
Abstract
The Mediterranean diet has positive effects on primary and secondary prevention of cardiovascular disease including stroke, yet dietary counseling to stroke patients is under-utilized. This study aimed to develop a culturally adapted Mediterranean diet and introduce it to patients admitted to the hospital for acute ischemic stroke with at least one metabolic risk factor (type 2 diabetes mellitus [DM], hypertension [HTN], high low-density lipoprotein [LDL], low high-density lipoprotein [HDL], and/or body mass index [BMI] > 25). Dietary adherence and nutritional knowledge were measured at baseline and 30, 90, and 120 days post-stroke. Weight, hemoglobin A1C [HbA1C], and triglycerides [TG] were assessed at baseline and follow-up. The study enrolled 54 participants, 50 of whom had sufficient data for analysis. Dietary adherence and nutritional knowledge scores increased in 76.4% of participants, with a statistically significant median increase for each. Additionally, participants had significantly lower weight, HbA1C, and TG at follow-up than baseline. This study showcases the potential to introduce a culturally appropriate Mediterranean diet at the point-of-care, and significantly influence dietary adherence and nutritional knowledge and multiple stroke risk factors.
“The Mediterranean diet has shown a benefit in reducing both acute CVD events and CVD mortality, in both primary and secondary prevention studies.”
Introduction
Stroke is the second most common cause of deaths worldwide, after ischemic heart disease, and a leading cause of long-term disability and lost wages. 1 Every year there are 795,000 incident strokes in the United States (US), with 23% of these being recurrent strokes, and 137,000 resulting in death. 2 Among these, 87% are ischemic, with the remaining 13% encompassing all types of hemorrhagic strokes. An additional estimated 240,000 of US adults experience a transient ischemic attack (TIA) every year, with an annual risk for future ischemic stroke after an initial TIA of 3% to 4%. 3 The Southeastern US, named the “Stroke Belt,” is disproportionately affected by stroke, with African Americans being the most affected. 4 Although the mortality rate from CVD had been on the decline for more than a decade, a concerning plateau in that trend and even increase in CVD mortality has emerged recently, largely fueled by the high prevalence of diet-related obesity and diabetes. 2
Poor diet quality has been identified as the leading cause of premature deaths and disability in the United States, 5 and has been found to be an independent risk factor for mortality in stroke. 6 Even though diet affects risk factors for primary and secondary strokes including hypertension, diabetes, hyperlipidemia, it may also be related to stroke through other mechanisms independent of their role in blood pressure and cholesterol 7 such as insulin resistance and inflammation. 8 The Primary Prevention of Cardiovascular Disease with a Mediterranean Diet trial (PREDIMED) showed that, in a population with mixed risk factors and treatments, compared to standard low-fat diets, consuming a Mediterranean-style diet was associated with a 30% reduction in major cardiovascular events, mainly driven by less strokes. 9 In secondary prevention, the Lyon Diet Heart study documented a 72% reduction of myocardial infarction (MI) and cardiac deaths through dietary modification reflecting the Mediterranean pattern. 10 In secondary stroke prevention, the Mediterranean diet has been shown to affect vascular risk factors and lower the risk of cardiovascular disease incidence. 11 A recent meta-analysis of nine prospective cohort studies showed that healthy diet scores defined as a Mediterranean dietary pattern tended to improve in all races/ethnicities. However, disparities present at the beginning widened with time, with smaller improvements in healthy diet scores seen in minority groups and those with lower income or education. 12
Strategies involving physicians to lower cardiovascular risk through diet education and support have been shown to be effective and well received by patients, yet they continue to be under-utilized. 13 This may be because very few, an estimated 10%–30% of physicians, get adequate training in delivering nutritional guidance and only 8% feel confident in their delivery. 14 The financial burdens of care to patients, families, and healthcare delivery systems from CVD are very high, especially for the uninsured and Medicaid patients.15,16 Given the potential for CVD event reduction of 30% to 70% from dietary changes,9,10 the potential for improving public health and lowering healthcare costs by emphasizing nutrition education and practice is substantial.
Methods
Study Overview
This study took place at the Emory University Hospital Midtown Hospital, Atlanta, GA. It is the initial phase of a dietary intervention study in stroke patients modeling the Mediterranean dietary pattern adapted to the southern soul food palate (Mediterranean Soul Food Diet, MSFD).
Study Aim
The objective of the study was to implement patient education on a culturally tailored diet in patients acutely hospitalized with a stroke, and to determine whether this implementation influenced Mediterranean diet adherence, nutritional knowledge, and reduction in stroke risk factors.
