
Abstract
In response to Covid-19, the Lifestyle Medicine Clinic at Midland Health elected to utilize telehealth to engage remotely with patients to deliver a 12-week intensive therapeutic lifestyle change (ITLC) program for patients with type 2 diabetes and prediabetes. This program utilized a shared medical appointment (SMA) group visit model. Beginning in May/2020, the program was offered again in-person; however, the telehealth option remained. This study is a retrospective chart review, aimed at comparing pre- and post-program changes in body weight, HbA1c, fasting lipid profile, systolic pressure, and diastolic blood pressure between in-person vs telehealth SMA formats. This study found no statistical difference in ITLC program health outcomes between telehealth vs in-person shared medical groups. At the end of ITLC Programs between both groups, an average weight loss of 9.66 pounds and 1% reduction was noted in ptHbA1C. Total cholesterol reduced by 7.1 mg/dL, and LDL by 15.19 mg/dL. The blood pressure readings showed a reduction in systolic blood pressure of 13.4 mmHg and diastolic blood pressure of 4.14 mmHg. Our results indicated that this novel telehealth delivery model could be equally successful in delivering an intensive therapeutic lifestyle program (ITLC) using an SMA approach to prevent, treat and often put chronic diseases in remission.
Keywords
“The program heavily relied on the science of behavior change, proving that technology is not a barrier if patients can be motivated to make the change.”
Introduction
As COVID-19 developed into a global crisis, restrictions on the management of healthcare became an overarching concern and challenge. As “shelter in place” developed into a norm across the nation, innovative approaches for managing chronic illness were needed. Telehealth emerged as a popular alternative. Accordingly, in 2021, the U.S. Department of Health and Human Services stipulated a modification of the enforcement related to the Health Insurance Portability and Accountability Act of 1996 (HIPPA) that allowed providers to engage with patients via remote techniques without any concern of imposed HIPAA penalties. 1 According to a report from the US Department of Health and Human Services (HHS), telehealth visits for Medicare beneficiaries had increased 63-fold in 2020. 2 Herzer and Pronovost 3 offer 3 guiding principles for telemedicine implementation arguing that virtual care should achieve safety and effectiveness comparable to traditional care, improve efficiency without increasing costs, and respect patient preferences and values without exacerbating healthcare disparities.
The Lifestyle Medicine Clinic at Midland Health was one of the many programs that pivoted to telemedicine format in March 2020. In February 2020, Midland Health developed an innovative 12-week intensive therapeutic lifestyle change (ITLC) program for patients with type 2 diabetes (T2D) and prediabetes. This program was intended to be delivered in-person but was shifted to telemedicine due to Covid-19. Programs targeting diabetes management are essential, as T2D is acknowledged as a critical public health issue that directly impacts not only health outcomes but also health management and expenditures. 2 According to Gutierrez-Cruz, 4 healthcare expenditures for the treatment of diabetes within the U.S reflected 380 billion U.S. dollars, while the prevalence among American adults (20-79 age group) was almost 14%. In addition, Kelly and associates 5 noted that the cost within the U.S. resulted in a decrease in productivity of approximately $90 billion (about $280 per person in the US). Lifestyle change is an effective approach for both treatment and remission of T2D and can produce meaningful clinical improvements among patients. 5 A recent expert consensus statement from the American College of Lifestyle Medicine (ACLM) further identifies lifestyle, specifically diet, as a primary intervention for achieving T2D remission. 6
Midland Health’s ITLC program for patients with diabetes utilizes a shared medical appointment (SMA) group visit model. Shared medical appointments (SMAs) are one way to initiate lifestyle-based changes in T2D patients. The successful use of SMAs in improving clinical outcomes for T2D has been documented, the majority of which included lifestyle-based nutrition and/or physical activity components. 7 Research has shown that benefits of group visits include greater patient and physician satisfaction, improved behaviors, increased self-efficacy, and improved quality of life. Group settings create a collaborative relationship in which practitioners help patients build confidence, set goals, and remain accountable. 8 For certain conditions such as those treated through mental health counseling, virtual care could be as effective as in-person visits, 9 although there is insufficient data to support this finding for other conditions. Zulman and Verghese further note how virtual care has led to “the unexpected consequence of offering clinicians humbling insights into patients ‘lives’” with respect to factors that inevitably influence health, including living conditions, food security, and available food security support systems. 9
Thus, while the use of lifestyle medicine for treatment and remission of diabetes is well-established and the effectiveness of SMAs has been demonstrated, the efficacy of SMAs delivered via telehealth vs traditional in-person format has not been examined. This study is a retrospective chart review aimed at comparing pre- and post-program changes in body weight, HbA1c, fasting lipid profile, systolic pressure, and diastolic blood pressure between in-person vs telehealth SMA formats.
