
Abstract
Objective: To assess physician attitudes on the status, value, and future of board certification in lifestyle medicine (LM). Study design: Cross-sectional survey of physician members of the American College of LM. Methods: A 49-item, web-based survey with a 5-point Likert response scale. Results: The 351 respondents did not differ significantly from the eligible sample of 6334 members regarding gender (68% female), country of residence (88% U.S), or census region, but did include more ABLM diplomates (63% vs 22%). Certification by ABLM was considered a source of personal pride (95% agree or strongly agree) that could help in marketing clinical services (85%) and potentially increase job opportunities (60%). Certification by ABLM is sufficient for certification needs (67%), but there was interest (65%) in LM becoming a member board of the American Board of Medical Specialties (ABMS) as an aspirational goal (48%). Few respondents (22%) practiced intensive therapeutic lifestyle change (ITLC) even though most (57%) considered it an essential aspect of LM. There was agreement (94%) that LM is essential to mainstream medicine. Conclusion: Survey respondents, regardless of certification status, agreed that becoming an ABLM diplomate both meets their certifying needs and offers substantial benefits, with the caveat that ABMS recognition is an aspirational goal.
Keywords
Introduction
“The ACLM and ABLM, despite their relatively recent appearance in medicine, are well-positioned to support the rapid and ongoing growth of LM by meeting the needs of members, clinicians, the public, educators, health systems, and other stakeholders.”
Growth of Interest in Lifestyle Medicine Using Diverse Metrics.
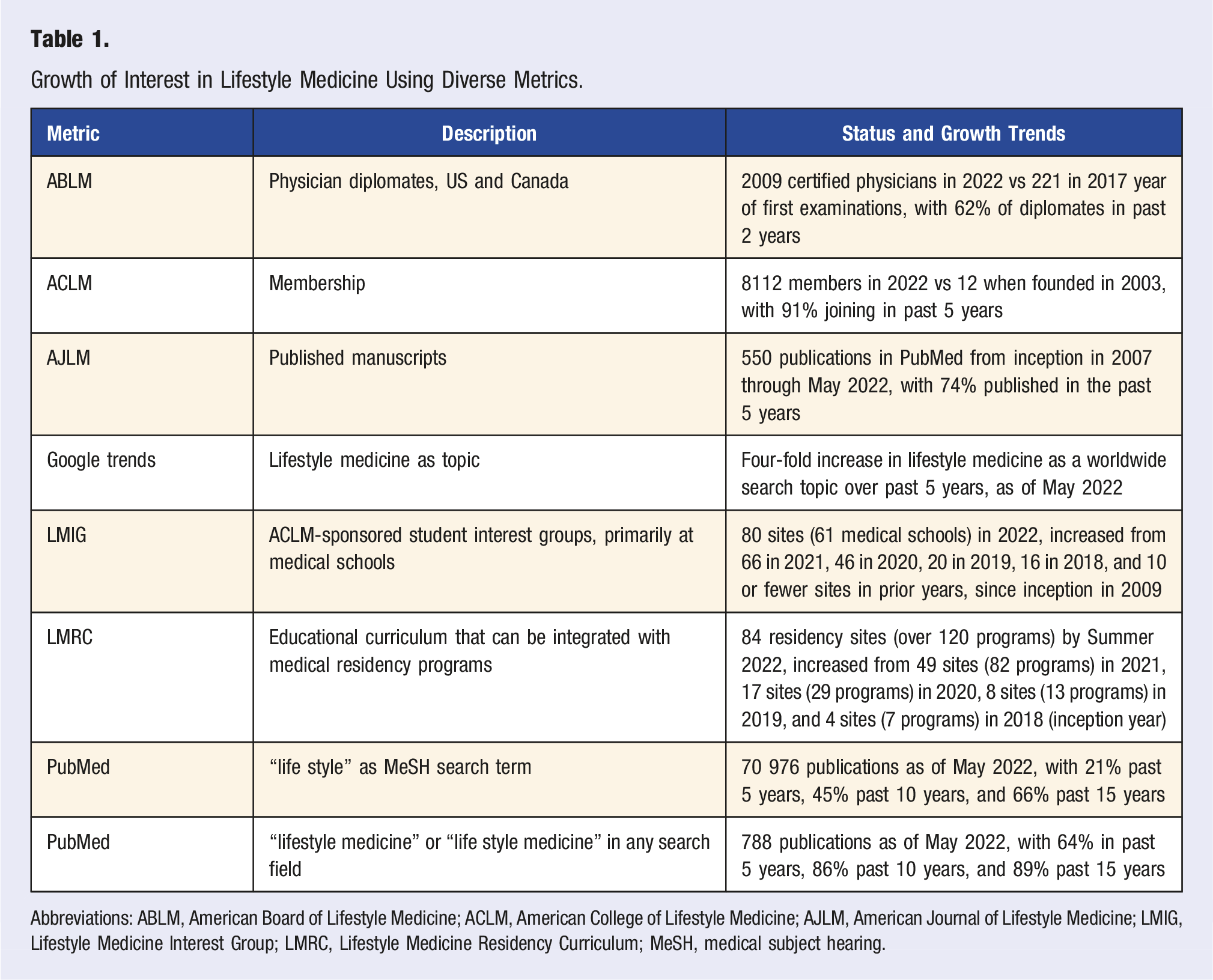
Abbreviations: ABLM, American Board of Lifestyle Medicine; ACLM, American College of Lifestyle Medicine; AJLM, American Journal of Lifestyle Medicine; LMIG, Lifestyle Medicine Interest Group; LMRC, Lifestyle Medicine Residency Curriculum; MeSH, medical subject hearing.
Certification of physicians in the U.S. began in 1917 with the American Board of Ophthalmology, leading to the American Board of Medical Specialties (ABMS) in 1937, which since 1991 includes 24 member boards. Boards arose in the early 20th century primarily to define the boundaries and content of specific specialties, as a voluntary system deemed a mark of excellence and professional achievement. 1 Although still voluntary, board certification is increasingly recognized by consumers, health systems, and insurers as a highly desired, or even mandatory, credential. Most boards issued lifetime certificates until 2002, when all ABMS boards agreed upon standards for recertification and evaluation of practice performance every 6- to 10-years, through maintenance of certification (MOC).
The 3 leading entities in the U.S. that collectively oversee physician board certification in 26 recognized medical specialties (excluding LM) are the ABMS, with 950 000 certified diplomates by 24 member boards, 2 the American Osteopathic Association (AOS), with 38 000 certified diplomates by 18 medical specialty boards, 3 and the American Board of Physician Specialties (ABPS), with 5000 certified diplomates by 20 governing boards. 4 The ABLM is one of many U.S. independent specialty boards (not affiliated with ABMS, AOS, or ABPS), but does require physician diplomates be board-certified in their primary specialty by an ABMS member board or AOS as a prerequisite to further certification in LM. 5 Additional recognition, as an LM specialist/intensivist, can be achieved after completing a 1-year LM specialist/intensivist fellowship (educational pathway) or with a threshold level of clinical and scholarly activity in LM (experiential pathway).
