
Abstract
Heart failure with preserved ejection fraction (HFpEF) is a complex clinical syndrome that constitutes nearly half of all heart failure cases. Because of lack of effective pharmacological targets to improve outcomes, the emphasis of the management and prevention of HFpEF should be through control of risk factors. This review will use the framework proposed by the American Heart Association on 7 simple measures (“Life’s Simple 7”) that involves diet and lifestyle changes to achieve ideal cardiovascular health. These 7 measures include (1) smoking, (2) obesity, (3) exercise, (4) diet, (5) blood pressure, (6) cholesterol, and (7) glucose control, which can help control the most common comorbidities and risk factors associated with HFpEF, such as hypertension, diabetes, and obesity. Therefore, application of these 7 simple measures would be a patient-centered and cost-effective way of prevention and management of HFpEF.
‘Several large clinical trials conducted over the past decade have shown that pharmacological interventions can dramatically reduce the morbidity and mortality associated with HFrEF . . .’
Introduction
Heart failure is a major health problem that affects patients and health care systems worldwide. Statistics have shown that heart failure affects approximately 5.1 million patients in the United States and more than 23 million patients worldwide.1,2 There are 2 main types of heart failure: heart failure with reduced ejection fraction (HFrEF) and heart failure with preserved ejection fraction (HFpEF).1,2 More than 650 000 new patients are diagnosed with heart failure in the United States each year, and at least half of them have HFpEF.1,3,4
Heart failure can be diagnosed by clinical signs or symptoms of fluid overload, low cardiac output, or both. In contrast to HFrEF, which is easily diagnosed by the presence of clinical signs or symptoms of heart failure and a left-ventricular (LV) ejection fraction (EF) ≤40%, 4 the diagnosis of HFpEF is controversial. In addition to the American Heart Association (AHA)/American College of Cardiology heart failure guideline requirements of signs or symptoms of heart failure and an LVEF ≥50%, 1 the European Society of Cardiology guidelines have more strict criteria for HFpEF diagnosis. They also require the presence of (1) elevated levels of serum natriuretic peptides and (2) documentation of either left-ventricular hypertrophy, left-atrial enlargement, or diastolic dysfunction. 2 Currently, evidence of diastolic dysfunction can be easily derived either from cardiac catheterization or tissue Doppler imaging. 5
