
Abstract
Frailty is a multidimensional syndrome associated with a state of vulnerability to external stressors. Though women have a longer life expectancy than men, they have a higher risk of frailty. Frailty is prevalent in women, affecting ∼9-15% of community-dwelling older women, and over 50% of nursing home residents. Women have unique risk factors for frailty at distinct life stages such as pregnancy and menopause. Women who have children at a young age and those who experience premature menopause have a higher risk of developing frailty later in life. Frailty is modifiable, and preventive strategies can be implemented using the framework of the six pillars of lifestyle medicine. Moreover, frailty is also a therapeutic target, with the best approach to prevention occurring earlier in life. Implementation of the six-pillar approach to frailty prevention is best achieved by considering specific benefits and barriers to each pillar for women. For example, implementing strength training alongside diet optimization while bolstering social connections. The six pillars are closely interrelated. As such, a holistic approach targeting all six has the greatest potential for success. Future studies are needed to guide therapeutic interventions specific to preventing frailty in women.
Keywords
“Disordered sleep impedes the growth process, contributing to muscle loss and ultimately resulting in frailty.”
Definition of Frailty
Frailty is a state of vulnerability to external stressors, often attributed to physiological changes throughout the lifespan. 1 Although frailty is more common in older adults, it can occur across the lifecycle. 1 Frailty is associated with declines across multiple physiological systems. It is multidimensional, encompassing physical, cognitive, social and psychological domains. Frailty has been associated with a myriad of negative outcomes including falls, cognitive decline, reduced quality of life, and mortality. 2 Frailty itself is an independent predictor of survival.3,4
In the general population of older adults, the prevalence of frailty varies widely, in large part based on the definition used. On average, about 4-60% of community-dwelling adults over age 65 are frail, with lower rates of frailty identified using the Fried definition (7-10%) compared to the Rockwood (25-30%).1,2,5 In assisted living and long term care or nursing homes, rates of 50% or higher are common, and can approach 80% in older adults living with underlying conditions such as heart failure.6,7 At older ages, the prevalence of frailty rises as well. 8
There are two leading operational definitions of frailty, both published in 2001, that frame how frailty can be measured.9,10 The accumulation of deficits approach, developed by Rockwood and colleagues, is based on the comprehensive geriatric assessment, and takes a systems view of the human body, positing that changes across the system can be quantified as a ratio of deficits present to those assessed. There are key criteria to selecting deficits for the cumulative deficit approach: ensuring that all are related to health and aging, are neither too common nor too rare, and cover a range of domains, such as nutrition, function, cognition, and morbidity. 