
Abstract
Intensive therapeutic lifestyle change (ITLC) programs have been shown to consistently achieve improved biologic markers for cardiac heart disease risk in short periods of time. We propose a standard definition of ITLC and discuss the specifics that are critical to their success. We include a discussion of our experiences with delivering ITLC programs in large health care systems and use that to illustrate opportunities for ITLC implementation in the future. Finally, we discuss the current drivers of change in the US health care reform movement and comment on their predictable effects on the current health care landscape.
Keywords
‘Intensive therapeutic lifestyle change (ITLC) programs affect health behaviors but can have an even stronger impact on population health than TLCs alone.’
The Need for Intensive Therapeutic Lifestyle Changes
Therapeutic lifestyle changes (TLCs) are recommended to patients suffering from chronic illnesses. TLC is a comprehensive lifestyle approach that includes specific dietary recommendations (TLC diet), weight management, and increased physical activity that formally arose from the Third Report of the National Cholesterol Education Program. 1 Traditionally tobacco cessation is also included. Therapeutic lifestyle changes have been shown to be the foundation of clinical primary prevention. TLCs encourage small lifestyle changes to help patients improve their health. In a meta-analysis completed in 2013, which reviewed the impact of primary care physicians’ weight loss counseling on patients’ weight loss behavior changes, most studies demonstrated a positive effect. 2 While there is evidence that TLCs affect health behaviors, they have been challenging to execute and sustain by individuals based on counseling alone. The support structure needed for behavior change is rarely found in a clinical setting.
Intensive therapeutic lifestyle change (ITLC) programs affect health behaviors but can have an even stronger impact on population health than TLCs alone. Currently, ITLC programs are being coordinated in residential and community settings throughout the United States by integrated teams of caregivers. They are focusing on all 4 critical components of health: nutrition, activity, stress management, and social support. A key component of ITLC programs is the fact that they are delivered in a group setting. In 2008, an analysis for group diabetes care found improved satisfaction for patients and clinicians, along with better quality of care and reduced emergency department and specialist visits. 3 ITLCs bring forth larger, life-altering changes that are critical for improving well-established chronic disease. This is why such profound health improvements are being seen in patients participating in ITLCs, even to the point of disease reversal.4-7
To this point a formal definition of ITLCs has not been created. We propose to define ITLCs as programs that meet the following criteria:
Evidence-based (ie, use approaches shown to work using accepted research methods)
Multimodal (ie, nutrition, physical activity, stress management, social support, etc)
Multiple sessions over a short period of time (from 8 to 20 sessions, at least 60 minutes per session, at least weekly, and no shorter than 10 days for all sessions to occur)
Specific health outcome metrics are measured and consistent results are obtained, accounting for variation in populations, adherence, and engagement
Initial Use of ITLCs in the United States
There are examples of ITLC’s running throughout the nation, even in this narrowed definition. These examples have shown consistent health metric improvements as well as return on investments, bending the cost curve of health care (see Tables 1 and 2). The example in Table 2 demonstrated a cost difference in health care spend for a population of diabetic patients in a workplace setting of $1826 in 6 months. 8
ITLC 30-Day Outcomes a .
