Abstract
Pediatric lifestyle medicine encompasses key aspects of preventive medicine, which is at the heart of pediatric care. Lifestyle choices are important determinants of health outcomes. Key components of preventive health care include optimal nutrition, maintaining an appropriate weight, developing an active lifestyle, and avoidance of tobacco, alcohol, and other substances of abuse. In addition, reduction of risk behaviors through incorporation of safe health habits is important. Incorporation of the tenets of pediatric lifestyle medicine by pediatricians and other primary care providers of infants, children, and adolescents will promote a healthier population, prevent disease and disability, and ultimately decrease health care costs and use of health care resources. Communities, including school systems, must also embrace concepts of pediatric lifestyle medicine.
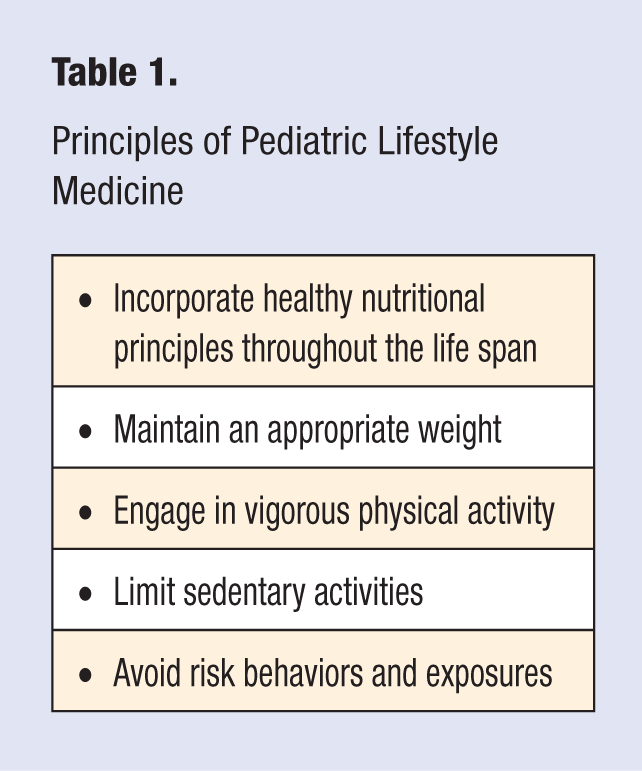
Pediatrics arose as a discipline designed to promote the health and well-being of children. Treating disease and preventing social abuse and neglect of children were paramount to the survival of children in the past. In an era of ever increasing health care costs and an aging population with many chronic diseases, prevention has never been more important. Pediatric lifestyle medicine encompasses health promotion and disease prevention, while ensuring that individuals have emotional health and the ability to enjoy a healthy, active lifestyle into retirement age. The major tenets of pediatric lifestyle medicine are outlined in Table 1. Determinants of health include both modifiable and nonmodifiable factors. Lifestyle medicine capitalizes on the modifiable factors. Many of these issues have been addressed in the comprehensive Bright Futures Guidelines for Health Supervision of Infants, Children, and Adolescents, now in its third edition. 1 This work was funded by the US Department of Health and Human Services (HHS) Health Resources and Services Administration Maternal and Child Health Bureau. The Bright Futures Children’s Health Charter, originally published in 1994, had a key element that “every child deserves to be born well, to be physically fit, and to achieve self-responsibility for good health habits.” 2
Obesity prevention begins in infancy, and pediatric lifestyle medicine must include a comprehensive preventive anticipatory guidance approach, coupled with targeted intervention for risk factors.
