
Abstract
Objective. History of stroke increases risk for recurrent stroke, which is a significant issue faced by survivors. The Diabetes Prevention Program–Group Lifestyle Balance (DPP-GLB) program is an effective lifestyle modification intervention for ameliorating cardiovascular risk factors but has not been adapted to account for common stroke-related deficits. The purpose of this study was to determine appropriate adaptations to the DPP-GLB for adults with stroke. Design and Methods. In this phenomenological qualitative study, a total of 15 community-dwelling adults with stroke and 10 care-partners participated in 4 focus groups to review DPP-GLB curriculum materials and provide recommendations for adaptation. Focus groups were recorded and transcribed. Inductive content analysis was used to identify key themes. Results. Three themes were identified. First, physical, cognitive, sensory, and psychosocial stroke-related deficits could affect DPP-GLB participation. Second, existing DPP-GLB characteristics could facilitate participation by adults with stroke. Third, stroke-specific adaptations were recommended, including modified session content and format, adapted physical activity and dietary recommendations, and inclusion of care-partners. Conclusion. Current DPP-GLB content and structure may be insufficient to meet the unique needs of adults with stroke. The suggested adaptations should be incorporated into a stroke-specific curriculum and tested for preliminary efficacy for reducing recurrent stroke risk.
Regular physical activity, healthy dietary behaviors, and weight management are lifestyle behaviors that can reduce risk for diabetes and recurrent stroke.
In the United States, approximately 795 000 people experience a stroke each year, of which approximately 25% are recurrent events. 1 The American Heart Association identifies physical inactivity, poor nutrition, cigarette smoking, overweight or obesity, high cholesterol, high blood pressure, and diabetes as risk factors for cardiometabolic diseases, including cardiovascular disease and stroke. 2 Modification of these risk factors to achieve improved cardiovascular health metrics can lower risk for recurrent stroke. 3 Unfortunately, estimated prevalences of these risk factors are high in adults with stroke, particularly for physical inactivity (56.5%), overweight and obesity (70.2%), and diabetes (22.6%), and exceed estimates for adults without stroke. 4
Common stroke sequelae include physical, cognitive, and psychosocial deficits. 5 Deficits may include hemiparesis, fatigue, depression, and impaired concentration, comprehension, and memory. These deficits may contribute to physical inactivity and poor dietary behaviors, which, in turn, contribute to diabetes, overweight, and obesity. Physical activity, dietary modification, and weight management are recommended for secondary stroke prevention 3 and also recommended for primary and secondary diabetes prevention.6,7 While evidence-based interventions for health behavior modification after stroke are lacking, such programs exist for diabetes prevention and could be used as a model for secondary stroke prevention.
The Diabetes Prevention Program (DPP) is an evidence-based intervention that promotes ≥7% weight loss through regular physical activity and dietary behavior for preventing or delaying diabetes onset.8,9 Furthermore, the DPP can lead to desirable long-term improvement in blood pressure, blood cholesterol, and triglyceride concentration. 10 Originally an individual-based intervention, the DPP has been adapted into group-based formats such as the DPP Group Lifestyle Balance (DPP-GLB) program, 11 with demonstrated efficacy in community and clinical settings.12,13 The DPP-GLB consists of 22 sessions delivered over a 12-month period, and session content includes making healthy food choices, increasing awareness of calories/fat intake, and engaging in physical activity. Sessions also promote personal goal setting and self-monitoring physical activity and dietary behaviors.
The efficacy of the DPP-GLB for achieving these outcomes in adults with stroke has not been examined. Given the physical, cognitive, and psychosocial challenges experienced by adults with stroke, the DPP-GLB likely needs to be modified to be feasible for use with this population as has been done with other populations, including mobility impairment 14 and traumatic brain injury. 15 Therefore, the purpose of this study was to explore how the DPP-GLB might be adapted to promote participation among adults with stroke.
Materials and Methods
Design
This phenomenological study used focus groups consisting of adults with stroke and available care-partners. Focus groups were chosen to enhance credibility (ie, internal validity) of research findings because data are triangulated across participants in real time as participants discuss topics of interest. 16 This study was approved by the Institutional Review Board at Washington University in St. Louis and conformed to the Declaration of Helsinki.