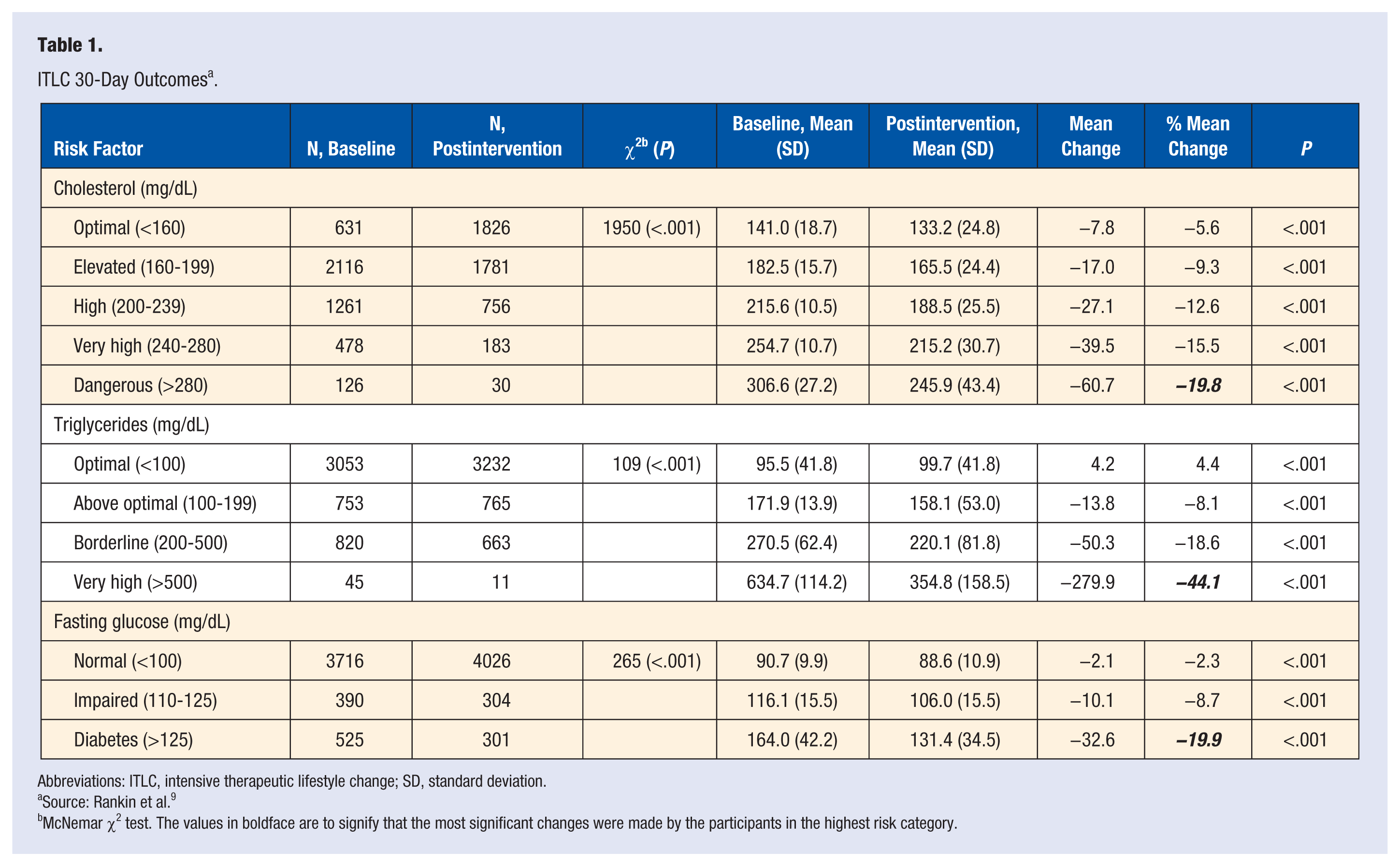
Abbreviations: ITLC, intensive therapeutic lifestyle change; SD, standard deviation.
Source: Rankin et al. 9
McNemar χ2 test. The values in boldface are to signify that the most significant changes were made by the participants in the highest risk category.
Community-Based ITLC and Cost: Average Cost and Utilization (Plan-Paid Medical, Prescriptions, and Copays).