Several large clinical trials conducted over the past decade have shown that pharmacological interventions can dramatically reduce the morbidity and mortality associated with HFrEF1,2,4; however, many effective treatments for HFrEF have shown disappointing results when applied to HFpEF patients (Table 1). To date, there is no definitive evidence of pharmacological therapies that have shown reduced morbidity or mortality in HFpEF. 3 The mainstay of pharmacological treatment is diuretics to control volume status and symptoms, with little data to support long-term outcomes.1,2 In view of a lack of proven effective pharmacological therapies that can improve morbidity or survival in patients with HFpEF, prevention remains the best approach to reduce its burden. 6 Therefore, the cornerstone of HFpEF management is implementation of healthy lifestyle measures for primary and secondary prevention.
Randomized Controlled Trials of Pharmacological Therapy for Heart Failure and Preserved Ejection Fraction. a
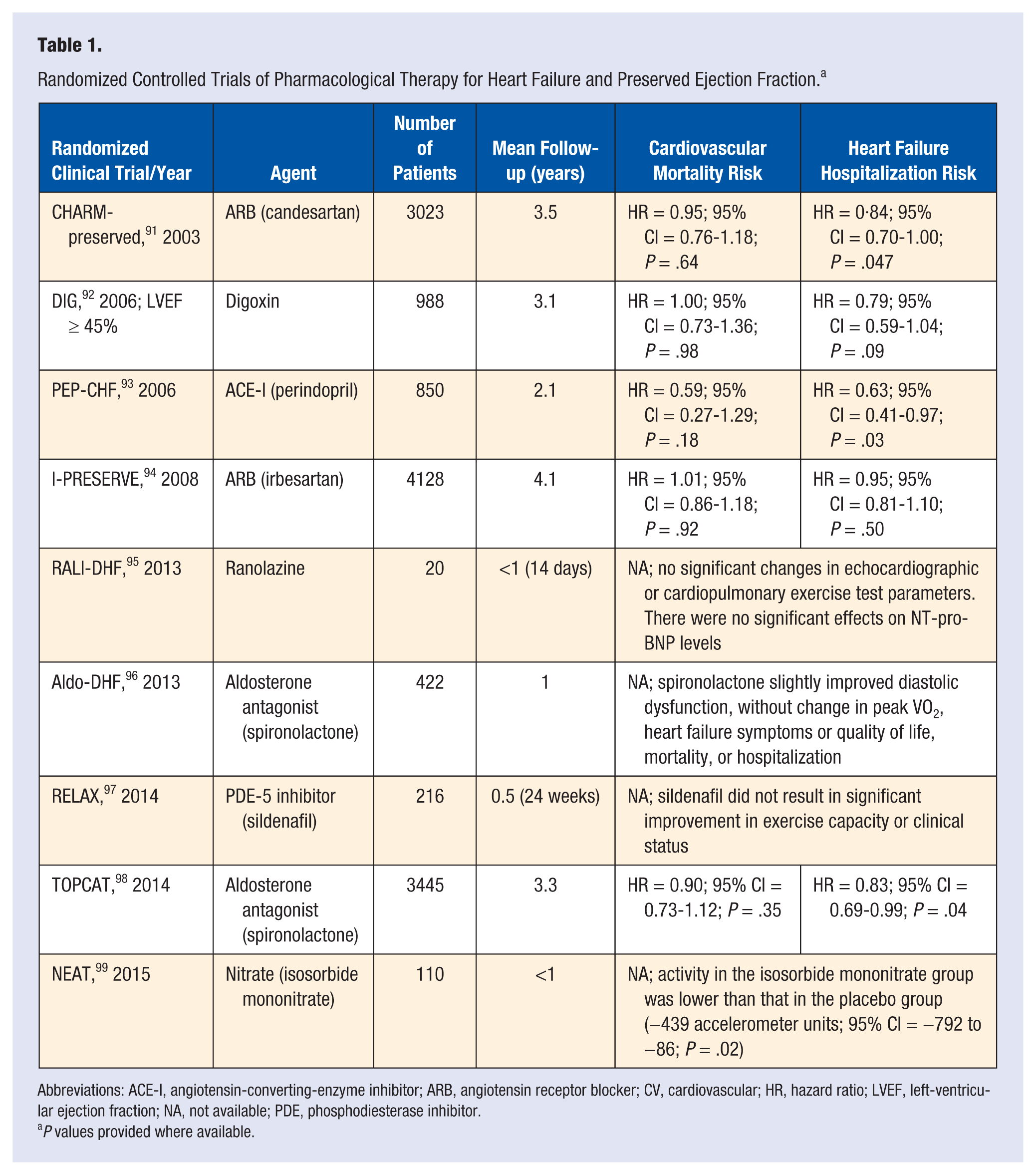
Abbreviations: ACE-I, angiotensin-converting-enzyme inhibitor; ARB, angiotensin receptor blocker; CV, cardiovascular; HR, hazard ratio; LVEF, left-ventricular ejection fraction; NA, not available; PDE, phosphodiesterase inhibitor.
P values provided where available.
In 2010, the AHA used 7 criteria to define ideal cardiovascular health to put emphasis on diet and lifestyle factors to work toward the AHA’s 2-pronged national goals of (1) improving the cardiovascular health of all Americans by 20% by 2020 and (2) reducing deaths from cardiovascular diseases and stroke by 20% by 2020. 7 A campaign was launched in January 2016, by the AHA, to link the tenets of ideal cardiovascular health to 7 simple measures (“Life’s Simple 7”) that people can influence through diet and lifestyle changes to move from poor and intermediate to ideal health. The 7 measures identified include (1) smoking, (2) obesity, (3) exercise, (4) diet, (5) blood pressure, (6) cholesterol, and (7) glucose control.
This review article will focus on how the proposed 7 risk factors and lifestyle changes can help prevent and manage HFpEF.
