
Abstract
Along with proper diet and avoidance of tobacco use, physical activity is extremely important to maintain and improve overall health of the individual and population. Despite evidence for the cost-effectiveness of physical activity counseling in primary care, only one-third of patients report that they received physical activity counseling by their primary care physician (PCP). Both PCPs and patients face numerous barriers to addressing insufficient physical activity. To assist patients in overcoming their barriers to regular physical activity, the PCP should assess and address the patient’s specific barriers to physical activity and counsel patients about the most common general barriers, such as lack of time, knowledge, and motivation. Numerous benefits and barriers are present, and the PCP should understand them and use the information to better counsel patients regarding the benefit of and need for regular physical activity. Brief counseling is an efficient, effective, and cost-effective means to increase physical activity and to bring considerable clinical benefits to various patient populations.
‘The new physical activity guidelines encourage adults to move more and to sit less, acknowledging that some physical activity is better than none . . .’
Physical Activity
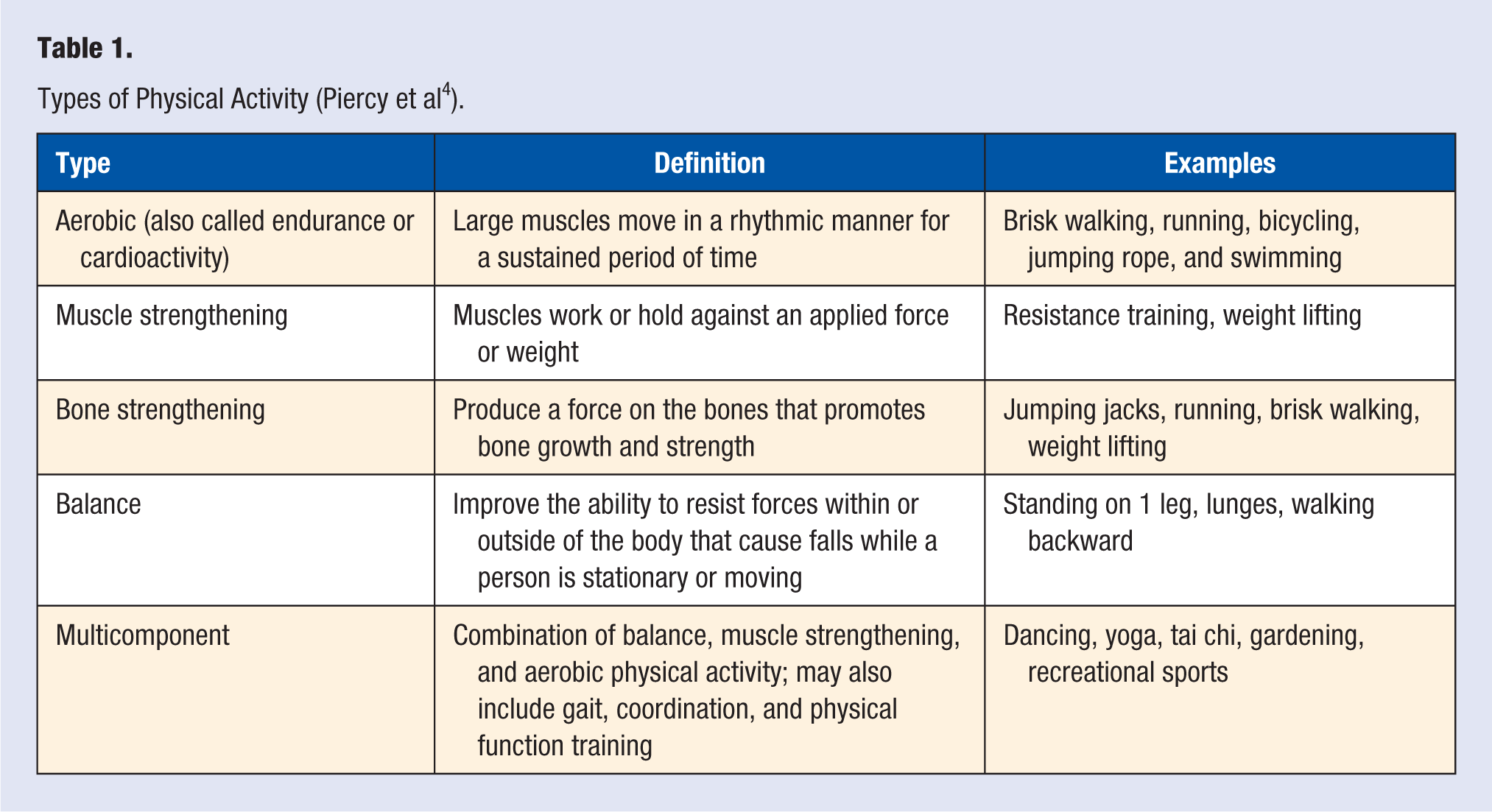
Physical activity is any bodily movement produced by skeletal muscles that results in energy expenditure above the resting (or basal) level.1,2 Physical activity includes exercise, sports, household activity, occupation, leisure, and active transportation. 3 Several forms of physical activity exist (Table 1). Exercise, a subcategory of physical activity, is planned, structured, repetitive, and purposeful. 2
Types of Physical Activity (Piercy et al 4 ).