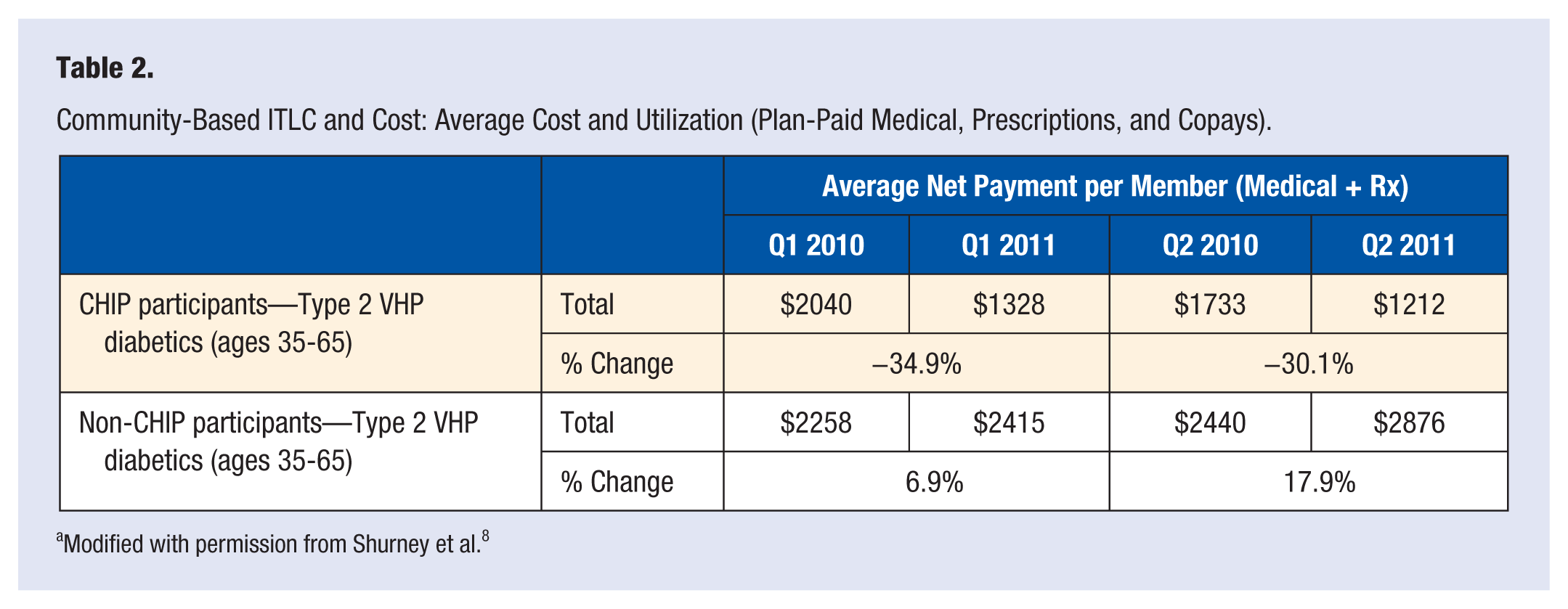
Modified with permission from Shurney et al. 8
Loma Linda University
At Loma Linda University Health (LLUH), ITLCs have been implemented in clinical and educational settings since 2006. In 2006, a group of medical students familiar with the Complete Health Improvement Program (CHIP) worked with faculty to implement the first on-campus ITLC program. This was so successful that it became a standard 4-week elective available to fourth-year medical students. This has since evolved into a 4-hour introductory exposure to TLC, ITLC, and lifestyle medicine assessments and prescriptions that are given to all medical students during their first year, and another 4-hour specific experience around running the CHIP program for all fourth-year medical students. ITLC/CHIP electives remain, but are now 2 weeks in length.
At the residency level, there are 2 concrete exposures to ITLC experiences. The first is in the Lifestyle Medicine Education Concentration. This is a program designed to provide a certificate of completion and added competency to any resident interested in Lifestyle Medicine. It consists of 20 hours of skill and knowledge building experiences for residents that take place over the course of one academic year. One of those experiences is 6 hours of exposure to an actual CHIP program. The second is only for Preventive Medicine residents (PMRs). All PMRs are given 1 day early in their third post-graduate year where they are trained to be CHIP facilitators. This provides every single PMR graduate with a specific ITLC skill set.