Principles of Pediatric Lifestyle Medicine
Infancy and Early Childhood
The health of infants begins with appropriate maternal care during pregnancy. This care includes optimal nutrition, appropriate weight gain, blood sugar control, and avoiding exposure of the fetus to noxious substances, such as tobacco, alcohol, illicit drugs, nonessential prescription drugs, or other environmental contaminants or exposures, such as radiation. Adequate intake of iron, calcium, vitamin D, and foods rich in docosahexaenoic acid help ensure appropriate development of the growing fetus. Inclusion of adequate folic acid in the diet prevents neural tube defects. 3 The Food and Drug and Administration and the Environmental Protection Agency recommend avoiding fish potentially high in mercury, such as swordfish, king mackerel, shark, and tilefish. Limiting total fish intake to 12 ounces per week, with no more than 6 ounces of canned albacore tuna per week, has been recommended. Although fish is high in essential fatty acids and docosahexaenoic acid, important for the growth and development of the brain and neurological system, the fetus may be exposed to environmental pollutants, such as dioxins and polychlorinated biphenyls. 4 Moderate physical activity during pregnancy contributes to appropriate weight gain and maintains maternal health and well-being.
All women should be informed about the benefits of breastfeeding throughout their pregnancy. The American College of Obstetricians and Gynecologists calls on obstetric providers to support breastfeeding among mothers and infants. 5 Breast milk not only provides optimal nutrition for infants and children, but also promotes attachment between mother and child. Compared with breastfed infants, formula-fed infants have a higher incidence of infectious diseases, such as otitis media, gastroenteritis, lower-respiratory infection, urinary tract infections, and certain types of bacterial meningitis. Breastfed infants are less likely to develop obesity, diabetes mellitus, and childhood leukemia. Breastfeeding may reduce the risk of immune-mediated conditions, such as inflammatory bowel disease, and reduce the incidence of hypertension, especially among those infants born prematurely. Breastfeeding is associated with decreased risk of sudden infant death syndrome, may prevent the development of certain types of allergies and eczema, and may delay the development of childhood asthma. Breastfeeding also helps to protects mothers from developing breast and ovarian cancer. 6 Because of these demonstrated health outcomes related to optimal breastfeeding, the Centers for Disease Control and Prevention (CDC) published guidance to support breastfeeding. 7
For newborns, lifestyle medicine includes initiation of breastfeeding soon after delivery and continued exclusive breastfeeding through the first 6 months of life. Hospital maternity practices must support breastfeeding by promoting early skin-to-skin contact, continuous rooming in, and avoidance of artificial nipples, in the form of pacifiers or bottle nipples, until breastfeeding is well established. 8 The American Academy of Pediatrics recommends exclusive breastfeeding for about 6 months and continued breastfeeding for at least the first year of life. 9 The World Health Organization recommends breastfeeding for a minimum of 2 years of life. 10
Among those infants born in 2008 in the United States, about 75% begin breastfeeding, but by 6 months, only 15% were exclusively breastfed. 11 Using the analysis of the Agency for Healthcare Research and Quality in the 2007 evidence-based review, 6 it has been further estimated that, if 90% of US families would comply with current recommendation to breastfeed exclusively for 6 months, the US would save $13 billion per year and prevent 911 deaths. 12 Healthy People 2020 Maternal, Infant, and Childhood Health objectives include increasing all of the following: the percentage of children who were ever breastfed to 81.9%, those who are breastfed at 6 months to 60.6%, those who are breastfed at 12 months to 34.1%, and those who are exclusively breastfed at 6 months to 25.5%. 13 To achieve these benefits requires a coordinated system of breastfeeding support from health care providers, maternity care facilities, and the community. Lack of maternity leave and early return to work contribute to early cessation of breastfeeding or lack of exclusive breastfeeding. Breastfeeding is cost-effective, environmentally friendly, and reduces the cost for employed workers for health benefits as well as contributing to less parental absenteeism. These effects are so significant that the US Department of HHS published the “Business Case for Breastfeeding” to encourage employers to provide lactation support in the workplace. 14 The Affordable Care Act of 2010 includes breaks for employed workers to express milk in the workplace. 15
The US Surgeon General issued a Call to Action to Support Breastfeeding in 2011, encouraging 20 action steps in 6 major categories: mothers and families, communities, health care, employment, research and surveillance, and public health infrastructure. These action steps are designed to support women in their choice to breastfeed and to eliminate barriers both to exclusive breastfeeding and to longer duration of breastfeeding. 16 Many of the health benefits of breastfeeding, such as obesity prevention, are dose dependent. In other words, the longer the child is breastfed exclusively and the more breast milk the child consumes, the greater are the benefits.
