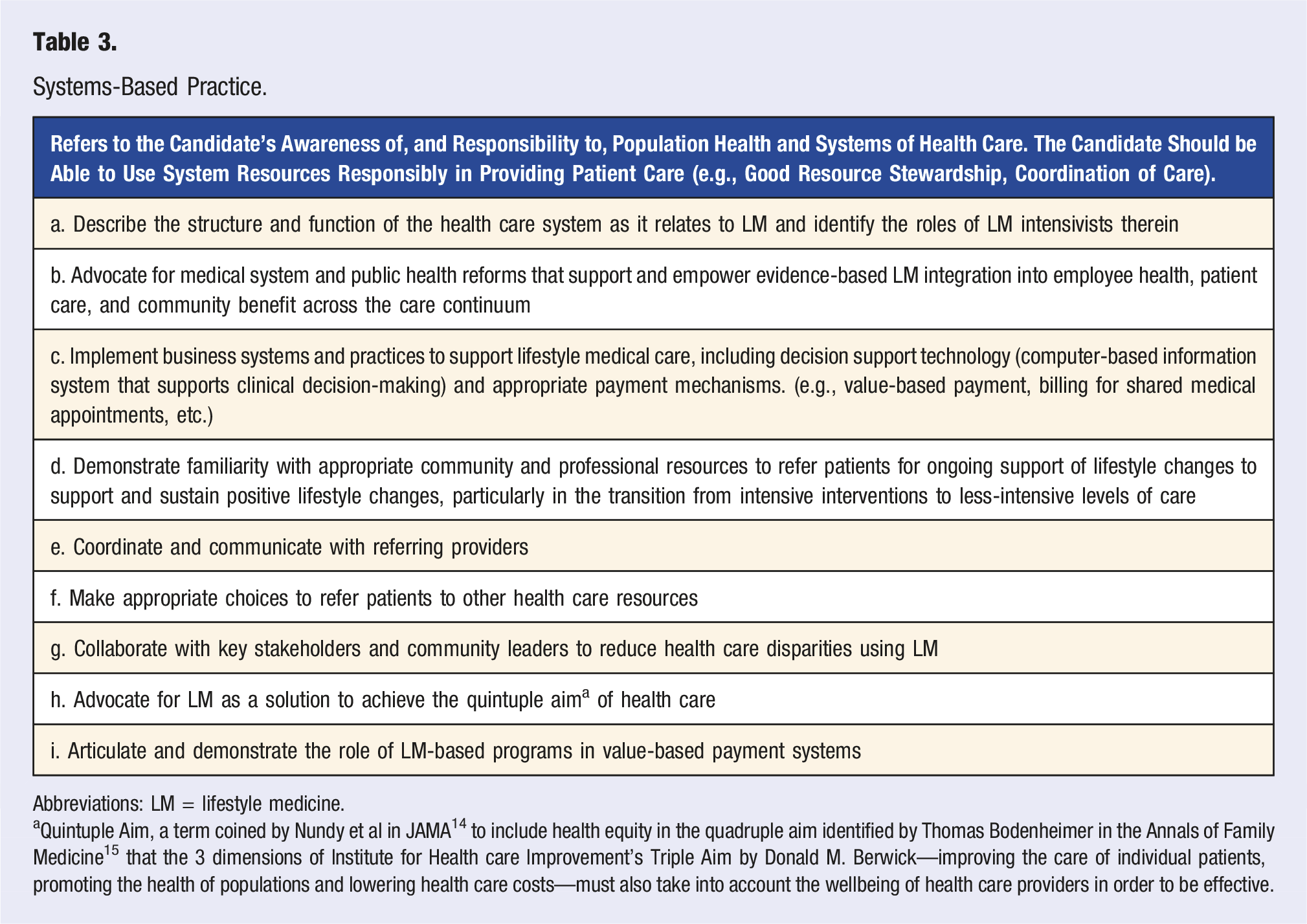
Abbreviations: LM = lifestyle medicine.
aQuintuple Aim, a term coined by Nundy et al in JAMA 14 to include health equity in the quadruple aim identified by Thomas Bodenheimer in the Annals of Family Medicine 15 that the 3 dimensions of Institute for Health care Improvement’s Triple Aim by Donald M. Berwick—improving the care of individual patients, promoting the health of populations and lowering health care costs—must also take into account the wellbeing of health care providers in order to be effective.
Medical Knowledge.