Participant Selection and Enrollment
Eligible participants were hospitalized patients with (1) imaging-proven acute ischemic stroke 18-80 years-old; (2) one or more risk factors including type 2 diabetes mellitus or HTN, elevated LDL cholesterol levels >100, low HDL cholesterol levels <40, overweight or obesity defined as a BMI >29; and (3) discharged home on an oral diet. Exclusion criteria included TIA patients, patients not discharged home, patients unable to take an oral diet, and patients with a positive urine drug screen. Enrollment began in September 2019, and the last participant was recruited in March 2020. The study was stopped prematurely due to the sudden drop in acute stroke admissions related to the coronavirus disease of 2019 (COVID-19) pandemic.
Informed consent was obtained from patients or their power of attorney caregivers when patients were unable to provide consent. During their acute hospital stay, subjects completed two validated baseline questionnaires: a 14-item dietary questionnaire to assess adherence to the Mediterranean diet (Mediterranean Diet Adherence Score, MEDAS) 17 and a 15-item dietary questionnaire to assess nutritional knowledge (Mediterranean Diet Nutritional Knowledge, MDNK). 18 MEDAS scores ranged from 0 to 14 with scores lower than 10 defined as low adherence to the Mediterranean diet. MDNK scores ranged from −15 to 15, with higher scores indicating more nutritional knowledge of the Mediterranean diet.
Interventions
The dietary intervention is detailed in the Supplementary Appendix. It was created by a food and nutrition nonprofit, Oldways, that first developed a Mediterranean Diet Pyramid in 1993 in collaboration with the Harvard School of Public Health and the WHO. They subsequently adapted the Mediterranean diet to various cultures including the African American culture, which was deemed the MSFD for the purposes of this study. No total calorie restriction was advised, nor was physical activity promoted. The dietary education was performed using motivational interviewing by the inpatient registered dietician (RD), as well as by the neurologist and the neurology advanced practice provider who were initially coached by the RD. Participants completed the initial baseline MEDAS and MDNK during their inpatient stay for their acute stroke as well as over the phone with the neurologist and neurology resident at 30, 90, and 120 days. The education was reinforced with printed materials including a pamphlet and a booklet with 4 weeks of recipes and shopping lists for the three daily meals. Patient caregivers were also educated during their loved ones’ inpatient hospital stay and received the same printed materials. Weight, BP, Hemoglobin A1C (HbA1C), LDL, and triglycerides (TG) values were obtained at baseline and 120 days, the latter collected in clinic.
End Points
The primary end points were dietary adherence to the Mediterranean diet based on the MEDAS questionnaire and nutritional knowledge retention based on the MDNK questionnaire as well as weight, HbA1C, and TG.
Statistical Analysis
Wilcoxon Signed-Ranks tests were performed for ordinal MEDAS and MDNK data while paired t-tests were performed for numerical weight, HbA1C, and TG data. Two-tailed tests were used for all analyses. Follow-up MEDAS and MDNK scores were obtained at 30, 90, and 120 days post-stroke whereas weight, HbA1C, and TG values were obtained at 120 days. It was decided to average the MEDAS and MDNK follow-up values given missing data at later time points.