11 The physical phenotype definition, developed by Fried and colleagues, considers five interrelated aspects of physical function: exhaustion, physical activity, walking speed, weakness, and weight loss. These two leading theories of frailty will identify different groups of individuals in a population as frail, with about 30% overlap,12,13 yet both are associated with similar risks of poor outcomes. 14 These two overarching frameworks of frailty help classify over 60 tools developed to measure frailty clinically. 15 Separately, sarcopenic obesity defined as the coexistence of obesity and sarcopenia (low muscle mass and function) is on the rise, is different from the Fried frailty phenotype, and also leads to increased vulnerability to adverse outcomes. 16
What has emerged over the last two decades of frailty research is a recognition that any valid tool can be used to measure frailty, and is better than the “eyeball” or “end of the bed” test,
17
which risks over- or underestimating frailty. The different approaches to evaluating frailty are depicted in Box 1. Major frailty models and commonly used tools; see eFrailty.org for additional details. The AMED - alternate mediterranean diet score, DASH - dietary approaches to stop hypertension) AHEI-2010 - (alternate healthy eating index 2010).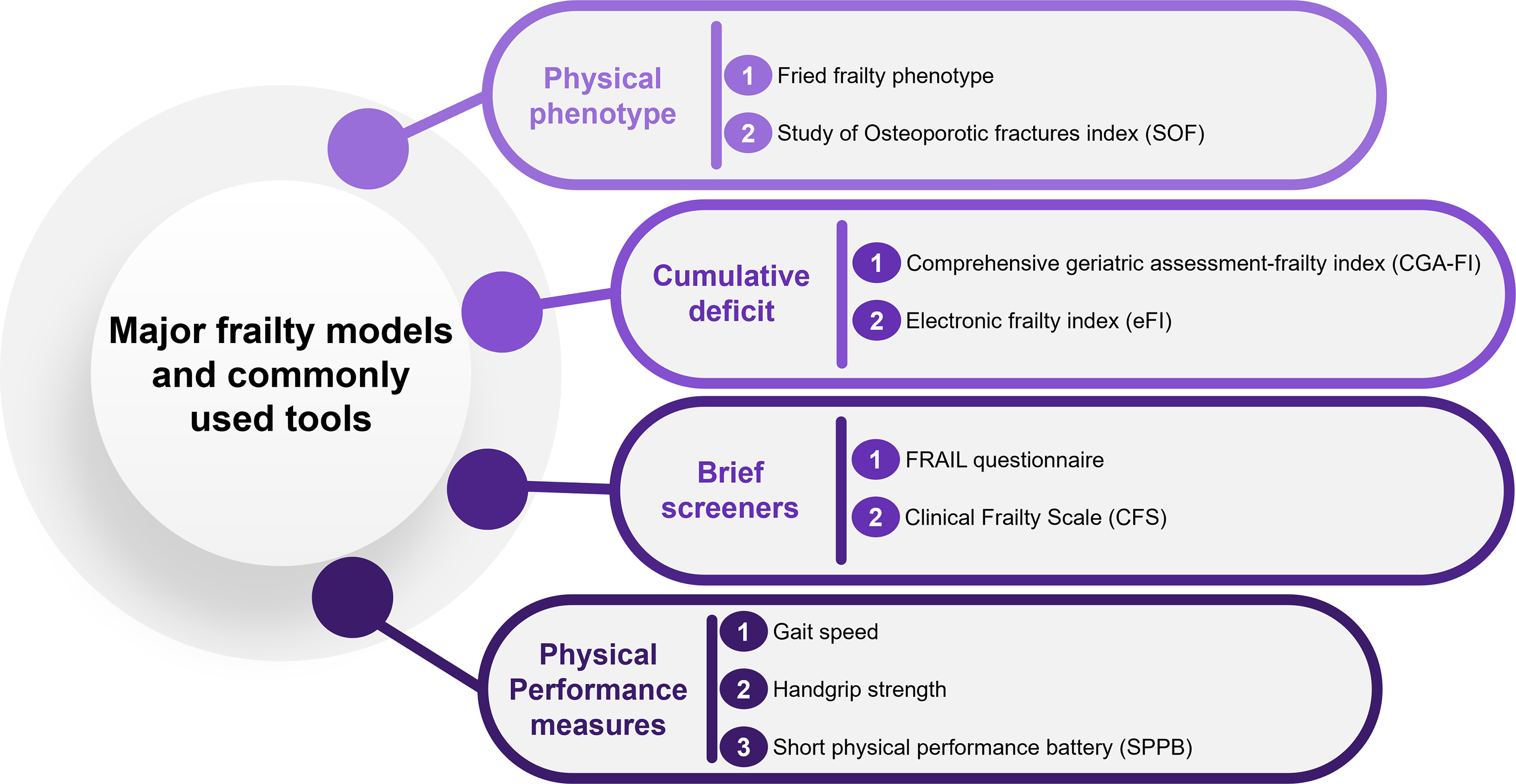
Screening
Frailty screening occurs across three major settings: primary care, hospitalization, and prior to stressful treatments such as chemotherapy 2 or surgery. 18 There is currently mixed evidence to support population-based screening for frailty in general primary care. 19 A task force of the International Conference of Frailty and Sarcopenia Research (ICSFR) recommends screening for frailty in primary care using a simple, validated frailty instrument for all adults aged 65 and older. 20 Clinicians can identify both brief screening and comprehensive care planning tools for frailty at eFrailty.org (see Box). 21 Regardless of screening approach, abnormalities should be followed up with dedicated geriatric assessment, tailored clinical management, and referral to appropriate services. Care plans can include lifestyle elements, especially physical activity and nutrition interventions as these have been found to be most effective in women at risk of and living with frailty. 2
Frailty in Women
Summary of Pivotal Frailty Studies with Female Participants.
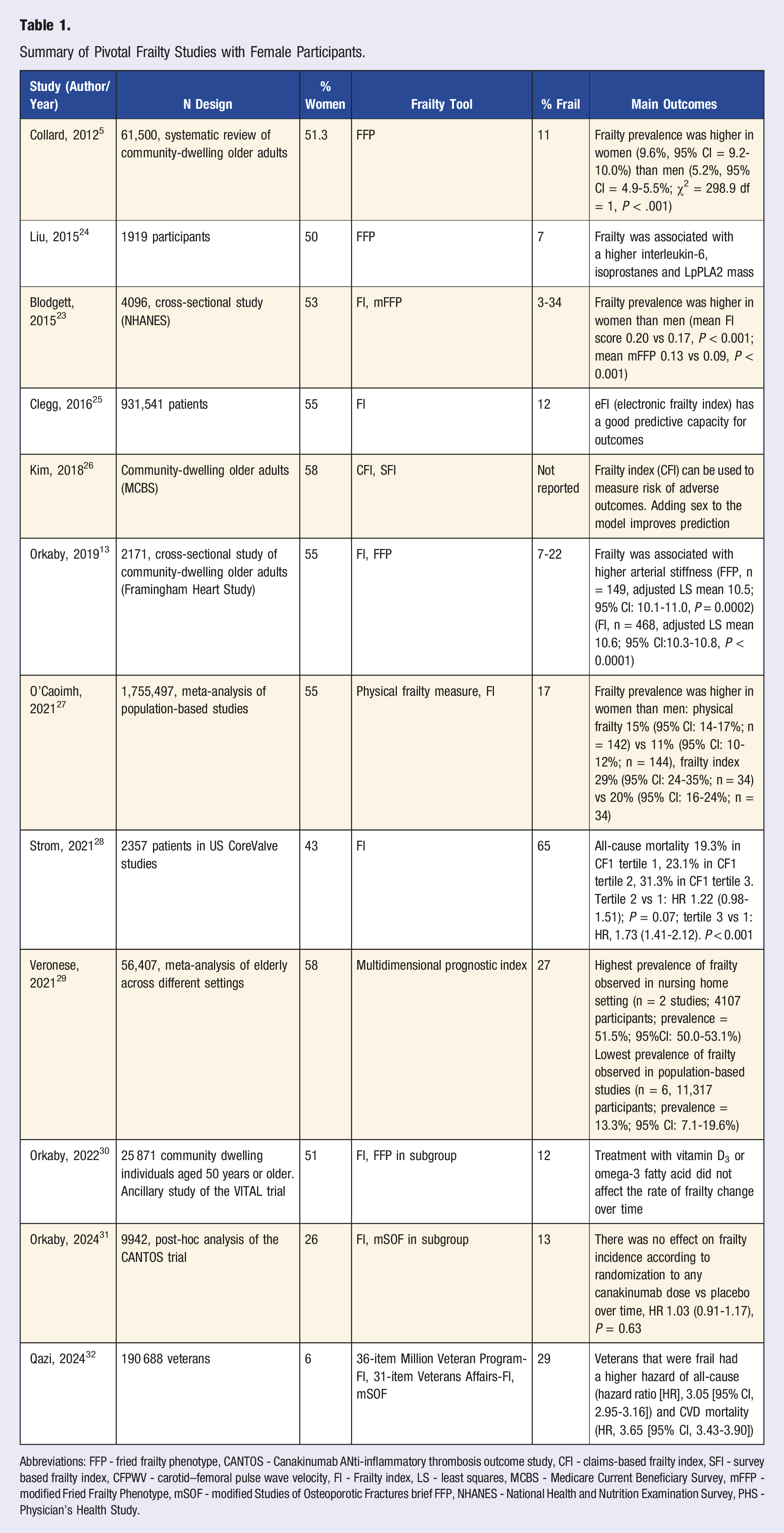
Abbreviations: FFP - fried frailty phenotype, CANTOS - Canakinumab ANti‐inflammatory thrombosis outcome study, CFI - claims-based frailty index, SFI - survey based frailty index, CFPWV - carotid–femoral pulse wave velocity, FI - Frailty index, LS - least squares, MCBS - Medicare Current Beneficiary Survey, mFFP - modified Fried Frailty Phenotype, mSOF - modified Studies of Osteoporotic Fractures brief FFP, NHANES - National Health and Nutrition Examination Survey, PHS - Physician’s Health Study.
