
Abstract
One theme of the article (“Time for Lifestyle Medicine to Take Injury Prevention Seriously,” by Teitge and Francescutti) that should resonate with contemporary injury prevention proponents—whether they are researchers, practitioners, policy makers, or advocates in the public health arena or providers, administrators, and patient advocates in the health care arena—is the need for an increased injury prevention focus among health care providers. In particular, the call for providers to link injury prevention approaches and tools to the clinical care of patients is both noteworthy and compelling. However, the authors’ description of the current injury experience in the United States fails to acknowledge important changes over the past decade and a half that have had an impact on the injury prevention roles of providers. Plus, the notion that progress in injury prevention has been limited in the 3 decades since the publication of Injury in America, undervalues the advances that have occurred.
Keywords
‘However, the authors’ description of the current injury experience in the United States fails to acknowledge important changes over the past decade and a half that have had an impact on the injury prevention roles of providers.’
One theme of the article “Time for Lifestyle Medicine to Take Injury Prevention Seriously,” by Teitge and Francescutti, that should resonate with contemporary injury prevention proponents—whether they are researchers, practitioners, policy makers, or advocates in the public health arena or providers, administrators, and patient advocates in the health care arena—is the need for an increased injury prevention focus among health care providers. In particular, the call for providers to link injury prevention approaches and tools to the clinical care of patients is both noteworthy and compelling. However, the authors’ description of the current injury experience in the United States fails to acknowledge important changes over the past decade and a half that have had an impact on the injury prevention roles of providers. Plus, the notion that progress in injury prevention has been limited in the 3 decades since the publication of Injury in America undervalues the advances that have occurred.
An Elephant in the Room: Changes in the Injury Landscape
The injury landscape in the United States has changed substantially since 1985, when Injury in America 1 was published. For example, heading into the second half of the decade of the 1980s, the leading causes of unintentional injury death were motor vehicle crashes, falls, poisonings by solids/liquids, fires and burns, and drownings.2,3 By 2013, the annual number of motor vehicle crash deaths had substantially declined, whereas deaths by poisonings and falls had substantially increased (Table 1). 3
Leading Causes of Unintentional Injury Death, United States: Number of Deaths, 1985, 1999, and 2013. 3
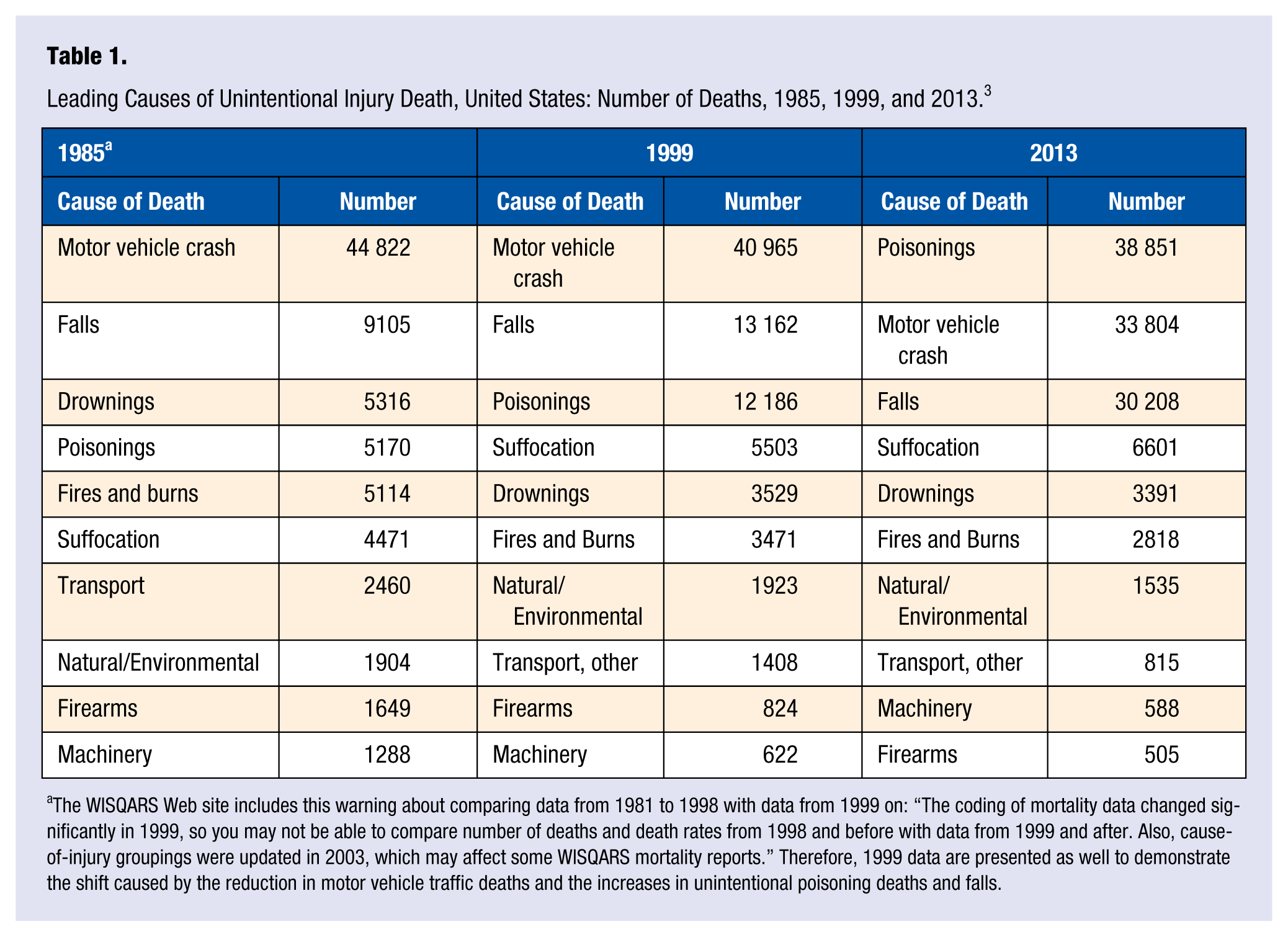
The WISQARS Web site includes this warning about comparing data from 1981 to 1998 with data from 1999 on: “The coding of mortality data changed significantly in 1999, so you may not be able to compare number of deaths and death rates from 1998 and before with data from 1999 and after. Also, cause-of-injury groupings were updated in 2003, which may affect some WISQARS mortality reports.” Therefore, 1999 data are presented as well to demonstrate the shift caused by the reduction in motor vehicle traffic deaths and the increases in unintentional poisoning deaths and falls.
So the authors neglect to mention the epidemic of drug overdose deaths that has driven increases in unintentional poisonings since the late 1990s in the United States, Canada, and other nations in North America and around the world. Nearly 92% (35 633) of the unintentional poisoning deaths reported for 2013 were attributed to drugs, 3 and as others have noted, a large proportion of the drugs causing the increase in unintentional overdoses for the past decade and a half have been prescription drugs, particularly opioid painkillers. 4