At a clinical level, ITLC experiences within LLUH occur 4 or 5 times each year. Experiences include the CHIP program, the Full Plate Diet program, and the Health Ropes program. The CHIP program is a classic ITLC consisting of 18 sessions that are typically given over 6 to 9 weeks in a relatively intense format. CHIP is best suited for individuals who are relatively sick or at high risk for disease. The Full Plate Diet program is a less-intense ITLC that works well for individuals who are less sick but are looking to fine tune their approach to health. The Health Ropes program is technically not an ITLC, but is designed to be a lifestyle maintenance program. A useful comparison would be to consider ITLCs to be similar to an inpatient or outpatient intensive alcohol rehabilitation program, and Health Ropes to be the weekly AA meeting that is part of full recovery.
Referral streams for the ITLC experiences have been developed through outpatient clinics (Family Medicine, Orthopedics, General Internal Medicine, Ophthalmology), inpatient services (general hospitalist, cardiac rehabilitation, physical medicine and rehabilitation), and employee wellness (CHIP is a fully covered benefit for all enrolled diabetic employees). Despite these connections, the flow of patients into the ITLC programs has still not been maximized. Current work continues on streamlining the capabilities of referring through the electronic medical record and educating providers and support staff on the consistent value of ITLCs for certain patient categories.
The Christ Hospital Health Network (TCHHN)
At The Christ Hospital Health Network, a hospital in Cincinnati, Ohio, the CHIP began in 2012. The CHIP ITLC is, originally, an 18-session program designed to reduce disease risk factors through the adoption of better health habits and appropriate lifestyle modifications. Since starting at TCHHN, over 8 programs have been completed. Results in this institution have mirrored the national results for over 55 000 participants in health improvements noted in the biomarkers of cholesterol, blood pressure, weight, and glucose. The delivery team for CHIP is composed of trained facilitators who at TCHHN are exercise physiologists, nutritionists, and or meditation/yoga providers. A medical director and business director maintain oversight. The focus market for the corporate CHIP program has been self-funded employers. These employers assume the direct risk for payment of the claims for the health benefits of their employees. Improving the health of their workforce is aligned with their goals of decreasing the costs of health care provided to their employees. CHIP creates a culture of change, empowering self-care and responsibility for health risk behaviors.
As many employers are in different states of change and evolution in their wellness initiatives, flexibility in the approach to improved health is necessary. Our greatest measured return on investment to date is our ITLC program. In addition to corporate strategy and wellness consulting, TCHHN also creates and facilitates well-being programs for the community, which includes tobacco cessation programs, weight loss programs, nutritionist services, wellness coaching, and stress resiliency programs.
A referral in the electronic medical record system has been created for clinicians to be able to order the CHIP program or one of the other interventions, just as they would order physical therapy or refer to another specialist. Patients also come to the programs through word of mouth or through the website.
Currently private nor public insurers do not reimburse the programs that are offered. Individuals that participate are self-pay. A few of the self-funded companies have embedded the offerings in the design of their benefit plans though. Furthermore, two advancing areas in third party payer realization have shown promise in the last few years. First, under the Patient Protection and Affordable Care Act (PPACA), the US Preventative Task Force A and B recommendations will need to be a covered benefit under non-grandfathered insurance products. ITLCs fit the designated intervention that would be covered. Additionally, new G codes are now being used to bill for medical nutrition therapy. If one is interested in using the MNT codes, there are very specific criteria to follow and current variation in reimbursement from payers. Second, the continued increase in consumer directed products like Health Savings Accounts will make ITLCs very attractive because these put the financial responsibility of health care costs on these consumers. ITLCs can be the value path that leads us to better patient health, which will reduce overall population health spending.