Methods
ITLC Program Description
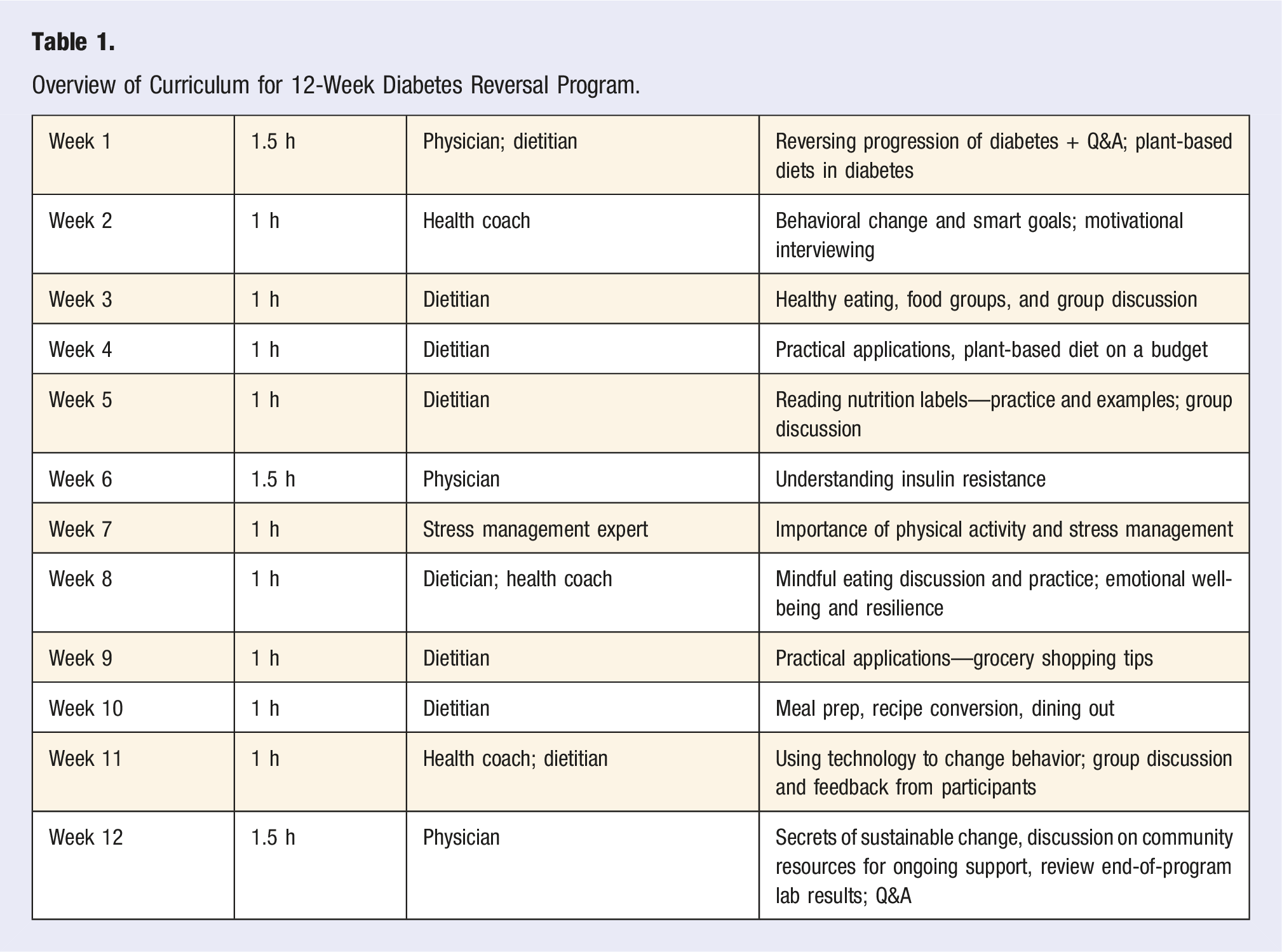
Midland Health’s ITLC is a 12-week program, delivered by a physician, dietitian, and health coach, focusing on teaching lifestyle change in the context of the 6 pillars of lifestyle medicine—plant-predominant diet, exercise, stress management, social connectedness, restorative sleep, and avoidance of risky substances—to promote, treat and potential remission of prediabetes and T2D. The program provided weekly interactions addressing a wide variety of appropriate educational topics. Routine health information, including measurements of HgbA1C, body weight, blood pressure (systolic and