Participants
Participants with stroke were recruited from 2 stroke support groups at local rehabilitation hospitals as well as a university-run stroke clinic in St. Louis, Missouri, USA. Interested participants were screened for eligibility by telephone. Inclusion criteria for adults with stroke were the following: (1) being between 30 and 80 years, (2) having a stroke at least 6 months prior to the study, (3) the ability to walk at least 150 feet with or without an assistive device, (4) currently living in the community, and (5) sufficient cognition to participate (determined by a score ≤8 on the Short Blessed Test, a screening test used to determine impairment in memory, orientation, and concentration). 17 Exclusion criteria included the following: (1) neurological or psychiatric conditions other than stroke and (2) moderate or severe aphasia. Care-partners were encouraged, but not required, to participate in the study.
Procedure
Individuals who met eligibility criteria were scheduled to attend 1 of 4 focus groups. The focus groups were held in a conference room at Washington University in St Louis and led by a study team member. Upon arrival, participants provided written, informed consent to participate and completed a questionnaire that collected information on demographics, disability, and physical activity.
Each focus group lasted 1.5 to 2 hours and was audio-recorded. A semistructured interview guide was developed using materials from the DPP-GLB curricula adapted for impaired mobility 14 and traumatic brain injury, 15 which were obtained from the study authors. Questions were developed for understanding potential facilitators and barriers to program participation among adults with stroke and were used during each focus group to guide discussion. The first focus group focused on the structure, format, and overall general content of the DPP-GLB; the second group focused on physical activity; and the third and fourth groups focused on dietary behaviors, including food choices and meal preparation. Participants in focus groups 2 through 4 were also asked to confirm or refute participant responses from previous groups to triangulate responses across sessions, further facilitating credibility of findings. 18
Measures
A study questionnaire was used to solicit demographic (age, sex, ethnicity, marital status) and health information (number of strokes, years since stroke, height, weight). Level of functional disability was obtained using the Modified Rankin Scale, a valid and reliable assessment used to quantify the degree of dependence in daily activities. 19 Participants indicated their level of disability across 4 categories (ie, no disability, no significant disability, slight disability, moderate disability but able to walk). The 2 remaining categories (ie, severe disability, dead) were omitted because they conflicted with study inclusion criteria. Whether or not participants met recommended levels of physical activity as described by the Physical Activity Guidelines for Americans (ie, ≥150 minutes of moderate-to-vigorous physical activity) 20 was determined by the Stanford Leisure-Time Activity Categorical Item, a single-item instrument that assesses national physical activity recommendations. 21
Data Analyses
Quantitative
Descriptive statistics were computed for demographic and study measures data using SPSS Version 24 software (IBM Corp, Armonk, NY). For disability status, disability categories “no significant disability” and “slight disability” were condensed into one category (ie, “slight disability”) because the number of responses in each individual category was low.
Qualitative
NVivo 12 software (QSR International, Melbourne, Australia) was used to code focus group transcripts, and inductive content analysis 22 was used to analyze the data. First, the study principal investigator (RRB) and a research assistant (JLS) independently read the transcripts and developed a preliminary codebook. Second, both coders met to discuss and agree upon a final set of codes. Third, the coders independently applied the codes to the focus group transcripts. Fourth, the coders met to identify key themes from the coded data. Disagreements were resolved by consensus among the entire research team. This systematic process enhances dependability (ie, reliability) of findings. 16
Results
Participant Characteristics
Four focus groups were conducted with a total of 15 adults with stroke and 10 care-partners. Thirteen participants with stroke were recruited from local stroke support groups and the 2 remaining participants with stroke were recruited from a university-run clinic. Participation by adults with stroke and care-partners varied by session: Group 1 (4 stroke, 2 care-partner), Group 2 (6 stroke, 5 care-partner), Group 3 (2 stroke, 2 care-partner), and Group 4 (3 stroke, 1 care-partner). Demographic and health information are reported in Table 1. Adults with stroke were mostly male, non-Hispanic White, married or cohabitating, overweight (ie, body mass index >25 kg/m2), reported moderate disability, and reported not meeting physical activity recommendations. Care-partners were mostly non-Hispanic White, married or cohabitating, and overweight; however, most did not experience disability and reported meeting physical activity recommendations.
