
Abstract
Nearly 1 in 4 women and 1 in 13 men experience intimate partner violence (IPV) at some time in their life. Victims of IPV suffer significant negative health consequences because of the physical, sexual, and emotional abuse they have experienced. Elevated risks have been observed for a wide range of adverse health outcomes. Research has substantially improved our understanding of the physiology that underlies the association between violence victimization and an array of adverse health outcomes. Given the high prevalence of IPV and the associated medical consequences and costs of IPV, it is critical to address this public health problem. IPV prevention and intervention can substantially decrease the public health burden of IPV and greatly improve the health of patients being seen in the medical system. Primary care and family physicians are in an ideal position to diagnose victims of IPV and provide the victims and their families the appropriate care that is needed. However, to accomplish this goal, there remains an urgent need to integrate information on IPV into medical and health care curricula, and to train future physicians and other health care providers about the pervasiveness of IPV and the far-reaching implications for patient health.
If this were an infectious disease, we would have a treatment center in every neighborhood. There is a huge disconnect between the prevalence of domestic violence and what is done in the health system.
An astonishing number of adverse health outcomes have been linked to intimate partner violence (IPV) victimization. This has important implications for clinicians given the high prevalence of IPV. The most current national-level data are from the 1995-1996 National Violence Against Women Study (NVAWS), indicating that 24.8% of women and 7.6% of men reported experiencing physical or sexual IPV during their lifetime. 1 The prevalence rates for the 12-month period before the survey were 1.5% and 0.9% for women and men, respectively. More recent data from 18 states participating in Centers for Disease Control and Prevention’s (CDC) 2005 Behavioral Risk Factor Surveillance System (BRFSS) indicate that 23.6% of women and 11.5% of men reported experiencing physical or sexual IPV during their lifetime. 2 Prevalence rates for the 12-month period before the survey were 1.4% and 0.7% for women and men, respectively. A decade later, the BRFSS prevalence rates are remarkably similar to NVAWS rates, suggesting the need for further primary prevention efforts, including comprehensive and integrated approaches at the individual, relationship, community, and societal levels.
“Victims of IPV (also referred to as domestic violence) suffer significant negative health consequences because of the physical, sexual, and emotional abuse they have experienced.”
Rates of IPV reported in studies conducted in primary care and other medical settings are generally higher than what is reported in population-based surveys. IPV victims are found in large numbers across a wide range of clinical settings, including primary care, internal medicine, obstetrics and gynecology, gastrointestinal clinics, and family practice. 3 In some instances as many as 1 out of every 2 or 3 patients reported experiencing some form of IPV during their lifetimes. For example, estimates of the lifetime prevalence of IPV among women who sought treatment in primary care settings or family practice clinics, range from 35.0% to 50.0%.3-11 Lifetime prevalence estimates for emotional abuse in these same medical practices ranged from 14% to 72%. Twelve-month prevalence estimates for physical, emotional, and sexual violence have been shown to be as high as 33.6%, 44%, and 26%, respectively.
Adverse Health Consequences Related to Intimate Partner Violence
Intimate partner violence occurs among women and men, opposite and same-sex partners, and cohabiting and noncohabitating partners. It includes threatened, attempted or completed physical or sexual violence, emotional abuse, or stalking by a current or former spouse, boyfriend or girlfriend, or dating partner. 12 Although both women and men experience IPV, adult women experience higher rates of IPV victimization and are much more likely to be injured or killed by an intimate partner, compared with men.13,14 Because of the higher burden of IPV on women compared with men and the higher impact of IPV that women experience, the vast majority of research has been focused on IPV against women. Thus, many of the findings presented in this review are derived from studies of women who have experienced IPV. It is important to keep in mind, however, that both women and men can be affected by IPV and much of the findings presented in this manuscript may be relevant to both female and male patients.