diastolic), and fasting lipid profile were obtained before program participation began. This same health information was obtained again at the end of the program. A total of 51 patient were enrolled of which 46 had complete data within the patients enrolled in 9 different cohorts, 4 virtual (4 groups #2n = 4, #4n = 6,#6n = 5, #8n = 4) and 5 in-person (5 groups #1n = 4, #3n = 5 #5n = 5, #7n = 5, #9n = 8), were delivered over 9 months.
Overview of Curriculum for 12-Week Diabetes Reversal Program.
Retrospective Chart Review
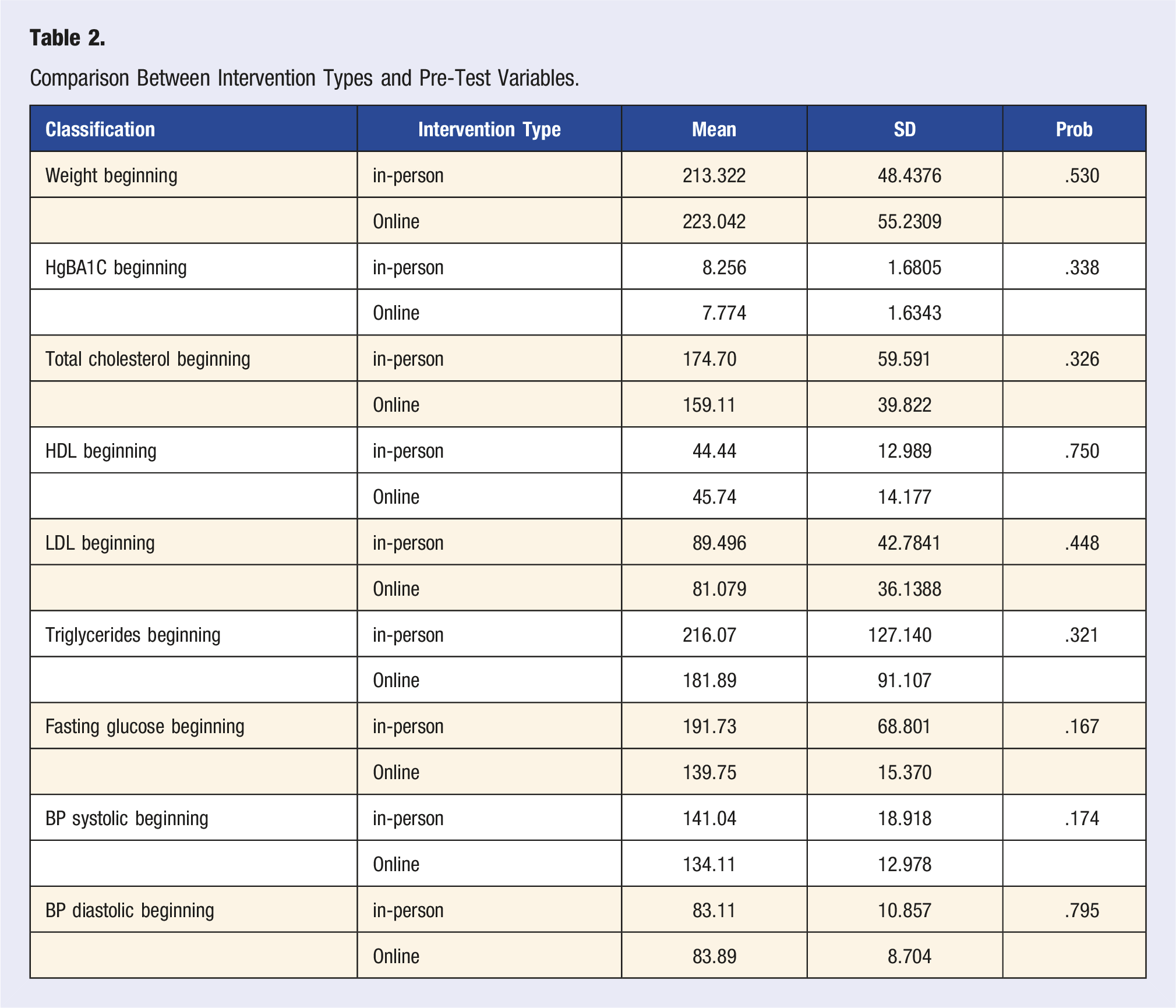
Medical records were reviewed for n = 46 ITLC program participants, n = 19 participants for the virtual group