The biological reasons for this sex discrepancy are complex and multifactorial. Women tend to acquire a higher number of chronic conditions and functional impairments over the lifespan, though with a lower risk of mortality as compared to men. 22 Hormonal factors may play an important role, for example, higher levels of estrogen in younger years may delay atherosclerosis and delay getting cardiovascular disease, and therefore mortality in women. 33 In addition, pregnancy transiently elevates biologic age, and a higher number of pregnancies is associated with higher frailty index.34,35 Earlier age at first birth is associated with higher likelihood of frailty in middle and older age, 36 and earlier age at menopause is associated with higher risk of frailty.37,38
Inflammatory factors may also play a role in the sex-frailty discrepancy. Testosterone may reduce the immune response in men, increasing susceptibility to infections in late life. 39 Yet, women have a higher prevalence of autoimmune disorders and abdominal adiposity, exposing them to higher levels of chronic inflammation.40,41 Women may be more susceptible to the effects of chronic inflammation on frailty as well: for every standard deviation increase in C-reactive protein (CRP) and fibrinogen, women have approximately 1.3 increased odds of frailty, whereas there is no association with frailty with either CRP or fibrinogen in men. 42
Lower mitochondrial energetics in women compared to men may partly explain the increased risk of sarcopenia and mobility impairment in women. 43 Women have a lower peak muscle mass than men, with corresponding higher rates of sarcopenia.
There are important sex differences in physical activity behavior that may further exacerbate women’s vulnerability to sarcopenia and frailty. Women also have lower peak bone mass and higher risk of osteoporosis as compared to men, which increases risk for disabling fractures. 44
Understanding the true prevalence and underlying risk factors for frailty in women is vital to designing preventive strategies that can be implemented early in life and during pivotal life stages.
Chronic Disease Management
Frailty prevention in women is notably underrepresented in chronic disease guidelines, despite its significance for the overall aging population. Most chronic disease prevention frameworks primarily focus on the management of the disease, such as cardiovascular disease, diabetes, and hypertension, without explicitly addressing frailty as a preventable outcome.45–47 In chronic disease literature, frailty is often treated as an inevitable consequence of aging rather than a condition that can be actively prevented or even reversed. 48 While the benefits of exercise, nutrition, and cognitive health in chronic disease management and prevention of frailty are well established, these interventions are typically generalized and not tailored to the specific needs of women. For example, strength training is particularly important for women due to their higher risk of frailty and osteoporosis, and although recommendations are made, they are not systematically included across chronic disease prevention guidelines.49,50 To address this gap, it is essential that frailty prevention be integrated into chronic disease management and clinical practice guidelines, 51 with sex-specific strategies that emphasize a holistic approach to frailty prevention in women with chronic disease.
Implementation
There are several examples of successfully implemented programs for frailty screening and interventions, although the impact on clinical outcomes is mixed. Though the U.S. has not widely operationalized frailty assessment, Medicare assesses important geriatric risk factors through the Annual Wellness Visit (AWV). Though the AWV has been only modestly adopted and has unclear impact on several intended clinical outcomes, it increases use of some preventive services, increases screening rates for falls, and may reduce health care cost. 52 The National Health Service (NHS) in the United Kingdom systematically identifies older adults living with moderate and severe frailty using population-based approaches, notably using the automated electronic frailty index (eFI). 53 The World Health Organization (WHO) has adopted the Integrated Care for Older People (ICOPE) program, which has been shown to be feasible to integrate in clinical practice (n = 10,903 older adults, mean age 76, 61% women) and had high follow-up rates (70%) for those with abnormal screens. In Japan, persons identified as pre-frail or frail during primary care screening (n = 916) were referred to a group community program which over 10 years improved functional status at the population level. 54 Other health systems, including those in Hong Kong, Canada, and Singapore, have implemented population-level screening and management initiatives, though clinical outcomes data are not yet available. 55
Lifestyle Strategies for Frailty Prevention and Intervention
The six pillars of Lifestyle Medicine are a framework of lifestyle interventions that have been implemented with success in optimizing health
56
(Figure 1). As detailed below, these pillars are interconnected and include physical activity, nutrition, stress management, social connection, sleep and avoidance of risky substances. Central illustration; pillars of lifestyle medicine as it relates to frailty in women.
