
Abstract
We have developed, tested, and successfully implemented an affordable, evidence-based, technology-enabled, data-driven, outcomes-oriented, comprehensive lifestyle health coaching (LHC) program. The LHC program has been used primarily to provide services to employees of larger employers (ie, with at least 3000 employees) but has also been implemented in a variety of other settings, including hospitals, cardiac rehabilitation centers, physician practices, and as part of multicenter clinical trials. The program is delivered mainly using the telephone and Internet. Health coaches are guided by a Web-based participant management and tracking system. Lifestyle management interventions are based on several behavior change models and strategies, especially adult learning theory, social learning theory, the stages of change model, single concept learning theory, and motivational interviewing. The program is administered by nonphysician health professionals whose services are integrated with the care provided by participants’ physicians. Outcomes data from published studies, including randomized clinical trials and independent third-party conducted research, have documented the clinical effectiveness of this evidence-based approach in terms of modification of multiple risk factors in healthy persons as well as those with certain common chronic diseases.
‘The widespread failure of current medical practice to reflect the recent advances in knowledge of risk factors for chronic disease and their effective modification through lifestyle intervention undoubtedly results in avoidable death, disability, and human suffering.’
Introduction
Data from a variety of credible sources, including epidemiological, prospective cohort, and intervention studies, have shown that regular physical activity, correct nutrition, tobacco cessation, and a few other common lifestyle interventions can help mitigate the progression of many noncommunicable chronic diseases and, in certain instances, even reverse existing disease.1,2 Despite this overwhelming scientific evidence, potentially preventable lifestyle-related chronic diseases remain the leading causes of death, disability, and avoidable health care costs in Westernized society and are increasing dramatically in many developing nations.3-5
In particular, 3 lifestyle-related chronic diseases—cardiovascular disease (CVD), cancer, and type 2 diabetes—combine to make up approximately two-thirds of all deaths in the United States.4,5 Yet with the exception of cigarette smoking cessation, there is evidence that minimal, if any, improvement occurred in recent decades in key lifestyle practices related to the prevention of these and other potentially preventable chronic diseases. 2 Indeed, an increase has been reported in the prevalence of inappropriate caloric intake, obesity, and type 2 diabetes, and fewer than 1% of adult Americans currently exhibit ideal levels of cardiovascular health behaviors and factors based on 7 American Heart Association—defined metrics.4,5
Although sound clinical reasons exist for emphasizing lifestyle intervention in day-to-day medical practice and national clinical guidelines advocate a multifactorial lifestyle approach to chronic disease risk reduction, studies show that physicians often fail to provide adequate counseling on lifestyle management.2,6 This observation is not entirely unexpected, given that physicians generally work in an intensely busy environment; typically do not have the time, infrastructure, or resources to focus adequate attention on lifestyle management; and receive little or no compensation for the provision of such preventive services. In view of these and other well-documented barriers, it is not surprising that physicians in the United States generally tend to limit most of their attention to acute medical problems, give relatively low priority to preventive interventions, and when focusing on chronic disease risk reduction, prescribe pharmacological therapy in preference to lifestyle intervention. Regarding the latter, because of the widespread availability of many powerful and relatively safe medications, the value of lifestyle management per se in contemporary medical practice is often discounted by physicians, health insurers, and patients. 7
The widespread failure of current medical practice to reflect the recent advances in knowledge of risk factors for chronic disease and their effective modification through lifestyle intervention undoubtedly results in avoidable death, disability, and human suffering. 8 Moreover, this failure is believed to be an important contributing factor to rising health care costs, which, in turn, is a critical driving force behind the current unsustainable trajectory of the United States fiscal deficit. Clearly, this failure remains a frustrating impediment to fulfilling the potential for improving quality of life, productivity, and longevity through healthy lifestyles while simultaneously reducing avoidable health care expenditures.
The aging of the United States population, high prevalence of lifestyle-related chronic diseases and risk factors for chronic disease, and rising cost of health care in the United States provide a sense of urgency and immediacy for finding innovative solutions aimed at helping individuals make and adhere to meaningful lifestyle changes. In recent years, a variety of innovative approaches to lifestyle intervention have been successfully implemented in a variety of clinical and nonclinical settings. 9 These approaches span a broad spectrum, ranging from physician-supervised/nurse case-managed interventions to interactive Web-based programs and mobile apps. Likewise, the settings in which these newer interventions have been implemented range from hospital-based settings to the workplace. Regarding the latter, the current unprecedented interest in workplace lifestyle management programs in the United States stems in part from the recognition that more than 60% of Americans obtain their health insurance coverage through employment-based plans and the fact that most employees spend the majority of their time at work.2,10
In this article, we describe the key features of an affordable, evidence-based, technology-enabled, data-driven, outcomes-oriented, comprehensive lifestyle health coaching (LHC) program that we have successfully implemented in the workplace and other clinical and nonclinical settings. We also summarize outcomes data from key published scientific abstracts and manuscripts on the LHC program’s clinical effectiveness in healthy persons as well as those with certain common chronic diseases.