Another injury cause that has produced increased numbers of injury deaths during the past decade and longer is falls, particularly among older adults. From 1999 to 2013, the number of fatal falls increased among adults 65 years of age and older by more than 250% (10 097 to 25 464). 3 The aging of the post–World War II baby boom generation may partly explain the increased numbers, though the number of fall-related deaths per capita has nearly doubled over that 14-year time span as well. 3 Numerous risk factors have been implicated in the ballooning levels of fall risk faced by adults as they age, including lack of physical activity, frailty, gait and balance changes, polypharmacy, chronic medical conditions, vision problems, depression, poorly designed and unforgiving living environments, lack of social support (isolation and neglect), history of falls, and fear of falling. 5
These shifts must be acknowledged because they point to additional injury prevention roles for health care providers.
More Injury Prevention Roles for Health Care Providers
Prescription Drug Overdoses
Health care providers can play multiple roles in preventing prescription drug overdoses, including, first and foremost, the adoption of best practices in pain management and opioid prescribing and increased awareness of precautions necessary to prevent diversion of opioids to nonmedical use. Although in some states professional health boards have added continuing education requirements that include training in appropriate prescribing practice, pain management, and drug diversion awareness, in the absence of such requirements, providers can proactively seek guidance, courses, and workshops that address these important topics. Evidence-based screening tools, such as SBIRT (Screening, Brief Intervention, Referral to Treatment), implemented at provider-patient points of contact, whether in hospitals, emergency departments, urgent care facilities, clinics, or private practice, can provide “early intervention and treatment to people with substance use disorders and those at risk of developing these disorders” according to the Substance Abuse and Mental Health Services Administration (SAMHSA). 6 Also, coprescribing the opioid antagonist naloxone to patients initiating opioid therapy for pain can provide patients and their family members with a safeguard—a proven antidote that works by reversing the respiratory depression produced by opioid intoxication. 7 Other important provider prevention efforts include checking state prescription drug monitoring programs to avoid inadvertently prescribing opioids to individuals engaged in doctor shopping and other drug diversion activities that may be fueling their own or others’ dependences and risks 8 and providing patient education regarding the risks inherent in the use of opioids and other potentially dangerous controlled medications. 9
Falls Among Older Adults
Health care providers can also play multiple roles in the prevention of falls among older adults, including screening patients for fall risks (as Teitge and Francescutti note), 5 avoiding overprescribing medications or combinations of medications that may induce dizziness or are known to compromise balance and alertness, 10 and referring patients to exercise or physical therapy programs. 11 For other potential interventions that could be accomplished at the point of contact between providers and patients, such as counseling and education, the evidence of effectiveness is limited. 11
Screening for injury risk is one particular role for health care providers that cross-cuts a number of injury causes. Opportunities exist for providers to interact with patients not only via direct probing conversation, but also via the use of screening methods and instruments from among a growing set of validated tools—for example, instruments that screen for the potential presence of substance abuse, 6 intimate partner violence, 12 fall risks, 5 depression, 13 self-harm and suicidality,14,15 and so on—to enable them to identify at-risk patients, educate and counsel them and their family members, and refer them to specialists and providers who are equipped to suggest or implement evidence-based programs and interventions.