Demographic and Health Information for Study Participants.
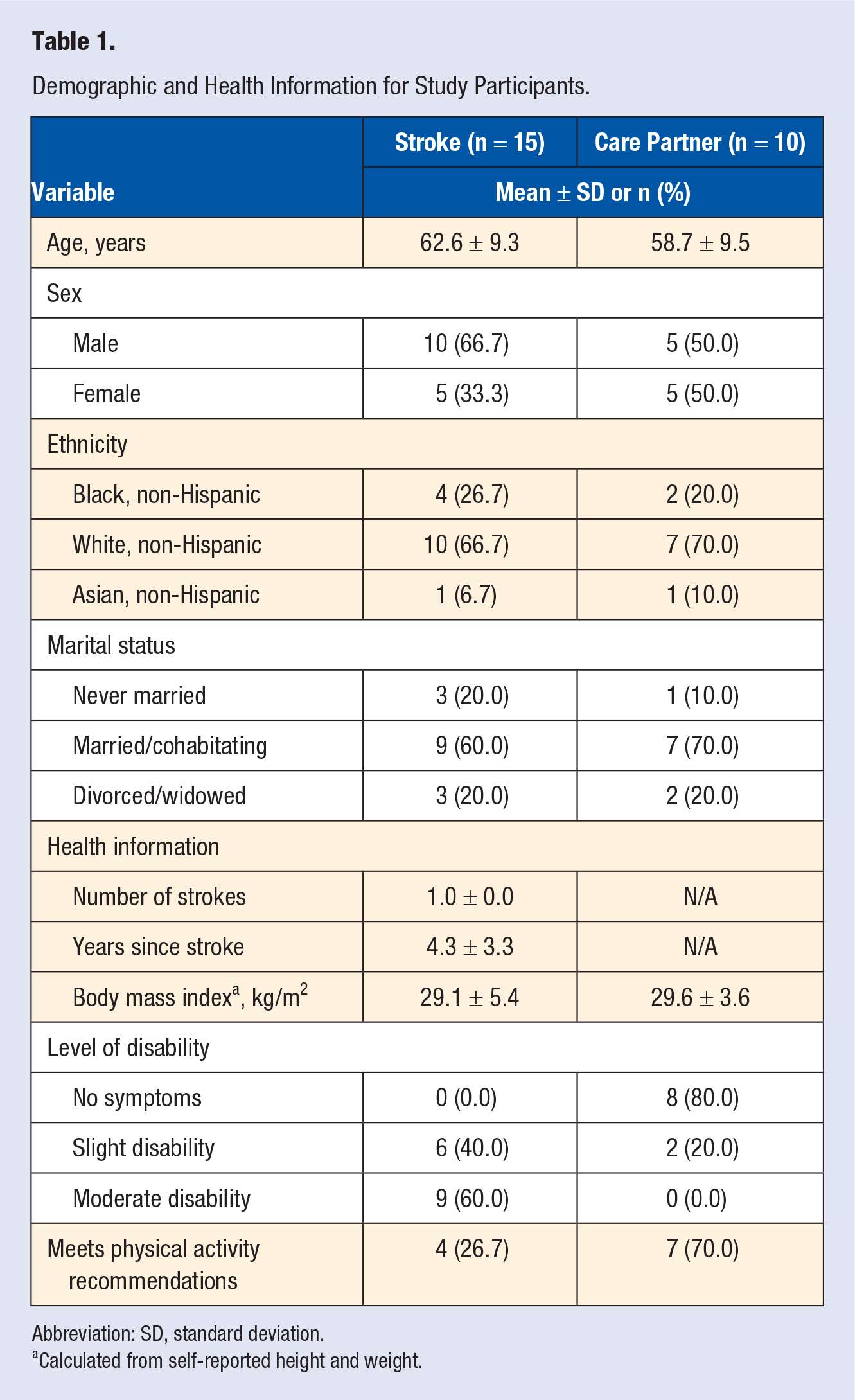
Abbreviation: SD, standard deviation.
Calculated from self-reported height and weight.