Core Components of an Evidence-Based LHC Program
We have spent over 2 decades developing, testing and implementing evidence-based LHC programs.11-13 As recommended by expert professional groups, we based our initial program development efforts on models shown to be effective in randomized clinical trials. Of the various studies completed at that time, we considered the Stanford Coronary Risk Intervention Project (SCRIP) to be of particular relevance because it utilized what appeared to be the most logical approach to lifestyle management and chronic disease risk reduction—namely, intensive modification of multiple risk factors via comprehensive lifestyle interventions combined with appropriate pharmacotherapy. 14 In SCRIP, the multifactor risk reduction program resulted in a 47% lower rate of narrowing of diseased coronary artery segments and reduced hospitalization for clinical cardiac events by 39% versus usual care during the 4-year study period. Although the initial focus of our lifestyle management programs was exclusively on CVD risk reduction, the programs have evolved considerably over time and now successfully target multiple risk factors and potentially preventable chronic diseases.
Briefly, the content of our lifestyle management program is organized into 2 core sets of services. One set is coach assisted, involving one-on-one counseling of participants by a nonphysician health professional and is referred to as a LHC program. The other set is an array of individualized self-help programs, all of which are Web enabled. Whereas the LHC program is comprehensive in nature, in that it targets multiple behaviors and risk factors in an integrated fashion, the self-help programs generally target a single major behavior (eg, exercise training/physical activity, correct nutrition, weight management, tobacco cessation, or stress management). Our comprehensive LHC program is the focus of the remainder of this article.
Currently, our LHC program is delivered mainly in the United States and Canada using the telephone and Internet and has been used primarily to provide services to employees of larger employers (ie, with at least 3000 employees), including multinational corporations with employees in multiple countries. However, over the years, the program has also been successfully implemented in a variety of other settings, including hospitals, cardiac rehabilitation centers, physician practices, and even health clubs, shopping malls, and other retail settings. Most recently, the LHC program has been modified for use in collaboration with the American College of Cardiology’s CardioSmart patient-centered care initiative and as part of 2 multicenter, randomized clinical trials funded by the National Institutes of Health. In each of the different settings, the program content has been adapted to enhance the applicability to the specific settings and, where appropriate, clinical and cultural circumstances. From a global perspective, many adaptations have been made to facilitate culturally appropriate service provision in multiple countries and languages, including English (several variations), French (Canadian), Spanish, Portuguese (Brazil), Portuguese (European-Angolan), and Thai.
The primary specific objectives of our LHC program are to help participants with the following: (1) make and adhere to meaningful, evidence-based lifestyle changes (eg, regular exercise/physical activity, healthy nutrition, weight management, stress management, tobacco avoidance, and appropriate sleep hygiene/fatigue risk management); (2) address gaps in their preventive care (eg, compliance with recommended preventive screenings, tests, and immunizations); (3) learn about their specific risk factors for chronic diseases and known chronic medical conditions; and (4) comply with prescribed medications. To accomplish these objectives and help ensure the attainment of clinically meaningful and reproducible outcomes, our LHC program is delivered using a formal, structured, systematic approach together with rigorous quality assurance protocols. The core components of our LHC program and key steps typically involved in their delivery to employees in a workplace setting are described in what follows.
Step 1: Participant Identification, Risk Stratification, and Enrollment
In the workplace setting, employers have often paid for and provided financial incentives for their employees and, in some instances, their spouses and adult dependents to participate in the LHC program. Following completion of appropriate preprogram launch activities, potential participants are identified primarily through the use of a health risk assessment (HRA). After the provision of informed consent by each individual, HRAs are typically completed online via a secure Web site that serves as the primary point of entry to the HRA and other useful resources (such as wellness-related incentives, challenges, and educational content). The HRA can also be completed telephonically or in hard copy (“pen and paper”) format. In addition to the use of HRAs, potential participants may be identified using medical and pharmacy claims data and can also be self-referred to the LHC program or referred via a variety of other channels, including onsite biometric screenings, disease management programs, disability management programs, and physicians/other health care providers.
The baseline HRA is used to provide individuals with basic awareness and education information on their risk for potentially preventable chronic diseases, the specific factors placing them at risk, and the actions they can take to mitigate their risk, with a focus on lifestyle management. The HRA is also used to evaluate and stratify individuals for triage to LHC programs involving different intensities of intervention. In this respect, a 2-level HRA stratification process is typically used. First, an industry-standard, population level 1 stratification categorizes individuals into 3 levels of risk for future direct and indirect health care–related expenditures (also referred to as health risk stratification) as follows: 0 to 2 risk factors, lower risk; 3 to 4 risk factors, moderate risk; and 5 or more risk factors, higher risk. 15 Second, to determine the most appropriate intensity of intervention needed to optimize risk reduction in accordance with principles of evidence-based medicine, the stratification status of individuals who fall into the lower and moderate health risk stratification categories is further refined using proprietary unpublished algorithms that consider a variety of additional factors, including severity of individual risk factors, presence of other risk factors, behavioral versus nonmodifiable risk factors, and the difficulty associated with modifying specific risk factors. This level-2 stratification categorizes individuals into 3 levels of intervention (also referred to as “intervention intensity stratification”) as follows: lower-, moderate-, and higher-intensity intervention.