“Limited Progress” or Progress Along With New Challenges?
Reflecting on the 1985 Injury in America publication, Teitge and Francescutti declare that “Our progress since then has been limited.” However, the notion that progress has been limited because the overall toll of injury remains largely undiminished from 1985 aggregate levels (1 in 10 deaths attributed to injury) belies the fact that progress has been made in reducing injury and deaths from specific causes (as the authors note in the case of motor vehicle morbidity and mortality), whereas injuries and deaths resulting from other causes have increased or emerged (eg, the opioid overdose epidemic).
In addition to decreases in motor vehicle crash deaths, there have been steady declines in both numbers and rates of fatal and nonfatal occupational injuries. Work-related fatal injuries decreased from 1992 (6217) to 2013 (4585) by more than 26%. 16 The rate of fatal work injuries declined from 2006 (4.2 per 100 000 workers) to 2013 (3.3 per 100 000) by more than 21%. 16 The Centers for Disease Control and Prevention (CDC) named both motor vehicle safety and workplace safety improvements as 2 of 10 great public health achievements of the 20th century. 17
Other “success stories,” highlighted in the book While We Were Sleeping: Success Stories in Injury and Violence Prevention by David Hemenway 18 include the following:
The increasing use of bicycle helmets and the corresponding reduced likelihood of bicycling head injuries. Wearing helmets can reduce the likelihood of bicycling head injuries by 60%. In 1990, the state of Victoria in Australia enacted a law mandating helmet wear for bicyclists. As compliance with the law increased (up to 83% by 1992), bicyclist head injuries dropped by 70%. 18
Decreased suicide rates in the US Air Force. By implementing a program aimed at decreasing stigma related to seeking help and enhancing understanding of mental health across the ranks, suicide fell from an annual rate of 16.4 suicides per 100 000 in 1994 to 3.5 in 100 000 among US Air Force personnel in 1999. The program—which was endorsed by the Chief of Staff and other top leadership throughout the Air Force—was also associated with a decline in domestic violence and homicide. 18
The reduced risk of fatalities resulting from plane crashes in the US airline industry. Through a systems approach to airline safety that includes in-depth investigations of all incidents, documentation and analysis of near misses, the use of expert observers and sophisticated simulators, and other approaches, “the yearly average number of fatalities per billion miles on passenger and cargo airlines has fallen dramatically each decade . . . totaling 99.9 percent in eight decades.” 18 (pp132) The trend continued from the 1980s through the decade of the 2000s, with fatalities per billion miles dropping more than 4-fold, from 0.9 (1980s) to 0.2 (2000-2006). 18
Injury prevention has evidenced significant progress in the United States in the 30 years since 1985, not only in reduced fatal and nonfatal injuries but also in improved infrastructure and funding. For example, the foremost recommendation made by the Injury in America panel in the mid-1980s was the need for “the establishment of a center for injury control within the federal government.” Since then, the National Center for Injury Prevention and Control was created in 1992. 19 CDC extramural funding levels for unintentional injury had reached $88 million by 2014. 20 The CDC’s Violence and Injury Prevention Program (VIPP), which funds states engaged in injury prevention activities, and the Injury Control Research Center (ICRC) programs were initiated, providing injury prevention funds for VIPP programs (currently in 20 states) and ICRC programs (currently 10 centers in the United States) that focus on leading causes of injuries in the United States. 19 National Institutes of Health (NIH) funding for injury exceeded $400 million in 2014 and is expected to grow to nearly $420 million by 2016. 21
Suggesting the increased involvement of health care providers in injury prevention will help foster an important and timely discussion. Increases in the number of providers who fill screening, counseling, and referral roles to address injury risks among their patients will contribute to higher awareness among patients and their families, opportunities to intervene through counseling, education and referrals, and ultimately reduced risk. Teitge and Francescutti are to be congratulated for raising this discussion in Lifestyle Medicine.