and n = 27 for the in-person group. This study utilized convenient sampling since it was a retrospective chart review of those individuals receiving lifestyle medicine based therapeutic interventions during the COVID-19 pandemic. Each participant was offered a choice to participate in in-person or telehealth groups based on personal preferences. Personal preferences were valued within the learning process to facilitate the effective acquisition of the content related to the disease process. All the data was reported in the aggregate.
Comparison Between Intervention Types and Pre-Test Variables.
Results
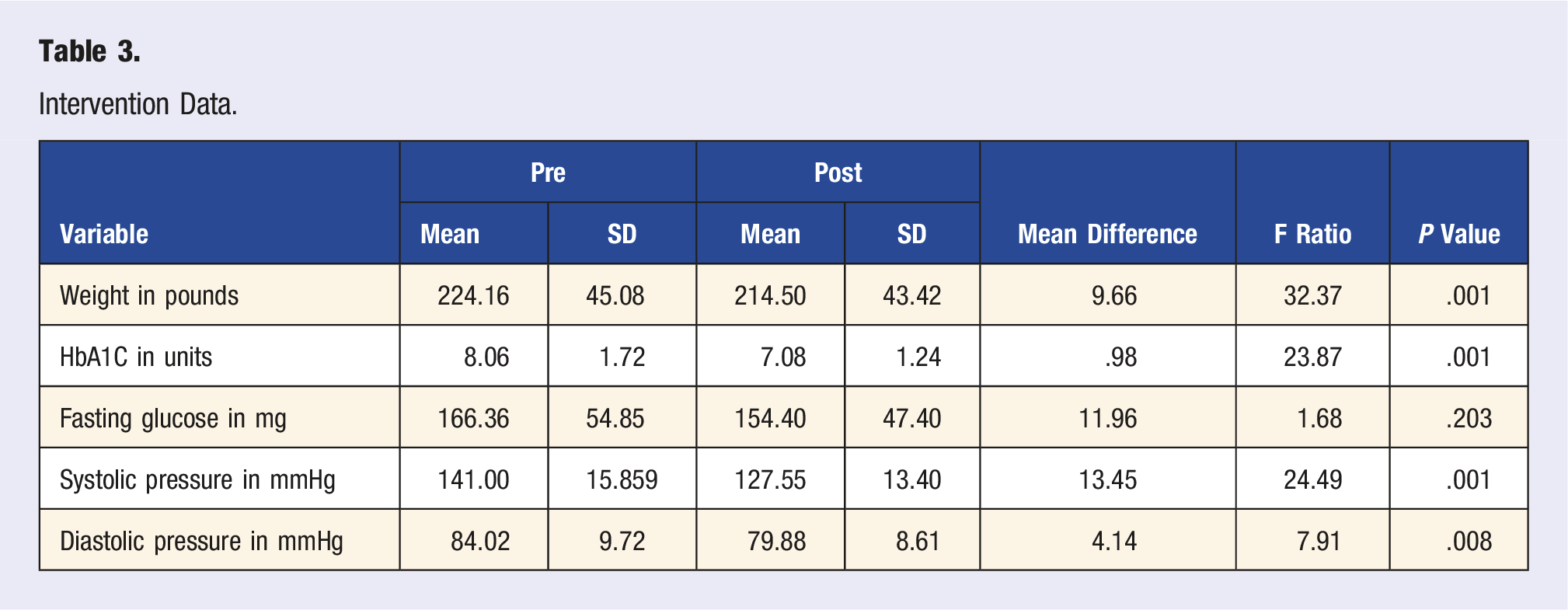
Intervention Data.