Victims of IPV (also referred to as domestic violence) suffer significant negative health consequences because of the physical, sexual, and emotional abuse they have experienced. The most visible and obvious consequences of IPV are physical injuries. Each year, millions of people in the United States, predominantly women, suffer acute IPV-related injuries, ranging from relatively minor injuries to disfigurement, permanent disability, life-threatening injuries, and death. For women alone, IPV results in more than 2 million injuries and 1300 deaths each year. 15 More than 1 out of every 4 women who are injured by an intimate partner require medical care. 16 Many of these injuries are caused by blunt force trauma to the head, face, and neck.17,18 Between 81% and 94% of women being seen for IPV-related injuries have facial injuries.19,20 An estimated 67% of women who are treated in emergency rooms as a result of IPV have head injuries and 1 out of every 3 women has experienced loss of consciousness at least once as a result of IPV. 16 It has been estimated that between 54% and 68% of women seeking emergency care had been strangled by an intimate partner.21,22 Although traumatic brain injuries and strangulation injuries are common, they are frequently undiagnosed.21,23 At the extreme end of physical IPV is death. Although homicides are relatively rare, compared with the other consequences of IPV, the United States has the highest rate of intimate partner homicides among the 25 wealthiest countries in the world (1.2 homicides per 100 000 people) with approximately 1500 murders each year.13,24,25 Several studies have found that between 42% and 66% of women who were killed by their intimate partner sought medical care in the 12 months prior to their murder.26-29 Thus, intervention opportunities were likely to have been missed. One research review of pregnancy-associated homicides estimated that as many as 66% were perpetrated by an intimate partner; many of these victims had also recently used health care prior to their death but had not been identified as victims of IPV. 27 Beyond injuries and death, an increasingly large body of evidence now indicates that IPV has both direct and indirect effects on the health of victims.