The need for this survey arose from a guiding principle upon which ABLM was founded, namely, that eventual ABMS recognition of lifestyle medicine as a subspecialty or member board was needed to fully establish lifestyle medicine as a legitimate specialty of mainstream medicine. This premise, however, had never been validated through feedback from current, and future, ABLM diplomates, so the need for a survey was apparent. In particular, the rapid growth of ABLM diplomates in recent years provide a robust potential survey base, and the growing interest in LM certification created an opportune time to incorporate diplomate feedback into future collaborative efforts.
Methods
A survey invitation was sent electronically to all physician members of ACLM with a completion incentive based on a random drawing from all respondents for 5 free registrations to the fall 2022 annual meeting of ACLM (approximately an $800 value). The 49-item survey was created in Microsoft Forms and completed using a web-based interface. Descriptive information was anonymous, and limited to essential information to reduce administrative burden, with data including ACLM membership year, country of residence, state (in U.S.) of clinical practice, gender, medical specialty, percentage of clinical practice time dedicated to lifestyle medicine, ABLM diplomate status, and intent to pursue certification if not a current ABLM diplomate.
In addition to basic, descriptive information, the broad survey topics were achieved through consensus of the ABLM Board of Directors, and included ABLM certification benefits, the general impact of certifying body in lifestyle medicine, the personal impact (on the diplomate) of certifying body in lifestyle medicine, the future of certification in lifestyle medicine, intensive therapeutic lifestyle change (ITLC), and the relationship of lifestyle medicine to mainstream medicine. A draft of the survey questions was provided to members of the ABLM Board of Directors for feedback and revision prior to agreeing upon the final survey format. The survey required approximately 15 minutes of time for completion.
Most responses were graded with a 5-point Likert scale of strongly agree, agree, neutral, disagree, and disagree strongly. For purposes of analysis and presentation, the strongly agree and agree responses were combined as “agree,” with the strongly agree responses listed parenthetically in all summary tables. The same format was followed for strongly disagree and disagree responses. Descriptive and analytic statistical analysis was performed using IBM SPSS Statistics, version 28. Comparison of responses for ABLM diplomates vs those not certified by ABLM was performed with the independent-samples Mann–Whitney U test, with a 2-tailed significance value of P = .05.
Results
Descriptive Characteristics of Survey Respondents and Eligible Sample.
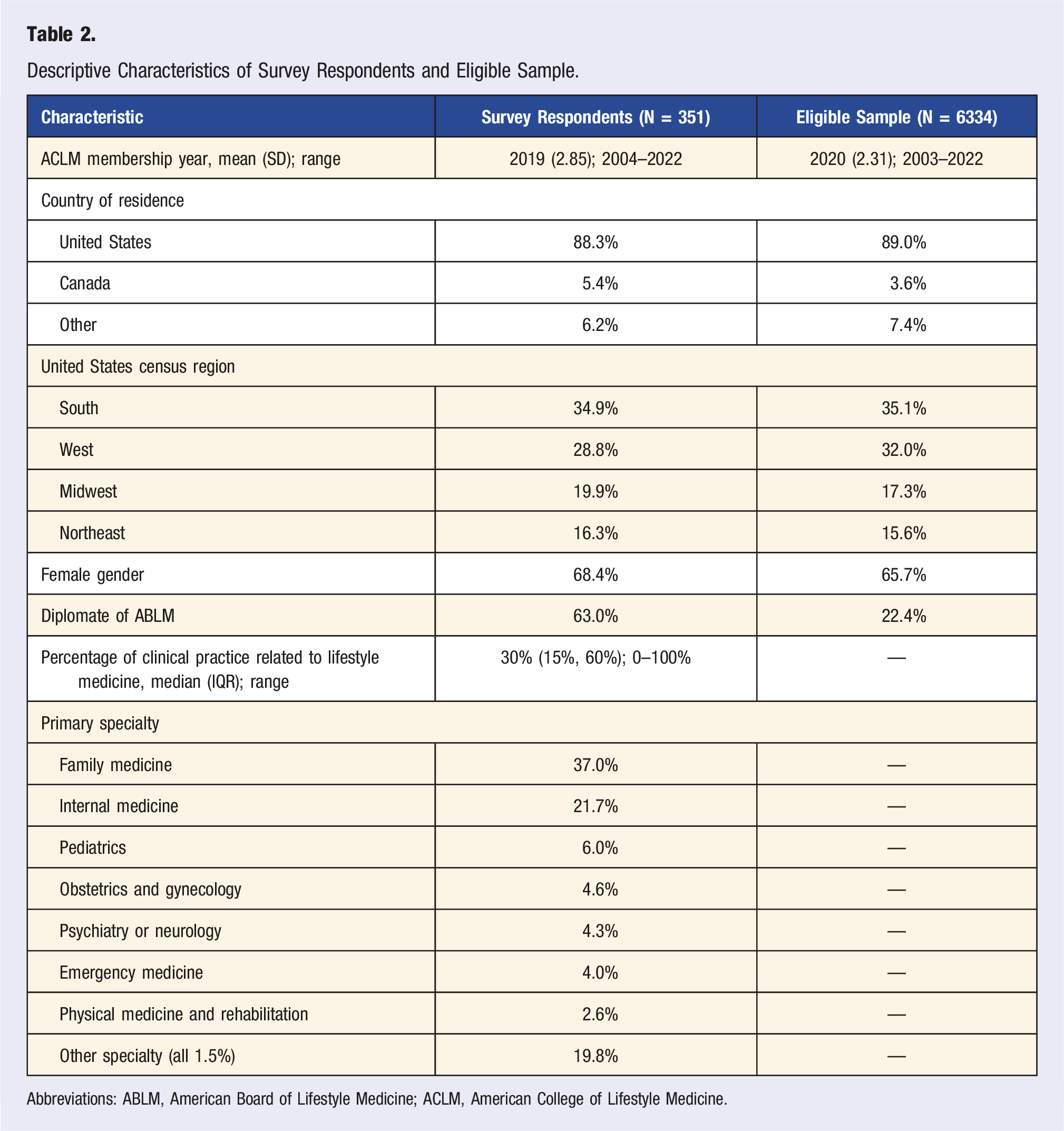
Abbreviations: ABLM, American Board of Lifestyle Medicine; ACLM, American College of Lifestyle Medicine.
American Board of Lifestyle Medicine vs American Board of Medical Specialties as Certifying Body
Perceived Benefits of Certification in Lifestyle Medicine.