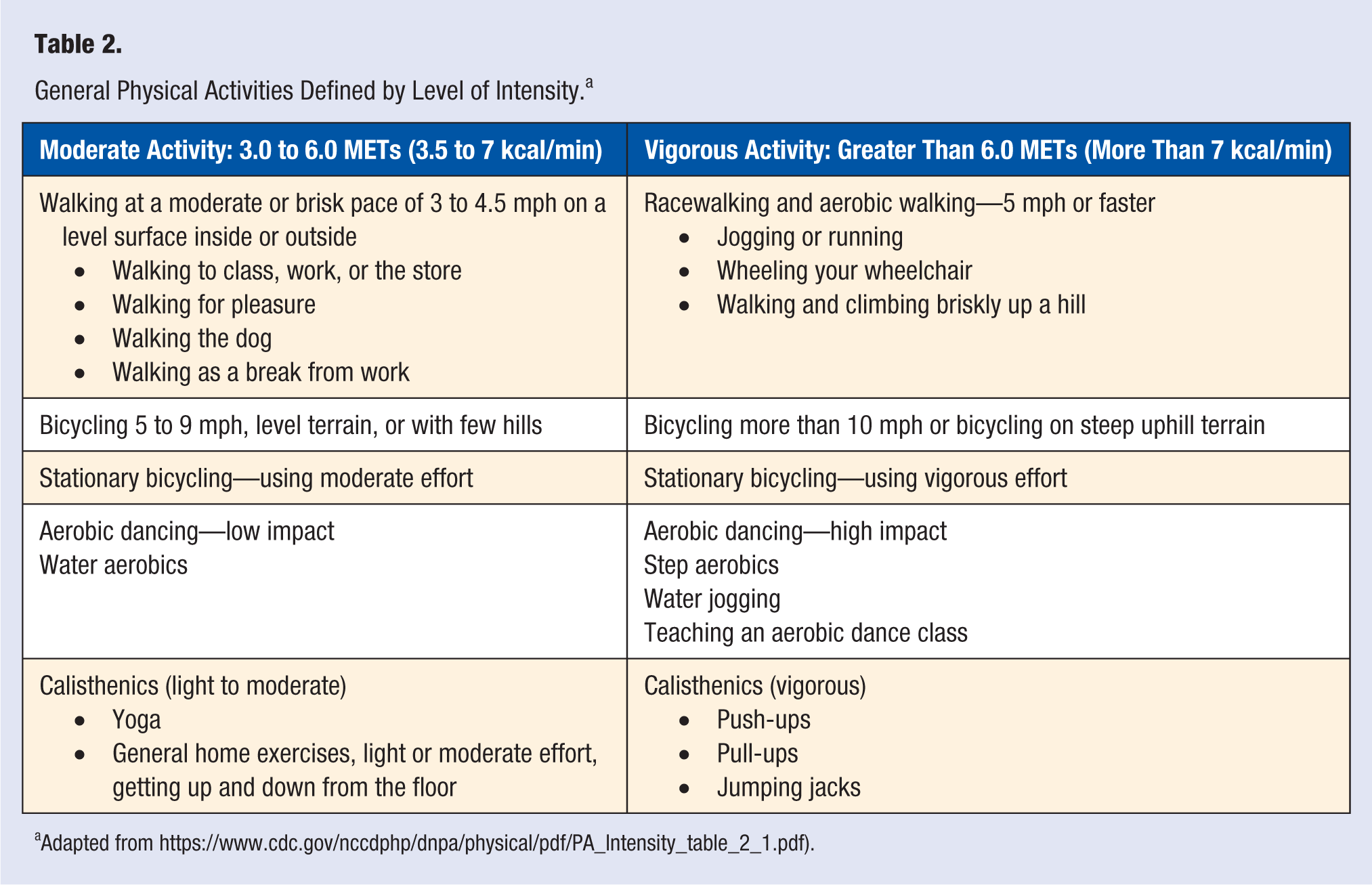
Aerobic physical activity has 3 components: intensity, duration, and frequency. 4 The intensity is measured as absolute or relative. Absolute intensity is the amount of energy spent during physical activity without the consideration of the person’s cardiorespiratory fitness or aerobic capacity and is expressed in metabolic equivalent task units or MET units. A MET is the ratio of the activity metabolic rate to the resting metabolic rate. 1 Resting metabolic energy expenditure equals 1 MET. Physical activity requiring 5 times more energy expenditure than just resting equals 5 METs (Table 2).
General Physical Activities Defined by Level of Intensity. a
Relative intensity is the ease or difficulty with which an individual performs any given physical activity compared with their capacity. 4 A 10-point Perceived Exertion Scale is often used to measure relative intensity (0 is the minimal exertion level and 10 is maximal physical effort). Some experts use the ability of singing or talking during exercise as a way to measure intensity: one is able to sing during very mild activity, can only use single words during more vigorous tasks, and is unable to talk during maximal exertion.
Similarly, weight training has 3 components: intensity, frequency, and sets and repetitions. 4 The amount of weight or force used relative to how much a person is able to lift or the force applied to a stationary object is the intensity. Frequency is how often a person does the strengthening activity. Finally, sets and repetitions are how many times a person does the activity.
Recommended Amount of Physical Activity