Immediately on completing the online HRA, participants are able to enroll in the LHC program and schedule their first appointment using an online enrollment tool. Participants may also contact the program via secure online chat, e-mail, or telephone to obtain additional information prior to enrollment and subsequently enroll in the LHC program via the telephone. For individuals who do not enroll online and who do not contact the program, a formal outreach process involving use of the postal mail, e-mail, text messaging, and/or telephone is utilized in an attempt to optimize enrollment. On program enrollment, each participant is assigned to an appropriately trained nonphysician health professional who serves as the participant’s dedicated health coach.
Health coaches are supervised by a director of health coaching who reports directly to the LHC program’s medical director. All health coaches have a minimum of a 4-year college degree in a health-related area and at least 2 years of relevant work experience. Coaches include health educators, nurses, dietitians/nutritionists, exercise scientists, and other health professionals. Newly hired coaches receive approximately 160 hours of structured, competency-based training prior to engaging with participants. Ongoing training occurs during weekly staff meetings. Coaching calls are recorded and monitored for quality assurance and training purposes. Specialized in-depth training for the health coaches is also conducted as new program materials and processes are introduced.
Step 2: Initial/Intake Assessment
The HRA typically forms the basis of the intake or initial assessment and evaluates factors such as past and current medical history, risk factors for chronic disease, medications, current lifestyle practices, self-reported health status, productivity (including absenteeism and presenteeism), psychosocial status, preventive screenings and immunizations, safety practices, readiness for change, biometric measurements (such as height, weight, waist circumference, resting blood pressure, fasting serum lipids and lipoproteins, fasting glucose, and A1C), and other relevant information. Participants who have already completed the HRA prior to enrollment in the LHC program are asked to review and, where appropriate, update their HRA. To facilitate the provision of evidence-based and clinically-responsible LHC, participants who have not previously completed the HRA (eg, participants referred to the program through one of the above-mentioned alternative referral channels) are required to complete the HRA or another similar intake assessment prior to the initiation of LHC.
Step 3: Goal Setting
Based on the initial assessment, computer-generated, individualized, short- and long-term goals are set for multiple risk factors (including weight, systolic and diastolic blood pressure, serum lipids and lipoproteins, fasting glucose, and A1C), health behaviors (including physical activity/exercise training, nutrition, stress, tobacco use, and sleep hygiene), and risk scores (including the Framingham 10-year coronary heart disease risk score and other atherosclerotic CVD risk scores) in accordance with clinical guidelines published by credible expert groups (eg, in the United States, the American College of Cardiology, American College of Sports Medicine, American Diabetes Association, American Heart Association, Centers for Disease Control and Prevention, National Institutes of Health, Obesity Society, and US Preventive Services Task Force). In addition to the computer-generated, guideline-based goals, health coaches help each participant formulate key, specific action-based, realistic, and time-line driven goals that the participant wants to accomplish.
Step 4: Action Plan Formulation
Based on the initial assessment, a computer-generated, individualized action plan is formulated to help each participant achieve the short- and long-term goals. The action plan focuses on important lifestyle practices (especially physical activity/exercise training, correct nutrition, weight management, tobacco cessation, and stress management). In addition to behavior modification, the action plan identifies the need for specific preventive screenings, immunizations, other self-care activities, and physician referrals—for example, for consideration of new medications and/or changes in prescription medications to optimize the management of common chronic conditions such as hypertension, hyperlipidemia, and diabetes, consistent with expert clinical guidelines.
Step 5: Review/Revision of Goals and Action Plan
Based on their interaction with the participant and/or input from the participant’s physician or other health care providers, health coaches have the ability to revise the computer-generated, guideline-based goals and action plans but are required to document the rationale for any such changes in the computer database. Typically, participants access their goals and action plan reports via the Internet, but in some instances, reports are mailed to participants. Reports are accompanied by an audio explanation, which can be accessed online. Health coaches review goals and action plans with participants and, when doing so, are guided by both the program database and written instructions, referred to as coaching prompt sheets (or lesson plans). If the action plan includes referral to a physician or other health care provider, the health coach emphasizes the importance of this and subsequently documents the outcome of the referral in the program database. Letters may be mailed, faxed, or transmitted via secure e-mail to physicians notifying them of their patients’ participation in the program.
Step 6: Action Plan Implementation
With guidance from the program’s Web-based participant management database, health coaches assist participants in implementing their individualized action plans over the course of each program year. Coaching occurs during proactive, formally structured, one-on-one counseling sessions conducted via brief (usually ~15 minutes in duration) prescheduled telephone appointments and, if the participant prefers, via secure online chat or e-mail.