The impact of breastfeeding on the decreased risk of obesity is likely multifactoral and includes not just the hormonal and endocrine response to the composition of breast milk, but also infant feeding behaviors. Breastfeeding promotes satiety control, because the breastfed infant feeds when hungry and stops when full, unlike bottle-fed infants who can be coaxed to finish all the formula in a bottle. Breastfed infants showed better self-regulation in terms of intake in the Infant Feeding Practices Survey II.17,18
After breastfeeding exclusively for about 6 months, healthy solids should begin to be introduced to contribute to overall nutrition. Developmental readiness for solids include good head control, the ability to sit with minimal support, loss of the tongue extrusion reflex, and, most important for pediatric lifestyle medicine, the ability to indicate food refusal. 19 Satiety control should continue with the introduction of solids, allowing the infant to indicate when he or she is full, instead of the infant being encouraged to finish the last bite. The infant’s need for additional iron increases by 6 months of age. Therefore, first solids should be high in protein, iron, and zinc, making pureed meats a good initial choice. Vegetables, fruits, and iron-fortified cereals complement the diet by adding fiber, vitamins, and minerals. Initial infant foods should be single ingredient, with water or expressed breast milk added to make the ideal consistency. Limiting the addition of extra fat, salt, and sugar promotes lifelong healthy habits, helping to decrease the risk of developing cardiovascular disease, hypertension, and diabetes mellitus.
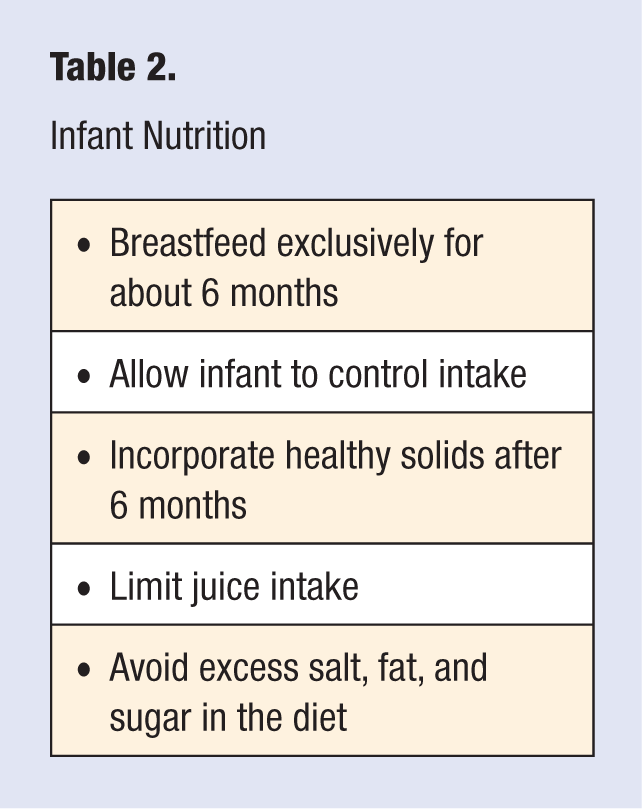
Excess consumption of juice in childhood can contribute to pediatric obesity. Juice is high in calories but low in overall nutritional value. In the early years of life, fruit juice should be limited to no more than 4 to 6 ounces per day of a 100% fruit juice. 20 Consumption of whole fruits provides higher nutritional value because some nutrients are lost in processing and storage of juice. In addition, fiber content is higher, which contributes to satiety and also decreases constipation. Table 2 summarizes key aspects of infant nutrition.
Infant Nutrition
As children progress beyond infancy and consume the typical family diet, it is important that this diet supports heart healthy habits, with decreased saturated fat and dietary sugars, and with appropriate attention to dietary needs for iron, 21 zinc, calcium, and vitamin D. 22 Recent studies indicate that much of the population may be deficient in vitamin D. A minimum intake of 400 IU of vitamin D per day is recommended for all children. 23 This can be provided in the form of fortified formula or milk or by supplementing the diet of the exclusively breastfed baby.