The current physical activity guidelines recommend 150 to 300 min/wk of moderate-to-vigorous intensity physical activity or 75 to 100 min/wk of vigorous intensity physical activity, which extends to general as well as clinical populations. 1 Whereas a clear dose-response relationship between physical activity and health, with 20% to 30% risk reduction for premature mortality and chronic disease, is often observed in those individuals who meet or exceed current international recommendations, lower levels of physical activity can lead to significant health benefits. 5 The new physical activity guidelines encourage adults to move more and to sit less, acknowledging that some physical activity is better than none, and that adults who sit less and do any amount of moderate to vigorous activity gain some benefits. 1
In general, the greatest relative health benefits are seen in physically inactive individuals who become physically active. 6 As such, minor increases in physical activity in inactive individuals may lead to marked reductions in the risk for chronic disease and mortality. Wen et al 7 found that 15 min/d or 90 min/wk of moderate-intensity physical activity had a 14% reduced all-cause mortality and a 3-year longer life expectancy. Every additional 15 minutes of daily exercise beyond the minimum amount of 5 min/d further reduced all-cause mortality by 4% and all-cancer mortality by 1%. A systematic review and meta-analysis by Hupin et al 8 found that low doses of moderate to vigorous physical activity at half of the recommended amount (equating to 15 minutes of brisk walking a day) led to a 22% reduction in all-cause mortality in older adults. These findings indicate that the relative health benefits of physical activity are achieved at lower doses than the current recommendation of 150 min/wk and should not discourage patients who may not be able to achieve it.