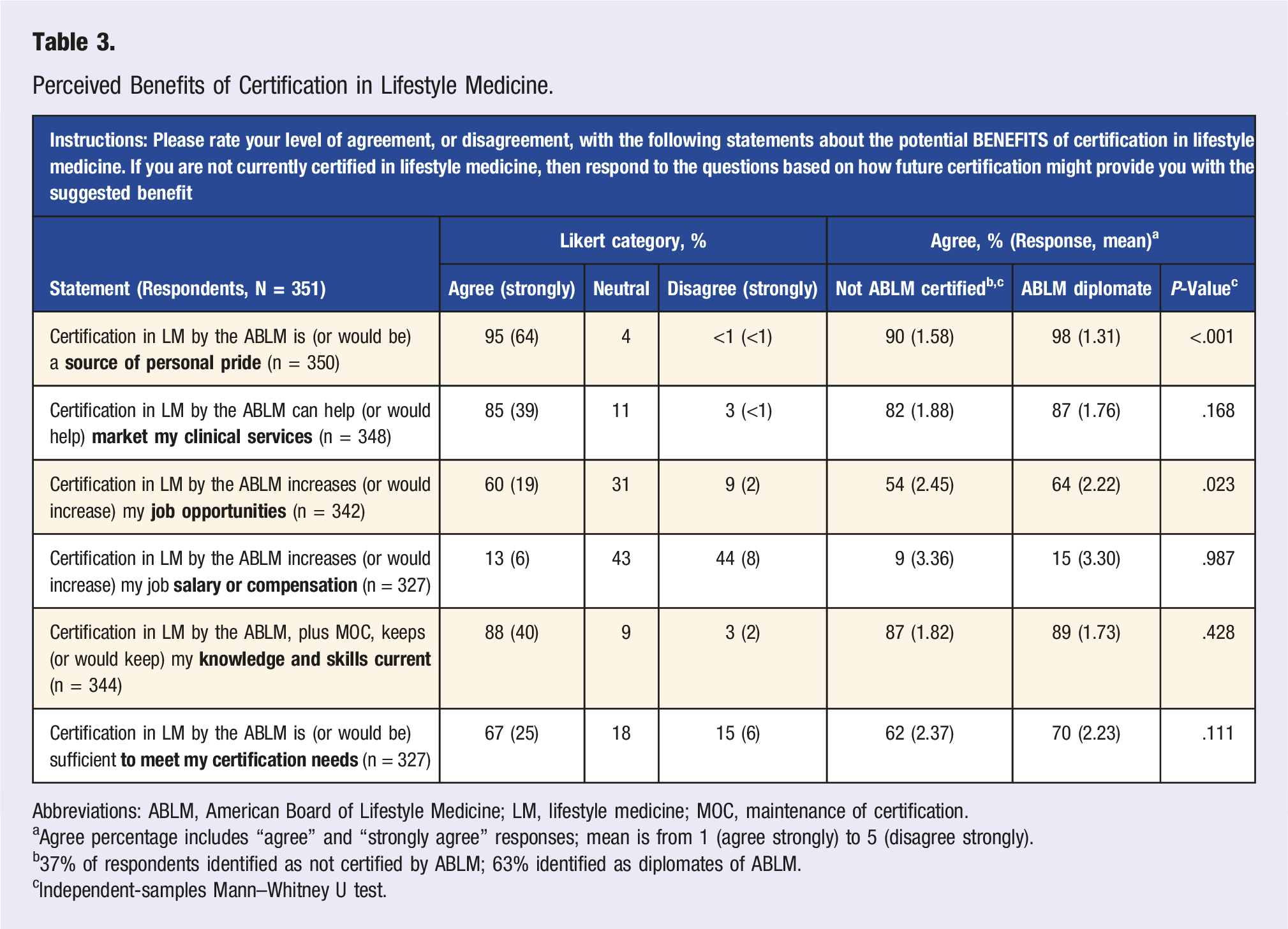
Abbreviations: ABLM, American Board of Lifestyle Medicine; LM, lifestyle medicine; MOC, maintenance of certification.
aAgree percentage includes “agree” and “strongly agree” responses; mean is from 1 (agree strongly) to 5 (disagree strongly).
b37% of respondents identified as not certified by ABLM; 63% identified as diplomates of ABLM.
cIndependent-samples Mann–Whitney U test.
Open Text Response for Additional ABLM Certification Benefits.
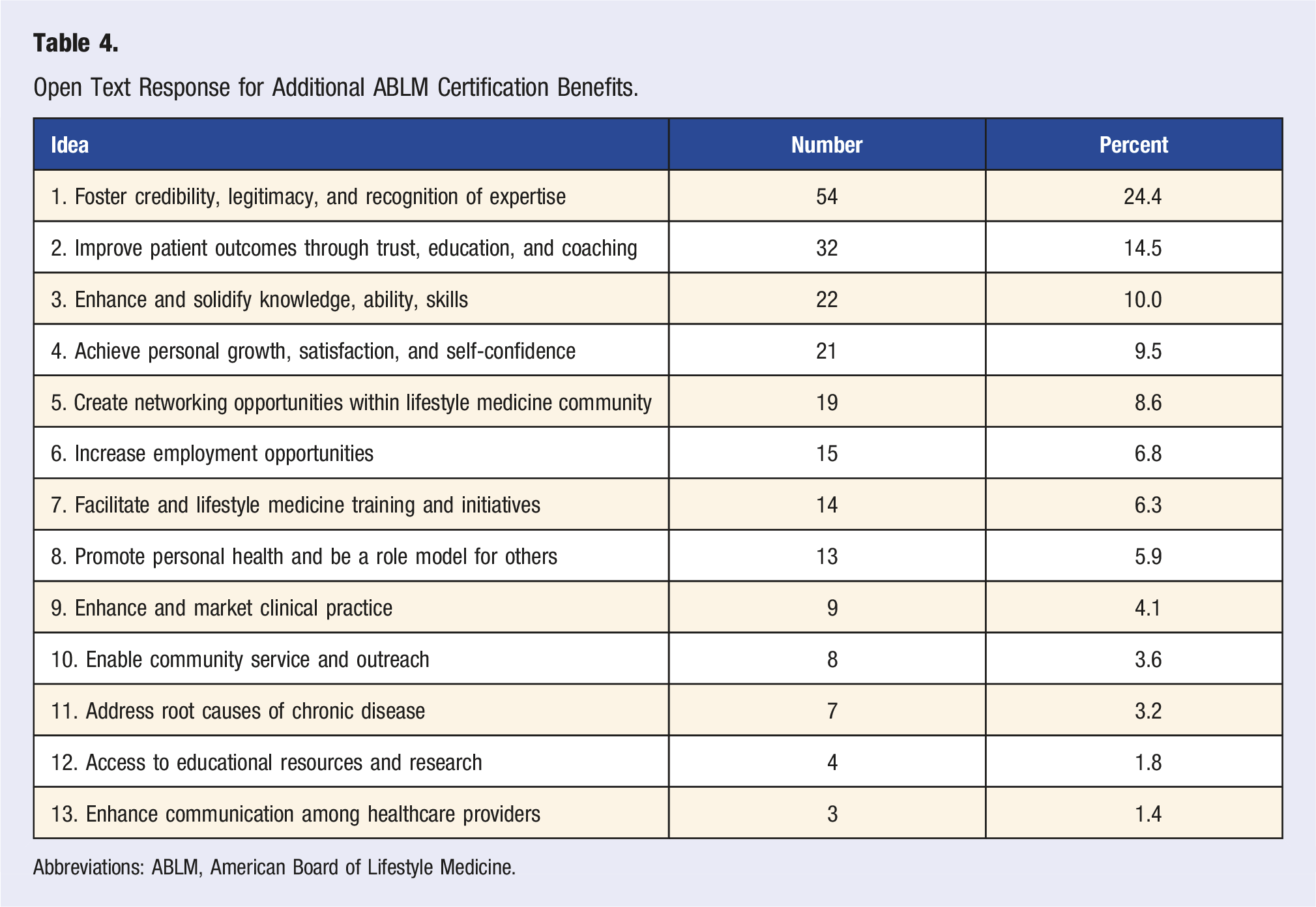
Abbreviations: ABLM, American Board of Lifestyle Medicine.