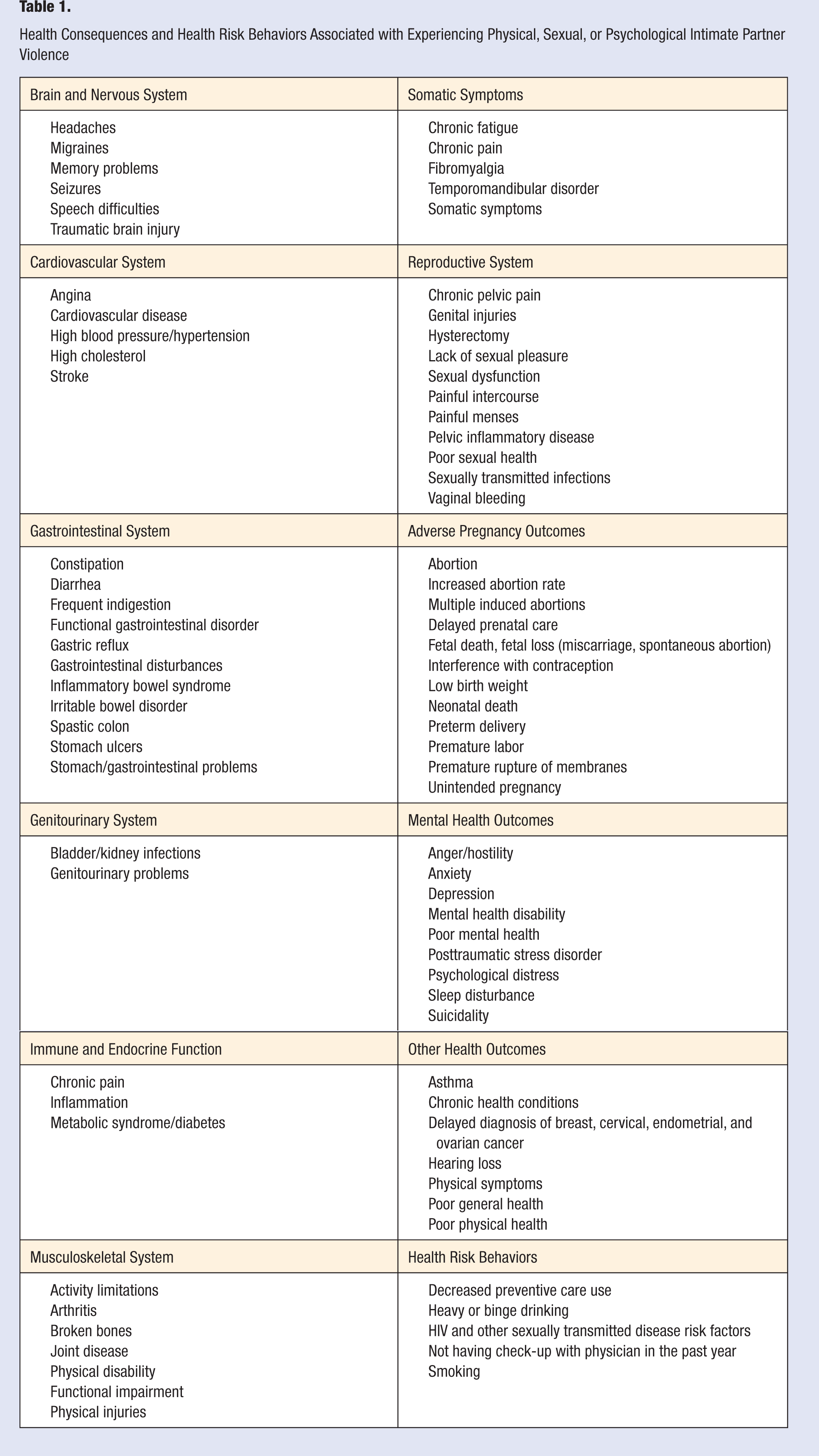
Researchers from a wide range of disciplines have evaluated the health consequences of physical violence, sexual violence, and emotional abuse in dozens of populations; many of the findings have been replicated in multiple studies (Table 1). Elevated risks have been observed for a wide range of adverse health outcomes affecting the brain and nervous system,4-6,21,30-32 cardiovascular system,4,5,7,14,33,34 gastrointestinal system,4,6,35 genitourinary system,4,30 immune and endocrine system,32,35-38 musculoskeletal system,4-6,14,39 reproductive system,4,6,8,40-42 adverse pregnancy outcomes,43-50 and other health outcomes.* A number of somatic syndromes,4-7,35,51,52 adverse mental health outcomes, † and health risk behaviors have also been linked to IPV. ‡ Additionally, evidence from several studies suggests a dose–response effect of violence; as the frequency and severity of violence increases, the impact of the violence on the health of victims also becomes increasingly severe.30-32 Furthermore, although physical, sexual and psychological violence each have significant mental and physical health consequences, women who have experienced multiple forms of IPV are more likely to develop serious health consequences. 33
Health Consequences and Health Risk Behaviors Associated with Experiencing Physical, Sexual, or Psychological Intimate Partner Violence
Physiologic Mechanisms Linking Intimate Partner Violence With Adverse Health Consequences
During the past 2 decades, research has substantially improved our understanding of the physiology that underlies the association between violence victimization and an array of adverse health outcomes. Although a complete review of this extensive literature is beyond the scope of this article, several reviews in the literature provide excellent overviews of the links between disease and the complex and interconnected neural, neuroendocrine, and immune responses to acute and chronic stress.33,35,51,61-66 A brief review of selected research findings will provide information that is useful to understanding some of the biologic mechanisms that link IPV and a wide range of adverse health outcomes.