Most guidelines focus on moderate-intensity and vigorous-intensity physical activities. Moderate-intensity physical activity is defined as one with a MET of 3.0 to 5.9. When engaged in moderate-intensity physical activity, most people are able to talk but not sing. On a 10-point scale, moderate-intensity activity is about 5 to 6 points. Examples include walking 3 to 4 mph, mopping, vacuuming, or raking the yard. Vigorous-intensity physical activity is defined as one with a MET of 6 and greater. When engaged in vigorous-intensity physical activity most people are not able to speak more than a few words without pausing to take a breath. On a 10-point scale, vigorous-intensity activity is about 7 to 8 points. Examples of vigorous exercises are walking 4.5 to 5 mph, running, carrying heavy groceries upstairs, shoveling snow by hand, and mowing grass with the hand-push mower.
Benefits of Physical Activity
Along with proper diet and avoidance of tobacco use, physical activity is extremely important to maintain and improve overall health of the individual and population. Nearly 10% of premature deaths in the United States, especially adults older than 40 years of age, are associated with inadequate physical activity.9,10 Less than half of adults meet the recommended level of moderate- or vigorous-intensity aerobic physical activity, and less than one-quarter meet the recommendations for strength training. 11 Physical activity rates are disproportionately lower among rural residents, residents of the southwestern region of the United States, women, older individuals, and racial and ethnic minorities.12,13
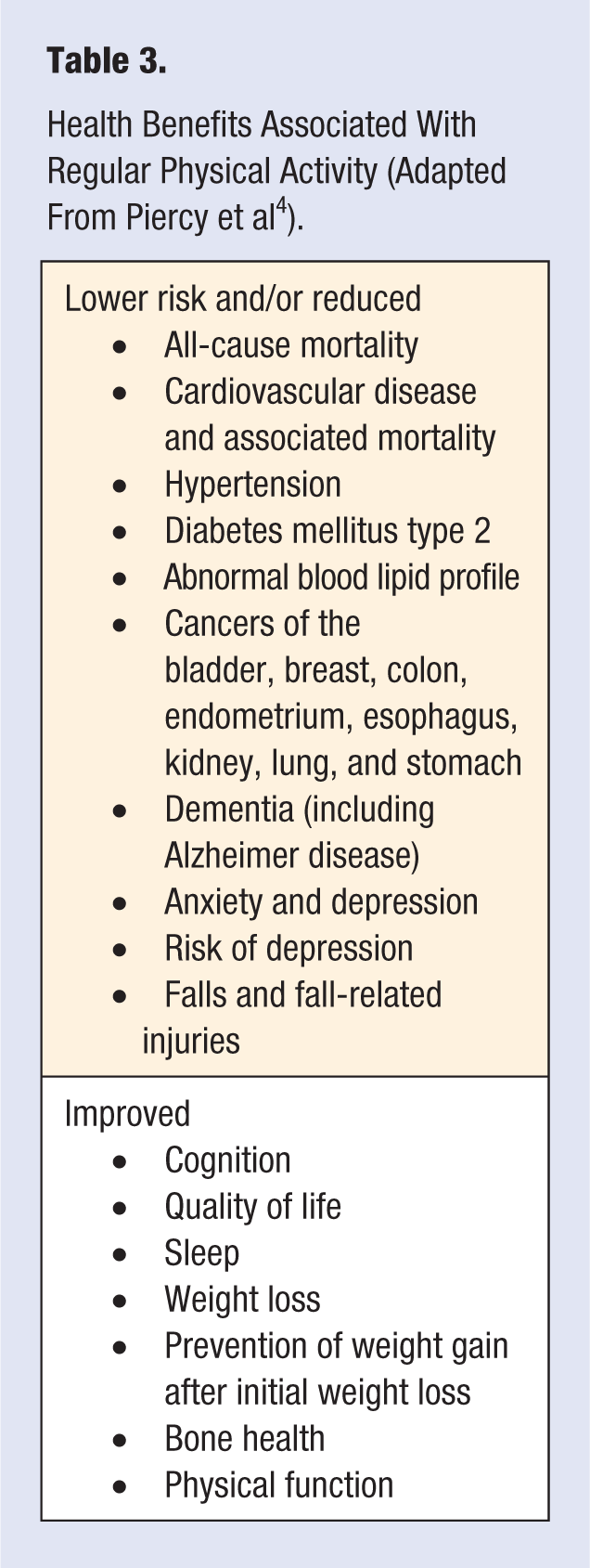
Overall, an inverse relationship is present between physical activity and rates for all-cause mortality and cardiovascular death.14-19 Activity and exercise have been recommended for the prevention and treatment of numerous diseases and medical conditions (Table 3). Most notably, habitual physical activity prevents the development of coronary artery disease and reduces symptoms in patients with established cardiovascular disease.20,21 Evidence also supports the role of exercise in reducing the risk of other chronic diseases, such as type 2 diabetes mellitus, osteoporosis, obesity, and cancer of the breast and colon.
Health Benefits Associated With Regular Physical Activity (Adapted From Piercy et al 4 ).