General impact of certifying body for lifestyle medicine.
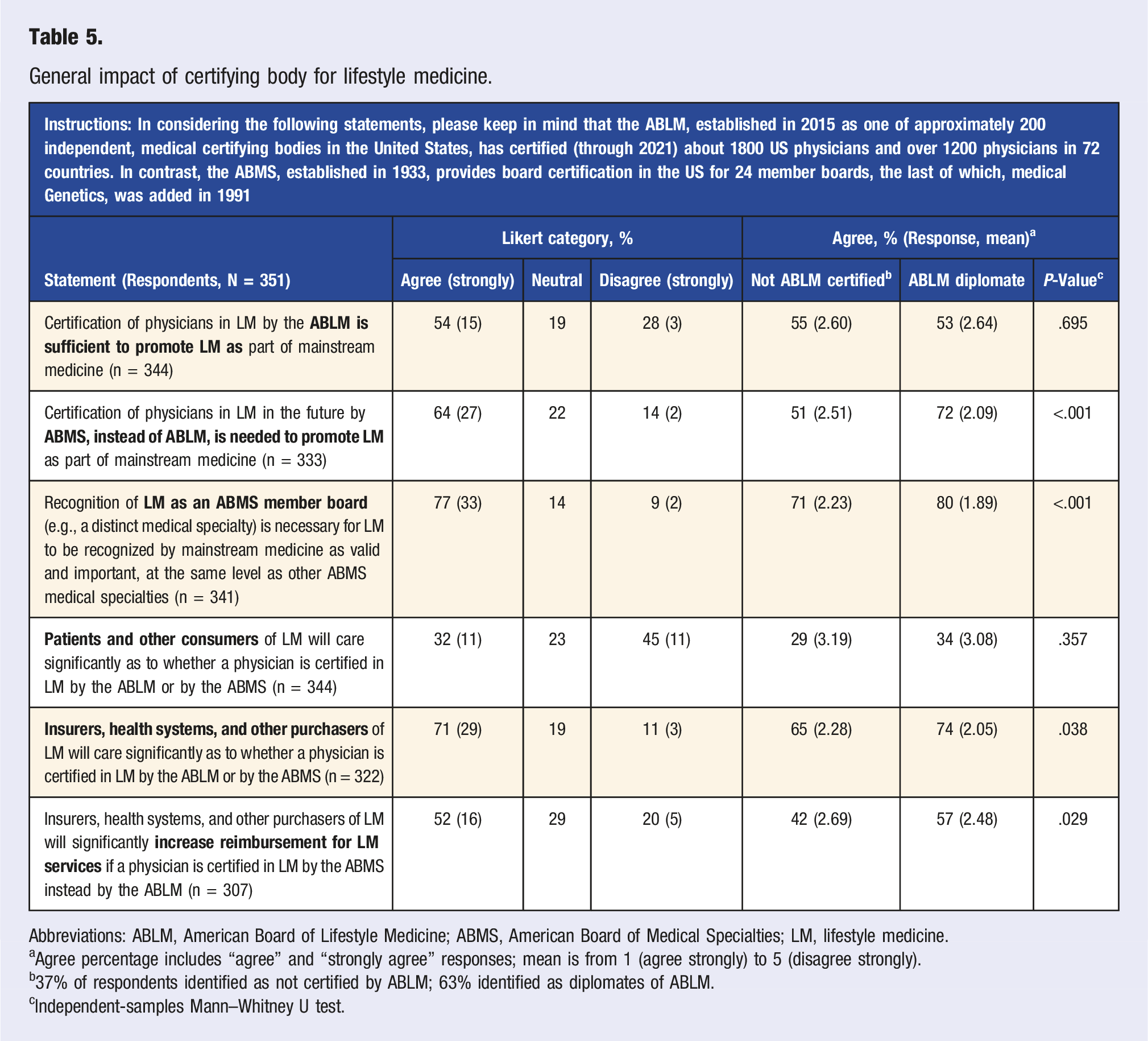
Abbreviations: ABLM, American Board of Lifestyle Medicine; ABMS, American Board of Medical Specialties; LM, lifestyle medicine.
aAgree percentage includes “agree” and “strongly agree” responses; mean is from 1 (agree strongly) to 5 (disagree strongly).
b37% of respondents identified as not certified by ABLM; 63% identified as diplomates of ABLM.
cIndependent-samples Mann–Whitney U test.
Personal impact of certifying body for lifestyle medicine.