Coaching is conducted using behavioral interventions derived from several well-established behavior change models and strategies—primarily adult learning theory, social learning theory, motivational interviewing, and the stages of change model. Materials and messages are matched with the participant’s stage of readiness for change for each health behavior. Cognitive and behavioral processes are emphasized to varying extents in different ways depending on the participant’s stage of readiness for change. Cognitive processes include increasing knowledge, comprehending benefits of changing a behavior, warning of risks and consequences of not changing, and empowering the participant to take action based on internal motivation. Participants engage in numerous self-assessment and self-monitoring activities, including weighing the pros and cons of changing, keeping online exercise and food diaries, completing stress and smoking logs, and assessing self-efficacy. Behavioral processes include counter-conditioning, enlisting social support, using incentives and rewards (including the ability for participants to track their specific incentives/rewards online), controlling stimuli, and building confidence. Because participants are continually at risk for relapse, emphasis is given to planning for high-risk situations and dealing with and learning from slips.
Typically, only 1 major concept or skill is introduced at a time (ie, single concept learning theory) in a relatively easy-to-understand and carefully sequenced way. This approach is facilitated by the use of an individualized series of behavior change and education modules. The written and audio versions of each module can be accessed via the Internet and via “hard copy” format. The modules incorporate many of the above-mentioned behavior change models and strategies.
The precise number of telephonic LHC sessions scheduled for each participant is based primarily on the participant’s intervention intensity stratification status. Generally, during the first year of program participation, lower-intensity-intervention participants are preassigned to receive 4 coaching sessions, moderate-intensity-intervention participants 9 coaching sessions, and higher-intensity-intervention participants 12 to 18 coaching sessions. Coaching schedules are front loaded, so that 50% or more of the assigned coaching sessions occur approximately within the first 12 weeks of intervention in order to better support behavior change. It is possible for a participant to complete additional coaching sessions if the participant requests to do so and the health coach believes that the participant could benefit from the additional LHC.
The appropriateness of our coaching schedules is supported both by our unpublished research on the dose-response relationship between the total number of completed telephonic LHC sessions and the reduction in the number of health risks and by published outcomes data documenting the clinical effectiveness of our LHC program (Table 1). However, additional research is needed to clarify the optimal number, frequency, and duration of coaching sessions, both from a cost and effectiveness perspective.
Case Study: Outcomes Data from Select Published Scientific Manuscripts on the Clinical Effectiveness of the LHC Program.
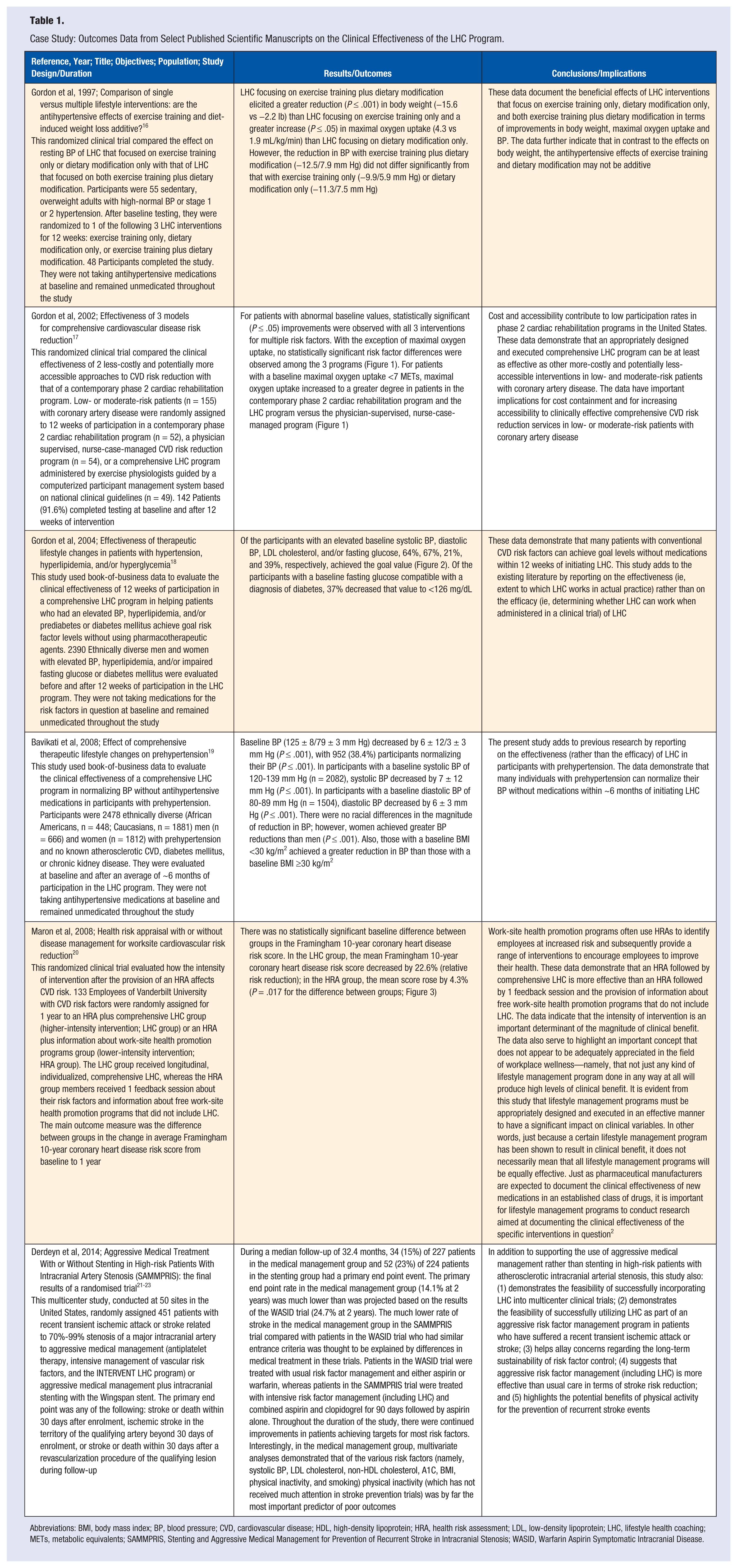
Abbreviations: BMI, body mass index; BP, blood pressure; CVD, cardiovascular disease; HDL, high-density lipoprotein; HRA, health risk assessment; LDL, low-density lipoprotein; LHC, lifestyle health coaching; METs, metabolic equivalents; SAMMPRIS, Stenting and Aggressive Medical Management for Prevention of Recurrent Stroke in Intracranial Stenosis; WASID, Warfarin Aspirin Symptomatic Intracranial Disease.