Results
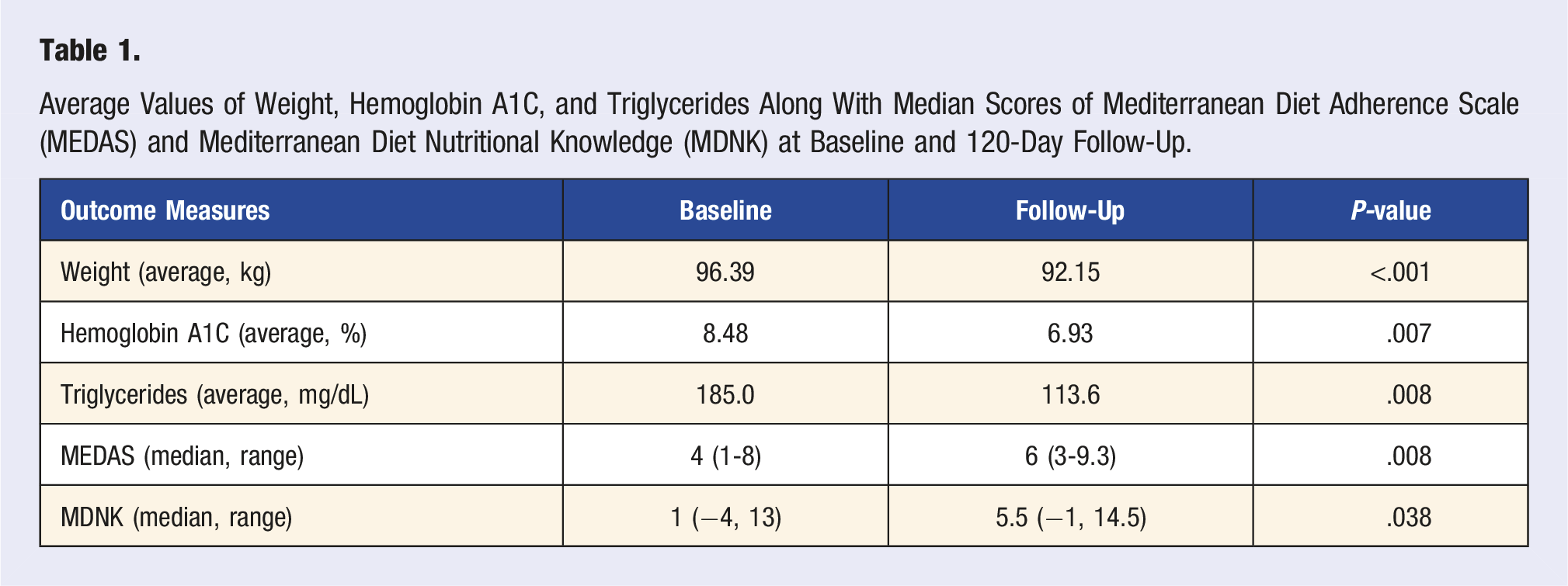
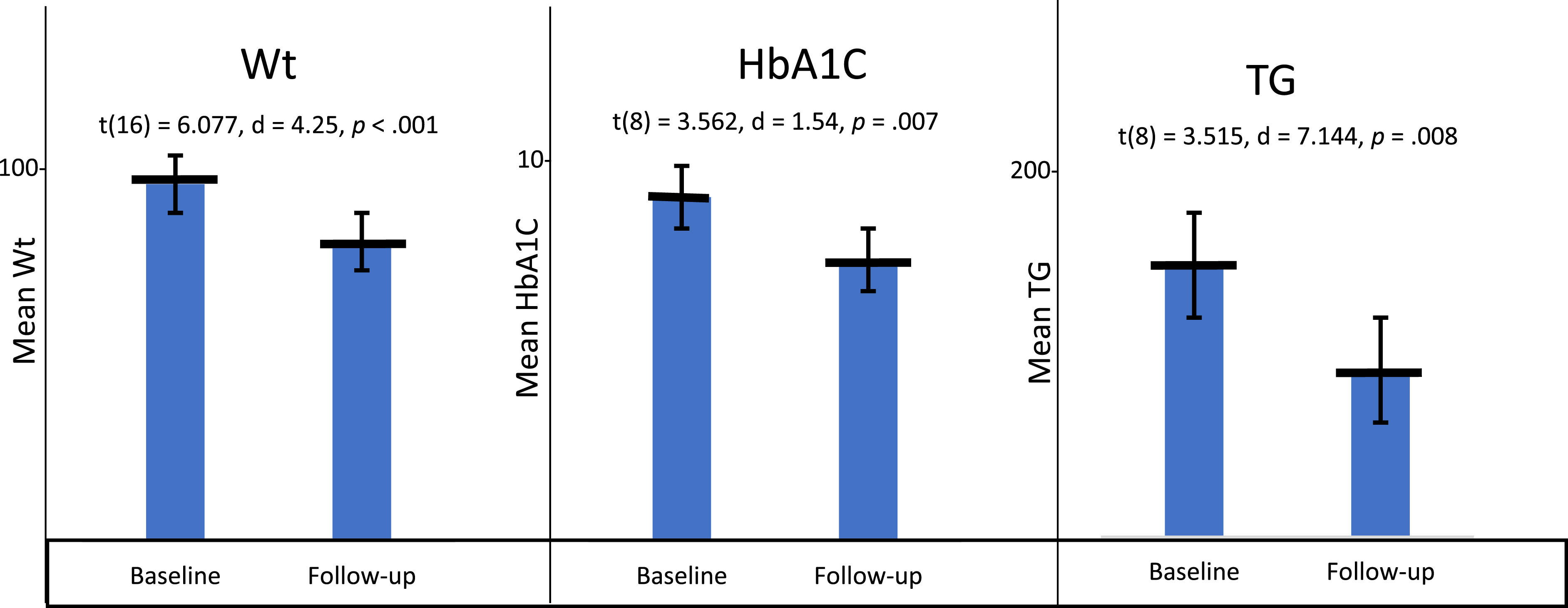
Fifty-four participants were enrolled in the study from September 2019 to March 2020 [Mean age 59 (46-80), 62% Female, 83% African American]. All patients had at least one vascular risk factor, 77% (41) were obese, 91% (49) had a history of hypertension, 66% (35) had a history of diabetes, 77% (41) had a history of hyperlipidemia, and 42% (22) had all 4 vascular risk factors. Dietary adherence increased in 72.8% of participants with an increase from a median MEDAS of 4 at baseline to 6 averaged across the follow-up periods (Z = -2.663, P = .008). The range of MEDAS scores at baseline was 1 to 8 compared to 3 to 9.33 at the 120-day averaged follow-up. Similarly, nutritional knowledge increased in 80.1% of the participants. Scores on the MDNK questionnaire increased over the follow-up period from a median of 1 at baseline to 5.5 at 120-day averaged follow-up (Z = −2.083, P = .038). MDNK scores ranged from –4 to 13 at baseline to –1 to 14.5 at averaged follow-up (Table 1, Figure 1). Weight decreased in participants at 120 days follow-up by an average of −4.24 kg (SD = 2.88, t16 = −6.077, P < .001); HbA1C by an average of –1.54% (SD = 1.30, t8 = −3.562, P = .007); and TG by an average −71.4 mg/dL (SD = 61.0, t8 = −3.515, P = .008) (Table 1, Figure 2). BP did not show a statistically significant difference (data not shown) and LDL was omitted from statistical analysis given concurrent statin initiation as standard of care for stroke secondary prevention. Average Mediterranean Diet Adherence Scale (MEDAS) and Mediterranean Diet Nutritional Knowledge (MDNK) at baseline and follow-up at 120 days. Average Values of Weight, Hemoglobin A1C, and Triglycerides Along With Median Scores of Mediterranean Diet Adherence Scale (MEDAS) and Mediterranean Diet Nutritional Knowledge (MDNK) at Baseline and 120-Day Follow-Up. Baseline and follow-up at 120 days of weight (Wt), hemoglobin A1C (HbA1C), and triglycerides (TG).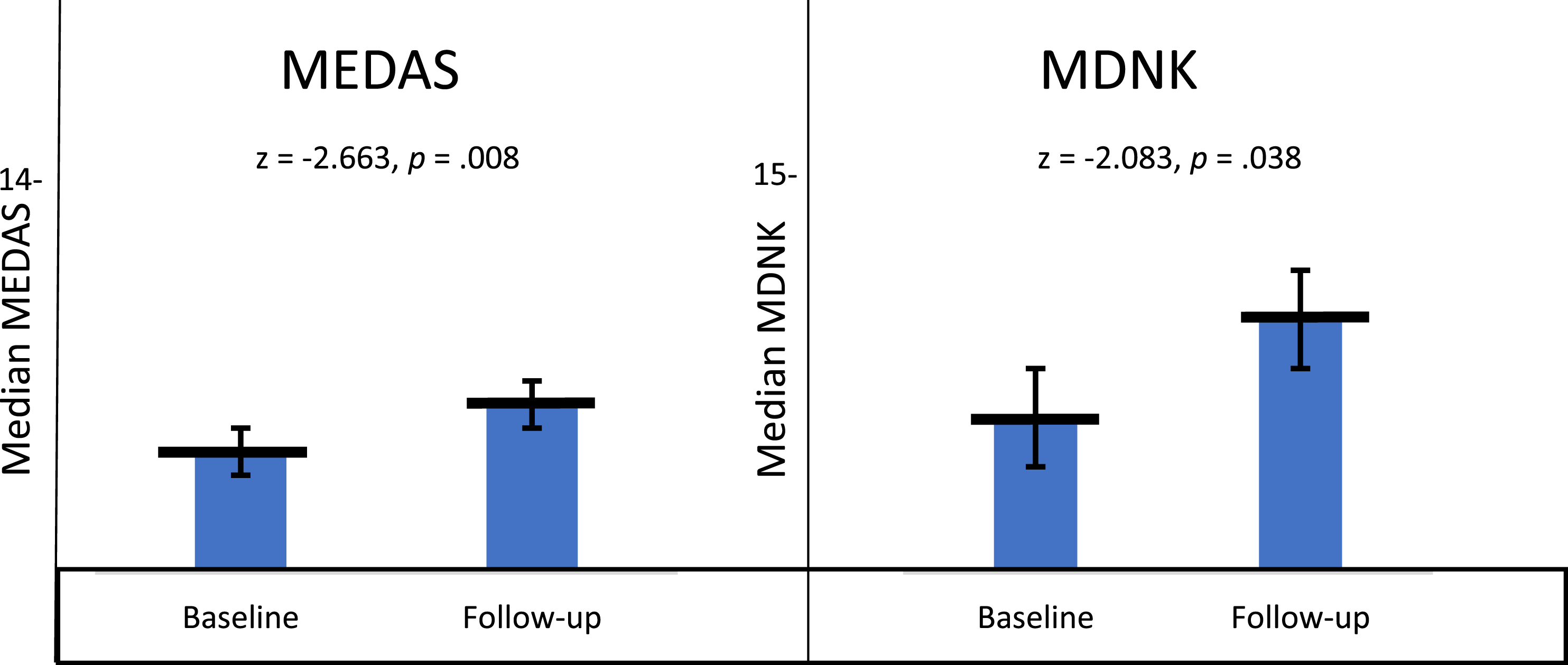
Discussion