Qualitative Findings
Three key themes related to DPP-GLB participation for adults with stroke were identified: (1) stroke-related deficits impact participation, (2) existing program characteristics facilitate participation, and (3) recommended stroke-specific adaptations to promote participation. These themes and their related subthemes are illustrated in Figure 1. Selected quotations are included in the supplemental file to illustrate key themes (available online).
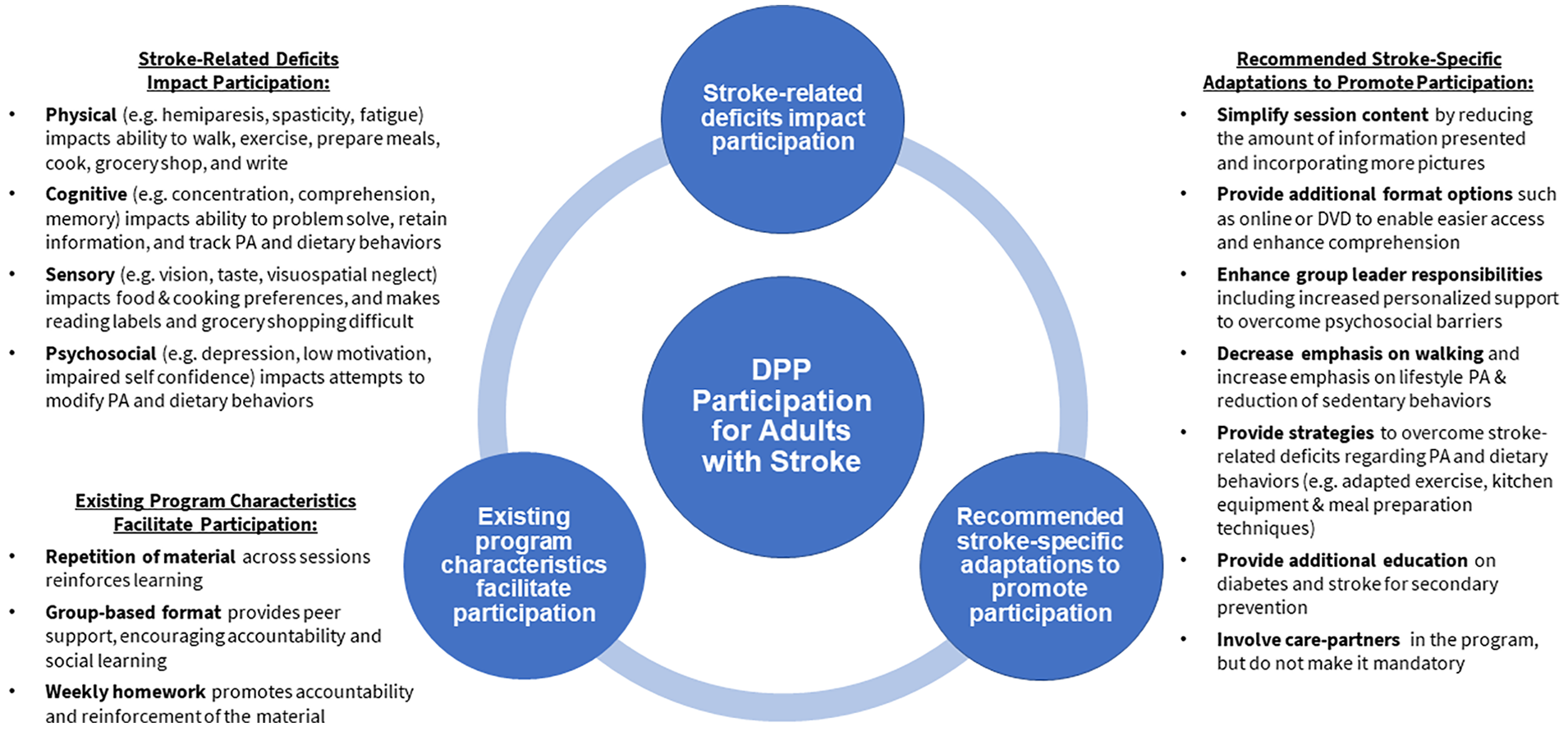
Key study findings. Participants’ responses were summarized into 3 themes and related subthemes.