Step 7: Follow-up Assessment
After ~12 weeks and 1 year of program participation, and at least annually thereafter, participants complete a formal follow-up assessment. In addition to the follow-up assessment, participants typically retake the HRA on an annual basis.
Step 8: Progress Reports and Revision of Goals/Action Plan
Based on program participation and the follow-up assessments or repeat HRAs, participants are provided computer-generated reports documenting their progress and updating their goals/action plans. Progress reports are reviewed at LHC sessions. As with the initial goals and action plan reports, if the revised action plan includes referral to a physician or other health care provider, the health coach emphasizes the importance of this and subsequently documents the outcome of the referral in the program database. Letters may be sent to physicians notifying them of their patients’ progress in the program.
Step 9: Maintenance
Participants usually enroll in the program for 1 year at a time but have access to continuing years of ongoing LHC or self-help programs. Compliance with scheduled LHC sessions and interventions is tracked using the program’s Web-enabled participant management and tracking database.
Step 10: Outcomes Assessment
Detailed aggregate outcomes reports are generated on a regular basis for specific employers and other groups of program participants. Benchmarking may be included using book-of-business analyses.
As stated earlier, the core components and key steps of the LHC program have been adapted for cost-effective implementation in many other settings. For example, in physician referral settings, physicians may refer patients using a variety of modalities, including a mobile app; track the outcome of referrals online and via the mobile app; access goals, action plan, and progress reports generated for their patients via a secure online portal; provide input to health coaches for their patients via the portal; and receive aggregate outcomes reports (including participant satisfaction reports) for their patients.
Clinical Effectiveness of the LHC Program: Modification of Multiple Risk Factors
Our LHC program is based on models shown to be effective in randomized clinical trials and is conducted in accordance with published national and international clinical guidelines, where appropriate. In addition, the effect of our specific LHC program on multiple risk factors has been carefully evaluated in randomized clinical trials, including independent third-party conducted studies, as well as by analyzing our book-of-business data as part of formal research initiatives. Outcomes data from the key published peer-reviewed manuscripts on the clinical effectiveness of our LHC program in healthy persons as well as those with multiple risk factors are summarized in chronological order (based on year of publication) in Table 1 and Figures 1 to 3.16-23 Collectively, these studies and our other published research (including scientific abstracts)24-52 show that our LHC program accomplishes the following:
(a) It helps participants favorably modify multiple behaviors (including exercise training/physical activity, nutrition, and tobacco use).16,24
(b) It results in clinically relevant improvements in multiple biomarker risk factors (including systolic and diastolic blood pressure, total cholesterol, LDL cholesterol, HDL cholesterol, triglycerides, fasting glucose, body weight, body mass index, waist circumference, and cardiorespiratory fitness) in diverse populations. These populations include male and female patients,25-28 African Americans and Caucasians,19,29-31 educated and less-well-educated participants, 32 and apparently healthy participants as well as those with a variety of chronic medical conditions (including overweight/obesity,33,34 prediabetes/diabetes,18,25,35-37 prehypertension/hypertension,18,19 the metabolic syndrome,38,39 hyperlipidemia,18,40,41 coronary artery disease,17,42 stroke/TIA/carotid artery disease,21-23,29,43-45 arthritis, 46 and cancer 47 ).