A large body of work by McEwen and others regarding homeostasis, allostasis, and allostatic load lays the foundation for understanding the protective and damaging effects of acute and chronic stress and the multifaceted and interconnected links between stress and disease.61-66 Homeostasis is the physiologic regulation of the body that is required for survival (eg, body temperature, blood pressure, heart rate, pH balance). 62 Allostasis, which means “maintaining stability through change,” 67 is critical to survival and is defined as the ability of the body to increase or decrease vital bodily functions in response to everyday life challenges and stressors (eg, hunger, heat, fatigue, noise). 61 The responses to both acute and chronic stress are mediated through the brain, autonomic nervous system, and the neuroendocrine system. The primary organs and tissues that are affected by the stress mediators are the immune system, the cardiovascular system, adipose tissue, and muscle. 61 During the stress response, the body releases a host of chemical mediators, for example, adrenaline and noradrenaline, cortisol, catecholamines, glucocorticoids, pro- and anti-inflammatory cytokines, serotonin, systemic hormones (eg, insulin), pituitary hormones, and a number of neurotransmitters.63-66
These mediators are interconnected in a network of regulation; when any one mediator increases or decreases, there are compensatory changes in the other mediators.63-66 Whereas this increased physiologic activity in response to challenge is protective in the short run (eg, the release of hormones that act on multiple neural and endocrine receptors to produce the adaptive physiologic fight or flight response), the long-term effects of prolonged stress (eg, increased heart rate or blood pressure over extended periods) take a toll on the human body.63-66 Allostatic load refers to the strain on the brain and the body produced by the prolonged and elevated physiologic activity, changes in metabolism, and immune function; the resulting organ and tissue damage and changes in body function can lead to increased susceptibility to disease. 61 Areas in the brain such as the hippocampus, amygdala, and prefrontal cortex undergo structural changes in response to acute and chronic stress, which has implications for mental health and cognitive functioning. 65 Sustained and acute elevated stress levels have also been linked to cardiovascular disease, hypertension, gastrointestinal disorders, diabetes, cancer, and changes in immune system function.61,65 For example, in response to stress, the immune system can be compromised, exacerbating the spread of cancer and viral infections.68,69 Similarly, elevated levels of cortisol promote elevated insulin production, which can accelerate atherosclerosis. 70 Chronic stress has also been linked to the development of insulin resistance, a risk factor for non-insulin-dependent diabetes. 65
There are both physical stressors (eg, trauma, physical abuse) and psychological stressors (eg, fear, threats, humiliation, disappointment) related to IPV to which the autonomic nervous system, the hypothalamic–pituitary–adrenal (HPA) axis, and the cardiovascular, metabolic, and immune systems respond. 65 These pathophysiologic processes are closely tied to conflict, distress, and safety issues. 65 Anticipation, worry, or hypervigilance in a person who feels threatened or in danger because of past or current experiences with IPV can increase the secretion of stress hormones such as corticotrophin-releasing hormone, cortisol, dehydroepiandrosterone (DHEA), epinephrine, and neruropeptide Y.66,71 Similarly, intrusive memories of past traumas can also cause similar stress hormone responses.66,71,72 Thus, for some individuals, the impact of IPV can continue well after the abuse itself has stopped.
Studies conducted by Kiecolt-Glaser and colleagues found that couples in high-stress marriages have higher levels of circulating pro-inflammatory cytokines and are at increased risk for infectious disease, decreased vaccine effectiveness, and increased wound healing time.73,74 Among adult women in long-term marriages, just 30 minutes of conflict-related discussions was associated with decreased immunological response, and changes in cortisol, adrenocorticotropic hormone, and norepinephrine.74,75
Kendall-Tackett 34 presents evidence suggesting that increased risk for illness may also be a result of chronic inflammation caused by frequently observed sequelae of IPV—depression, sleep disturbances, and hostility. As previously mentioned, those who have experienced IPV have increased risk for a range of adverse health outcomes, including cardiovascular disease,4,5,7,14,33,34 metabolic syndrome, 34 and somatic syndromes.35,51,52 Evidence suggests that these conditions may be caused by increased levels of pro-inflammatory cytokines (eg, interleukin-1β, interleukin-6, tumor necrosis factor-α). 76 Disturbed sleep, common among survivors of violence, also has an enormous impact on immune, metabolic, and neuroendocrine function and the HPA axis. 77 Similarly, the harmful impact of disturbed sleep has been directly measured in a sample of female rape survivors with posttraumatic stress disorder (PTSD). 78 Depression also causes immune dysfunction, suppressing some aspects of immune function while elevating others.79,80 Researchers have also directly measured the biological impact of IPV on the endocrine and immune systems.37,38,81 Similarly, alterations in the HPA axis have been measured among abused women with chronic pelvic pain. 82
Like survivors of child maltreatment, victims of severe IPV may be at risk for long-term health problems well after the violence has ended. 83 A study of daily cortisol levels among women with chronic pain (fibromyalgia and osteoarthritis) found a dose-dependent relationship between cortisol concentration and severity of self-reported child maltreatment and neglect. 84 Long-term hormonal disruption and dysregulation of the HPA axis has also been measured in child survivors of sexual abuse or maltreatment.84-86 Although these findings were among victims of other forms of violence, it is likely that similar stress response mechanisms are being triggered.
