
Abstract
Unintentional injury remains a leading health problem in developed nations, making injury prevention imperative. Practitioners are primary stakeholders in the injury prevention process but rarely can devote significant time to complicated prevention efforts. Furthermore, theory-based approaches to support injury prevention are less common than atheoretical approaches. We propose a simple method for injury prevention grounded in concepts found in antecedent models. Barriers, attitudes, social context, and environmental factors (or BASE) are suggested as a simple injury prevention model practitioners can follow when working with patients. We present each component of BASE and offer examples of how the approach can be applied to risk factors associated with several types of injury risk behavior.
BASE offers a simple synthesis of some critical aspects of injury antecedent models that practitioners can easily remember and implement without spending much time.
Unintentional injury is a significant health problem in the United States. Among individuals between the ages of 1 and 44, unintentional injuries were the leading cause of death and the third leading cause of death across the lifespan in 2018. 1 An additional 26 million nonfatal unintentional injuries occurred in 2018. 1 Preventing injury risk behaviors and reducing the greater impact of unintentional injury on society remains imperative for reducing the burden of unintentional injury on society. Health practitioners are primary stakeholders in the problem of unintentional injury and can play a part in injury prevention.2,3 However, practitioners do not generally have a significant amount of time to devote to prevention efforts and theory-based approaches to assist practitioners are lacking. 4 Our goal is to provide a simple method for injury prevention applicable in a short amount of time. We first turn to the process of how injuries unfold.
Unintentional injuries and risk behaviors emerge from a process. Researchers have examined the etiological factors involved in this process for decades and have identified important risk factors. Some elements are environmental, while others are intrapersonal, for example, sex differences, 5 personality characteristics, 6 cognitive development, 7 and misperception of ability.8,9 Such studies point to injury as dependent on a cluster of predictive risk factors. However, we must be mindful that the process preceding injury risk behaviors is not merely a collection of orthogonal risk factors. Instead, a perhaps more appropriate perspective is to view injuries as resulting from a dynamic antecedent process prior to an injury event comprising many factors including risk behaviors themselves.
Grouping Antecedents in Useful Ways
Researchers have used various approaches for explaining and understanding the antecedent process preceding injury risk behaviors. Each of these approaches group factors in ways that are understandable and practical to apply. Some common examples are the Haddon matrix, the theory of planned behavior, the stages of change model, and the Health Belief Model.4,10,11 To better illustrate one way the antecedent process can be modeled, consider the Haddon matrix. Haddon conceptualized injury as a process of unfolding antecedents consisting of factors described in the epidemiological triangle: host, agent, and environment. The interactions between host, agent, and environment are examined before, during, and after an injury event. By applying the epidemiological triangle at various stages of an injury event rather than one, our understanding of injury etiology improves by multiplying the contributing factors detected by the observer.12,13 Health practitioners have traditionally treated injuries after an event, but understanding antecedent processes can help practitioners more effectively reduce injury.
A recently introduced framework for understanding the psychological process preceding injury risk behavior provides another example of antecedent modeling. Researchers proposed a risk appraisal framework to describe the evaluative phase preceding injury risk behaviors. 14 In this evaluative phase, one appraises the risk involved in a behavior and any means of mitigating risk. The risk appraisal framework describes this process based on environmental context, personal experience with the behavior, social forces surrounding behavior, and personal strategy for risk mitigation. An appraisal using these four factors leads to a sense of efficacy related to performing the risk behavior, which determines whether the behavior is enacted. The risk appraisal model is uniquely suited to injury risk behaviors and inspired by concepts from established approaches, such as the Health Belief Model and the theory of planned behavior.
Yet another way the antecedent process can be understood is through the lens of human error, a concept borrowed from the field of human factors. Human error, simply put, is a mismatch between the intention and the outcome of a behavior. 15 Placing a vehicle in drive, when a driver’s intention is to go in reverse, is a simple example of an error potentially leading to injury. The field of human factors provides various models for examining human error, but one simple model examines three components: human fallibility, context, and barriers. 16 As individuals interact with their environment, their perceptual or physical limitations may inhibit their ability to meet the demands of the situation. When mismatches between human fallibility and context occur, barriers can mitigate or prevent unintended outcomes such as injury. The basic human error model presents a simple framework that can be used for understanding the major factors necessary to predict and prevent injury.