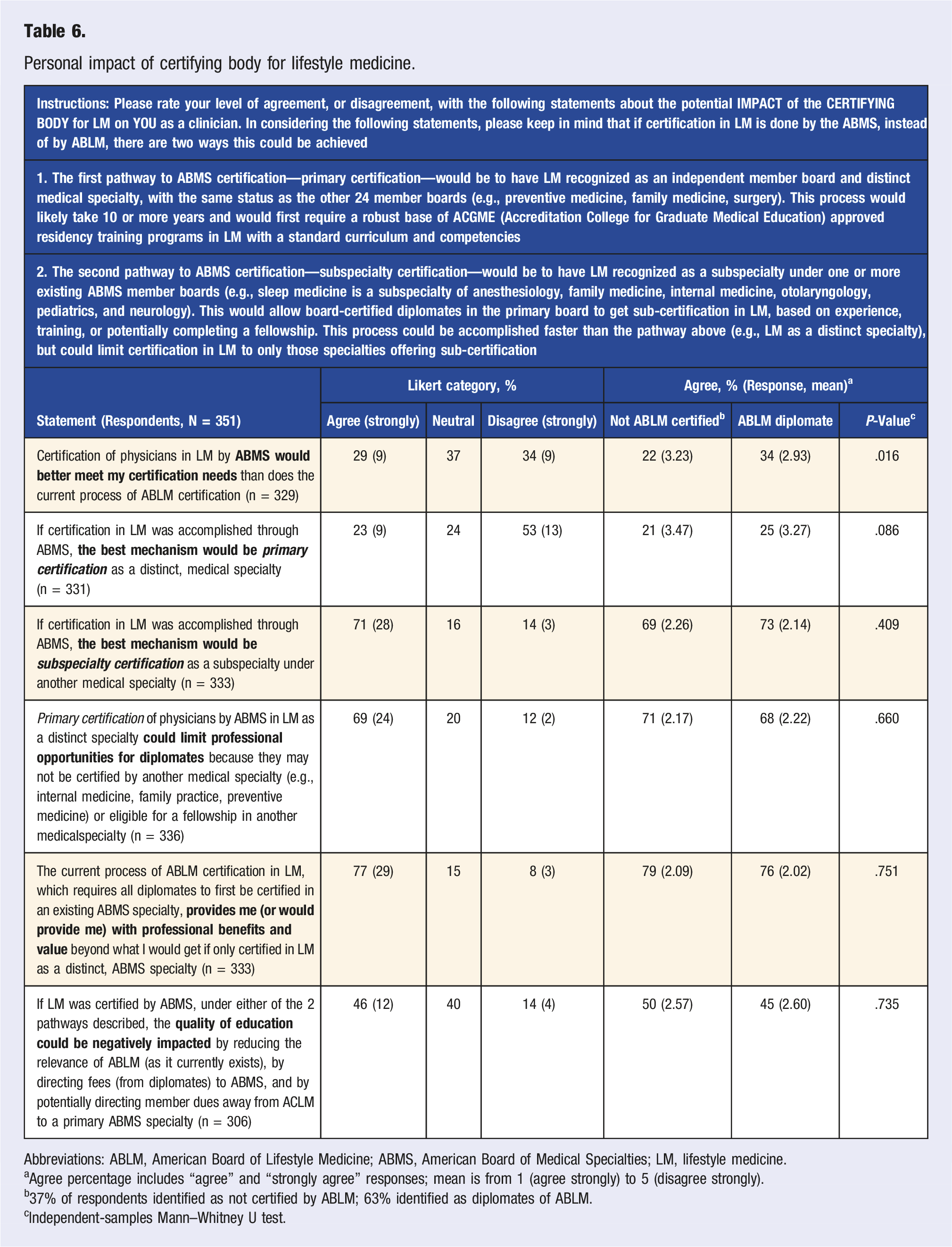
Abbreviations: ABLM, American Board of Lifestyle Medicine; ABMS, American Board of Medical Specialties; LM, lifestyle medicine.
aAgree percentage includes “agree” and “strongly agree” responses; mean is from 1 (agree strongly) to 5 (disagree strongly).
b37% of respondents identified as not certified by ABLM; 63% identified as diplomates of ABLM.
cIndependent-samples Mann–Whitney U test.
Future of Lifestyle Medicine and Intensive Therapeutic Lifestyle Change
Future of Certification in Lifestyle Medicine.
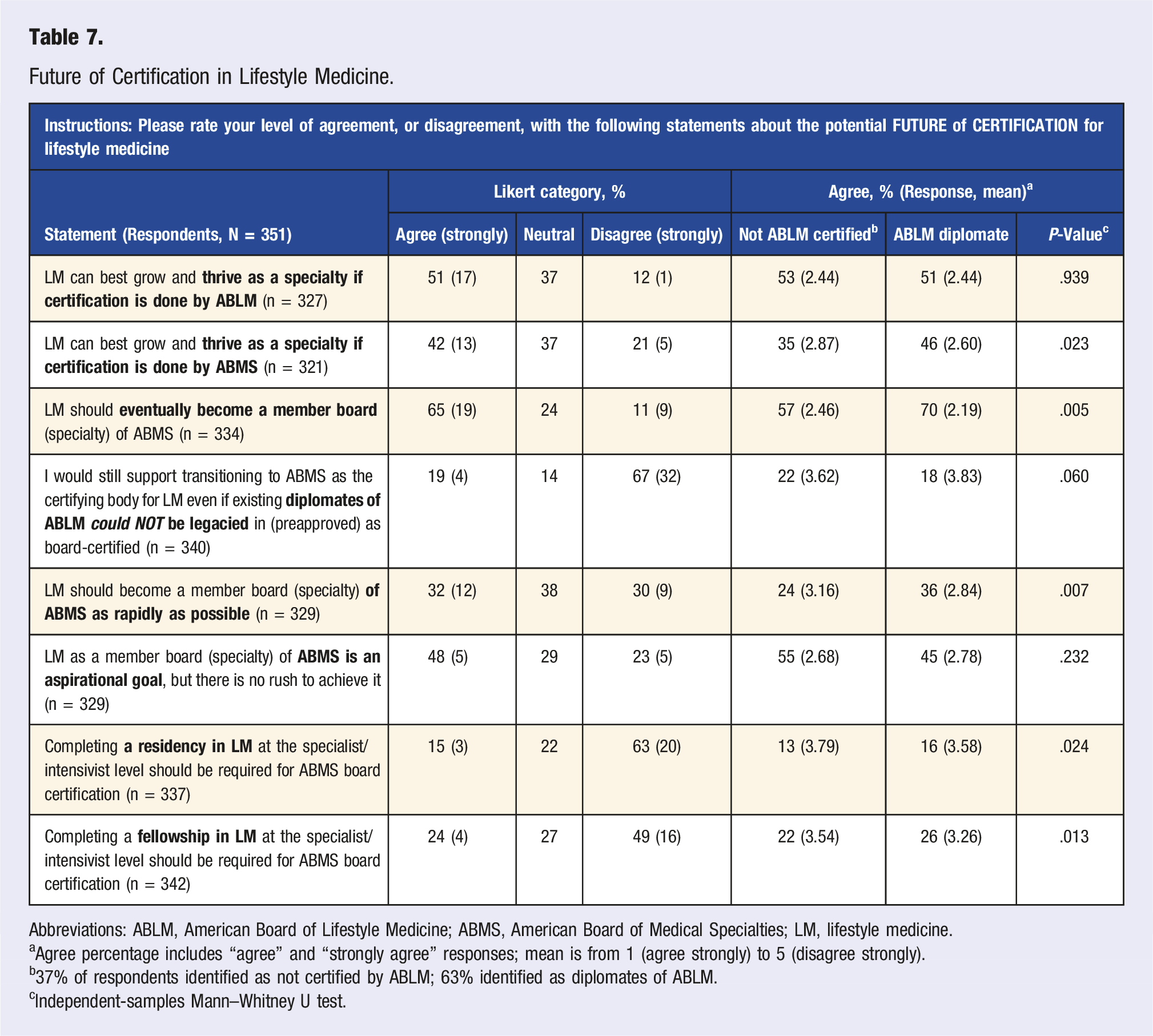
Abbreviations: ABLM, American Board of Lifestyle Medicine; ABMS, American Board of Medical Specialties; LM, lifestyle medicine.
aAgree percentage includes “agree” and “strongly agree” responses; mean is from 1 (agree strongly) to 5 (disagree strongly).
b37% of respondents identified as not certified by ABLM; 63% identified as diplomates of ABLM.
cIndependent-samples Mann–Whitney U test.