In addition to the biologic stress response, there are other factors that are likely to play a role in the link between IPV and adverse health outcomes. For example, some IPV victims try to manage the negative consequences of the abuse through the use of alcohol, prescription medication, illegal drugs, or tobacco. 87 Thus, some of the observed associations between IPV and adverse health consequences may be related to such usage (eg, tobacco and cardiovascular disease). Regardless of the specific biologic mechanisms that directly or indirectly link IPV with a wide array of adverse health outcomes and health risk behaviors, there is no doubt that by preventing IPV there is potential to greatly improve the health of patients being seen in the medical system. Research has also shown that for many survivors who have escaped from violent relationships, the negative health effects diminish over time and their overall health improves. 87
Health Care Utilization and Costs
Victims of IPV have increased health care needs and increased utilization, including increased visits to physicians, pharmacies, and mental health providers, increased surgeries, and increased hospital stays.88,89(p102) In 2003, using the most recent data available at that time (collected in 1995-1996), CDC estimated that more than 807 000 overnight hospital stays and 971 000 outpatient visits that year were directly caused by IPV. 15 Similarly, more than 95 000 ambulance calls and more than 486 000 emergency department visits each year are also directly linked to IPV. 15 An estimated 11% to 30% of injured women seeking emergency care have been injured by an intimate partner. 30 Studies have also demonstrated that as the frequency and severity of violence increases, the use of health care services also increases.4,30,87
Conversely, evidence suggests that victims of IPV may be less likely to seek preventive care. Both women and men who have experienced IPV are also significantly less likely to have had a checkup with a doctor in the past year or seek preventive health care (eg, flu shots, cholesterol checks).14,60 A recent study of women who reported fear and safety concerns reported using fewer preventive care services, including breast examinations, mammograms, cholesterol, blood pressure, cervical, or colon cancer testing. 90 These findings have obvious implications for the overall health of victims of IPV and for health care costs, in general.
Several studies have quantified the increased health care utilization and costs among women with histories of IPV.83,91,92 One study of a large health plan showed significant increased health care usage and costs associated with IPV, with IPV-related costs in excess of $19.3 million for every 100 000 women enrolled in a large health plan. 91 Another large study of a metropolitan group health cooperative compared health care use and costs among women who had experienced physical or nonphysical IPV with women who had not experienced IPV. 83 Women who had experienced physical IPV used significantly more health care services, including mental health, emergency department, hospital outpatient, primary, pharmacy, and specialty care. Utilization was the highest among women who were in ongoing abusive relationships. 83 Annual health care costs were 42% higher among women who were currently experiencing physical IPV, 24% higher among those who had experienced physical IPV in the past year and 19% higher among those who had experienced physical IPV in the previous 5 years. Similarly, health care costs among women who had experienced nonphysical IPV in the past year were 33% higher than women without these experiences. 83 Many women who have experienced IPV continue to use increased levels of service years after the abuse has stopped.30,53
The National Center for Injury Prevention and Control estimated that in 1995, the annual health cost and productivity losses of rape, physical violence, and stalking by an intimate partner were $5.8 billion per year, which included $4.1 billion in direct medical and mental health service costs. 15 When updated to 2003 dollars, the medical and lost productivity costs of IPV exceeded $8.3 billion. 93 These cost estimates substantially underestimate the overall costs of IPV because they do not include expenditures beyond medical care and lost productivity (eg, significant costs related to pain, suffering, and decreased quality of life for the victims, children and other family members, law enforcement, or judicial costs associated with IPV). 15
Universal Screening and Assessment in Health Care Settings