Hypertension is a well-known and leading cause of mortality and risk factor for heart disease, stroke, and renal disease. Patients with hypertension are able to reduce their systolic and diastolic blood pressure by up to 11.0 and 7.7 mm Hg, respectively, as a result of aerobic exercise.17,22 An inverse dose-response association between levels of recreational physical activity and risk of hypertension is present.18,23 Specifically, the risk of hypertension is reduced by 6% with each 10 MET h/wk increment in leisure-time physical activity.19,24
Stroke is a leading cause of death and disability in the industrialized world. High-levels of physical activity are associated with risk reduction of about 31%.21,25 This benefit is seen both in men and women and present for both ischemic and hemorrhagic stroke. Physically inactive people have a significantly elevated stroke risk.22,26
Diabetes mellitus is a major source of morbidity, with significant health, social, and economic implications, and obesity and physical inactivity are the main nongenetic determinants of the disease. Current diabetes treatments help control hyperglycemia and slightly decrease diabetic complications. However, they cannot eliminate all the adverse consequences, and the treatments have had limited success at reducing macrovascular complications.
In the general population, higher levels of leisure time physical activity are associated with lower rates of type 2 diabetes mellitus.23,27 Of interest, the greatest relative benefits are achieved at low levels of activity. Regular physical activity and exercise is important in the overall management of diabetes.24,28 A structured exercise program of at least 8 weeks’ duration lowered hemoglobin A1C by an average of 0.66% in people with type 2 diabetes.25,29
Like many diseases, cancer is a multifactorial pathogenesis with risk factors that include poor nutrition, obesity, inflammation, and physical inactivity. Individuals with high cardiorespiratory fitness levels have a 45% reduced risk of total cancer mortality when compared with unfit patients.26,30 The mechanisms of this finding have not been established and are likely to include decreased insulin and glucose, reduced adipose tissue, altered adipocytokines (less leptin and inflammation), and improved immune function. The combinations of these factors may attenuate cancer risk and promote survival.