Intensive Therapeutic Lifestyle Change.
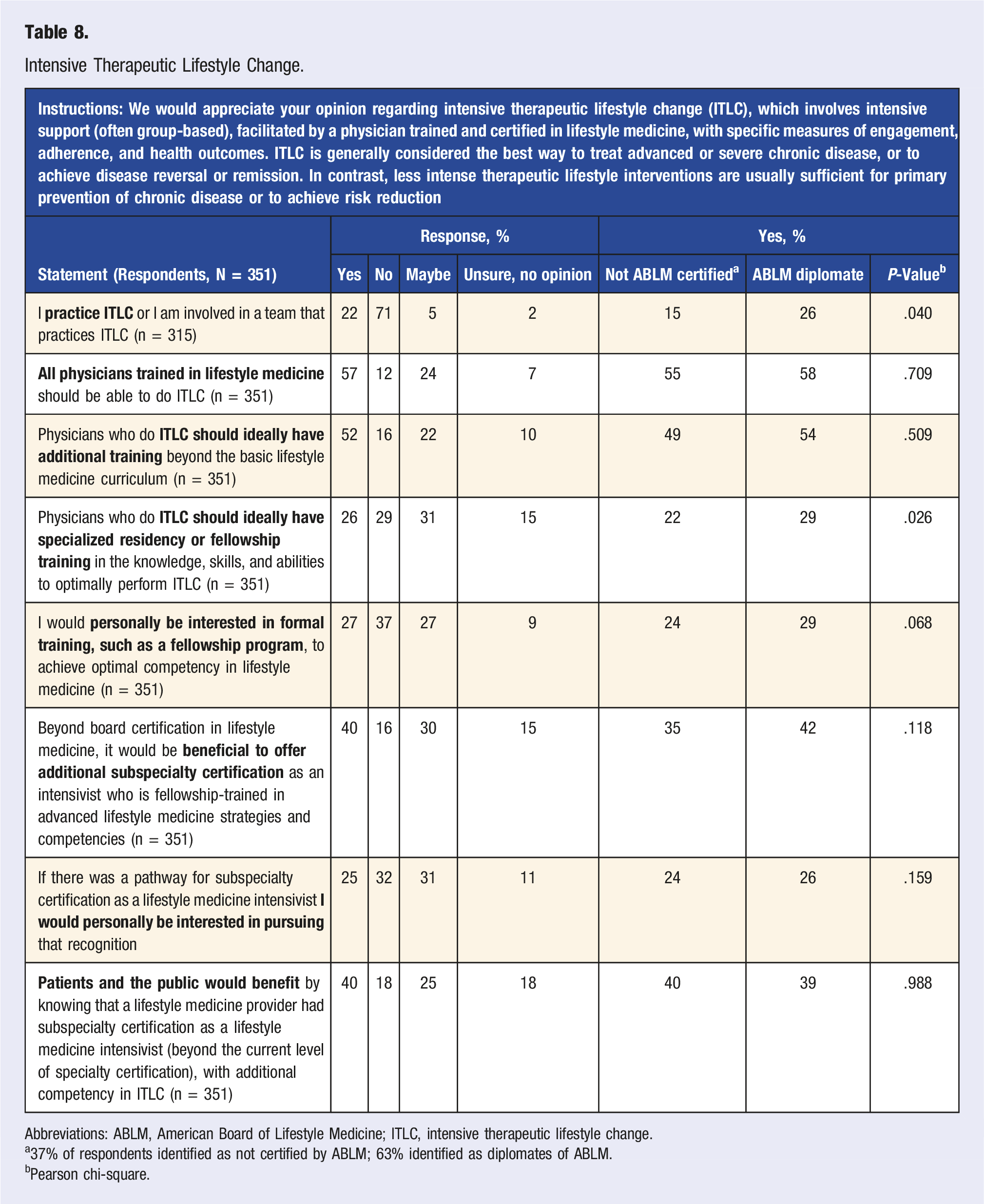
Abbreviations: ABLM, American Board of Lifestyle Medicine; ITLC, intensive therapeutic lifestyle change.
a37% of respondents identified as not certified by ABLM; 63% identified as diplomates of ABLM.
bPearson chi-square.
Lifestyle Medicine and Mainstream Medicine.
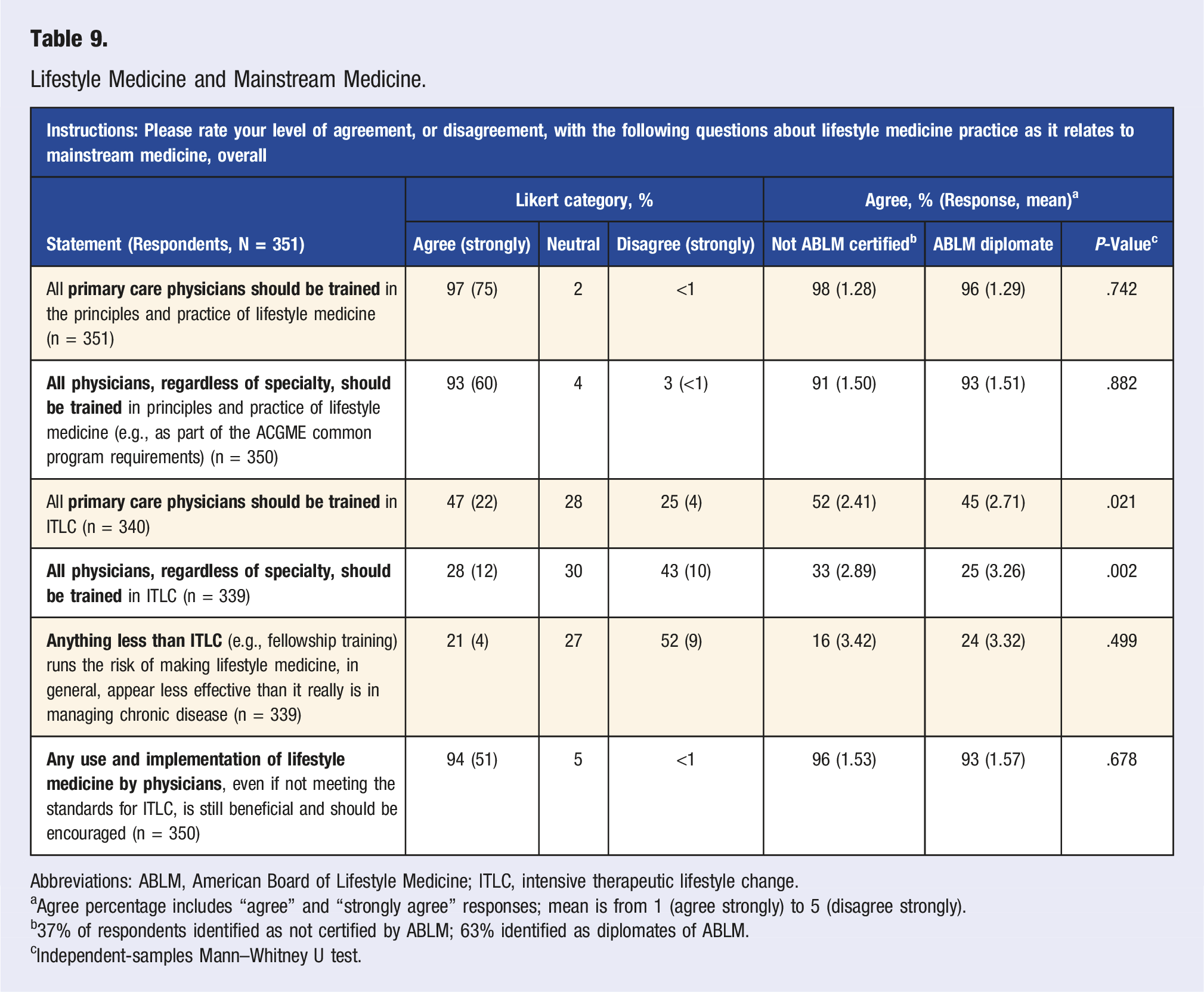
Abbreviations: ABLM, American Board of Lifestyle Medicine; ITLC, intensive therapeutic lifestyle change.