Lifestyle approaches are key for frailty prevention and intervention. At present, there are no proven pharmacologic approaches for frailty. Effective frailty management strategies with the highest level of evidence are physical activity and nutrition interventions. Multicomponent programs are particularly effective, with several elements such as physical activity and protein intake having synergistic effects. 57
Foundations for strong lifestyle pillars should start early in life and be adjusted across life stages. Establishing healthy exercise, nutrition, sleep, and stress management habits early can impact health in later life. Women may benefit from additional interventions at specific life stages. For example, only half of working mothers in the United States met the guidelines for regular physical exercise, with lack of self-compassion and guilt being main drivers of abstaining from health promoting activities.58,59
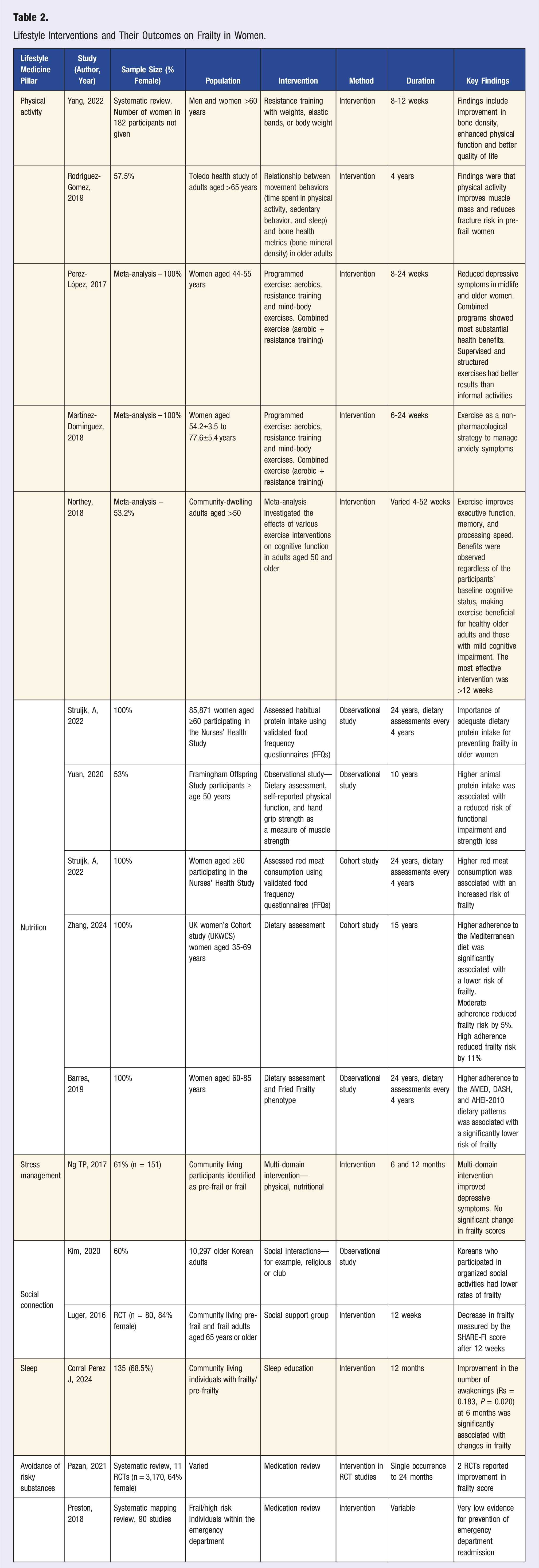
Lifestyle Interventions and Their Outcomes on Frailty in Women.
Pillar 1: Physical Activity
Physical activity is fundamental to preserving health and function in aging women, particularly in mitigating frailty.60–62 A robust inverse relationship exists between physical activity and frailty, underpinned by multifaceted mechanisms related to body composition, bone density, and functional ability.63,64
Strength training has demonstrated positive impacts on frailty-related parameters, including significant improvements in bone mineral density (mean difference 0.01 g/cm2, P = 0.03), skeletal muscle mass (mean difference 1.19 kg, P = 0.0007), and body fat percentage (mean reduction of 1.61%, P = 0.02). 65 Adverse health effects associated with sarcopenic obesity, a condition of increased adiposity with reduced muscle mass that is closely related to frailty, can also be mitigated with strength and resistance training via the simultaneous increase in muscle mass while reducing adiposity. 66 Moderate to vigorous physical activity has been shown to improve skeletal muscle mass and reduce fracture risk in pre-frail women. 64 The benefits of these activities in women extend beyond the musculoskeletal system, reducing cardiovascular disease risk, improving mental health, and fostering social connections that reinforce adherence and create a positive feedback loop of improved health outcomes.67–72
A growing body of evidence supports physical activity interventions for frailty prevention and reduction in women. Randomized trials have shown significant improvements in functional performance and quality of life (qOL) among women engaged in resistance training, 73 and qOL has been linked to frailty outcomes. 74 Community-based strength training programs exemplify targeted interventions that maintain strength, function, and independence in aging females. 75 Despite the established benefits, barriers to engagement persist, including sex-based stigmas, knowledge deficits, limited accessibility, and time constraints.76,77 However, research has identified facilitators such as social support and peer accompaniment during exercise sessions, which can enhance participation, particularly among older women. 78
To optimize frailty-reducing interventions, programs should highlight benefits that resonate with women, such as enhanced muscular health, improved body composition, and potential mental health improvements. Supervised sessions with expert feedback can address safety concerns and refine technique, crucial for older adults apprehensive about injury risk. 79 Additionally, designing flexible programs that accommodate diverse lifestyles and life stages can promote consistent engagement and long-term adherence to physical activity regimens.
Mind-body exercises, such as tai chi and yoga, represent promising interventions for addressing frailty in older adults. Nuanced benefits of these integrative practices have been demonstrated in previous research, with tai chi practice resulting in significant improvements in 30-second chair stand test scores (weighted mean difference (WMD): 2.36, P < 0.0001), timed up and go test scores (WMD: −0.7 P = 0.0002), and decreased fear of falling (standardized mean difference: −0.50 P = 0.0006) when compared to non-exercise controls. 80 One study showed that 8 weeks of 4-movement qigong exercise improved cognitive function and physical performance in women specifically. 81 Yoga-based interventions have demonstrated moderate-certainty evidence for enhancing gait speed and lower extremity strength and endurance, with low-certainty evidence for improving balance and multicomponent physical function. 82 This systematic review included 33 studies, with 3 including only women where interventions were focused around pain reduction and did not meet statistical significance. Yoga has also been shown to reduce inflammatory markers in healthy female subjects. 83 One large meta-analysis highlighted mind-body exercises as the second most effective physical activity intervention for frailty reduction, following resistance training. 84 While these approaches may not consistently alter muscle mass or grip strength, they offer holistic approaches to mitigating frailty that extend beyond traditional exercise paradigms.