Theme 1: Stroke-Related Deficits Affect Participation
Participants in all focus groups identified stroke-related deficits that would affect participation in the DPP-GLB. Deficits included physical (hemiparesis, spasticity, and fatigue), cognitive (concentration, comprehension, memory, and cognitive fatigue), sensory (changes in taste, vision, and visuospatial neglect), and psychosocial (depression, low motivation, and decreased self-confidence) impairments. Participants explained that physical deficits would make it difficult to successfully engage in walking, exercise, meal preparation, grocery shopping, and writing when tracking physical activity and dietary behaviors. Cognitive deficits would make it difficult to track physical activity and dietary behaviors, problem solve how to overcome physical activity and dietary challenges, and retain information taught during sessions. Sensory deficits would affect food and cooking preferences and could result in difficulty tracking physical activity and dietary behaviors in the written log. Last, psychosocial deficits would negatively influence attempts to modify physical activity and dietary behaviors.
Theme 2: Existing Program Characteristics Facilitate Participation
Participants identified preexisting characteristics of the DPP-GLB that would facilitate participation for adults with stroke, which included overall program structure, the group-based format, weekly homework, and involvement of a supportive lifestyle coach.
Program structure
DPP-GLB sessions interweave physical activity and dietary behavior content across multiple sessions, so the information is repeatedly reviewed throughout the program. Participants identified this as a facilitator, stating that they need repetition and reinforcement to aid in retention of newly learned material. Participants also identified personalized goal setting, leader follow-up on participant tracking, and facilitated discussion as helpful characteristics of the program.
Group-based format
Participants stated that the group-based format of the program would provide peer support, which would encourage accountability and social learning. Participants preferred in-person meetings rather than remote or online sessions. The DPP-GLB adapted for mobility impairment 14 included monthly conference calls in place of an in-person meeting. However, participants in our study preferred in-person meetings for the reasons described above, but they also acknowledged the need for flexibility due to scheduling conflicts (eg, medical appointments, outpatient therapies, unavailability of care-partners) that might arise. Participants also explained that small group discussions would facilitate comprehension of the material apart from simply reading the material because processing a lot of written and spoken information could be overwhelming following stroke.
Weekly homework
Participants believed that weekly homework, including self-monitoring of physical activity and dietary behaviors, would help with both reinforcement of the information and provide accountability.
Supportive lifestyle coach involvement
Participants indicated they would benefit from supportive involvement of the lifestyle coach, specifically in helping participants identify appropriate goals for their unique situation and providing increased personal support via phone calls, personalized feedback, and supportive encouragement. For many, this recommendation was tied to overcoming psychosocial barriers and was thought to be imperative for successful participation in the program.
Theme 3: Recommended Stroke-Specific Adaptations to Promote Participation
Throughout the focus groups, participants suggested many adaptations that they believed would make participation in the DPP-GLB more suitable for adults with stroke. These recommendations included adaptations to session content and format, physical activity and dietary behaviors, stroke and diabetes education, and care-partner involvement.
Session content and format
Participants identified the length and visual presentation of the handout materials to be a concern. Some felt overwhelmed by the amount of information and the majority agreed that the visual presentation should be simplified by incorporating more pictures and less words. Overall, it was agreed that 4 to 5 pages maximum of handout materials (per session) was optimal, while the rest of the information was still beneficial and could be placed in an appendix and referenced as needed. Participants also suggested that multiple formats of the session should be available. A DVD/video or ability to access materials online was proposed for those who could not make it to the session or wanted to enhance their comprehension of the material by reviewing it later.
Physical activity and dietary behaviors
Participants suggested that using mobile apps for tracking physical activity and dietary behaviors would be helpful to overcome the physical and cognitive deficits associated with these behaviors. Regarding physical activity, participants requested information on how to safely exercise within the context of stroke, education on adapted gym equipment, and instruction in home-based exercises. Participants also agreed that there should be less emphasis on walking as the main type of physical activity, preferring more emphasis on daily (ie, lifestyle) physical activity and decreasing sedentary behavior.