aAgree percentage includes “agree” and “strongly agree” responses; mean is from 1 (agree strongly) to 5 (disagree strongly).
b37% of respondents identified as not certified by ABLM; 63% identified as diplomates of ABLM.
cIndependent-samples Mann–Whitney U test.
Discussion
Key Insights from ACLM Member Physicians Regarding Certification in Lifestyle Medicine.
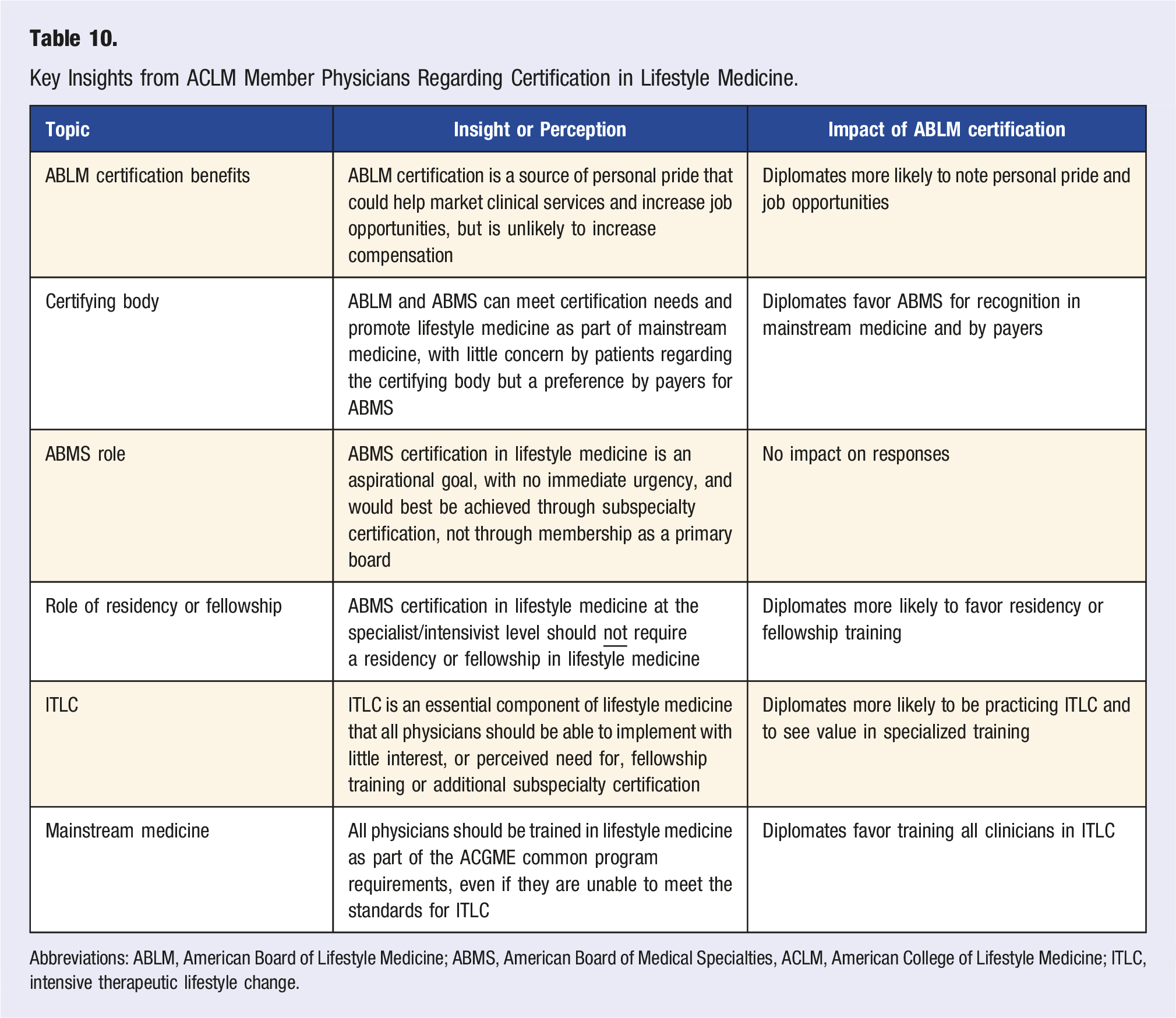
Abbreviations: ABLM, American Board of Lifestyle Medicine; ABMS, American Board of Medical Specialties, ACLM, American College of Lifestyle Medicine; ITLC, intensive therapeutic lifestyle change.
Strengths of our research include face validity based on extensive feedback on question stems and responses from the ABLM board of directors, which helped promote clarity, relevance, and timeliness. We used a 5-point Likert response scale with well-defined cut-points that are standard in survey research. The sample of 351 respondents, although reflecting only 5.5% of ACLM physician members, is representative of the accessible sample (Table 2), except for a higher prevalence of ABLM diplomates (63% vs 22%), which may improve insight into the certification value and process. About 65% of respondents practice primary care (Table 2), potentially limiting generalizability to specialty settings. Last, it is unclear how well respondent perceptions about the public, insurers, and health systems truly reflect their views on the value and meaning of certification in LM.
History and Value of Board Certification
Board certification is a natural consequence of medical specialization, which began with specific body parts in ancient Greece and continued later in Rome under the humoral theory of systemic disease. 6 Medical specialists, however, first became a recognizable social category in 19th century Europe and North America, leading to a community of scholars who considered proper classification the best way to manage population health and promote innovation. Specialist recognition through board certification began in the early 20th century, which defined specialty boundaries and offered a voluntary system to acknowledge physician excellence and achievement. 1 Although board certification remains largely voluntary, it is increasingly sought by consumers, insurers, and health systems as a highly desired, or sometimes mandatory, credential.