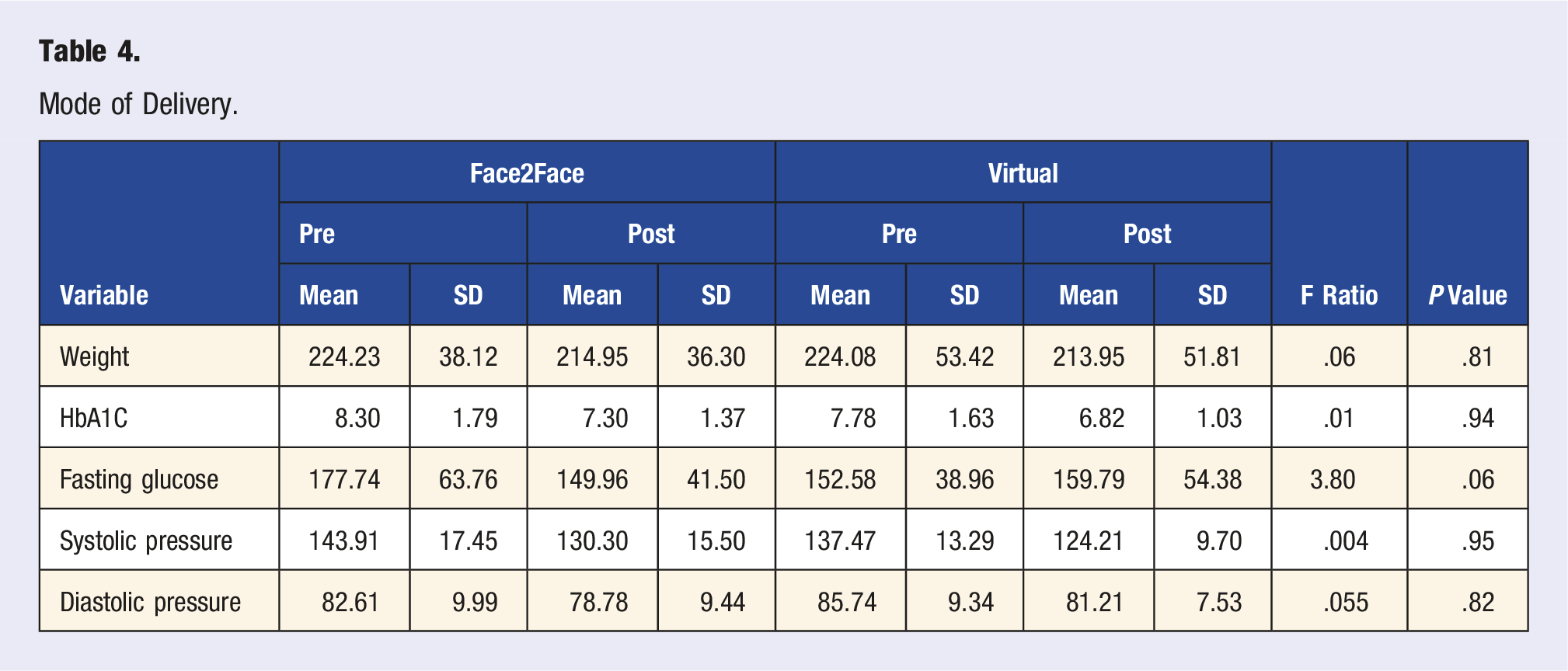
Mode of Delivery
Mode of Delivery.