Obesity Prevention
The growth of children should be monitored closely at all recommended well-child visits. Body mass index (BMI) should be calculated and plotted, with particular attention to trends. BMI is the most cost-effective and widely available measurement of overweight and obesity in childhood. In general, obesity is defined as a BMI at the 95th percentile or greater. A BMI between the 85th and 94th percentiles indicates overweight. 24 As children approach late adolescence, the adult cutoff of a BMI of 25 kg/m2 can be used. A BMI less than the 85th percentile but trending upward, especially beyond the 75th percentile for age, may be a risk factor for the development of overweight and merits careful review of dietary intake and physical activity patterns. Analysis of the National Health and Nutrition Examination Surveys (NHANES) from 2003 to 2008 showed that 10.4% of children aged 2 to 5 years of age, 19.6% of children aged 6 to 11 years, and 18.1% of children aged 12 to 19 years of age are obese. These rates have increased significantly since the NHANES survey of 1976 to 1980, doubling or even tripling in some cases. Some estimates place 1 in 3 children in the category of overweight or obese, with as many as 12.5 million children in the United States being overweight today. In addition, there is a disproportionately high prevalence of obesity among African American women, Hispanic males, and Native Americans. 25 Children or adolescents who are obese are more likely to become obese adults. 26 There has been an increase in severe obesity among children and adolescents, and these individuals appear to be at highest risk of morbidity related to obesity. 27
Obesity prevention begins in infancy, and pediatric lifestyle medicine must include a comprehensive preventive anticipatory guidance approach, coupled with targeted intervention for risk factors. In addition to nutritional guidance, behavioral management is important. Limiting fast food consumption, limiting snacks and meals consumed in front of the television, teaching appropriate portion size, and eating meals together as a family are important. More recent recommendations focus on limiting highly processed foods and increasing consumption of locally grown vegetables and fruits. Motivational interviewing and assessing readiness of the child and family to change have been shown to be important tools in the treatment of the overweight and obese child. 28 Because children spend a significant proportion of their time in school, school-based programs and attention to nutrition at the school breakfast and lunch programs are essential in both the prevention and management of obesity. School campuses should limit the access of children to soft drinks, juices, candy, and snack foods that are low in nutritional value. These items have traditionally been found in vending machines on school property, and this practice should be eliminated.
Watching television has been associated with increased consumption of fast food items among preschool-aged children, with greater time spent watching television correlating with higher consumption. 29 Time spent watching television programs and the number of fast food or low-nutritional density food advertisements viewed by children also have been associated with increased incidence of obesity, diabetes, and metabolic syndrome. 30 Children with television sets in their bedrooms are more likely to be overweight, and these children watch more television or videos than do children who do not have televisions in their bedrooms. 31 In early childhood, parents and caregivers are responsible for what the child is offered to eat and must make sure that children are provided a nutritionally sound meal plan and snacks.