As noted in other articles in this issue, a number of medical associations have issued policy directives and recommendations in support of universal screening for IPV (ie, asking all patients about their experiences with IPV at every visit and providing referrals for services as indicated), including the American College of Obstetricians and Gynecologists, the American Medical Association, the American Academy of Family Physicians, and the American Academy of Pediatrics.94-97 A universal screening approach (defined above) differs from a diagnostic approach where only those patients presenting with risk factors for IPV or signs and symptoms consistent with IPV are asked about their experiences and followed-up accordingly. In 2004, the US Preventive Services Task Force (USPSTF) concluded that there was insufficient evidence to recommend for or against universal screening, citing a lack of strong evidence to support the recommendation, the lack of available efficacious treatment options, and the possibility of unintended negative consequences or harm. 98 In the absence of being able to determine the balance between the benefits and harms of universal screening, the USPSTF pointed to a diagnostic approach stating the clinicians should be alert to the physical and behavioral signs and symptoms associated with abuse and provide treatment, arrange for skilled counseling, and provide information about available local crisis centers, shelters, and protective services. The USPSTF has been criticized for focusing on overt health consequences related to morbidity, disability, and mortality outcomes with less consideration given to the physiologic impact of chronic stress related to experiencing IPV and the resulting health outcomes. 99 As our understanding increases regarding the multitude of biological mechanisms through which physical and psychological stress have a detrimental effect on health, it becomes increasingly evident that health care providers should consider the potential role of stress in the diseases experienced by their patients and furthermore, consider assessing for a previous history of violence when patients show signs and symptoms that are consistent with potential victimization. Because those who have experienced IPV often seek medical attention for health conditions that may not appear to be related to abuse, a better understanding of the potential role of violence may influence the diagnosis and treatment plan.14,34
Barriers to Assessment
Given recent health care reform and the focus on health promotion and disease prevention, it is worth considering the cost and quality-of-life implications when victims of violence are not identified, services are not provided, and interventions do not take place. It has been estimated that health care providers correctly diagnose as few as 1 in 35 patients who are seeking medical care for problems related to IPV. 96 Even when patients present with injuries resulting from abuse, few health care providers ask their patients about IPV.6,96,100-107
It is worth considering the barriers that may be contributing to so few physicians asking their patients about IPV, even when there are signs and symptoms that should trigger suspicion for abuse. James Ferguson, 102 in his 2009 presidential address to the American Gynecological and Obstetrical Society, spoke of IPV and its unacceptable consequences on women as the number one problem to be addressed by gynecologists and obstetricians. Ferguson and others have noted a number of barriers for physicians, including a lack of training; lack of resources/referrals; and the belief that asking about IPV history is an inefficient use of limited time.102,105,106 Another potential barrier includes the physician’s own experiences; 12% to 15% witnessed domestic violence during childhood or experienced IPV at some point in their lives. Sugg and Inui 108 also reported that potential barriers for physicians include: fear of getting overly involved in their patient’s personal issues; feeling they do not have enough time or knowledge to adequately address the issue; lack of comfort with the subject; fear of offending the patient; and sense of powerlessness or loss of control. 108 Additional barriers described by the American Academy of Family Physicians (AAFP) that impede physicians’ recognition of family violence are related to several myths: the misconception that victims are poor, inner city women; violence is rare or does not exist in families that appear to be normal; violence is a private matter; and victims are in some way responsible for their abuse. 96
Although patients who have experienced IPV are distributed throughout the health care system, IPV is particularly important and relevant to primary care, family care, and general practices; such practices are often where victims of IPV can be reached as they seek care for themselves and their families. According to the AAFP, family physicians are not only in an ideal position to identify victims of IPV and provide the victims and their families the appropriate care that is needed, they also are obliged to do so because of the magnitude of the problem. 96 If they are adequately trained to identify and address IPV when patients present with signs and symptoms consistent with IPV, providers in these settings can play an important role in secondary prevention. Because of their training to care for the entire family within the context of the larger community, family care physicians can provide continuity of care, gain patient confidence over time, and provide patient advocacy and appropriate referrals when appropriate. 96 Each health care visit for a patient with IPV provides the potential for secondary prevention, intervention, and provision of referrals to further reduce the adverse health impacts of IPV. Not asking about IPV when patients present with signs and symptoms that should raise suspicion, represents a missed opportunity to decrease risk and increase safety. 6 Furthermore, earlier intervention opportunities may improve health by lessening the long-term negative impacts of IPV.