Stroke remains a prevalent cause of mortality and disability in the United States (US). Approximately 795,000 people in the US have a stroke each year. 19 HTN, hyperlipidemia (HLD), tobacco use, DM, and obesity are strong but preventable risk factors for both ischemic and hemorrhagic stroke. 20 In the US, since the 1940s, stroke mortality has a geographical predisposition with mortality rates being 2-4 times higher in the Southeast in a region known as the Stroke Belt. The higher mortality rates may be a product of higher incidence, higher case-fatality or both. Currently, the states of Alabama, Georgia, Tennessee, Arkansas, Louisiana, North Carolina, and South Carolina are considered part of the Stroke Belt. This disproportionate divide is likely multifactorial but the high presence of vascular risk factors as well as poor diet and lack of physical activity likely play a substantial role. 21 The REGARDS study estimated the prevalence of stroke risk factors geographically and found that HTN, DM, and tobacco use had higher prevalence in the Southeastern US. 22 While evidence is lacking, another hypothesized etiology of this geographical propensity is dietary differences with presumed poorer dietary intake in the Southeastern region. 21
Lifestyle including diet is an important yet overlooked risk factor for stroke. A large prospective cohort study including two populations of US health professionals that investigated primary prevention of stroke found that about half of ischemic strokes could potentially be attributed to unhealthy lifestyle choices, including smoking, lack of regular exercise, diet, obesity, and alcohol consumption. On the contrary, those who achieved healthy choices in all 5 domains had about an 80% lower risk of ischemic stroke. 23 In a large international case-control study with nearly 27,000 participants from 32 countries, modifiable risk factors, including diet, were investigated in controls as well as ischemic and hemorrhagic stroke patients. Diet was divided into tertiles using the modified Alternative Healthy Eating Index. In patients with ischemic and hemorrhagic stroke, diet scores in the lower 2 tertiles were associated with a 23.2% population attributable risk (PAR) for all stroke worldwide when compared to the highest tertile. Similarly, when the regions of North America, Western Europe, and Australia were grouped together and explored, diet scores in the lower 2 tertiles were associated with 33.3% (CI 24.3-43.7) PAR. 24