Pillar 2: Nutrition
Dietary patterns and intake of specific nutrients influence frailty risk and progression in aging women.85,86 The underlying mechanisms linking nutrition to frailty are complex, encompassing protein synthesis, muscle maintenance, regulation of inflammation, and metabolic function. Protein consumption plays a central role, with intake ≥1.1 grams of protein per kg body weight being significantly associated with reduced odds (OR) of both pre-frailty (OR = 0.45, 95% CI = 0.01-0.73) and frailty (OR = 0.09, 95% CI = 0.01-0.75) in older women compared with those that ate less protein.85,86 While animal protein correlates with preserved grip strength and functional capacity, plant protein demonstrates superior protective effects against frailty development, suggesting potential benefits of plant-based protein substitution in preventive strategies.87,88
The Mediterranean dietary pattern, characterized by abundant consumption of vegetables, fruits, whole grains, and nuts, while limiting pro-inflammatory components such as processed foods and red meat, 89 shows particularly robust associations with reduced frailty risk, with stronger adherence associated with greater protective effects.90–92 This diet’s value appears to stem from its optimal balance of anti-inflammatory components, protein content, and essential nutrients that collectively support metabolic health and physical function.93,94 These dietary components significantly influence mortality risk, with increased intake of vegetables, nuts, and whole grains associated with a respective 9% (P = 0.02), 13% (P < 0.001), and 17% (P < 0.001) reductions in mortality, respectively. 94 A large meta-analysis of 19 studies (18 of which included >50% female participants) showed that the Mediterranean diet is inversely associated with physical frailty. 95 Another study of 21,643 women showed that over 13 years of follow-up, adherence to the Mediterranean diet is associated with lower risk of frailty. 90 Although limited direct evidence exists on many specific diets, emerging research suggests potential longevity benefits with a sirtfood-rich diet which contains sirtuin-activating foods (containing nicotinamide adenine dinucleotide (NAD+)-dependent deacylases and ADP-ribosyltransferase enzymes) 96 of both the Asian and Mediterranean diets. 97 In an analysis of the Nurses’ Health Study, including 71,941 women with 11,564 incident cases of frailty, healthy eating is associated with lower frailty scores using the FRAIL scale. 98 This study included a number of diets including adherence to the alternate Mediterranean diet (AMED), Dietary Approaches to Stop Hypertension (DASH) diet where foods that lower blood pressure are consumed and the Alternative Healthy Eating Index (AHEI-2010 diet) which measures the risk of chronic disease based on diet.
Broader dietary patterns demonstrate varying impacts on frailty risk in women, with healthful plant-based diets showing protective effects while processed food-dominated patterns increasing risk. 99 The “biscuits and snacking” pattern, for instance, demonstrates significantly higher frailty risk compared to “healthy” patterns (HR 1.8; 95% CI 1.2-2.8). 100 Dairy consumption presents a nuanced relationship with frailty, as cheese consumption potentially increases risk while milk and yogurt demonstrate neutral effects. 101 Higher fruit and vegetable intake consistently is associated with reduced frailty risk in women aged ≥60 years, potentially attributed to reducing inflammation and micronutrient content, including magnesium.102,103
When considering nutritional interventions for women, targeting both macro and micronutrient intake through anti-inflammatory dietary patterns represents an evidence-based approach to frailty prevention.91,102 Implementation of dietary recommendations emphasizing adequate protein intake, particularly from plant sources, combined with increased consumption of anti-inflammatory foods and limited intake of pro-inflammatory components, may offer the most effective nutritional strategy for reducing frailty risk and maintaining functional capacity in aging women.
Beyond nutrient composition, the manner that food is consumed consumption such as mindful eating practices and social engagement during meals, represents an evolving line of inquiry in understanding the dietary influences on frailty104–106 These approaches to eating not only provide physiologic sustenance but potentially modulate psychological resilience, bridging nutritional intake with mental health outcomes. 90 There is emerging evidence in animal models that intermittent fasting 107 and calorie restriction 108 may attenuate frailty in older adults. When these strategies are combined with physical activity this may maximize the benefit especially in women. 109
Successful frailty prevention requires individualized, multicomponent lifestyle interventions that address generational barriers and personal preferences.110,111 Recognizing that engagement varies across age groups, interventions should balance evidence-based recommendations with practice implementation strategies. For younger pre-frail women, emphasizing long-term health benefits of adopting a healthy diet and integrating exercise into social contexts may enhance adherence.112,113 Older generations may require more targeted approaches addressing safety concerns, incorporating supervised exercise sessions, and providing nutritional counseling.110,114
Overall diet (and exercise) influences the majority of frailty risk factors, such as body weight, chronic disease risk, muscle mass, and bone density.
Pillar 3: Stress Management
Frailty in women is influenced by various psychosocial factors, including stress and mental health. 115 Understanding these dimensions is crucial for developing effective interventions aimed at preventing frailty and enhancing women’s overall well-being. Frail individuals have higher levels of perceived stress and stress related symptoms, although the exact mechanism is poorly understood.116,117 Women often assume the role of primary caregiver for children, aging parents, or other family members, which has been identified as a major contributor to stress.118,119
From early developmental stages onwards, emotion-focused coping strategies to manage stress are more often observed in women. 120 Developing coping strategies to control the effect of potential sources of stress or to diminish the extent of their impact has successfully been utilized in a complementary approach to frailty. 121 Supporting women to develop their emotion-focused coping strategies across the lifespan may play a role in the prevention of frailty, however further research in this area is necessary.
Mind-body approaches are effective for stress management. Mindfulness-based stress reduction (MBSR), an eight-week mindfulness training program, is the most studied intervention and effective for stress reduction. 122 Yoga and tai chi are also effective for stress management, and adapted programs for older adults may improve their effectiveness. 123 Stress and mental health encompasses areas like depression, anxiety, low life satisfaction and social connection.
Depression
Depression and frailty are interrelated, with distinct domains that are bidirectionally associated.124,125 Compared to men, both depression and frailty are more prevalent in women.125,126 Notably, the combination of frailty and depressive illness has been linked to a heightened risk of mortality, with the association being particularly pronounced in women. 127 This underscores the critical need for integrated care approaches that address both mental health and physical frailty.