An exhaustive list of approaches modeling antecedent processes is beyond the scope of our effort here but at least two more deserve mentioning due to their presence in the injury literature. The Health Belief Model focuses on understanding how the adoption of preventative behaviors for health threats relies on beliefs about susceptibility, severity, self-efficacy, and the costs and benefits of adopting preventative behaviors. 17 The Health Belief Model has been widely applied to injury risk behaviors such as biking without wearing a helmet 18 and seat belt use. 19 The theory of planned behavior examines the concurrent antecedent roles of subjective norms, attitudes, and perceived level of behavioral control in predicting intention to engage in risk behavior. 4 This approach has seen use in pedestrian safety, 10 seat belt use, 19 and driving behaviors. 20 Each approach predicts intention to engage in health risk or protective behaviors.
Our goal is to provide a simple, theory-based method health practitioners may use for injury prevention in the context of working with patients and without having to devote significant time to the task. To this end, we have selected a set of four components from which practitioners can enact injury prevention. The components are inspired by antecedent models in the literature and draw primarily from the risk appraisal and human error approaches. Barriers, attitudes, social context, and environment (or “BASE”) offer practitioners four components that can be easily identified in individual cases and applied for injury prevention. Below, we outline the four components and describe the role of each in injury prevention. We purposely simplify the concepts in BASE to offer a useful structure to implement in conditions of time constraint and across individual characteristics and injury types.
Barriers
Barriers are any means of preventing risk behaviors or injury after a risk behavior is enacted.21-23 Barriers, as used for our purpose, comprise only physical barriers. For example, a child stair gate might prevent a child from falling down a stairway, eliminating the risk of injury on the stairs. A bicycle helmet prevents serious head injury from occurring after a fall off a bicycle by providing a barrier between the skull and the ground. Some research within human factors expands the concept of barriers and includes more abstract mechanisms such as social, moralistic, and symbolic features.24,25 However, for our purposes of providing a quick tool to curb injury risk, understanding barriers as physical means of preventing injury or injury behavior is sufficient.
Researchers have long used physical barriers as a tool for injury prevention and have examined their efficacy in various contexts. Injury prevention research has provided copious support for using barriers to prevent risk behaviors and prevent injury after risky behaviors. Using gates as a barrier to control access to fall risks, 26 4-sided pool fencing to prevent drowning risk, 27 and child-proof packaging to prevent poisoning 28 are examples of barriers to prevent risk behavior. Safety harnesses for construction-related falls 29 and seatbelts to reduce transportation injuries 30 are examples of successful barrier use to prevent injuries. In sum, physical barriers are established tools for injury prevention by preventing risk behaviors and preventing injury after risk behaviors.
Attitudes
An attitude is a pre-existing disposition that colors a person’s approach to a given behavior. Attitude, as used for our purpose, comprises efficacy and perceived vulnerability in relation to risk behavior; two factors that are established in the injury literature in relation to various health risk behaviors. 31 Efficacy can be described as a sense of capability of enacting and completing the injury risk behavior without being hurt14,32 or a sense of control over the danger involved in a situation. 33 Perceived vulnerability is one’s perception of the personal risk associated with an injury.4,17 The greater the sense of efficacy and the less perceived vulnerability to health risk, the more likely a person will enact the risk behavior.
Attitudes have been in use for some time as predictors of health risk behaviors. Notably, attitude toward risk behavior is an important concept in theories such as the theory of reasoned action and the theory of planned behavior.4,34,35 Research employing the theory of planned behavior often finds attitude to be a significant predictor of intention to engage in injury risk behavior. 10 Essentially, how an individual regards a particular risk behavior partly governs the likelihood of engaging in that behavior and is an important concept to consider in the context of external factors.
Social Context
Social context refers to the various influences that encourage or discourage injury risk behavior emerging from interaction with others. Social context, for our purposes, includes proximal group influences and the demonstration of risk behaviors by others. These two categories provide a multitude of factors with the potential to increase the likelihood of injury and have rich empirical support from the injury literature. Peer and social norms, 36 family context, 37 and safety culture 38 are all proximal group influences linked to injury risk. Other research has drawn a clear line between injury risk and the encouragement or demonstration of risk behaviors by others. 14 People may imitate risk behaviors performed by others immediately or later from memory. Basically, the social component of BASE refers to the ways behavior is impacted by group culture and the observation of similar behaviors in others.