The significant increase in pediatric obesity has also been related to a steep rise in the rates of Type 2 diabetes mellitus in children in the past 2 decades. Obese children should be screened for type 2 diabetes. 32 Insulin resistance has been associated with increased adiposity in children. Pubertal growth spurts, with high levels of growth hormone and decreased insulin sensitivity, may make this population particularly vulnerable to developing type 2 diabetes. 33 Lifestyle management—preventing obesity, losing weight, or decreasing the rate of weight gain; increasing activity or decreasing sedentary lifestyle; and avoiding smoking—has been recommended in the management of obesity,34,35 which translates to decreasing the incidence of type 2 diabetes. Among obese children 5 to 17 years of age, 70% were shown to have at least one risk factor for cardiovascular disease, such as hypertension or high cholesterol. 36 Obese children are at increased risk of becoming obese adults, at which point, their risk of morbidity resulting from heart disease, stroke, diabetes, cancer, and osteoarthritis increases. 37
The US Department of HHS launched a Childhood Overweight and Obesity Prevention Initiative in 2007 to target obesity prevention and the promotion of healthy weight for children. Two recent federal initiatives have also addressed the issue of childhood obesity. The White House Task Force on Childhood Obesity Report entitled “Solving the Problem of Childhood Obesity Within a Generation” outlined initiatives involving early childhood, the roles of parents and caregivers, healthy food in schools, access to healthy and affordable food, and increasing physical activity as the key areas for emphasis in reducing childhood obesity. 38 “Let’s Move,” the obesity prevention program initiated by First Lady Michelle Obama enlisted parents, schools, community leaders, chefs, health care providers, elected officials, and children to become involved in promoting healthy lifestyles through access to and choice of healthier foods and providing healthier streets and playgrounds for safe outdoor activities. Health care providers were encouraged to include the following steps in their lifestyle medicine programs: (1) join “Let’s Move,” (2) make BMI screening a standard part of care, (3) talk to patients about breastfeeding and first foods, (4) prescribe activity and healthy habits, and (5) be a leader in the community. 39
Cardiovascular Health
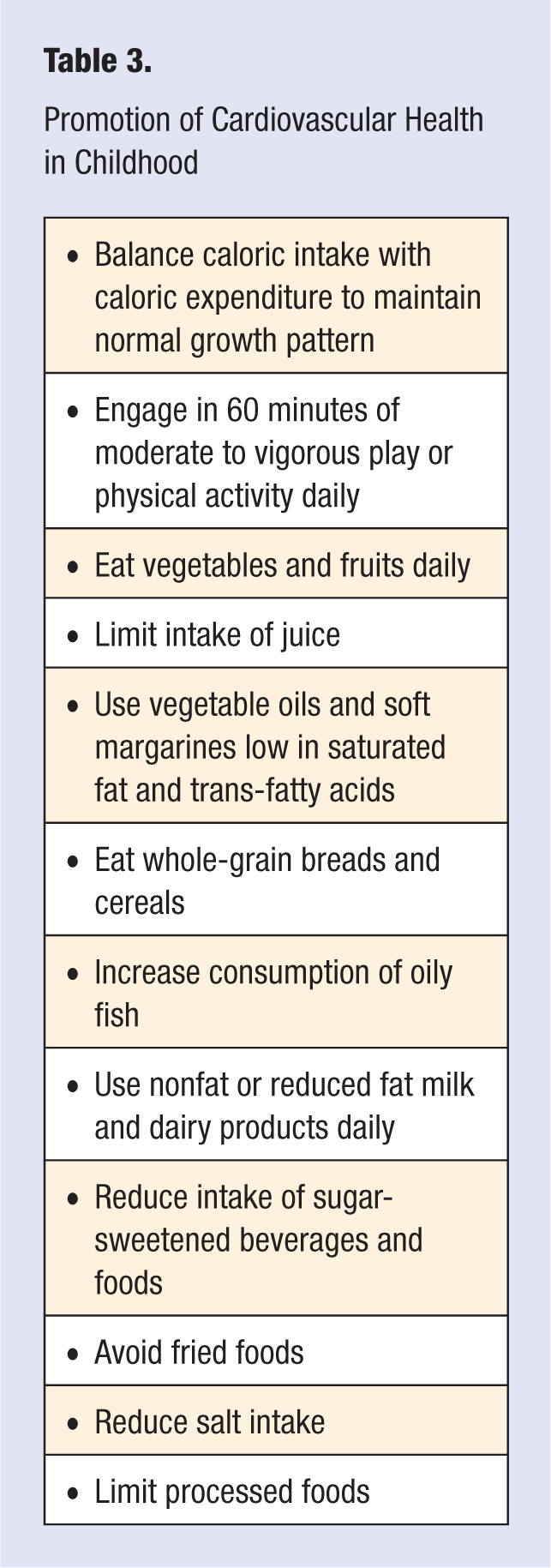
American Heart Association recommendations for children aged 2 years and older include many key components of lifestyle medicine. 40 These are outlined in Table 3. The 2010 US Dietary Guidelines for Americans included additional recommendations about maintaining appropriate calorie balance during each stage of life, beginning in childhood and adolescence: reducing sodium intake to 1500 mg/d for children, consuming less than 10% of calories from saturated fats, replacing saturated fats with monounsaturated and polyunsaturated fats, and consuming less than 300 mg/d of dietary cholesterol. Individuals were encouraged to consume half of all grains as whole grains, increase the intake of fat-free or low-fat dairy products, eat lean protein, and substitute fish for meat and poultry at some meals. 41
Promotion of Cardiovascular Health in Childhood
Cardiovascular risk factors have their genesis in childhood, with fatty streaks evident in the arteries of children. Blood cholesterol and triglycerides in children have increased in recent years, whereas levels of high-density lipoproteins (HDL) have decreased. Approximately 10.8% of adolescents aged 12 to 19 years have total cholesterol levels greater than 200 mg/dL. 42 In addition, more than 23% of adolescents aged 12 to 19 years have elevated triglycerides and low HDL. 43 Early identification of cardiovascular risk factors, with screening and implementation of dietary recommendations are appropriate. In addition to following proposed dietary recommendations, moderate to vigorous daily physical activity for 60 minutes or more; limited sedentary time, such as television viewing, computer activity, or sedentary videogames 44 ; and avoiding tobacco smoke and secondhand smoke exposure should be recommended for all children. 