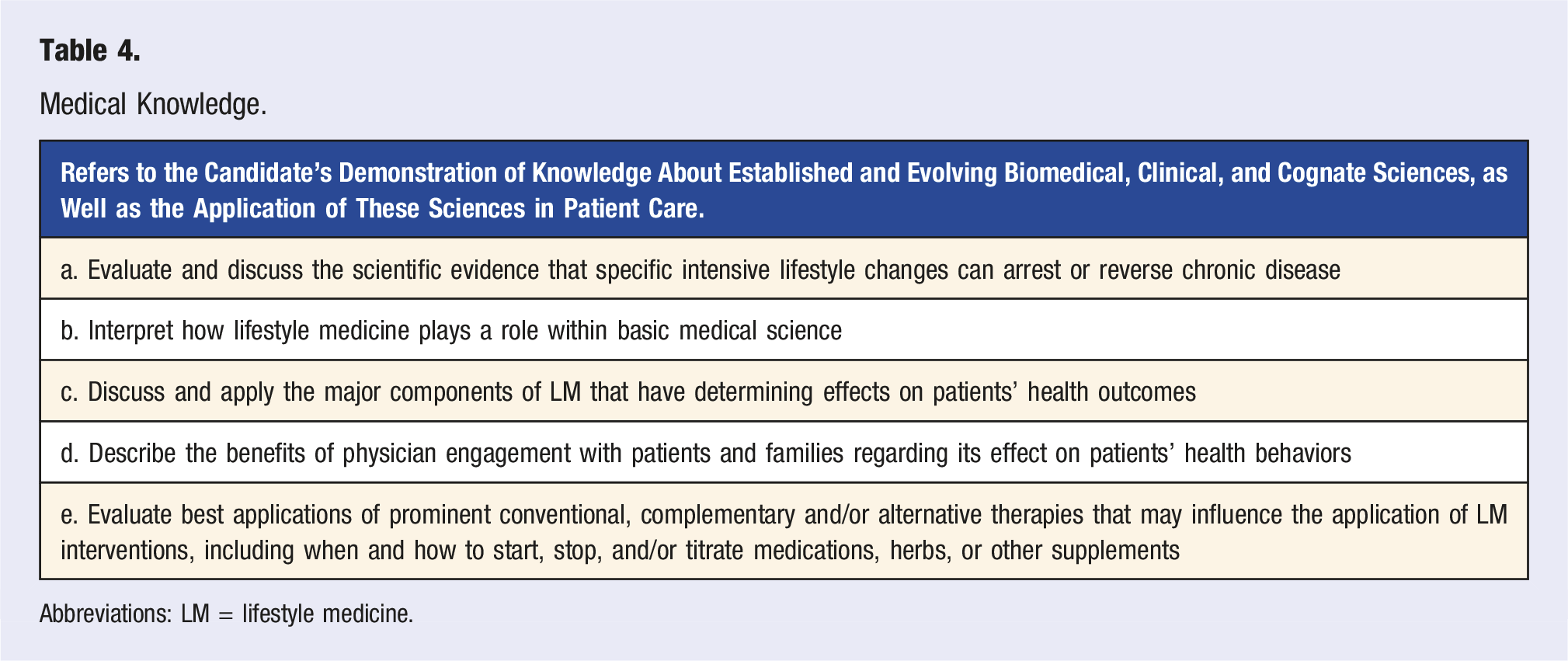
Abbreviations: LM = lifestyle medicine.
Interpersonal and Communication Skills.