Suggested dietary behavior strategies included information on adapted kitchen equipment and meal preparation techniques, along with online grocery order and home delivery services for those who experience difficulty grocery shopping. Participants were shown a handout of adaptive equipment from the impaired mobility-adapted curriculum 14 for overcoming barriers in the kitchen, which participants unanimously indicated would be very helpful for inclusion in a stroke-adapted curriculum.
Additional diabetes and stroke education
Participants indicated that they would like more stroke-related education relating to diabetes. Multiple participants expressed the desire for information on how physiological processes (eg, glucose regulation, insulin sensitivity) can be affected by stroke and their role in diabetes and stroke management and prevention.
Participants also recommended that information on local community resources should be provided. Throughout the focus groups, participants shared resources they had used since their stroke. Some reported using many community resources while others reported not knowing about any such resource. Example resources that participants recommended included gyms with accessible equipment, physical activity programs for older adults (eg, Silver Sneakers), local stroke support groups, and other stroke-related community offerings (eg, free clinics, social events).
Care-partner involvement
Participants acknowledged that care-partner involvement could enhance DPP-GLB participation by adults with stroke through support and reinforcement, particularly in situations where the care-partner participates wholly or partially in the program. Participants were cautionary with this recommendation, however. They explained that care-partner involvement could increase relationship strain in situations where the care-partner was to demand program compliance from their stroke counterpart. To prevent straining the relationship, participants recommended that care-partners should be instructed to encourage (eg, act as a cheerleader) their stroke counterpart, rather than nag or shame them into compliance. Importantly, participants identified that care-partner involvement must be optional, as some people may not have a care-partner, or their care-partner may not be available to attend.
Discussion
Adults with stroke are at high risk for cardiometabolic diseases, recurrent stroke, and diabetes. Lifestyle management—including physical activity, dietary behaviors, and weight management—is a viable option to reduce risk for these conditions. The DPP-GLB is a model lifestyle management program; however, it was developed for a nonstroke population and without consideration for stroke-related deficits that may limit program participation.
Previous qualitative and quantitative investigations have identified stroke-related physical, cognitive, sensory, and psychosocial deficits that negatively affect physical activity23-26 and dietary behaviors.27,28 Similar stroke-related deficits were identified by our study participants that would challenge their ability to participate in the DPP-GLB. These findings support our assertion that an adapted DPP-GLB curriculum is needed that accommodates stroke-related deficits.
Study participants identified several existing program characteristics that would facilitate participation by adults with stroke. Participants liked how the DPP-GLB interweaves key concepts throughout multiple sessions, which is a practice supported by research indicating that spaced repetition of content produces stronger memories and leads to better learning. 29 Weekly homework also reinforces the learning process through repetition of key concepts, and enhances self-efficacy and responsibility for learning. 30
Many study participants also verbalized preference for an in-person, closed-group format. Previous research has identified that group-based peer support groups in adults with stroke can lead to feeling empowered and can increase one’s sense of agency and independence (ie, self-efficacy), 25 which is a characteristic that predicts DPP weight outcome achievement. 31 Furthermore, a systematic review concluded that peer support following stroke can also enhance social support and physical quality of life. 32
Related to the third theme, 4 stroke-specific adaptations were recommended to increase participation for adults with stroke. First, simplify session materials to reduce cognitive load and provide additional format options (eg, online or DVD in addition to in-person meetings). These recommendations are supported by healthy literacy research, which indicates that factors such as format, wording, and the medium through which information is delivered influences comprehension and recall, and further suggests that simplifying text and using a combination of text and video (ie, multiple presentation formats) may be more effective than either format alone. 33
Second, enhance lifestyle coach responsibilities to assist in overcoming stroke-related psychosocial barriers. Individualized goal setting, feedback, and positive reinforcement, provided by the lifestyle coach, are beneficial in maximizing success and adhering to dietary and physical activity modification goals.26,34,35
Third, provide information on adaptations for overcoming stroke-related barriers affecting physical activity and dietary behaviors. Study participants requested information on adapted equipment and alternative strategies (eg, chair-based exercise, one-handed cooking techniques) for physical activity and dietary behaviors. Importantly, similar information was included in the DPP-GLB adapted for impaired mobility pilot study and was reported to facilitate successful program participation.14,36
Last of all, inclusion of a care-partner in the program to compensate for stroke-related deficits. The traumatic brain injury-adapted DPP-GLB reported successful integration of care-partners to facilitate social and physical support as needed 37 and care-partner assistance has been reported as an inportant factor for facilitating physical activity 38 and dietary behaviors 28 in adults with stroke. Of note, our study participants acknowledged that the addition of care-partners could also cause strain on the relationship due to increased dependence on care-partners. Prior research has demonstrated direct associations between patient dependency and caregiver burden and caregiver quality of life. 39 Thus, it is important that individuals with stroke and their care-partners determine the appropriate level of care-partner involvement in a stroke-adapted program.