45 The American Academy of Pediatrics recommends no television viewing for children younger than 2 years and limiting television viewing to 1 to 2 hours of high-quality programming daily for children older than 2 years. 46 Total screen time should be limited, including time spent in front of televisions, computer screens, and video games. All these contribute to a sedentary lifestyle. Video games that engage children and adolescents in at least moderate physical activity should be encouraged, if video games are permitted.
Physical Activity
The US Surgeon General has called for increased physical activity levels for all Americans. 47 Most of the 60 minutes per day of physical activity should be in the moderate or vigorous intensity category and should include activities such as hiking, rollerblading, skateboarding, bicycling, and brisk walking. In addition, 3 times per week, the exercise should emphasize muscle strengthening with resistance or weight training and bone-strengthening activities, which include weight bearing. 48 Activities for children and adolescents should include activities that are enjoyable and incorporate other members of the family or friends. These activities may include team sports and school sport activities. School physical education programs are important in modeling and teaching lifelong physical activity. Although it is important for children to be exposed to team sports, not all children will be high caliber athletes playing team sports. Walking, jogging, bicycling, and swimming, all of which can be adopted as lifelong activities, are important activities to incorporate. Noncompetitive sports need to be an option. For those student athletes who desire organized sports activities, these should be available within the local school setting as well as in the community in the form of team sports. Physical activity is associated with increasing lean body mass, improving bone mass, maintaining a healthier weight, and improving emotional and mental health. 49 Prior to the pubertal growth spurt and increased muscle mass in males, boys and girls can participate in competitive sports teams together. After puberty, contact sports should be segregated based on body mass and muscle strength.
Children and adolescents should be taught about appropriate hydration during activity. In general, beverages, and especially water, should be consumed to avoid dehydration. By the time thirst occurs, the body is already mildly dehydrated. Outdoor physical activity should be limited during the hottest times of the day, especially during the summer months in warm climates. Consuming water before, during, and after physical activity is important. Cool drinks may be absorbed best. Flavored water may be consumed in greater quantity by some children. Sports drinks that include electrolyte replacement are not necessary unless the vigorous activity lasts for longer than 60 minutes. The American College of Sports Medicine recommends drinking 12 to 22 ounces of cool water (50-60°F) 1 to 2 hours before physical activity, 10 to 20 ounces of cool water 10 to 15 minutes before physical activity, 4 to 6 ounces of cool water every 15 to 20 minutes during physical activity, and 16 to 24 ounces of cool fluids for every pound of weight lost during the activity. 50 Coaches should be alert to signs of heat-related illnesses and monitor athletes for dehydration and heat exhaustion. For competitive athletes, education should be provided about the risks of performance-enhancing substances, such as anabolic steroids and creatine. Nutritional supplements for young athletes at best may be of no benefit; however, some may cause harm. Some products found in supplements may be on banned substance lists and may cause athletes to be eliminated from competition.