The Mediterranean diet has shown a benefit in reducing both acute CVD events and CVD mortality, in both primary and secondary prevention studies. The Lyon Diet Heart study was the first randomized controlled trial to illustrate secondary prevention in individuals with a history of MI, showing an impressive 72% relative risk reduction in the composite outcome of nonfatal MI and cardiac death. 10 Around two decades later, a corrected and republished randomized controlled trial, the PREDIMED study, revealed primary prevention with an approximate 30% relative risk reduction in nonfatal MI, stroke, and cardiac death which included a 40% reduction in stroke. 9 A meta-analysis in 2019 attempted to more definitively assess the benefit in regards to stroke incidence and mortality. 11 This analysis included both published and unpublished cohorts to elucidate the benefit by geographic region and subtype of stroke. It showed that for each 4-point increment in a Mediterranean diet adherence score, there was a 16% relative risk reduction for all combined studies, with 24% reduction in Mediterranean populations and 14% in non-Mediterranean ones. The Mediterranean diet was similarly associated with a 14% lower risk of ischemic stroke and 17% of hemorrhagic stroke. Other studies have further characterized this association, demonstrating that higher adherence is associated with lower NIHSS scores on admission as well as Rankin scores on discharge.25,26 Several dietary patterns outside of the Mediterranean diet have also shown benefits in reduction of acute CVD events including DASH, Nordic, vegetarian, and paleolithic. 27 A commonality among these is a transition to whole foods and minimizing ultra-processed foods. Incidentally, the comparison group in many of these studies is the Western prudent low-fat diet.