Sex
Sex Differences.

These numbers reflect the overall results independent of the delivery method. At the end of 12 weeks of the intensive therapeutic program between both groups, the change in HbA1C reflected an average drop of 1.00 (8.06 reduced to 7.06) while the fasting glucose demonstrated an average drop of 11.96 (166.36 reducing to 154.40). The change within the means for the lipids were: total cholesterol 7.1 (89.24 reduced to 82.14), HDL increased by 2.41 (71.93 changed to 94.34), LDL decreased by 15.19 (154.55 reduced to 139.36), and triglycerides increased by 15.79 (241.21 changed to 257.00). The blood pressure readings reflected: systolic reflected a 13.45-point decrease (141.00 down to 127.55) while the diastolic decreased 4.14 points (84.02 down to 79.88). The drop in weight was 9.66 pounds (224.16 down to 214.50).
Discussion
The pandemic forced the medical community to offer innovative care delivery models for chronic disease management. Our efforts to convert in-person ITLC to telehealth SMAs were one of those creative attempts. The virtual programs also offer convenience and flexibility to both providers and patients. We had never offered this program over a virtual platform and hence its efficacy in delivering expected health outcomes remains to be seen. A comprehensive solution offering a therapeutic dose of lifestyle medicine for a group of patients with T2D, and prediabetes successfully showed improvement in weight loss, blood pressure readings and improvement in HbA1c and lipid profile. No statistical difference in ITLC program health outcomes between telehealth vs in-person shared medical groups was found.
These findings demonstrate that well-designed comprehensive solutions can be effective for patients with T2D and prediabetes in both in-person and telehealth delivery models. These shared medical appointments were billed as individual office visits using E/M codes and billed to respective insurances; participants did not have to pay any additional cost apart from their co-pays and deductibles for office visits. The program heavily relied on the science of behavior change, proving that technology is not a barrier if patients can be motivated to make the change. These encouraging positive results are consistent with 2 evidence reviews on telehealth published by the AHRQ.9,11 Telehealth offered a safe care delivery model during the pandemic. The findings of this study suggest that telehealth can be an effective tool in delivering comprehensive, high-value care using multidisciplinary teams to address the lifestyle behaviors of patients with chronic diseases. This novel approach is not only to manage these conditions but to achieve remission or reversal of chronic diseases. In the post-pandemic era, where there is a significant shortage of healthcare workforce, higher rates of provider burnout, telehealth may offer a viable alternative.
A cohort study of 40.7 million US commercially insured adults found that the use of telehealth services to manage chronic conditions was comparable or even more efficient than in-person care when follow-up encounters were assessed. 12 This important finding defines the future of telehealth in chronic disease management. In addition to delivering similar health outcomes, telehealth has the potential to improve the quality of care in rural areas by increasing access to specialists and reducing costs. It can also contribute to healthcare system readiness and improve the ability to provide continued care during emergencies. However, quality measurement related to telehealth and system readiness is limited. To address these limitations, the National Quality Forum (NQF) convened a multi-stakeholder Rural Telehealth and Healthcare System Readiness Committee to develop a framework for quality measurement assessing the impact of telehealth on healthcare system readiness and health outcomes during emergencies in rural areas. 6 In addition, broadband access to rural areas will need to be addressed to ensure equitable access to telehealth services for all patients.
The limitation of this study is the smaller sample size. Although the study indicates that this novel telehealth ITLC delivery model could be successful in delivering a lifestyle medicine approach to treat and often reverse chronic disease burden, additional large-scale studies will need to be conducted to confirm these findings.
Conclusion
This small study with its limitations due to sample size, found no statistical difference in ITLC program health outcomes between telehealth vs in-person shared medical appointment groups. Comparing these two groups for their improvement in measurements of HbA1C, fasting lipid profile, weight loss, and blood pressure, there was no statistical difference between them.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.