Stop Smoking
Cigarette smoking is one of the leading risk factors for cardiovascular disease. 7 Smoking harms nearly every organ in the human body, including the cardiovascular system. The incidence of a myocardial infarction is increased 6-fold in women and 3-fold in men who smoke at least 20 cigarettes per day compared with nonsmokers. 8 A recent meta-analysis of 89 prospective studies showed that smoking is associated with an approximately 50% increased risk for total mortality and cardiovascular events. 9 In fact, active cigarette smokers had a 49% higher risk of developing heart failure than nonsmokers (Risk Ratio [RR] = 1.49; 95% CI = 1.30-1.70) in the NHANES-I Epidemiologic Follow-up study. 10 Smoking appears to increase inflammation, thereby promoting atherosclerosis; however, the increased risk of heart failure remains significant after adjusting for inflammatory markers, suggesting an independent effect of cigarette smoking on the incidence of heart failure. 11
Cigarette smoking can result in significant acute diastolic dysfunction in the left ventricle. 8 For patients with LV dysfunction, active smoking was an independent predictor of recurrent heart failure, myocardial infarction, and mortality. 12 In contrast, smoking cessation was related to a decrease in morbidity and mortality in patients with LV dysfunction within 2 years of quitting, which is of similar magnitude as proven drug treatments in this population, such as angiotensin-converting-enzyme inhibitors. 12
Although there are no randomized controlled trials to show definitive causation between smoking cessation and heart failure prevention, many of the cardiovascular risks associated with smoking can be reversed by quitting. 7 In addition, numerous studies have shown that smoking-related cardiovascular comorbidities that may cause or worsen heart failure, such as ischemic heart disease and peripheral arterial disease, are both highly prevalent in both HFpEF and HFrEF.12,13 This is especially important when the prevalence of ischemic heart disease (including previous myocardial infarction, angina, and revascularization) is present in 20% to 59% of HFpEF patients. 13 Given the association between smoking and diastolic dysfunction, and the worsening of comorbid conditions in patients with HFpEF, smoking cessation can potentially be one of the most cost-effective means to improve cardiovascular health of patients with HFpEF.
Lose Weight
Overweight and obesity are known risk factors for the development of heart failure,10,14 heart failure hospitalizations, 15 and heart failure mortality. 14 An analysis of 5881 participants in the Framingham Heart Study demonstrated a 2-fold increase in the risk for heart failure (HR = 2.04; 95% CI = 1.59-2.63) in obese individuals (body mass index [BMI] ≥ 30 kg/m2) compared with normal-weight (BMI = 18.5-24.9 kg/m2) participants. 10 Campbell and McMurray, 13 in a review, found a much higher prevalence of obesity in HFpEF, in any setting, than in patients with HFrEF. Obesity can cause several symptoms found in HFpEF—namely, fatigue, dyspnea, and ankle swelling. 13 Obesity is also known to cause obstructive sleep apnea, a comorbidity and risk factor frequently found in HFpEF, along with hypertension, LV hypertrophy, diastolic dysfunction, renal impairment, and atrial fibrillation.13,16
The association between obesity and heart failure can be better understood by investigating the mechanisms. Adiposity has been associated with increased concentrations of proinflammatory cytokines, such as tumor necrosis factor-α, interleukin-6, and C-reactive protein (a marker of systemic inflammation), all of which have been associated with an increased risk of heart failure. 14 Excess weight has also been associated with altered LV and right-ventricular remodeling, possibly as a result of increased hemodynamic load, neurohormonal activation, and increased oxidative stress. 11 Both animal and human studies have shown that obesity increases cardiac steatosis and lipoapoptosis.17-19
Although there are no randomized controlled trials to show causation between weight loss and heart failure prevention, observational studies have shown that several structural abnormalities in the left and right heart are reversed after weight loss, through bariatric surgery20,21 and/or dietary changes. 22 Indeed, large cohort studies have shown that weight loss improves HFpEF risk factors such as LV or right-ventricular hypertrophy, diastolic dysfunction, and aortic stiffness.22,23 Consequently, maintaining a normal weight is another vital lifestyle modification that can help manage and prevent HFpEF.
Get Active
Observational studies have related lower levels of cardiorespiratory fitness with a greater risk of heart failure,6,24 a phenomenon potentially mediated through a greater degree of diastolic dysfunction and LV remodeling among individuals with lower fitness levels,6,25 among other factors.
Exercise training has been shown to benefit cardiorespiratory health in patients with HFrEF.26 -29 Recent studies have started to address the biological effects of exercise training in patients with HFpEF.30 -32 A 16-week randomized controlled trial of supervised exercise training in patients with HFpEF showed that the peak exercise oxygen uptake was significantly improved in the exercise cohort as compared with the controls, although a significant improvement in the LVEF was not seen. 31 Another small randomized controlled study showed that physical exercise with weight reduction reduced blood pressure, decreased cardiovascular risk factors, and improved diastolic dysfunction. 33 Therefore, despite a paucity of randomized controlled trials that showed reduction in mortality or hospitalization related to exercise training in HFpEF, engaging in regular physical activity appeared to improve pathological pathways that might lead to HFpEF; hence, it is another important lifestyle approach to the management and prevention of HFpEF.