One of the key elements for running ITLCs is to understand your pipeline: where are you going to come in contact with your patients? For TCHHN, the brokers are well positioned to create that viable bridge to the companies served. The corporations are looking for answers to their wellness needs and to slow down the rising cost of their employees medical care costs. The Network is looking to provide high-value interventions, as well as data-driven analytics for population health, focused on meeting the triple aim: improving patient outcomes, improving the patients experience and lowering the cost of care. Another resource is engaging the physician network. The employed physicians are just beginning to understand the delivery changes for population health. We are developing Continuing Medical Education and a specific ITLC program designed for providers, in the same format as CHIP. TCHHN intensive hospital-based introduction to CHIP on the inpatient rehabilitation floor did not initially succeed. Change is difficult and prevention, even in the form of secondary and tertiary, is challenging for many to embody in a fee for service environment.
The most significant impact for pipeline engagement for TCHHN has been testimonials. When people, real people we can relate to, make meaningful change in their lives and it is noticed, that creates engagement. The hardest part in all of this work is the internal cultural change. Conservative health systems that have been successful in a fee for service business and in disease management have a hard time valuing prevention and cost avoidance in health care. It is a work in progress.
Why the United States Needs ITLCs
Why does an introduction of ITLCs make sense? We continue to hear how the current system is unsustainable, which is not disputed, especially when we see every population being burdened by chronic disease in epidemic fashion.
Health expenditures currently represent about 18% of our gross domestic product and are expected to reach roughly 20% by 2020. 10 The main response to this critical issue has been the enactment of PPACA in 2010. 11 This legislature has focused on increasing access to health care and health services by way of insurance reform, and even requires Medicare and all qualified commercial health plans (except grandfathered individual and employer-sponsored plans) to cover routine preventive services graded A and B at no cost to the consumer. Table 3 shows three specific recent grade B US recommendations, 12 which one can see are directly related to lifestyle medicine, satisfied by ITLCs.
Examples of Recent USPSTF B Recommendations Directly Relative to Lifestyle Medicine.
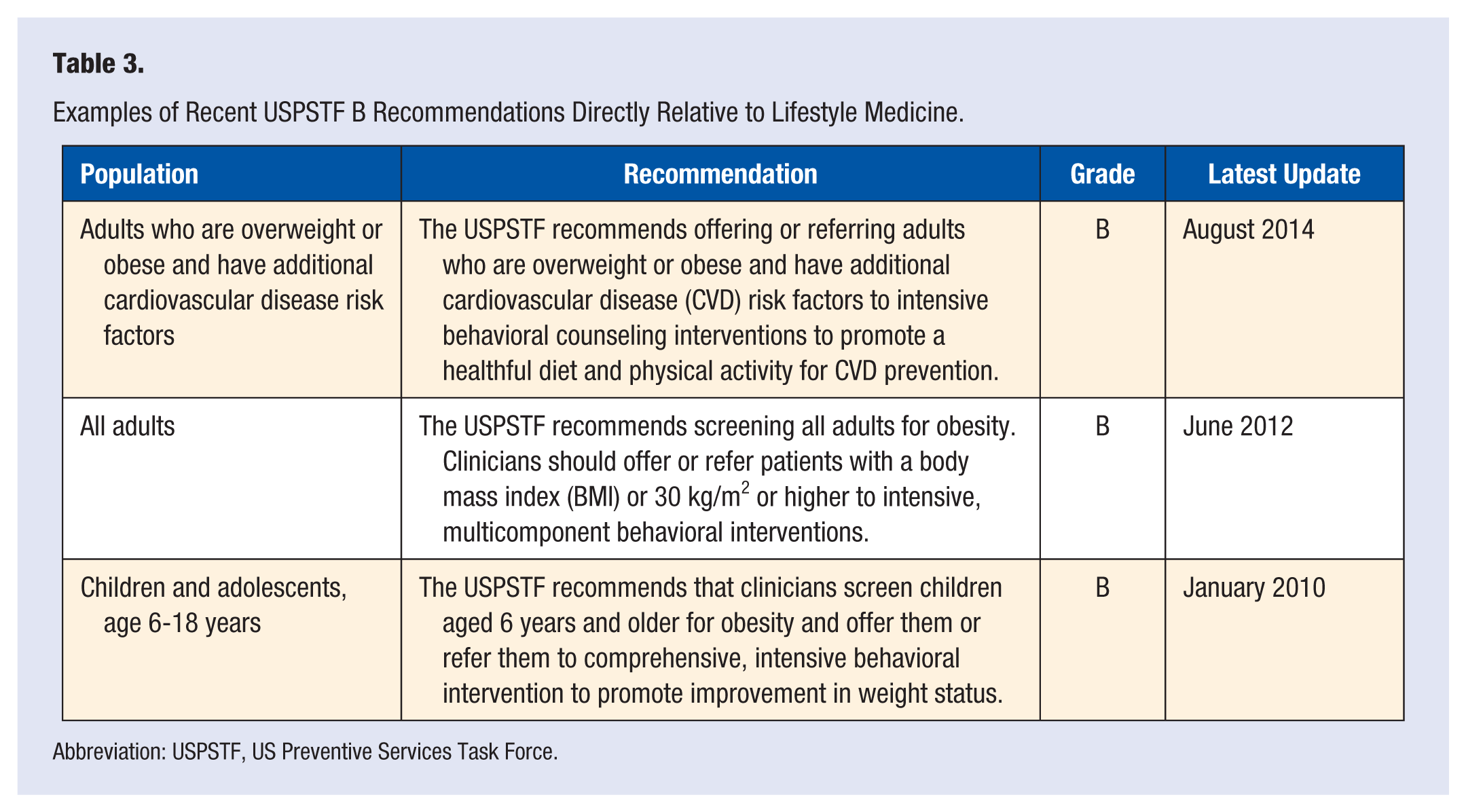