Regular physical activity in older adults can improve cognitive function and decrease the risk for developing Alzheimer disease. A reduction is found in the general deterioration of the gray matter in the frontal, temporal, and parietal lobes representing correlation between physical activity and reduction in brain aging and neuron loss.27,31
Depression and anxiety disorders are some of the most prevalent mental health disorders in the United States, with as many as 18% of adults demonstrating symptoms. Exercise has been shown to reduce symptoms associated with these disorders and has the potential to lessen the dependability on psychopharmacology.28,32 Additionally, a Cochrane review found exercise to be as effective at reducing depression symptoms when compared with psychological and pharmacological therapies.29,33
Approaches to Physical Activity Counseling
Despite evidence for the cost-effectiveness of physical activity counseling in primary care, only one-third of patients report that they received physical activity counseling by their primary care physician (PCP).30-32 Major barriers to physical activity counseling include the lack of resources, including time, skills, and reimbursement. 33
PCPs face numerous barriers to counseling their patients on a variety of preventive care issues including physical activity, but time limitation is the most significant issue as PCPs try to address multiple or complex medical issues. On average, PCPs address 3 medical issues per patient visit, with slightly higher averages for elderly and diabetic patients. 34 Despite these limitations, PCPs are ideally situated to provide initial and introductory physical activity counseling because of their ability to reach a large segment of the overall population, their role as a trusted source of health information for individuals, and the range of other health professionals available within clinics.33,35,36
Patients also have barriers that may limit their ability to participate in regular physical activity. In a study of older adults, prominent barriers to physical activity participation were physical limitations, mainly resulting from health conditions or aging, lack of professional guidance, and inadequate distribution of information on available and appropriate physical options and programs. 37 Younger patients more commonly do not have the resources for child care and have other impediments such as lack of time, energy, and willpower. 38 Other commonly identified barriers are embarrassment over body image, lack of knowledge of the benefits of exercise, the feeling that exercise is inconvenient or boring, and the lack of self-motivation or self-management skills. 1
Brief exercise training counseling is an efficient, effective, cost-effective means to increase physical activity and exercise training and to bring considerable clinical benefits to various patient populations. 39 For counseling to be most effective, a patient’s level of adopting to a new behavior should be assessed by identifying their current stage of change: precontemplation, contemplation, preparation, action, and maintenance. 40 This assessment allows the provider to focus their efforts on patients who are prepared, engaged, and ready for change. If the patient is amenable to changes, tools such as SMART goals can be utilized: Specific, Measurable, Attainable, Relevant, and Time-bound measures. 41 Additionally, individual feedback is more effective, and one-on-one discussion in an outpatient setting is an appropriate way to deliver this information. 42
As previously noted, individuals benefit from at least some regular physical activity, lending support to the concept of “some is better than none.” 39 Therefore, patients should be encouraged to do what they are able (or perceive they are able) to do, and adding to this over time can help. The message should be simple and clear, specific, and realistic. 39 For instance, expecting a patient who is not currently physically active to start running 40 minutes 3 times a week is unrealistic. Instead, the patient should be directed to initiate walking or light jogging with a goal of 10 to 20 minutes 3 d/wk, which is a more reasonable and achievable initial goal.
Other methods are available and should be considered as the physician incorporates counseling of physical activity into their care of patients. An understanding and use of behavioral change is important. For instance, the theory of planned behavior where patients’ attitude, behavior, and intention to change are balanced with their perception of control over change methods to assist may provide the physician a better understanding regarding how best to assist patients with behavioral changes. 39 The physician should provide clear short-term goals. For instance, set a goal of completing 3 to 4 days of regular exercise or 1 pound of weight loss over 1 to 2 weeks rather than 30 to 40 pounds of weight loss as the goal over the next year. Goals should be relevant to the patient and their medical history, keeping in mind possible physical limitations. The clinician should emphasize internal motivating factors, such as discussing the internal challenge associated with these goals and the joy of taking measures to improve one’s health. Social support should be encouraged to assist with goals. 38 Self-monitoring should also be encouraged.