Eat Better
Eating healthy diets, specifically focusing on controlled salt intake with the Dietary Approaches to Stop Hypertension (DASH) diet is another intervention to consider in HFpEF management. 34 Hummel et al36 investigated the physiological effects of dietary modification in patients with hypertension and HFpEF. In their study, 13 hypertensive HFpEF patients were provided a combination of a sodium-restricted diet and the DASH diet (rich in potassium, magnesium, calcium, and antioxidants). 35 The combination of the DASH diet and a sodium-restricted diet significantly reduced blood pressure and arterial stiffness and led to improvement in dyspnea and exercise capacity after just 3 weeks. 36 In another study by Hummel et al, 34 the combined DASH and sodium-restricted diets were associated with improved LV diastolic function and reduced arterial stiffness in hypertensive patients with HFpEF.
Other nutritional therapies, such as magnesium, may improve pathological pathways commonly shared by both diabetes and HFpEF, which include insulin resistance and hyperglycemia,37,38 as well as inflammation and endothelial dysfunction.39,40 In an analysis of the Jackson Heart Study, the largest cohort study of African Americans in the United States 41 as well as another analysis involving >80 000 postmenopausal women in the Women’s Health Initiative without heart failure history, 42 the quantity of dietary magnesium intake had an independent and negative relationship with incident or recurrent heart failure hospitalizations. For the subgroup with diabetes, individuals in the highest quartile of magnesium intake per kilogram of body mass were at a much lower risk for heart failure hospitalizations in comparison to those whose magnesium intake was in the lowest quartile (hazard ratio = 0.46; 95% CI = 0.26-0.84) during 5 years of follow-up. 41
In addition, there is new evidence supporting a beneficial effect of caloric restriction. Kitzman et al
43
examined the association between caloric restriction and exercise training in obese older patients with HFpEF and found that either caloric restriction or aerobic exercise training individually increased peak V.
Manage Blood Pressure
Studies have shown that hypertension antedates the development of HFpEF in nearly 90% of cases, and it confers a 3-fold increased risk of developing HFpEF. 45 There is a graded, continuous association between baseline systolic blood pressure and risk for heart failure, to the degree that even prehypertension was associated with an increased risk for heart failure compared with individuals with optimal systolic blood pressure (<120 mm Hg). 46
It is commonly accepted that diastolic dysfunction is one of the mechanisms through which hypertension leads to HFpEF.1,2 The increased LV stiffness and impaired LV relaxation secondary to high afterload pressures, often associated with concentric LV hypertrophy, result in diastolic dysfunction and are thought to be key components in the pathophysiological process of HFpEF.1,2,13 Diastolic dysfunction occurs in 50% of patients with hypertension and has been shown to be associated with increased cardiovascular morbidity and mortality as well as HFpEF.47,48 In the observational Assessment of Prevalence Observational Study of Diastolic Dysfunction (APROS-diadys) study, 49 26% of elderly hypertensive patients without heart failure symptoms and with an LVEF of 45% or greater had diastolic dysfunction on echocardiographic Doppler examination. The rate of diastolic dysfunction was significantly higher in those who had uncontrolled hypertension than in those with controlled hypertension,49,50 emphasizing the need for good blood pressure control.
Blood pressure can be controlled effectively in the majority of HFpEF patients with the use of common pharmacological agents such as diuretics, angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, and vasodilating β-blockers such as carvedilol. 44 In both the VALIDD (Valsartan In Diastolic Dysfunction) 51 and EXCEED (Exforge Intensive Control of Hypertension to Evaluate Efficacy in Diastolic Dysfunction) 52 trials, diastolic function improved in patients with hypertension after blood pressure control. The amount of improvement in diastolic function correlated with the amount of blood pressure lowering achieved, irrespective of the medications used to control blood pressure. 53 In the recent SPRINT trial, achieving an optimal systolic blood pressure of near 120 mm Hg was associated with a 38% reduction in the risk of heart failure and 27% risk reduction in all-cause mortality compared with a standard care arm who achieved a systolic blood pressure of 136 mm Hg. 54
With the high prevalence of hypertension and its associated complications, blood pressure management is an important and desirable goal that can improve diastolic dysfunction and reduce the incidence of heart failure, especially HFpEF.6,55
Control Cholesterol
Contrary to other risk factors, observational evidence has shown that lower cholesterol levels are associated with higher mortality in heart failure patients.56-58 However, it has been suggested that the pleiotropic effects of statins, such as antioxidant, anti-inflammatory, and antihypertrophic effects, 59 all of which are involved in the pathophysiological mechanisms of heart failure, may be of benefit in this population. Statins are also effective in the primary and secondary prevention of atherosclerotic coronary artery disease, 60 which may benefit patients with ischemia-related heart failure.