(c) It can be of significant benefit in helping control elevated blood pressure, hyperlipidemia, and hyperglycemia in many individuals through lifestyle intervention alone (ie, can help reduce the need for drug therapy and thereby be of benefit from a cost-containment perspective).16,18,19
(d) It is more accessible than and at least as effective, in terms of modification of multiple risk factors, as a traditional phase 2 cardiac rehabilitation program (an accepted standard of care) and a physician-supervised/nurse case-managed program in patients with coronary artery disease, despite its substantially lower cost.17,48
(e) It is more effective, in terms of CVD risk reduction, than a less-intensive approach to workplace health promotion that does not involve ongoing and carefully structured LHC. As emphasized in Table 1, not all lifestyle management programs result in meaningful clinical benefits, and therefore, emphasis should be placed on the use of LHC programs that have specifically been proven effective in peer-reviewed published clinical trials.2,20
(f) It elicits clinically relevant and reproducible improvements in multiple risk factors when administered by the clinical staff of licensee institutions in multiple geographic locations. 49
(g) It is at least as effective when administered remotely from a call center using the telephone and the Internet as compared with onsite, face-to-face, program delivery. 50
(h) It is clinically effective when administered via telephone and the Internet to adults living in rural communities. 51
(i) It results in a favorable population shift from higher to lower health-risk stratification levels when administered to employees, with a significant dose-response relationship between the total number of completed telephonic LHC sessions and reduction in the number of health risks. 52