Excessive and unhealthy weight loss to achieve a specific weight class may pose health risks. Excessive attention to weight may also increase the risk of developing eating disorders, especially among female gymnasts, skaters, and ballet dancers. Children or adolescents who present with a distorted body image, a BMI less than the 20th percentile for age, restricted intake, unexplained weight loss, and overtraining or excessive physical activity should be screened for eating disorders. Disordered eating behaviors are prevalent among adolescents. 51
Risk Behaviors
A final component of pediatric lifestyle medicine includes avoiding risk behaviors. Since 1991, a biannual CDC survey, the Youth Risk Behavior Surveillance System (YRBSS) has monitored trends as reported by 9th to 12th grade students. The YRBSS monitors 6 health-risk behaviors that contribute to both death and disability among adolescents and adults. These behaviors include violence and injuries, tobacco use, alcohol and other drug use, sexual risk behaviors, unhealthy dietary behaviors, and physical inactivity. Results from the 2009 national YRBSS indicated that many high school students are engaged in behaviors that increase their likelihood for death. Among high school students nationwide, 9.7% rarely or never wore a seat belt when riding in a car driven by someone else. During the 30-day period prior to completing the survey, 28.3% of high school students reported that they had ridden in a vehicle driven by someone who had been drinking alcohol, 17.5% had carried a weapon, 41.8% had consumed alcohol, and 20.8% had used marijuana. During the 12 months before the survey, 31.5% of high school students had been in a physical fight, and 6.3% had attempted suicide. Substantial morbidity and social problems among youth also result from unintended pregnancies and sexually transmitted infections, including HIV infection. Among high school students nationwide, 34.2% were currently sexually active, 38.9% of currently sexually active students had not used a condom during their last sexual intercourse, and 2.1% of students had injected an illegal drug. During 2009, 19.5% of high school students smoked cigarettes during the 30 days before the survey. During the 7 days before the survey, 77.7% of high school students had not eaten fruits and vegetables 5 or more times per day, 29.2% had drunk soda at least once per day, and 81.6% failed to engage in 60 minutes of physically activity each day. One third of high school students attended physical education classes daily, and 12.0% were obese. 52
Recommendations for solutions to these risk behaviors included better health education, more physical education and physical activity programs, healthier school environments, and better nutrition services. Specific consideration should be given to improving access to fresh fruits and vegetables in the school lunch; eliminating fried foods from the school lunch; limiting soft drinks, fruit drinks, and candy from school vending machines; incorporating health topics, nutrition and dietary behavior, and guidance about physical activity as part of school health education; and requiring physical education for all grades for the entire year. 53 Injury prevention guidelines for using seatbelts, not drinking and driving, and not boating and drinking should be included in health classes. The health education of adolescents should be a shared responsibility between parents, the school system, and health care providers. Media, social media, and the internet also play a significant role in influencing adolescent risk behaviors. Minimizing risk behavior and maximizing health behaviors should be the goals of pediatric lifestyle medicine. Key messages to provide to adolescents are noted in Table 4.
Minimizing Risk Behaviors in Adolescents
Tobacco use is often associated with other risk behaviors, and children who begin smoking are highly likely to continue smoking into adulthood. Most smokers begin smoking before the age of 18 years, making this a pediatric health problem. 54 Health care providers should inquire about tobacco use and secondhand smoke exposure at every encounter. 55 Tobacco cessation programs should be actively used for those teenagers who have already initiated the use of tobacco products, as well as for parents and other caregivers who use tobacco products. 56
Adolescence is a period of increased independence, reliance on peers instead of parents, and experimentation. When these occur in the context of a healthy lifestyle that has developed in early childhood and continues throughout adolescence, there is less long-term risk. Risk behavior in the household also affects younger children. The dangers of secondhand tobacco exposure and excessive use of alcohol or other illicit substances create an environment in which children experience both direct and indirect health risks. Younger children model the behaviors of their parents and caregivers. A safe home environment with stable caregivers promotes emotional health and well-being as children grow and develop.