In sum, our findings highlight the need for a modified DPP-GLB curriculum to meet the unique needs of adults with stroke. The DPP-GLB is an effective, evidence-based intervention and a modified curriculum has the potential to enhance healthy lifestyle behaviors in adults with stroke and serve as a model for secondary stroke prevention.
Limitations
This study is subject to several limitations. First, the sample size was small and limited to ambulatory, community-dwelling adults with chronic stroke, which limits generalizability to the larger stroke population. However, the study included adults who had experienced stroke from 6 months to 7 years previously, and therefore represents perspectives from individuals at various stages of recovery. Furthermore, findings are strengthened by triangulation of data through convergence of information across participants both within and across focus groups. Second, the DPP-GLB curriculum was not presented in its entirety to study participants; thus, there may be additional program characteristics that act as facilitators and barriers that were not identified by study participants. Core program content (ie, physical activity and dietary behaviors) is spread throughout all DPP-GLB sessions, however, and study participants’ suggestions likely generalize to all sessions. Third, most participants were recruited from stroke support groups, which may have influenced their favorable opinion of a group-based format. Additionally, only the DPP-GLB curriculum—a group-based program—was discussed in focus groups. Preference for a group- versus individual-based stroke-adapted curriculum could vary among adults with stroke and should be explored. Finally, the efficacy of the recommended adaptions was not tested in this study. Future directions include confirming our key findings in a larger sample of community-dwelling adults with stroke and empirically testing a stroke-adapted DPP-GLB curriculum to determine feasibility and efficacy.
Conclusion
Regular physical activity, healthy dietary behaviors, and weight management are lifestyle behaviors that can reduce risk for diabetes and recurrent stroke. These factors are key components of the DPP-GLB; however, as reported by adults with stroke and their care-partners, current DPP-GLB content and structure may be insufficient for meeting the unique needs of adults with stroke. Study participants identified barriers and facilitators to the existing program and suggested stroke-specific adaptations to increase DPP-GLB participation by adults with stroke. Although additional investigation is needed, these findings support the need for a stroke-adapted DPP-GLB curriculum and provide specific suggestions for adapting such a curriculum.
Supplemental Material
Supplemental_Material – Supplemental material for Health Behavior Change Following Stroke Recommendations for Adapting the Diabetes Prevention Program–Group Lifestyle Balance Program
Supplemental material, Supplemental_Material for Health Behavior Change Following Stroke Recommendations for Adapting the Diabetes Prevention Program–Group Lifestyle Balance Program by Ryan R. Bailey, Jennifer L. Stevenson, Simon Driver and Evan McShan in American Journal of Lifestyle Medicine
Footnotes
Acknowledgements
We acknowledge the complementary and concurrent work of Simon Driver and Evan McShan in adapting the DPP Group Lifestyle Balance program for adults with stroke, who have recently began recruiting for a randomized controlled trial to examine the efficacy of a stroke-adapted DPP (NCT03873467). In this current study, they provided input on the focus group interview guide and critically reviewed the manuscript.
Authors’ Note
The data that support the findings of this study are available on request from the corresponding author, RRB. The data are not publicly available due to the relatively small sample size and defined location from which participants were recruited, which could compromise the privacy of research participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health (Grant Numbers P30DK092950 and 5T32HL130357).
Ethical Approval
This study was approved by the Institutional Review Board at Washington University in St. Louis and conformed to the Declaration of Helsinki.
Informed Consent
Participants provided written, informed consent to participate.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Supplemental Material
Supplemental materials for this article are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.