First-line treatments for depression in older adults include standard approaches such as psychotherapy, especially cognitive-behavioral therapy (CBT) or acceptance and commitment therapy (ACT) for older populations, and/or antidepressant medications.128,129
Physical activity and other lifestyle factors also play an important role, highlighted by a recent meta-analysis that suggested exercise may be as effective as standard treatment approaches. 130 Certain types of exercise have been shown to be more effective at alleviating depressive symptoms, with combined muscle strengthening and balance training programs and yoga demonstrating benefit. 70 Additionally, multi-domain programs, including nutritional, physical, cognitive, and combination interventions designed to reverse frailty in community-dwelling individuals have been shown to also reduce depressive symptoms. 131
Anxiety
Several studies have demonstrated significant sex differences in anxiety and frailty, with women more likely to be frail and anxious than men.33,132 In a group of 390 postmenopausal women, anxiety was prevalent in 44% and was independently associated with frailty. 133 MBSR is effective for managing anxiety in women. 134 Women with concurrent frailty and anxiety are more reluctant to seek help compared to frail individuals with severe depression. Barriers to accessing support include difficulty scheduling appointments with a preferred primary care clinician and prioritizing mental health discussions during limited appointment time, with a preference for self-managing anxiety symptoms. 135 This highlights the importance of incorporating anxiety screening into comprehensive care programs and emphasizes the need for sex-specific interventions that consider the unique experiences of women.
Low Life Satisfaction
Low life satisfaction is often intertwined with mental health challenges faced by older women. The interplay between stress, anxiety, and depressive symptoms can create a cycle that diminishes life satisfaction, further exacerbating the risk of frailty. 136 A randomized controlled trial of 74 [n = 48 (64.9% women)] nursing home residents that frail older adults receiving Life Review Therapy showed significantly greater improvements in life satisfaction compared to those receiving usual care. 137 Moreover, a comprehensive continuum of care, including coordination of care by a case manager, interprofessional teamwork and care planning in frail older persons’ own homes had a positive effect on the older persons’ life satisfaction. 138 Interventions aimed at enhancing life satisfaction may be beneficial in developing more effective, holistic care models for older women, and decreasing the risk of frailty.
Pillar 4: Social Connection
The intersection between social isolation, loneliness, low life satisfaction, and frailty is well recognized. 139 Social engagement plays a critical role in mitigating the risk of frailty in women, with strong social networks and community involvement contributing to overall well-being. Particularly for older women, social relationships provide not only a sense of belonging and identity but also crucial emotional and practical support. 140 Family ties, caregiving roles, community participation, and religious involvement are all key forms of social engagement that contribute to well-being and can reduce frailty risk among women. 141
Women often have strong social networks and are likely to maintain close relationships with family members over the course of their lives. 142 Close family relationships offer social support and a sense of purpose, which can contribute to improved health and a reduction in frailty. 143 For women, caregiving roles are particularly significant, as women are more likely to care for children and older family members. This responsibility can be both fulfilling and challenging. Positive experiences of caregiving, including enjoyment being with the care recipient, feelings of closeness to them, and feeling more confident in one’s abilities, collectively termed positive emotions, have been shown to reduce the risk of frailty (RR = 0.94, 95% CI 0.90, 0.99). 144 However, caregiving can also increase stress, leading to burnout, lower quality of life, and reduced ability to care for one’s own health. 145 These challenges underscore the importance of balancing caregiving with other forms of social engagement for women to prevent frailty.
The effects of social engagement on frailty exhibits sex-specific nuances and can vary depending on the type of social activity. For women, promoting involvement in community organizations and volunteering can enhance social ties and provide meaningful engagement, potentially reducing the risk of frailty. 146 A randomized control study examining the effects of a social support “buddy” program demonstrated a significant reduction in frailty over 12 weeks (Adjusted OR 0.5 (95% CI 0.3-0.8; P = .003). 147 Religious participation is also associated with a lower risk of frailty (OR 0.4 (95% CI 0.2-0.8; P < 0.001)) and slower progression of frailty (OR 0.5 (95% CI 0.4-0.8; P < 0.001)). 148 Women are more likely than men to engage in religious practices, which have been shown to provide emotional support and a sense of community, protecting against the physical and cognitive decline associated with aging and frailty.149,150
Widowhood represents a significant social factor influencing frailty risk with unique sex-specific differences. Unmarried men carry the highest frailty risk, whereas widowed women are less likely to be frail (including exhaustion and unintended weight loss) than married women (OR 0.8 (95% CI 0.7-0.9; P = 0.002) due to increased social networks and less caregiver responsibilities. 151 By fostering stronger social ties and promoting active participation in community life, women can reduce their risk of frailty and enhance their overall well-being. 141
Pillar 5: Avoidance of Risky Substances
Polypharmacy
Polypharmacy, generally defined as taking five or more prescribed drugs, is associated with higher likelihood of adverse drug reactions, falls, cognitive decline, and mortality in older adult populations.152–154 Over 50% of older adults experience polypharmacy, and over 20% of older adults take ten or more medications. 155 The prevalence of polypharmacy, including the use of potentially inappropriate medications, has been reported to be higher among women compared to men.156,157 Excessive polypharmacy in frail individuals increases the risk for adverse outcomes, though the causal relationship is unclear and is likely bidirectional. 158 While the impact of reducing unnecessary medications in the community setting on frailty is unclear, medication review as part of a frailty care pathway may prevent readmission in frail populations. 159 Clinicians should be attentive to medication review for older female patients as they are at higher risk of polypharmacy than men. While deprescribing may not directly benefit frailty status, when integrated into the prescribing continuum and it may reduce other important and associated adverse outcomes such as falls, hospitalization, and mortality.
Substance Use
Women tend to smoke less often than men, with global prevalence of daily tobacco smoking reported to be 6.2% for women and 31.1% for men in 2012, decreased from rates reported in 1980. 160 In men and women those who smoke cigarettes are more likely to develop frailty, while smoking cessation may reverse frailty.161,162 Smoking increases the frailty index in a dose-dependent manner, with heavy smoking having worse outcomes. 163 Women who smoke lose their survival advantage at all levels of health. 164 Cigarette smoking has clear negative impacts on health, including accelerating frailty, and represents a high-yield target for promoting healthy aging.