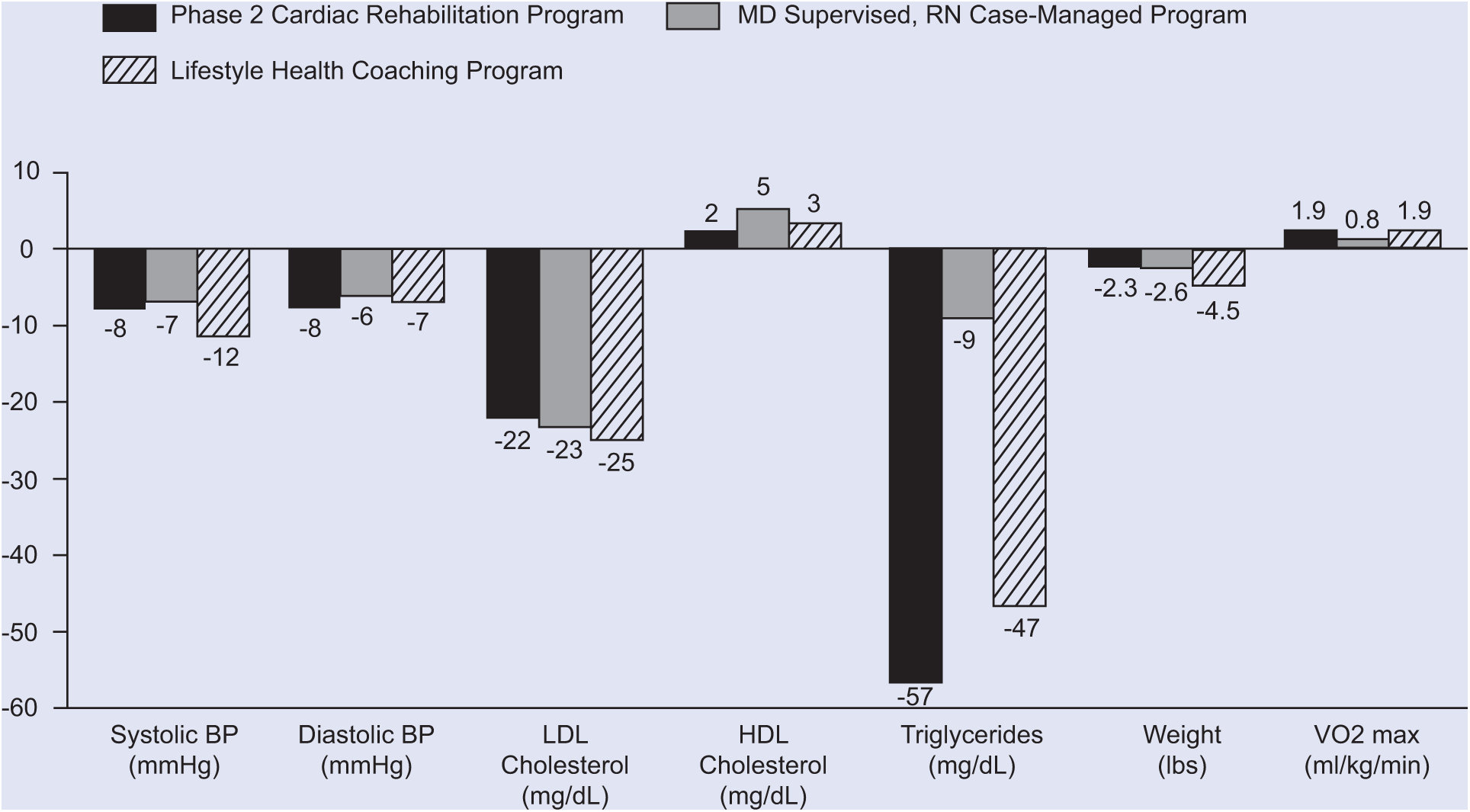
Comparative effectiveness of 3 models for comprehensive cardiovascular disease risk reduction: changes in clinical outcome measures after 12 weeks of intervention in individuals with abnormal baseline values (n = 142). Changes from baseline were statistically significant (P ≤ .05) except for HDL cholesterol (all 3 programs) and triglycerides (MD supervised, RN case-managed program). Differences among programs were statistically significant as follows: change in VO2max was greater with the phase 2 cardiac rehabilitation program and lifestyle health coaching program versus MD supervised, RN case-managed program (P ≤ .05). See Table 1 and Gordon et al. 17
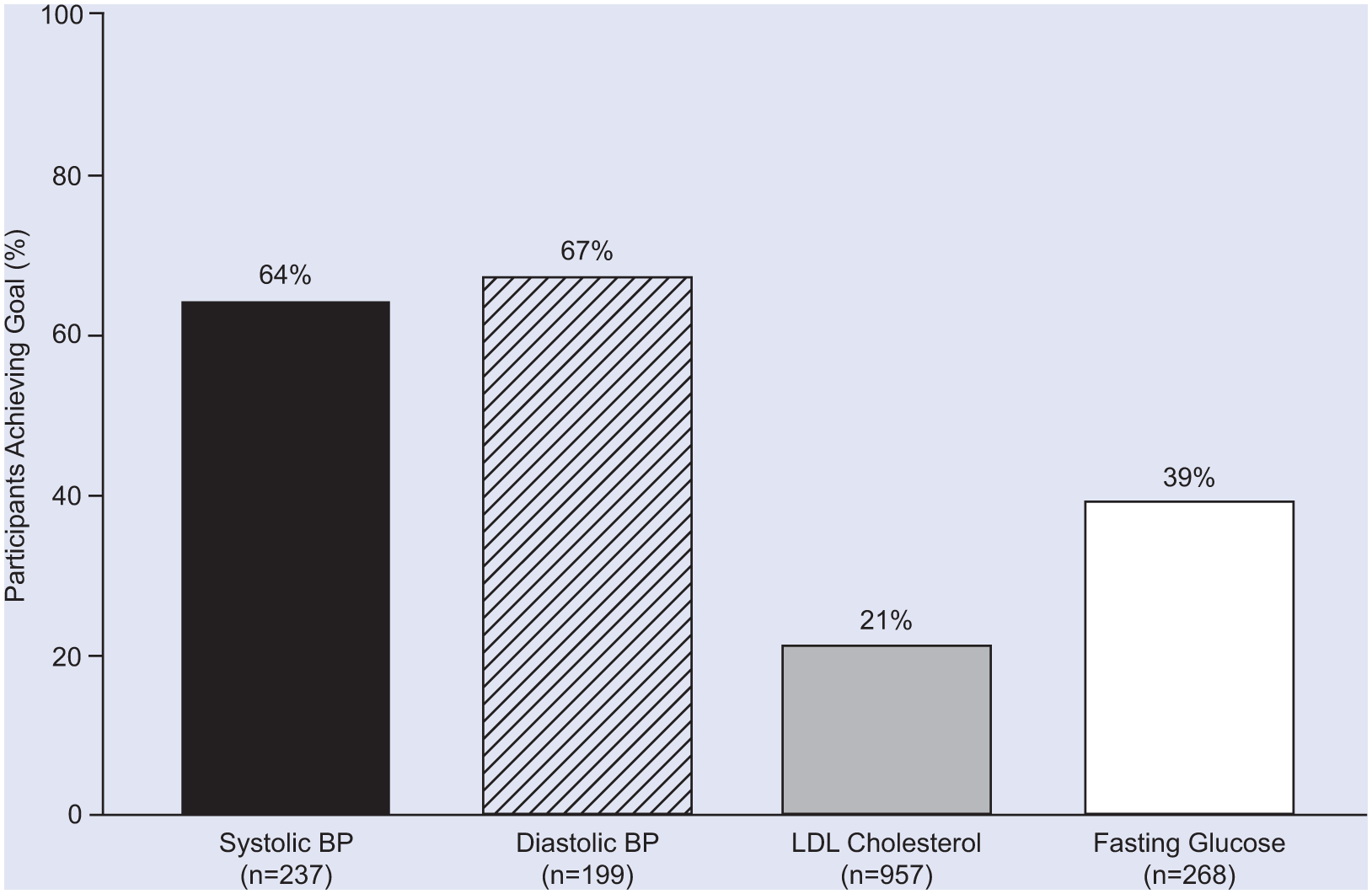
Effect of 12 weeks of lifestyle health coaching on control of systolic and diastolic BP in participants not taking antihypertensive medications, fasting glucose in those not taking antidiabetic medications, and LDL cholesterol in those not taking antilipidemic medications: percentage of participants with abnormal baseline values who achieved the goal level. See Table 1 and Gordon et al. 18
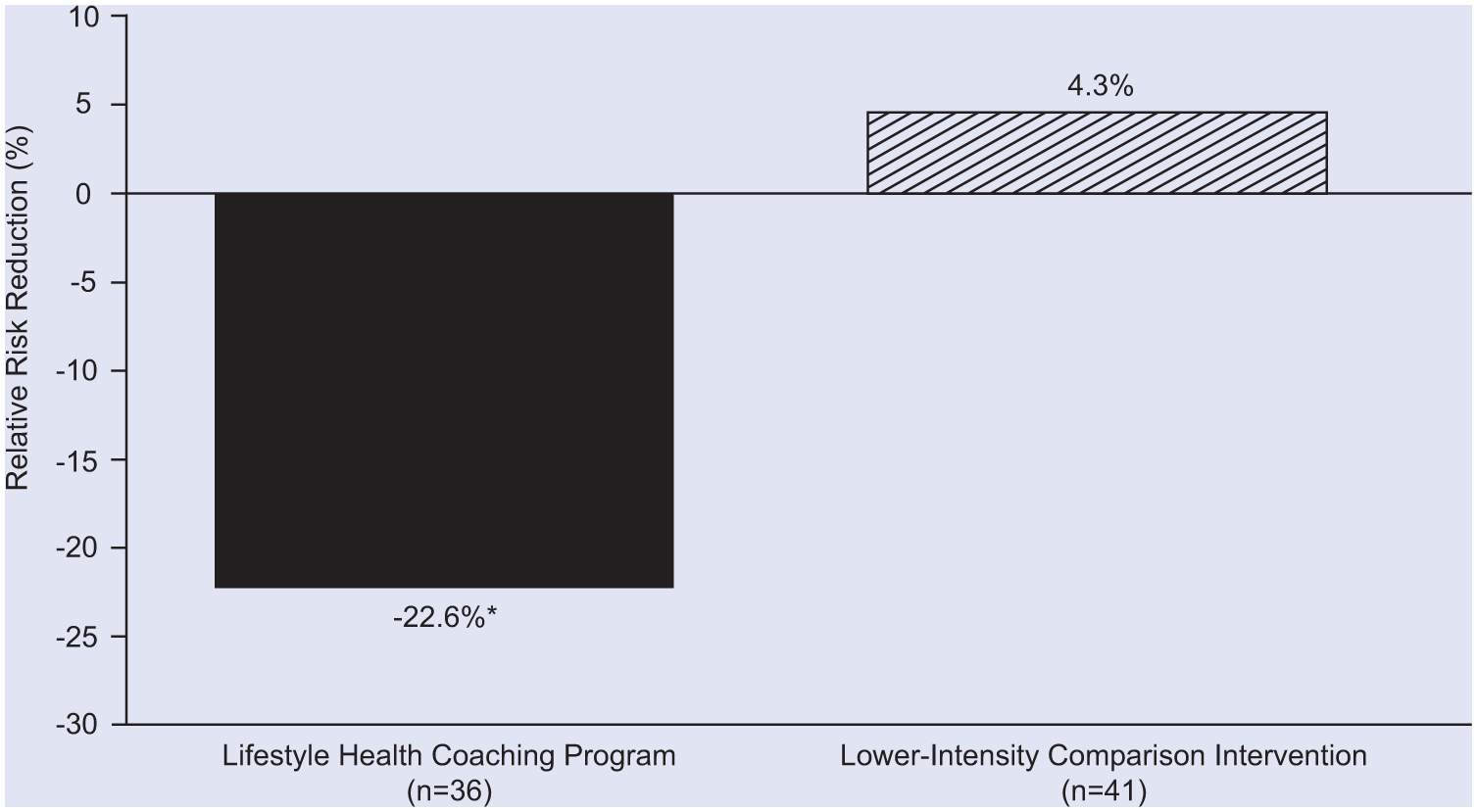
Clinical effectiveness of a lifestyle health coaching program versus a lower-intensity comparison intervention: percentage change (relative risk reduction) in Framingham 10-year coronary heart disease risk score. *P = .017 for lifestyle health coaching program versus lower-intensity comparison intervention. See Table 1 and Maron et al. 20
In addition to data on clinical effectiveness, and although not the focus of this article, our data document high participant satisfaction levels53,54 and the beneficial effect of our LHC program on multiple indices of quality of life. 55 Although further research is warranted, our data also suggest that our LHC program may favorably affect employee health care claims and productivity and that the above-mentioned clinical benefits are sustained over multiple years.13,23