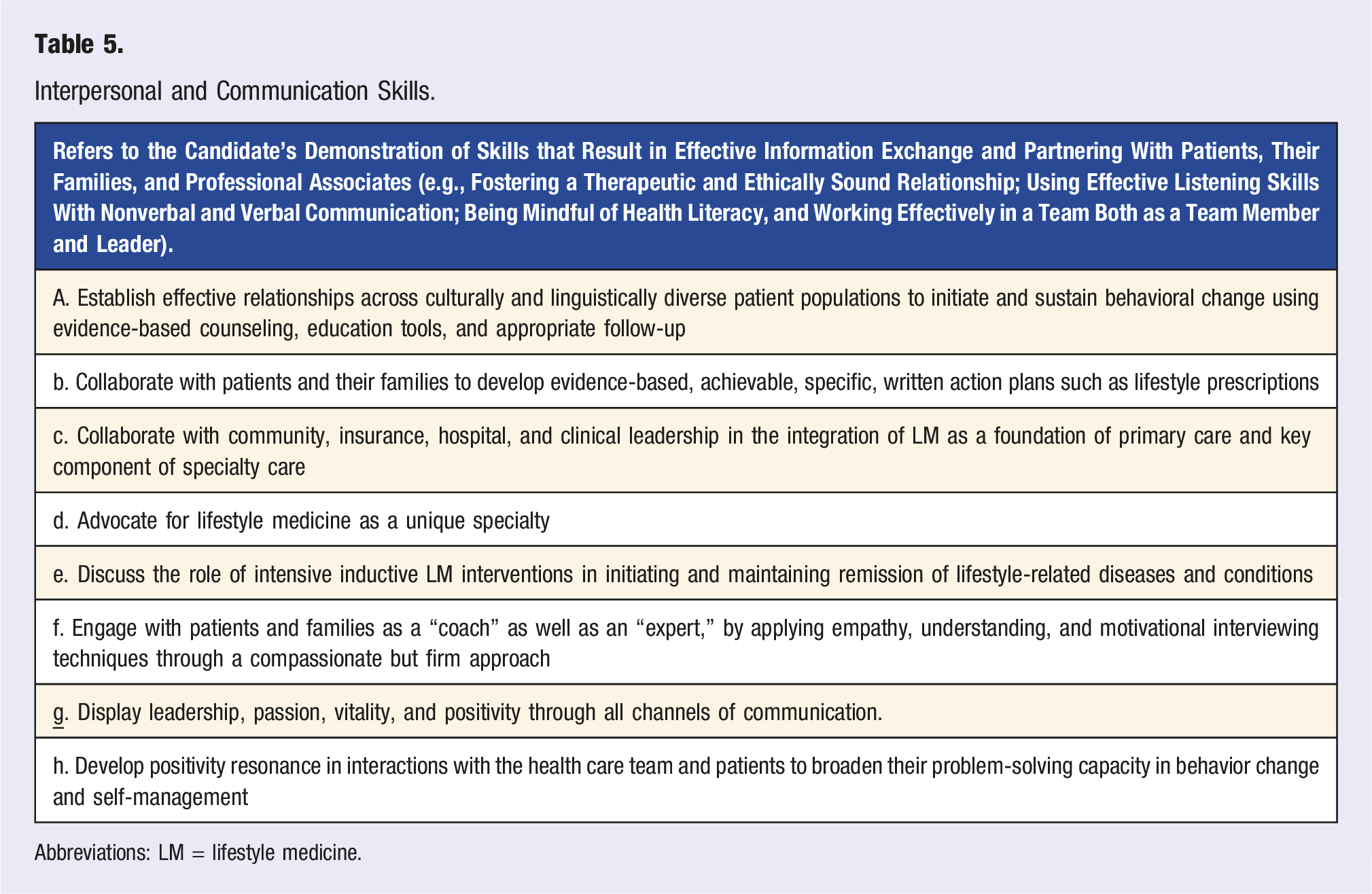
Abbreviations: LM = lifestyle medicine.
Professionalism.
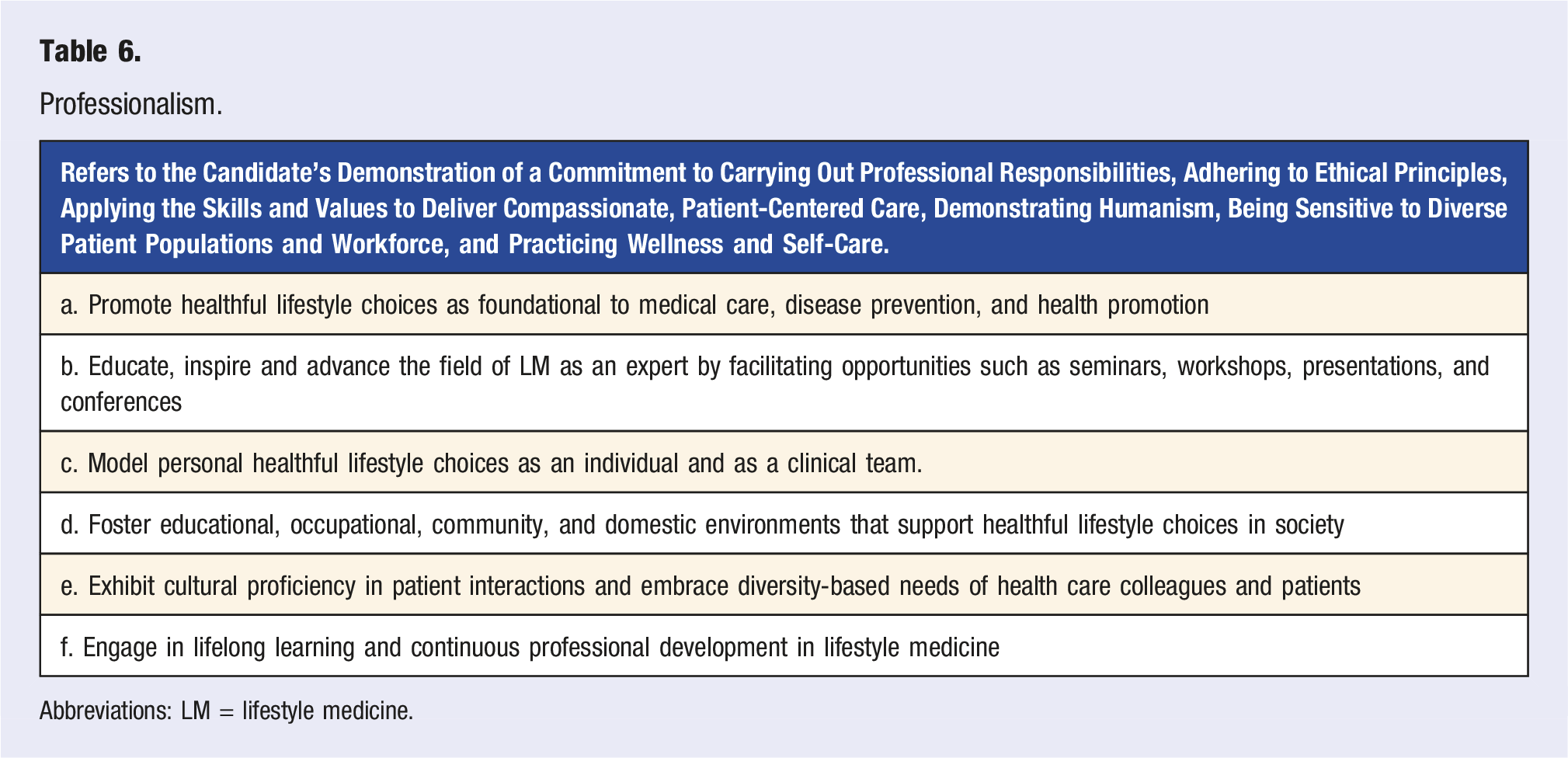
Abbreviations: LM = lifestyle medicine.
Discussion
We successfully used an expert consensus process to build upon, and validate, guidance for physicians seeking to develop expertise in the core ITLC competencies. Having achieved consensus on all recommendations with a diverse expert panel adds credence to the depth and validity of the competencies, beyond the original work in this field published in 2020 to first define competencies for then-called “Specialists.” 3
Therapeutic lifestyle change outcomes are considered “intensive” when large changes are made that dramatically improve biometric measures of health and disease. Therapeutic lifestyle change interventions are considered “intensive” when increased frequency and/or duration of patient encounters can be used to help patients make substantial changes rapidly with the intent of dramatically improving biometric measures of health and disease. 7 This type of LM treatment requires close supervision and oversight by a qualified LM physician, ideally a physician certified in LM and also appropriately trained to deprescribe medications as needed. 7 Intensive Cardiac Rehab (ICR) LM programs, for example, are “intensive” therapeutic lifestyle change interventions, which produce dramatic improvement in multiple biometric measures of health and disease status, as well as supervision and oversight by a qualified physician.