To facilitate assessment of IPV victimization, the CDC has published “Intimate Partner Violence Victimization Assessment Instruments for Health Care Settings,” a compilation of 34 IPV and 14 sexual violence assessment tools. The purpose of the compilation is to aid practitioners in the selection of instruments to use in health care settings to identify patients requiring additional services and referrals. 109 Several of these tools have been developed by medical organizations (eg, an IPV assessment tool designed by the American Medical Association and a sexual violence assessment tool developed by the American College of Obstetricians and Gynecologists). 109 Additionally, in the recently published second edition of the Violence Against Women Sourcebook, Hamby and Cook 110 provide an overview of assessing for violence victimization to detect the abuse, inform treatment, and provide appropriate referrals. The authors include practical information for health care providers to consider as they develop protocols for specific health care settings and information about current best practices in assessment and subsequent interventions and referral. 110
Educating Health Care Providers About Intimate Partner Violence
In 1985, the Surgeon General convened a workshop on Violence and Public Health, encouraging all health professionals to respond to the problem. 111 One of the recommendations from the workshop was to include education about IPV in the curricula of medical schools and other professional schools throughout the United States. In 1989, the CDC reported that more than half (53%) of 116 surveyed Canadian and US medical schools offered no training on IPV, with an average of less than 3 hours of training devoted to IPV curricula among those who did offer training. 112 Decades later, instructional time and clinical training remain woefully insufficient. 113 The Association of American Medical Colleges and other researchers reported that the amount of time spent on IPV training remains quite limited and the majority of medical textbooks still do not contain adequate information on IPV.114-116 For example, less than 40% of obstetrics and gynecology textbooks or primary care textbooks contain information on IPV. 116 In 2002, the Institute of Medicine (IOM) report “Confronting Chronic Neglect: The Education and Training of Health Care Professionals on Family Violence,” again concluded that physicians were not adequately trained to recognize IPV in their patients and were not fully aware of the negative health impact of IPV or the links between IPV and numerous common chronic illnesses. 117 Similar findings were published in a 2005 review. 113
There remains an urgent need to raise awareness about the pervasiveness of IPV and the far reaching implications for patient health, and to train health care providers to effectively identify, treat, and provide secondary prevention for victims of IPV. 118 To be most meaningful, medical education experts recommend that approaches to integrate IPV training into the medical curriculum (rather than a stand-alone curriculum) are needed and that training should be of an experiential and ongoing nature.102,115
As previously mentioned, one of the biggest barriers to physicians asking about IPV is that they frequently feel inadequate and unprepared to appropriately respond to a patient who reports experiencing IPV. A 2005 study of 928 final-year primary care residents regarding “perceived preparedness” found that 62% of residents reported being prepared to counsel patients about smoking and 53% reported being prepared to counsel patients about diet and exercise, but only 21% reported being prepared to talk about IPV. 119
Several studies have shown that IPV training has a positive impact on the attitude of medical students’ toward IPV as a health care issue, increasing comfort, skill, and efficacy to assist patients who were dealing with IPV and related health outcomes.120,121 Effective programs increase students ability to correctly suspect abuse, encourage student sensitivity and the development of appropriate responses to victims of violence within their future medical practices.112,121 Students also gain experience regarding when and how to ask about abuse with concern and respect; assessing an individual patient’s situation, including the risk of immediate danger; and intervening in a preventive manner.
Beyond teaching in medical school, increasing awareness among practitioners is also important. In 2005, following the 2002 IOM report recommendations, the Academy on Violence and Abuse (AVA) was founded to increase physicians’ awareness that violence is a health care problem and increase their understanding of the potential negative health consequences of undisclosed past or present violence. 122 The AVA Web site provides links to the most recent literature on the health impact of IPV and the underlying biologic mechanisms that are likely to play a role in adverse health outcomes. 122 AVA also works closely with academics to integrate information on IPV into medical and health care curricula. Similarly, the AAFP has several initiatives to decrease family violence, including educational programs for practitioners and is supporting and developing protocols and policies to address family violence in medical settings. 122
Patient Response to Being Asked About Intimate Partner Violence
One of the commonly noted barriers to assessing patients for IPV is the clinician’s concern about offending their patients. 108 Studies of women’s opinions about being asked about IPV indicate that they are not offended.102,108,123-126 Additionally, women reported being grateful that posters and pamphlets with information about abuse and where to go for help are available in waiting rooms, restrooms, and exam rooms.126,127
Women also report higher levels of satisfaction when they are asked about domestic violence and when physicians listen carefully in a compassionate and nonjudgmental manner.128,129 Research also suggests that abused patients may interpret a failure to ask as an indicator that the physician does not wish to discuss abuse which, in turn, is associated with a significant decrease in patients’ satisfaction with their physician. 128 Furthermore, it is important to consider the harm that may occur when patients who are experiencing IPV are not asked about their experiences and not referred for assistance. For example, not asking about IPV when signs and symptoms should trigger suspicion for abuse, plays into the stigmatization of those who experience abuse.