Conclusion
In conclusion, we have developed, tested, and successfully implemented an affordable, evidence-based, technology-enabled, data-driven, outcomes-oriented, comprehensive LHC program. The program has been used primarily to provide LHC to employees of larger employers but has also been implemented in a variety of other clinical and nonclinical settings. Outcomes data from numerous published studies and scientific abstracts, including randomized clinical trials and independent third-party conducted research, have documented the clinical effectiveness of this evidence-based approach in terms of modification of multiple risk factors in healthy persons as well as those with certain common chronic diseases. On the basis of our outcomes data, it is evident that appropriately designed and implemented LHC programs constitute an important component of the armamentarium of interventions that can be used in the global “war” against potentially preventable noncommunicable chronic diseases. In the future, we and others anticipate that evidence-based LHC programs that have been proven effective in peer-reviewed published clinical trials will not only be deployed with increased frequency as part of employer-sponsored wellness initiatives but will also become a standard of care in daily clinical practice.2,56,57
Footnotes
Authors’ Note
Dr Gordon, Dr Salmon, Dr Wright, Mr Faircloth, and Mr Reid are members and Ms Gordon is an employee of a population health management company (INTERVENT International, LLC).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Gordon, Dr. Salmon, Dr. Wright, Mr. Faircloth and Mr. Reid are members of and Ms. Gordon is an employee of a population health management company (INTERVENT International, LLC).