In addition to medical knowledge and other foundational skills of medical practice, a core element of all LM intervention is supporting health behavior changes in patients. Effectively motivating patients to change behavior poses significant challenges for health care practitioners. 16 Merely encouraging patients at the conclusion of a brief office visit to attempt such changes yields limited results. 17 Examples of successful dietary interventions are high-intensity, with multiple follow-up visits and points of contact. 17 A systematic review of 9 studies, with participant groups ranging from N = 38 to N = 1065, on behavioral strategies used to increase adherence to lifestyle interventions among adults with obesity found that the inclusion of behavioral strategies supported more physical activity and better attendance in sessions, highlighting the relationship between provider-patient contact and the ability to support optimal adherence to treatment. 18
These competencies define the expected scope of skill for LM Intensivists, the physicians focused on delivering such ITLC treatment. They were organized around the 6 competency categories defined by ABMS and ACGME. This facilitates their use in developing medical education and training programs, including fellowships for LM Intensivists who can specialize in providing the most intensively-dosed therapeutic lifestyle interventions. Such interventions are typically needed for the more acute and/or severe cases of chronic disease, necessitating a higher level of expertise and clinical knowledge and skill than is typically available in the primary care setting. Ideally, these intensive LM interventions are requested and followed up after referral by primary care clinicians who desire to optimize LM dosing for maximal treatment effect.