The value of board certification is summarized nicely by the ABMS, which states “Certification by an ABMS Member Board helps demonstrate to the public that a physician and medical specialist meets nationally recognized standards for education, knowledge, experience, and skills and maintains their certification through continuous learning and practice improvement in order to provide high quality care in a specific medical specialty or subspecialty.” 7 Similarly, the ABPS notes that “Board certification with the ABPS serves as demonstrable proof that a physician has the skills and knowledge to deliver world-class medical care.” 8 With regards to LM, the ABLM mission statement reads, “Certification as an ABLM diplomate signifies specialized knowledge in the practice of LM and distinguishes a physician as having achieved competency in LM.” 9 The common thread in all of these statements is assuring patients, consumers, and other stakeholders that the practitioner has demonstrated the skill, abilities, and knowledge to deliver medical care of the highest quality.
Perceptions of higher quality of care from board-certified physicians are supported by studies associating better outcomes with certification, but effect sizes are modest and based on observational studies that do not necessarily imply causation. 10 More recently, however, a historical cohort of over 350 000 patients followed for 7 years found lower mortality and length of stay for attending physicians trained in a residency program with a 80% or greater certification rate when managing patients with heart failure, heart attacks, pneumonia, or gastrointestinal hemorrhage. 11 Other implications of certification, which overlap with those in Tables 3 and 4, include hospital staff privileges, peer recognition in professional societies, potential higher compensation, a competitive advantage (over non-certified physicians) in attracting patients, and establishing a standard for care and expert testimony in medical malpractice actions. 12 Whereas all respondents considered certification by ABLM a source of personal pride (Table 3), agreement was significantly higher, and nearly universal, for diplomates compared to non-diplomates (98% vs 90%, P < .001).
Implications of the Board Certifying Body
When certification is done by an independent medical board, not associated with ABMS, concerns can arise regarding legitimacy and equivalency of the certifying process. 13 This is much less of a concern when the independent board deals with a specialty that does not significantly overlap with specialty certification offered by ABMS, which is the case for LM because it is relevant to nearly all medical specialties. Given this diversity, the ABLM first requires a potential diplomate to be board-certified by ABMS in their primary specialty, with certification by ABLM as an add-on when qualifying criteria (experiential or educational) are satisfied and an examination is successfully completed. Moreover, 77% of survey respondents (Table 6) agreed that this dual process—with board certification by ABMS as a prerequisite to ABLM recognition as a LM diplomate—provides, or would provide (if not yet ABLM certified), professional benefits and value beyond what they could get if only certified by ABMS in LM as a distinct specialty.
The current model of ABLM physician certification as an add-on to the primary ABMS board serves diplomates well (Tables 3–6), despite 65% agreeing (Table 7) that LM should eventually become an ABMS member board (but with no urgency). Moreover, 77% agree (Table 5) that eventual ABMS recognition is needed for LM to be fully recognized by mainstream medicine as comparable to other official ABMS specialties. As LM is more formally integrated into residency programs (especially primary care) and specialized fellowship programs expand, the number of physicians who practice primarily LM, including ITLC, will likely grow significantly. 5 These clinicians with more intense LM training and experience can be recognized as specialist/intensivist diplomates by ABLM, but in the future may be more suited to direct ABMS recognition as a subspecialty or member board. For those with less intense training, who seek certification as physician diplomates through ABLM, the existing add-on process to a primary ABMS board is likely to persist.
There were significant differences (Tables 5 and 6) regarding implications of the certifying body for LM and for ABLM diplomates vs non-diplomates. Diplomates were more likely to agree that ABMS certification offered advantages over ABLM certification for recognition as part of mainstream medicine (72% vs 51%, P < .001), gaining equivalency to other ABMS medical specialties (80% vs 71%, P < .001), getting enhanced compensation from purchasers of health care (57% vs 42%, P = .029), and having their future certification needs met (34% vs 22%, P = .016). Conversely, there were no differences in whether consumers would care about the certifying body, or if ABMS certification would best be achieved by subspecialty certification under another member board or directly as a distinct, new member board.
Future of Board Certification in Lifestyle Medicine
The future of certification in LM will likely continue to include maintenance of certification (MOC), regardless of certifying body. Certification was initially a lifetime credential until the 1960s when time-limited certificates were introduced that required periodic reexamination. Recertification was superseded by continuing certification (MOC) in 2000, emphasizing physician learning, advancement, and current competence. 14 The ABMS requires all member boards to offer MOC, with the intent of “…serving diplomates, the public and the profession by providing a system that supports the ongoing commitment of diplomates to provide safe, high quality, patient-centered care.” 14 ABLM currently offers MOC to diplomates, but the process will likely evolve concurrent with other changes in LM medicine training and certification. Similar to the ABMS, the AOA uses osteopathic continuous certification 15 but, in contrast, the ABPS offers recertification every 8 years for diplomates of ABPS or other boards (ABMS, AOA) whose diplomates prefer this process over MOC. 16
Regarding the future of board certification in LM, current ABLM diplomates again showed a preference for more ABMS engagement than did non-diplomates (Table 7). Diplomates were more likely to agree that LM would grow best if certification was done by ABMS (46% vs 35%, P = .023), that LM should ultimately become an ABMS member board (70% vs 57%, P = .005), and that ABMS certification should require completing a residency in LM (16% vs 13%, P = .024) or a fellowship program (26% vs 22%, P = .013). Diplomates and non-diplomates agreed on ABMS recognition as a non-urgent, aspirational goal, ideally with a legacy exception to ensure that existing ABLM diplomates get preapproved for certification should ABMS become the certifying body.
Conclusion
LM is a vibrant, rapidly growing, and increasingly relevant medical discipline (Table 1) whose diplomates are well-served by the existing model of ABMS certification. The future is likely to see changes, and evolution, of the MOC process and the relationship of LM to ABMS, as a potential member board, subspecialty board, or focused practice designation 17 (not discussed in the survey). Concurrent with the evolution of certification, LM training will evolve through enhanced integration with residency training, expansion of fellowship opportunities, and potential inclusion in residency common program requirements.
The ACLM and ABLM, despite their relatively recent appearance in medicine, are well-positioned to support the rapid and ongoing growth of LM (Table 1) by meeting the needs of members, clinicians, the public, educators, health systems, and other stakeholders. Survey respondents, regardless of certification status, agreed that becoming an ABLM diplomate both meets their certifying needs and offers substantial personal and professional benefits, with the caveat that ABMS recognition is an aspirational goal. The ABLM is committed to maximizing the value of certification, through ongoing stakeholder feedback and by engaging leadership at ABMS and its member boards on the value, relevance, and importance of LM as an essential aspect of mainstream medical practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Richard Rosenfeld compensated by ACLM for a part-time role as Sr. Advisor for Medical Society Relations and by the ABLM for a part-time role as Chief Medical Officer.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the funds from the American Board of Lifestyle Medicine to cover the cost of incentives for survey completion. Staff time and resources provided by the American College of Lifestyle Medicine.