Beyond improving patient–doctor relationships, research suggests that a trusting relationship between a patient and their caregiver can lead to a break in the cycle of abuse and enable the patient to change their circumstances. 130 When IPV is suspected, asking patients about their experiences may itself have a therapeutic effect.107,127,131,132 Furthermore, “simply acknowledging to patients that the abuse they experienced is hurting their health can greatly improve their health.” 133 Some victims of abuse seek services if given information or referrals. 35 Additionally, qualitative studies of abuse victims also indicate that talking to them about IPV can help them to recognize the problem, even if they are not ready to make life changes at that point. 129 If health care providers ask patients about IPV when they present with signs and symptoms consistent with IPV in a supportive and nonjudgmental way, even if they are not ready to disclose, such brief clinical encounters are likely to encourage disclosure at some point.
A growing body of literature also suggests improved health measures for victims of IPV when IPV assessment occurs in health care settings. 104 To be most effective in providing care for patients who are victims of IPV, clinicians should be encouraged to establish and develop relationships with victim’s advocates, rape crisis centers, and domestic violence shelters in their area. Programs that promote interdisciplinary collaborations between service providers are necessary to best meet the needs of IPV victims to provide adequate, appropriate and comprehensive care to IPV victims.101,131,134,135 Evidence suggests that victims who receive integrated and interdisciplinary assistance are more likely to achieve better outcomes than when a more traditional approach is used.74,131,136-138
Primary Prevention
The majority of this review is focused on IPV victimization, health consequences of IPV, and what physicians can do when patients present with signs and symptoms consistent with IPV. However, it is equally important to be proactive and put prevention measures in place to keep IPV from occurring in the first place. CDC’s strategy for preventing IPV is to promote respectful, nonviolent relationships through individual, relationship, community, and societal change. The prevention strategy is organized around the following principals: understanding the development of and ways to interrupt the development of IPV perpetration, improving knowledge of factors that contribute to respectful relationships and protect against IPV, creating and evaluating new approaches to prevention, and building community capacity. Comprehensive approaches and mobilizing communities, building on and joining well-organized, broad-based coalitions are important and can effectively create change in communities. 139 Key activities include implementing strategies that promote positive social norms among youth, families, adults, and community institutions and developing organizational policies aimed at preventing intimate partner violence. 139 Prevention strategies are described in more detail in Haegerich and Dahlberg’s overview of violence as a public health risk in this issue of the American Journal Lifestyle Medicine.
In 2010, the CDC produced a guide for Training Professionals in the Primary Prevention of Sexual and Intimate Partner Violence: A Planning Guide. 139 The guide, which may be useful to those who are developing training materials, describes how to develop, implement, and evaluate a training process, taking into account the available level of resources. The training process emphasizes turning awareness and knowledge into mastered skills and practices to prevent sexual violence and/or IPV by (a) teaching based on organizational context, (b) providing opportunities for skill development through participatory learning, and (c) following up to assess progress and determine level of mastery.
Conclusion
There is no doubt that victims of IPV suffer significant negative health consequences because of the physical, sexual, and emotional abuse they have experienced. Research has substantially improved our understanding of the physiology that underlies the association between violence victimization and an array of adverse health outcomes. Given the high prevalence of IPV, particularly among patients seeking care in primary care settings, and the associated medical and societal costs of IPV, it is critical to address this public health problem. IPV affects all members of the family and the larger community. IPV prevention and intervention can substantially decrease the public health burden of IPV and substantially improve the quality of life for many patients. Primary care and family physicians are in an ideal position to diagnose victims of IPV and provide them and their families with appropriate care and information about available resources. However, to accomplish this goal, there remains an urgent need to integrate information on IPV into medical and health care curricula and to train future physicians and other health care providers about the pervasiveness of IPV and the far-reaching implications for patient health. AJLM