The prevalence of alcohol use is generally lower for women than men, though the gap is narrowing.165,166 While moderate alcohol use was previously thought to be associated with reduced cardiovascular risk, more recent evidence has found that even low-risk drinking is associated with an increased risk of mortality compared to abstinence, especially in older populations. 167 The relationship between alcohol and frailty is still being investigated. One meta-analysis including studies with 52-100% female participation showed that heavier alcohol consumption, compared to no alcohol, was associated with lower incident frailty. 168 However, other studies have found that high alcohol consumption in midlife predicts future frailty. 169 Nondrinkers have been reported to have higher risk of frailty as compared to low alcohol use, though this appears to be explained by poorer baseline health. 170 The Women’s Health Initiative Observational Study followed 28,003 women aged 65-79 for the development of frailty and showed that women who consumed less than 1 drink per week were at decreased risk of frailty, however also showed that there was no difference in frailty risk between women who consumed 14 drinks per week (>28 g of alcohol/day) and those that consumed none. 171 Several methodological issues may explain discrepant findings, including that those who abstain 171 tend to have worse lifestyle than regular drinkers, and survivor bias where there is an overrepresentation of healthier drinkers in older age. 167 Drinking wine instead of beer or liquor, and drinking with meals both seem to be healthier drinking patterns. 167 However, it is unclear if any amount of alcohol is beneficial. In addition, older women are more vulnerable to adverse effects of alcohol, both acute and chronic, due to body composition changes.
There is little research on injection drug use and frailty. In one study, injection drug use among those with HIV stimulated epigenetic programming that is correlated with higher rates of HIV-related frailty. 172 Given clear adverse effects on general health, clinicians should screen for and treat substance use disorders to promote healthy aging.
Pillar 6: Sleep
Distinct hormonal and physical changes at specific points in a woman’s life, such as puberty, pregnancy, and menopause, can influence sleep health and can contribute to sex-specific discrepancies in conditions such as frailty. 173 There is a bidirectional relationship between sleep quality and frailty. Disordered sleep impedes the growth process, contributing to muscle loss and ultimately resulting in frailty. Conversely, frailty can also disrupt sleep patterns, as it is associated with increased inflammation and other physiological changes in the body. 174 In older women, poor sleep quality, including insomnia and sleep duration of less than 5 hours per night or greater then 8 hours per night, is associated with a higher incidence of sarcopenia, risk of frailty, and faster frailty progression, however this association is likely bidirectional.175–179
General sleep health guidelines recommend aiming for 7-8 hours of sleep per night, engaging in regular physical activity, managing stress, and maintaining a conducive sleep environment. 180 They also recommend establishing consistent sleep-wake times, minimizing daytime naps, and avoiding caffeine and alcohol close to bedtime.160,180 This is particularly relevant for women during times of hormonal fluctuation, which can exacerbate sleep disturbances.181–183 Sex-specific temperature-based interventions can improve sleep health in women and may contribute to the prevention and management of frailty. For example, maintaining a cooler sleeping temperature may be particularly useful for women in times of hormonal fluctuation. Head cooling has also been shown to improve sleep quality in young women during the luteal phase when women experience moderate estrogen and high progesterone levels. 184 In menopausal and postmenopausal women, manipulation of body temperature during sleep using a high heat capacity mattress and a forehead cooling device demonstrated improved sleep quality, a reduction in insomnia severity and menopausal symptoms.185,186
In women with sleep problems, exercise has been identified as a particularly effective intervention to optimize sleep health in women.187,188 Moderate physical activity improved overall sleep quality in middle-aged women, but did not reduce the insomnia severity, with similar effect observed in pregnant populations.187,189 Furthermore, behavioral interventions, including CBT, mindfulness, and relaxation techniques, improve sleep in peri- and postmenopausal women. 190 These strategies are particularly beneficial as they target the psychological and environmental factors that contribute to sleep disturbances. The emphasis on non-pharmacological interventions aligns with current recommendations to avoid medications for sleep issues in older women, focusing instead on lifestyle changes and behavioral therapies. 180
Taken together, sleep health is a crucial component in frailty prevention for women. With significant evidence linking sleep disturbances to frailty risk, interventions that promote healthy sleep and address the unique challenges faced by women at various life stages are paramount.177,178
Future Directions
Frailty in Clinical Trials
In the context of clinical trials, frailty has recently emerged as an important effect modifier, particularly in the pathogenesis of cardiovascular disease and cancer. 191 In trials of interventions for hypertension and heart failure, those who were frail at baseline had similar or even greater benefit of interventions, contrary to what many had hypothesized. 192 In most trials, frailty was not considered a priori and rather was added post-hoc, most commonly using the Rockwood definition. In some trials, variations of the Fried method were able to be calculated using the Study of Osteoporotic Fractures (SOF) definition which is a prospective multicenter study of risk factors for fractures.13,30 Standardized frailty assessments will enhance trial protocols by consistently measuring frailty’s impact on treatment effectiveness. Incorporating the frailty index and phenotype in data collection would enhance individual trial and meta-analysis findings, enabling better identification of high-risk frail participants who may need closer monitoring. Despite frailty’s variable impact on treatment efficacy, frail patients often benefit from interventions; frailty assessments are crucial for understanding adverse event risks, especially given frail patients’ higher likelihood of drug interactions and side effects. For example, among postmenopausal women with cancer, pre-diagnostic frailty and worsening frailty status were linked to higher mortality rates, highlighting frailty’s impact on survival. Few trials have considered frailty as the primary endpoint.
Advances in Frailty Models and Screening
The Age-Friendly Health Systems (AFHS) 4 Ms Framework was developed to guide health systems in providing high-quality clinical care across four evidence-based domains: What Matters, Medication, Mentation, and Mobility, which are closely tied with domains important for frailty. 193 Starting in 2025, the CMS Age-Friendly Hospital Measure will require hospitals in the Medicare Inpatient Quality Reporting Program to report on implementing age-friendly care protocols, which include 194 frailty screening and intervention, which will benefit affected female patients
A novel approach to frailty screening, the electronic frailty index (eFI) has potential to be scaled to the health systems level to meet these needs. The eFI was derived from the Rockwood deficit accumulation model from data existing in the electronic health record (EHR). Several large health systems, including the English NHS, U.S. Department of Veterans Affairs, and Atrium Health-Wake Forest Baptist have successfully developed and implemented the eFI. 195 An important next step will be implementing personalized frailty interventions, especially for women experiencing frailty.