Physical activity level could be adopted as another vital sign. 41 Although this change may be difficult in common practice because of time constraints, incorporating a question about physical activity into the routine flow of patient care would allow consistent evaluation of levels. Additionally, this vital sign sets the stage for the use of the physical activity prescription.
The physical activity prescription is another method used to increase physical activity and has improved patient-reported quality-of-life measures. 43 Adherence to physical activity on prescription is similar to adherence to other treatments for chronic diseases. 44 Such a prescription should include type of activity, time, frequency, and intensity.
More recently, smart phones have the ability to greatly influence behavior and may be useful in increasing the level of physical activity in patients.42,45 Apps are constantly accessible to and adjustable for the user. 42 An added benefit of some apps is that they can alert patients if they have not achieved their physical activity goals for the day.
In the future, apps and computer-based interventions will have an even greater capacity to help facilitate and support change in physical activity levels. Most apps, however, are not currently based on the application of behavioral theory (such as cues to action, vicarious modeling, and reinforcement). 46 Applying behavioral theory may increase the cost of the app; however, benefits are more likely to be seen in the long-term. 46 The results from a Cochrane study show that tailored web-based approaches seem to be the most effective; however, most studies did not evaluate long-term outcomes (beyond 12 months). 47 Web-based tailored interventions may improve their effectiveness by enhancing patient participation and helping individuals maintain changes over time.46,47
Finally, the physician should consider the use of other health professionals to assist. Health coaches, behavioral health providers, personal trainers, and others have a role in physical activity promotion.
Overcoming Patient Barriers to Physical Activity
To assist with counseling, the PCP should assess and address the patient’s specific barriers to physical activity and counsel patients about the most common general barriers, such as lack of time, knowledge, and motivation. Concerns regarding lack of time can be addressed by incorporating physical activity into our daily lives, such as walking, riding a bike to work, parking the car farther away from one’s destination, taking the stairs instead of the elevator, or exercising while watching television or reading a book. Additionally, reminding patients about the significant health benefits of doing just some physical activity, such as 15 minutes of brisk walking per day, is helpful. 48
Increasing social support, providing detailed planning, and helping patients overcome the pain and fatigue associated with exercise are also helpful in overcoming patient barriers to exercise. Several studies have found that people with good social support are more likely to engage in physical activity, especially when it comes from family members.49,50 When a person finds someone who shares the same goals, they can assist each other with adhering to the routine. Encouraging patients to announce their goals to their friends makes them accountable. Some people form support groups and meet to report their periodic progress.
Detailed planning on “what, when, and how” is an essential component of success when attempting to achieve an exercise goal. As previously described, the SMART goal tool is a popular and easy-to-remember mnemonic that can be used as a framework for goal setting. Another effective tool is the Intention Implementation.51,52 The idea of this tool is that creating a statement in the form “if . . . , then . . .” makes behavior more automated and likely to be executed.
Teaching patients how to balance the unpleasant and the pleasant sensations of exercise can help them overcome any pain and fatigue barriers. Unpleasant sensations related to exercise can be regulated by appropriately selecting the frequency, duration, and intensity of the workouts, so it is more bearable, and increasing the load gradually. Patients should be reminded that some pain and fatigue is expected and, in correct amounts, should be anticipated and perceived as signs of improved physical conditioning. Interestingly, studies support the use of physical activity for effective treatment of chronic pain.53,54 Additionally, the PCP should have patients focus on the positive emotions produced by exercise that can counterbalance the unpleasant feelings. Further emphasis on the positive emotions associated with exercise, including experiencing a “runners high,” socializing with friends during exercise, or feelings of accomplishment after an exercise session, may be beneficial. These emotions can be harnessed to drive and engage patients in further physical activity. 55
In conclusion, physical activity provides health benefits in terms of overall patient mortality and morbidity as well as addressing specific medical conditions. There are numerous benefits and barriers present, and the PCP should understand them and use the information to better counsel patients regarding the benefit of and need for regular physical activity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.