Two large randomized controlled trials did not show statins to be beneficial in patients with either ischemic HFrEF 61 or HFrEF in general. 62 Nonetheless, an initial single-center, observational study by Fukuta et al suggested that statins may improve mortality in patients with HFpEF. 63 Similarly, Nochioka et al 64 analyzed the effect of statins in more than 3000 patients with HFpEF and more than 1400 patients with HFrEF over 3 years in the Chronic Heart Failure Analysis and Registry in the Tohoku district-2 (CHART-2) project. 64 The authors found no effect of statins on mortality in HFrEF patients, but mortality reduction was found in patients with HFpEF (hazard ratio = 0.74; 95% CI = 0.58-0.94; P < .001). 64 A meta-analysis of observational studies relating the effect of statins and mortality in patients with HFpEF suggested that the use of statins was associated with a 40% reduction in mortality. 65 Thus, based on current evidence, statins may be one of the few pharmacological therapies that appear promising in patients with HFpEF, 59 but randomized controlled trials are needed to confirm these observations.
Reduce Blood Sugar
Individuals with diabetes are at increased risk of developing heart failure66,67 and have an increased risk of death related to heart failure.68,69 In a national sample of 151 738 Medicare beneficiaries with diabetes, the incidence rate for heart failure was 12.6 per 100 person-years. 68 Patients with diabetes are known to be at high risk for accelerated LV hypertrophy and functional abnormalities (in relaxation and contraction), both of which are harbingers of incident heart failure,69-71 specifically HFpEF.13,69,72 These changes in LV structure and function, collectively called diabetic cardiomyopathy, are multifactorial and can be explained by typical features of diabetes, such as insulin resistance and hyperglycemia,73,74 oxidative stress, and inflammation,40,75 all of which can lead to anatomical and functional changes in the heart and the peripheral vasculature. Changes such as myocardial fibrosis and deposition of fat in the myocardium19,76 -78 and endothelial dysfunction 79 contribute to the changes in LV mass as well as decreased exercise tolerance, which may result in decreased quality of life for the patient with diabetes and ultimately clinical heart failure. 69
Although there are no randomized controlled trials to show a relationship between improved glycemic control and HFpEF, observational evidence suggests a positive association between hemoglobin A1c and the risk of incident heart failure (HFrEF and HFpEF). 80 Therefore, glucose control is a potentially key element in HFpEF management. From a pharmacotherapy perspective, the risk of heart failure varied by the pharmacotherapeutic agent used to achieve glycemic control in diabetes. Both pioglitazone and rosiglitazone have been shown to increase the risk of heart failure by at least 40%.81,82 There is consensus that metformin is in general safe in heart failure,83,84 with 1 observational study suggesting that metformin may reduce mortality in these patients. 85 Among the dipeptidyl peptidase 4 (DPP-IV) inhibitors, saxagliptin was shown to increase the risk of heart failure by ~27%,86,87 whereas sitagliptin has been shown to be safe in patients with heart failure. 88 One new class of medications, the sodium-glucose co-transporter 2 (SGLT2) inhibitors, may have an impact on heart failure. Specifically, empagliflozin, is the only antidiabetic agent that has been shown to reduce the risk of hospitalization for heart failure in a multicenter randomized controlled trial (hazard ratio = 0.65; 95% CI = 0.50-0.85). 89
Based on the above, prevention of diabetes onset or glucose lowering in patients with diabetes should be considered an important strategy to prevent and manage HFpEF, and lifestyle changes (diet, weight, and exercise) in addition to specific antidiabetic medications should be utilized.
Conclusion
HFpEF constitutes approximately half of all heart failure diagnoses and is associated with considerable morbidity and mortality.1,3,4 The treatment of HFpEF can be challenging because of a lack of evidence to support the benefit of various drug therapies. 90 To date, multiple large-scale pharmacological clinical trials have failed to improve the outcome of patients with established HFpEF (Table 1). Therefore, the cornerstone of treatment for HFpEF remains prevention through early modification of risk factors. 6 The AHA Life’s Simple 7 highlights the specific lifestyle modifications that should be strongly considered to reduce the burden of this prevalent disease.
Footnotes
Acknowledgements
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This research protocol was approved by the Ohio University Institutional Research Board.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.