Future Preventive and Therapeutic Strategies for Frailty
Although multiple databases have been used to understand the prevalence of frailty in women, few have examined the role of preventive therapeutic strategies for frailty.13,23,26,28,30 Observational data from the Women’s Health Initiative (WHI) reported that women ≥65 years who reported statin use for 3 or more years had a trend toward a 12% lower frailty risk compared to non-users. 196 The role of statins for frailty prevention is now being tested as part of the Pragmatic evaluation of events and benefits of lipid lowering in older adults (PREVENTABLE) Trial, in one of the first drug trials for frailty prevention. 197 Additionally, in WHI, women who reported using angiotensin converting enzymes did not have a lower risk of in frailty. 195 Several recent post-hoc analyses of randomized trials have examined the role of Vitamin D, Omega 3, and the anti-inflammatory drug canakinumab for frailty prevention.30,31 None of these interventions lowered the risk of incident frailty or slowed the trajectory of frailty in men or women. Observational studies such as the Study of Osteoporotic Fractures suggest that women with diabetes treated with an insulin sensitizer such as metformin have slower decline in walking speed, a marker of frailty, compared to those who did not. 198 The Targeting Aging with Metformin (TAME) trial will test metformin for frailty prevention. 199 More studies are needed to understand the role of therapeutics for frailty prevention, particularly trials which can shed light on the role of drugs beyond their initial specified indications, to a more holistic outlook of overall aging health and biology through the lens of frailty.
Nonpharmacologic
Frailty and cardiovascular disease (CVD) have significant intersectionality with regards to their pathophysiology and outcomes. 200 Approximately 50% of patients with heart failure (HF) are frail. The relationship is bidirectional with the prevalence of HF increasing six to sevenfold with the increase in frailty severity. 16 An upregulated neurohumoral state, inflammation and sarcopenia all underpin both HF and frailty, mediated by inflammatory cytokines such as interleukin-1 (IL-1), interleukin-6 (IL-6), CRP, and tumor necrosis factor-α (TNF-α). 201
Management of cardiovascular risk factors (many of which overlap with life’s essential pillars), prevents cardiovascular disease, and frailty. For example, stress reduction techniques such as mindfulness-based mediation and yoga have been shown to reduce blood pressure. This is re-iterated by proteomics-based studies using the extreme phenotype of meditative monks, who have been shown to have a protective plasma proteome associated with reduced atherosclerosis and enhance oxygen release. 202
Nutrition is an essential component for good cardiovascular health and is also a target for frailty intervention. Future directions include precision based nutritional approaches. These include biomarker driven precision nutrition, which have already been built into app-based technology.203,204 In addition, metabolic signatures could be used for dietary compliance and to assess response, which have been linked to CVD outcomes. 205 Finally, there is an early signal regarding microbiota targeted interventions, nutrition and CVD, which may also have a role in frailty mitigation. 206
Pharmacologic
At present, there are no medications proven to treat frailty. Certain medications may be beneficial in targeting frailty beyond their role in treating CVD. Statins have both anti-cholesterol and anti-inflammatory effects, promising for reducing frailty. While statins have been found to reduce all-cause mortality in some populations, 207 in the Women’s Health Initiative study, concurrent statin use in women aged >65 years had no effect on frailty. 196
Due to beneficial effects on cardiac remodeling and blood pressure control, angiotensin converting enzyme inhibitors (ACEi) also hold potential for frailty treatment. Metformin has been successful in pre-clinical studies at treating frailty
Sodium-glucose cotransporter-2 inhibitors (SGLT2i) and glucagon-like peptide-1 receptor agonists (GLP1a) have both cardio- and reno-protective effects. A recent study showed benefit of both drugs older diabetic patients, with the greatest benefit in patients with more severe frailty. 208
Finally, mTOR inhibitors have potential for modulating inflammation and are under investigation as a therapeutic agent to target frailty, include the risk of immunosuppression. 209
Life stages
There is emerging evidence that genetic and epigenetic factors likely play a role in aging process and potentially in the development of frailty. Moreover, all of the hallmarks of aging play a role in the development of frailty.53,210 These include telomere length, mitochondrial dysfunction and altered intracellular communication. 211 As we study these biomarkers, personalized intervention may be possible to address dysregulated processes. At present, clinicians can identify women with specific cardiovascular disease risk factors who would benefit from targeted intervention, such as hypertensive disorders of pregnancy and/or gestational diabetes. Women who experience premature menopause or hysterectomy may also benefit from more intensive intervention. 38 Prehabilitation strategies prior to an upcoming stressor (e.g., surgery) may be of benefit in those that are pre-frail in later life, 212 including dedicated exercise and nutritional strategies. 213
Conclusion
Frailty is a multidimensional syndrome with unique biological and psychosocial considerations in women. Understanding the true prevalence of frailty in women is a first step. As an independent predictor of survival, screening for frailty may allow for optimum treatment. Moreover, prevention of frailty, particularly across the life stages may be possible by using the six pillars and understanding the relationship between these pillars. At present, the highest level of evidence for prevention lies in physical activity and nutrition, but these interventions are made more robust by the other pillars, as no one stands on its own.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosures
Bart NK - Research funding Pfizer, Speaking fees Pfizer, Advisory board fees Pfizer, Bridge Bio, Novo Nordisk and Bristol Myers Squibb. Orkaby AR: None. Friedman SM: None. Montgomery E: Research funding Pfizer and St Vincent’s Clinic Research Foundation. Ivey KL: None. Loewenthal JV: Supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of an award (GACA 6K01HP49053-01- 01 to J.V.L.) totaling $86,978 with 0% financed with non-governmental sources. Burton W: None. Kamali S: None. The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS, or the U.S. Government.