Most, if not all, of these studies utilized a dietary adherence tool as it is often not possible or practical to perform a feeding trial. Many of the initial Mediterranean diet studies relied upon food frequency questionnaires for which Mediterranean diet scores were subsequently calculated. However, a more convenient tool called the Mediterranean Diet Adherence Screener, or MEDAS, was validated as part of the PREDIMED trial in a 2011 study. 17 This study showed a significant correlation between MEDAS-derived PREDIMED and FFQ PREDIMED scores. Several years later a survey tool relating to Mediterranean nutritional knowledge, MDNK, was administered alongside MEDAS and validated first in university students then in adults at supermarkets and farmers markets, to create instruments applicable to the general US population. 18
Within the United States, studies have shown that racial and ethnic differences in dietary behavior exist, even after controlling for baseline sociodemographic differences. 28 Food preferences and dietary behaviors are a result of multiple factors, including cultural, lifestyle, socioeconomic, and demographic among others. At the individual level, these diet-related disparities can be addressed with more targeted and culturally appropriate dietary education and intervention programs. 29 Many targeted studies have shown that culturally relevant education has the potential to reach more patients and improve diet quality.30–33
Our intervention consisted of dietary counseling at the point-of-care during admission for acute ischemic stroke and discharge with a Mediterranean diet tailored for the southern US palate, which we called the Mediterranean Soul Food Diet (MSFD). We showed, in patients demographically representative of the Southeastern US, that it is feasible to implement a dietary intervention acutely in the hospital when using a culturally tailored dietary educational intervention. This was shown through a statistically significant increase in dietary adherence and nutritional knowledge at baseline compared to average follow-up scores. This was also associated with a significant decrease in weight, HbA1C, and TG levels. BMI, HbA1C, and TG are known risk factors for acute CVD events and mortality, including from stroke, and reduction of them is a known benefit of the Mediterranean diet. 34 Of note, these statistical differences occurred despite MEDAS scores at baseline and averaged follow-up in the low adherence range. It is suspected that this was a significant enough change from patient’s baseline diet to effect a positive change. To our knowledge this is the first study to show increasing Mediterranean diet nutritional knowledge and adherence borne out of a culturally tailored dietary counseling intervention at the point-of-care following an acute stroke.
Although scarce culturally tailored studies exist for vascular risk factors such as diabetes,35,36 to our knowledge this is the first culturally-cognizant dietary intervention study done in acute stroke in the Stroke Belt.
Limitations
As a feasibility study, there are numerous limitations. This study was started before the COVID-19 pandemic and had to be stopped early secondary to pandemic-related logistics difficulties. As a result, the sample size was small, which makes the generalizability of the results difficult to infer. The study length was 120 days and it is unknown if the observed effects would persist over a longer timeframe. As with many nutritional studies, although the scales used to determine nutritional knowledge and adherence to the Mediterranean diet are validated, they remain measures that are based on self-report with potential for bias from recall and social desirability. Lastly, the outcomes measured are all disease-oriented with benefits extrapolated from previous research.
Conclusion
This study showed that it was feasible to counsel patients with a culturally tailored diet while acutely hospitalized with a stroke. Moreover, it showed that this single dietary education affected vascular risk factors. Future studies including larger numbers of patients and evaluating dietary interventions in secondary stroke prevention as well as mitigation of stroke sequelae are needed.
Supplemental Material
Supplemental Material - The Mediterranean Soul Food Diet Intervention After Stroke, a Feasibility Study in the Stroke Belt
Supplemental Material for The Mediterranean Soul Food Diet Intervention After Stroke, a Feasibility Study in the Stroke Belt by Karima Benameur, Phillip Gross, Star Liu, and Sitara Koneru in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
We acknowledge the leadership of Nicole Franks, MD, CQO, EUHM, as well as the patients and their families, without whom this study would not have been possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Quality office of the Emory University Hospital Midtown (EUHM)
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.