These competencies will set a consistent standard for certification, allowing LM Intensivists to demonstrate mastery of the skills, ability, and knowledge to practice ITLC effectively. Preparation for certification will be supported by clinical training residencies and/or fellowships that are able to embrace these competencies in their curricula and track patient outcomes to demonstrate clinical expertise. Certification of LM Intensivists is intended to include a demonstration of mastery of these competencies, ideally by written exam and evidence of appropriate clinical outcomes.
Strengths and Limitations
These competencies have a number of strengths. They were developed using a systematic consensus process that produced robust discussion and solid consensus. The panel included LM experts from multiple continents with a wide scope of expertise and clinical experience in ITLC. They built upon the previous competencies for LM Specialists published in 2020. 3 They were also able to benefit from the updated competencies for primary care LM published in 2022. 4
There were limitations in developing this set of intensivist competencies. The number of practicing LM Intensivists and relevant experts is relatively small, in large part because LM is a nascent medical discipline with limited reimbursement by third-party payers. This tended to limit the number of experts available to serve on the panel. However, this was ameliorated to some extent by including international panelists, and the panel was of sufficient size to have diversity of opinion, with 12 experts serving on it.
Conclusions
These competencies will serve to guide the practice, education, clinical training and ideally certification of an intensivist category of physicians who specialize in LM vs the more generalist category of primary care LM practice.
CME/CE Article Quiz
American College of Lifestyle Medicine (ACLM) members can earn FREE CME/CE credit by reading this approved CME/CE article and successfully completing the online CME/CE activity. Non-members can earn CME/CE for $40 per article. Visit lifestylemedicine.org to join the ACLM.
AJLM CME/CE Articles and Quizzes are offered online only through the American College of Lifestyle Medicine and are accessible at lifestylemedicine.org/store. ACLM Members can enroll in the activity, complete the quiz, and earn this CME/CE for free. Non-members will be charged $40 per article.
A Passing score of 80% or higher is required in order to be awarded the CME/CE credit.
Supplemental Material
Supplemental Material - Lifestyle Medicine Intensivist Competencies: 2023 Expert Consensus Update
Supplemental Material for Lifestyle Medicine Intensivist Competencies: 2022 Expert Consensus Update by John H. Kelly, MD, MPH, FACLM, DipABLM, Liana Lianov, MD, MPH, FACLM, FACPM, DipABLM, Dexter Shurney, MD, MBA, MPH, FACLM, DipABLM, Sley Tanigawa Guimarães, MD, DipIBLM, Mechelle Palma, MD, MMHA, DipIBLM, FACLM6, Caldwell Esselstyn, MD, FACLM, Scott Stoll, MD, FABPMR, Padmaja Patel, MD, FACLM, DipABLM, Brenda Rea, MD, DrPH, PT, RD, FACLM, Koushik Reddy, MD, FACC, FACLM, DipABLM, George Guthrie, MD, MPH, CDE, CNS, FAAFP, FACLM, Michelle Reiss, MBChB, LMCC, CCFP, FRACGP, FASLM, and Micaela C. Karlsen, PhD, MSPH in American Journal of Lifestyle Medicine
Supplemental Material
Supplemental Material - Lifestyle Medicine Intensivist Competencies: 2023 Expert Consensus Update
Supplemental Material for Lifestyle Medicine Intensivist Competencies: 2022 Expert Consensus Update by John H. Kelly, MD, MPH, FACLM, DipABLM, Liana Lianov, MD, MPH, FACLM, FACPM, DipABLM, Dexter Shurney, MD, MBA, MPH, FACLM, DipABLM, Sley Tanigawa Guimarães, MD, DipIBLM, Mechelle Palma, MD, MMHA, DipIBLM, FACLM6, Caldwell Esselstyn, MD, FACLM, Scott Stoll, MD, FABPMR, Padmaja Patel, MD, FACLM, DipABLM, Brenda Rea, MD, DrPH, PT, RD, FACLM, Koushik Reddy, MD, FACC, FACLM, DipABLM, George Guthrie, MD, MPH, CDE, CNS, FAAFP, FACLM, Michelle Reiss, MBChB, LMCC, CCFP, FRACGP, FASLM, and Micaela C. Karlsen, PhD, MSPH in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
The authors wish to thank the leadership of the American College of Lifestyle Medicine and the American Board of Lifestyle Medicine.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: John H. Kelly: Receives consulting payments from the American College of Lifestyle Medicine Brenda Rea: Program Director of the Lifestyle Medicine Intensivist Fellowship at Loma Linda University Health; Board Member, American Board of Lifestyle Medicine; Co-Chair of Education Committee, American College of Lifestyle Medicine. Micaela C. Karlsen: Employed by the American College of Lifestyle Medicine.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the American College of Lifestyle Medicine.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.