Social forces are part of the context in which injury risk behaviors occur. We can offer several examples. Peer social norms have been the targets of injury prevention among children. 36 Among adults, supervisors and coworkers form a social context modeling risk-taking behavior in the workplace. 39 Driving while intoxicated 40 or speeding 41 are examples of behaviors open to social influence among drivers. Social context is established as a category of risk factors in injury etiology and plays a role in certain antecedent models. 14
Environment
Environment is the physical context offering opportunities to engage in injury risk behaviors. 14 In terms of etiology, environmental context can encourage or discourage risk behaviors. 42 For example, long straight sections of roadway invite drivers to speed, but curved sections decrease driver speed.43,44 On the other hand, rather than encouraging or discouraging risk behaviors, the environment could simply enable the possibility of risk behaviors. For example, stairs can enable the potential for a fall. Therefore, for our purpose, the environment is the current concrete context in which a person operates and in which injury risk behavior is afforded.
Human–environment interactions are essential components of injury and injury prevention. Injury researchers have studied the link between environmental characteristics and injury risk for quite some time now. Environmental features, especially for children, can have far more uses than their intended utilization. 45 Stairs, for example, are typically used to ascend and descend surfaces but may provide a surface of play for children or adults actively engaging in sports such as skateboarding.46,47 Environments may also interact directly with individual characteristics to extract riskier behavior. When a context requires ability judgments on environmental factors at the edges of an individual’s capability, they are more likely to attempt a potentially dangerous action. 9 Prevention efforts aimed at the environmental component of BASE can include removing an individual from a risky environment or introducing barriers into the system. 21
Component Interactions
One might have noticed the four components of BASE can be intertwined. Take barriers and the environment, for example. Barriers exist within the physical context of the environment. A helmet, a handrail, and traction devices are all parts of the environment capable of reducing injury. However, to provide suggestions for barriers, which may not always be present, one must understand the physical environment in which barriers exist. We capture a critical part of the environment potentially overlooked in a time-constrained discussion by including barriers as a separate component in BASE. The components of BASE are intertwined but by thinking of them individually, a more robust method for preventing injury is offered.
Example Applications of BASE
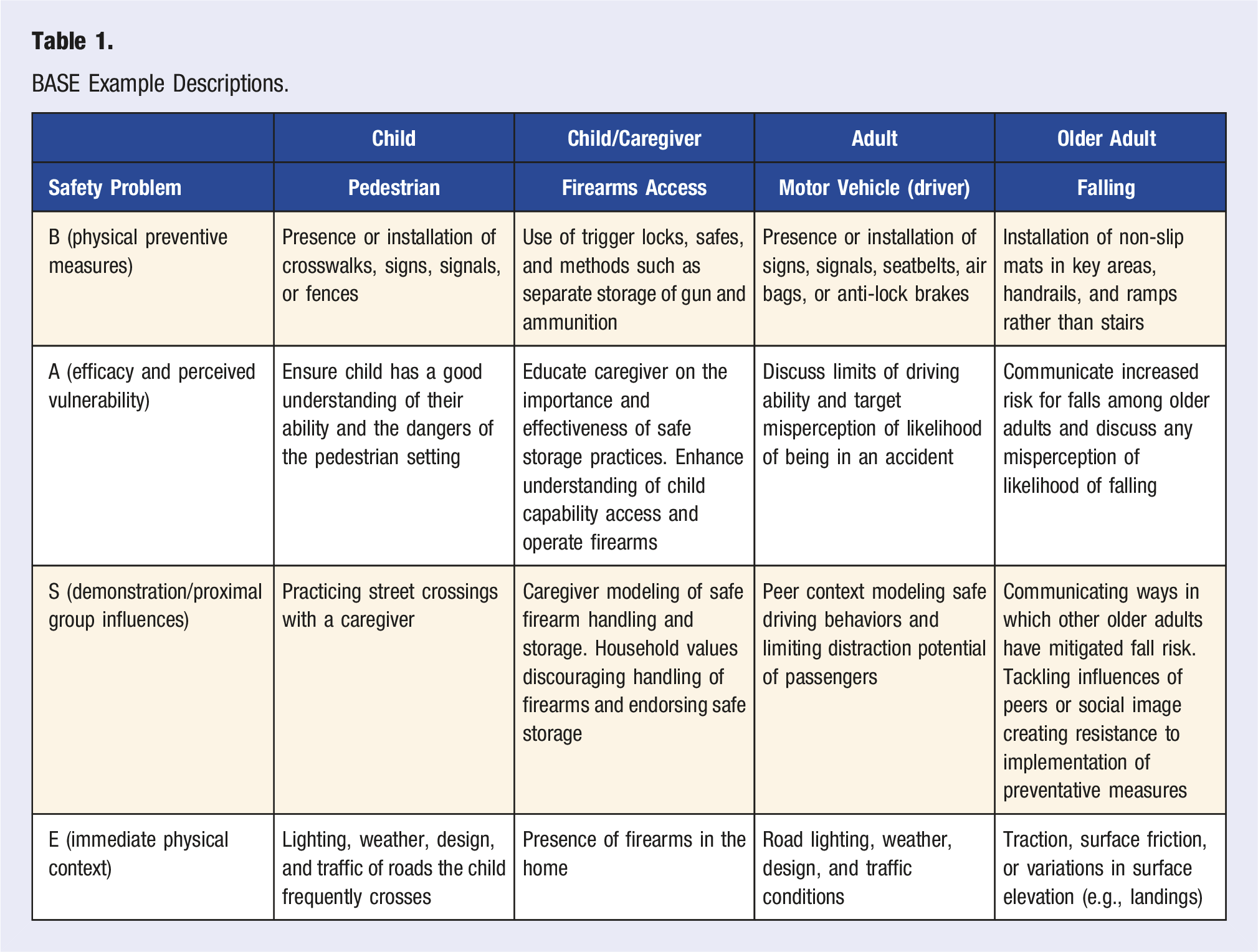
BASE Example Descriptions.
Child Pedestrian