Although pediatric lifestyle medicine has a central goal of health promotion and disease prevention, lifestyle medicine can also be incorporated in the management of childhood problems. Obesity, diabetes, metabolic syndrome, rheumatological and collagen vascular diseases, hypertension, and chronic pulmonary and cardiac diseases are but a few of the conditions that benefit from active lifestyle management. Achieving and maintaining a healthy weight, normalizing blood pressure, reducing hyperlipidemia, and increasing physical activity and exercise capacity improve the quality of life for a variety of childhood conditions. A multidisciplinary team approach from the medical, nutrition, exercise, psychology, and rehabilitation services to develop a comprehensive plan and provide ongoing monitoring will help achieve success.
Conclusion
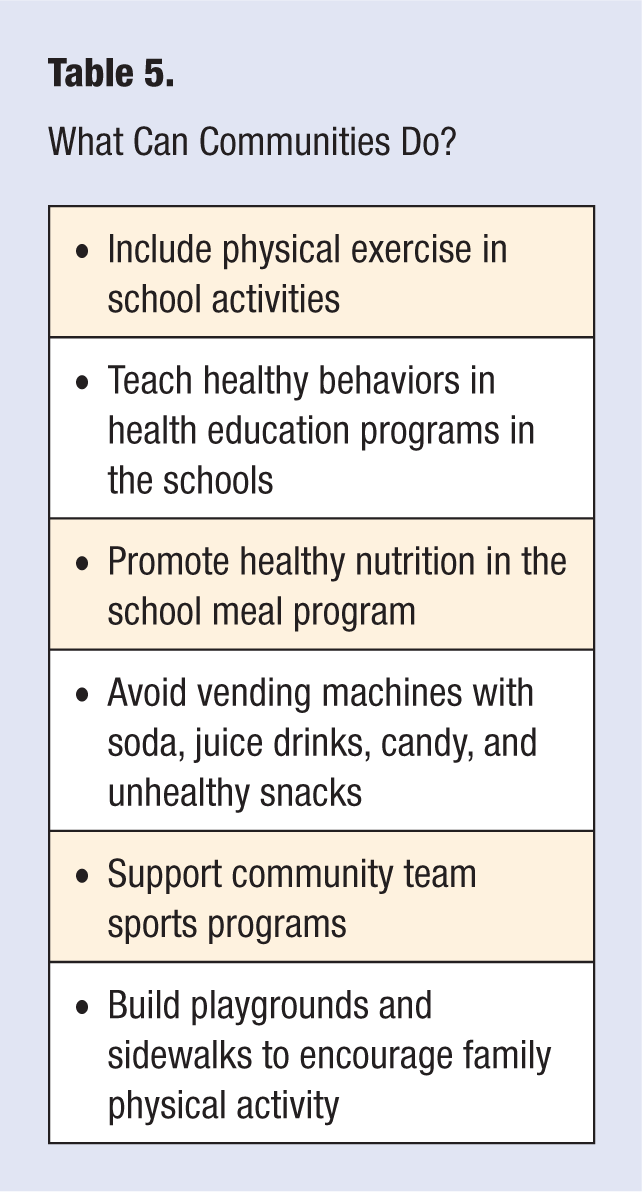
Key components of pediatric lifestyle medicine include optimal nutrition, beginning with early and exclusive breastfeeding, which may help program for a lifetime of health; maintaining appropriate weight throughout childhood and adolescence; 60 minutes of moderate physical activity per day; and avoiding risk behaviors, such as the use of tobacco products and alcohol. Pediatric lifestyle medicine should be incorporated by all pediatric health care providers at all encounters and should be reinforced in the school system, in our communities (see Table 5),and supported by government and legislatures in the structuring of our communities and resource use. Bright Futures Guidelines for Health Supervision of Infants, Children, and Adolescents serves as a helpful resource for providers, institutions, and educators.1 Healthier children and adolescents today contribute to the next generation of adults experiencing better health outcomes, using fewer health care resources, and living longer, healthier, and more active and productive lives.
What Can Communities Do?