Our first example is pedestrian behavior during middle childhood, roughly ages 5–10. Child pedestrian injury is a significant health problem influenced by multiple risk factors. 48 Quite obviously, higher traffic volume is one significant predictor of increased pedestrian injury risk 49 and other features, such as pedestrian refuge islands, can help mitigate the threat posed by traffic. 50 Among younger children, additional concerns for safety are posed by the nature of parental supervision during times when children are near roadways. 51 Cognitive developmental factors are also at play. Younger children’s attentional capabilities are still developing and often function much less efficiently than adults’. 52 Pedestrian safety is one of the most extensively examined categories of child injury, the nuances of which cannot be fully explored here. However, child pedestrian safety is one topic that can be readily addressed when practitioners find themselves working with parents and children.
Applying BASE, a practitioner is offered various conversation targets concerning child pedestrian safety. A practitioner might start by pointing out how crosswalks or pedestrian traffic signs increase safety if used appropriately (barrier). Ensuring the child has a good understanding of their abilities and the potential dangers of the road environment is another potential discussion point (attitude). The practitioner may also suggest the child take the lead when crossing with a caregiver in order to practice skills while under supervision to harness a powerful social learning opportunity (social). 53 Finally, discussing potentially dangerous environmental characteristics a child should not interact alone with, such as heavy traffic volume, high traffic speed, or low light conditions, could help ensure the child has optimal conditions to interact with traffic safely (environment). 54 Each element of the BASE model provides a target that may interact with each of the other aspects. Practitioners should use their best judgment when identifying what to target.
Child/Caregiver Firearm Access
Child access to firearms stored in the home serves as our second example of how BASE may be applied. Firearms are present in many American homes. 55 Research suggests parents use a variety of methods to store firearms, not all of which restrict child access. 56 Parents may underestimate children’s knowledge of where firearms are stored and ability to access a firearm. 57 Research also suggests the household culture surrounding the purpose of possessing firearms may play an etiological role, potentially deterring reckless behavior. 56 Alternatively, household culture could decrease risk depending on attitude toward safer storage interfering with the intended purpose of a firearm. 58 For example, teaching children that firearms are tools and are for use only in specific circumstances. Children’s access to firearms offers a way for practitioners to target a safety problem couched in the interaction between child and parent.
With BASE in mind, we see how each component can be used to identify ways to increase child safety in homes with firearms. Components need not be addressed in the order in which they are represented in our acronym. That is, we may begin here by simply determining the presence of firearms in the home (environment). If firearms are present, the practitioner may move on by inquiring about the kinds of storage techniques in use in the home (barrier). Caregivers can be educated on the importance and effectiveness of safe storage practices such as trigger locks, safes, separate storage of firearm and ammunition; all examples of effective methods. 59 The practitioner may enhance the caregiver’s understanding of child capability access and operate firearms or the caregiver’s ability to change storage methods (attitude). Indeed, some parents underestimate a child’s capability of accessing and operating a stored firearm. 60 The safety culture in the household should also be assessed (social) by inquiring whether caregivers' model safe firearm handling in front of children because children look to caregivers for examples of how to behave. Taken together, we see here an example of how a practitioner can use BASE to tackle a safety issue relevant to children by working indirectly through the caregiver.
Adult Driver
Our third example concerns an adult driver scenario. Motor vehicle collisions are one of the top causes of unintentional injury and death across the lifespan. 1 Risk factors relating to motor vehicle collisions include individual characteristics and contextual components. 61 Age, personality characteristics, smartphone use, and weather have all been linked to motor vehicle collisions.62-65 Protective factors, such as seatbelts, have been successful in reducing injuries related to collisions. 66 However, for adults, motor vehicle collisions are still a primary source of injury and death.
Similar to the other examples in this section, the practitioner can begin by assessing any component. The practitioner might begin by discussing potentially hazardous environmental conditions. The road condition, lighting, traffic conditions, and the weather could all be potential risk factors for injury (environment). The discussion of environmental factors might lead to a conversation regarding the driver’s ability to prevent an accident and the likelihood of being involved in a collision (attitude). Mitigating factors to injury might also be discussed, such as the use of seatbelts or the maintenance of their vehicle (barriers). A vehicle with functioning brakes, tires with sufficient tread, and using available safety mechanisms in the environment can provide powerful passive preventative mechanisms (barriers). Finally, the practitioner might want to discuss factors such as peer modeling of safe driving behaviors and limiting social distractions (social). 67 Moreover, social distractions do not need to share the same physical environment as the driver; a smartphone can also constitute a social distraction. 68
Older Adult Falls
Our final example, one concerning falls among older adults, reminds us injury prevention is a challenge across the lifespan. Unintentional falls are the 3rd leading cause of injury across the lifespan in the United States, peaking significantly for adults over the age of 65. 1 Some factors responsible for the increase in fall risk for older adults include cognitive and physical decline. 69 Reduction in muscle strength and balance, reduction in cognitive ability, reduced visual acuity, and environmental characteristics such as stairs are all associated with increased risk of falling.70,71 Knowing some of the risk factors, practitioners can begin to reduce the likelihood of falls for older adults.72,73
Much like our firearm storage example above, the practitioner may start by assessing environmental hazards in the home. The presence of issues such as traction problems, surface friction, or obstacles like stairs and landings may first be assessed (environment). Once the practitioner has gained a sense of environmental characteristics in the home, they may suggest barriers for preventing falls. As shown in Table 1, solutions here might include non-slip mats in key areas, installation of handrails, or use of ramps rather than stairs (barriers). The practitioner should at some points discuss increased risk for falls among older adults and identify any misperception of likelihood of falling (attitude). Ways in which other older adults have mitigated fall risk can be included, bringing influences of peers or social image into play (social). Fall risk offers another simple, conversational example of how BASE can be applied. Practitioners need not apply components in the order in which we have used them here but could begin with whichever component they feel is best or emerges naturally from the conversation with the patient.
Conclusion
Medical and public health practitioners are important contributors to the injury prevention process because they have the potential to identify and counteract antecedents. 14 However, practitioners do not have the luxury of spending copious amounts of time on injury prevention. BASE offers a simple synthesis of some critical aspects of injury antecedent models practitioners can easily remember and implement.
In the preceding sections, we outlined four examples to illustrate how BASE can be applied. Our examples are merely a small subset of numerous ways BASE could be applied; actual application of BASE could take many forms. We must also note the process of applying BASE can emerge organically from the conversation with a patient and components may be applied in any order the practitioner feels is appropriate. Our hope is practitioners can make use of the simple method afforded by BASE to enact basic injury prevention or, at the very least, be inspired to employ prevention tactics using antecedent concepts in general.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.