Abbreviation: USPSTF, US Preventive Services Task Force.
Additionally, accountable care organizations were formally initiated in 2012, at which time the Centers for Medicare and Medicaid Innovation also began to fund other reform projects like the Comprehensive Primary Care Initiative. These innovations were aimed at care coordination and creating infrastructures needed for risk shifting and delivering population health. The focus on population health in health care reform has been significant. Defining population health has been elusory. There is no single widely accepted definition. It is casually discussed but poorly understood. The scholarly definition by Kindig and Stoddart in 2003 is the “health outcomes of a group of individuals, including the distribution of such outcomes within the group” focuses appropriately on outcomes.13,14 According to the accepted working definition by the Institute of Medicine, “While not a part of the definition itself, it is understood that such population health outcomes are the product of multiple determinants of health, including medical care, public health, genetics, behaviors, social factors, and environmental factors.” 15 This is the heart of population health that many miss when discussing only components such as risk sharing, cost containment, growth strategies, and identifying and increasing resources for care of the top 5% of the high-cost population. By focusing on attaining health outcomes of a population, we focus on the root casual agents of health for the entire population, specifically on the malleable health behaviors.
Yes, policies and programs affect population health. However, the health of populations is more directly affected by determinants, such as the environment, genetics, behaviors, and health services, influenced by noted disparities. ITLCs can have a significant impact on these determinants and, therefore, health outcomes, mortality, and quality of life. 16
As population health is scaled and payment reform becomes more aggressive, greater financial risk will be assumed by the provider/system and patient. The question continues to be asked, “How well can we manage the patient?” A better question to ask is, “How can we engage the patient in health improvement and optimal health outcomes?” This is where ITLCs will be very effective. True positive shifting of a population’s health is the sustainable answer; otherwise we are just shifting the burden of cost or causing a temporary reduction in care.
These, among other policy changes, are creating an environment where the care of the individual is supporting population health improvement in all forms of preventive care. ITLCs will assist in these efforts by equipping the patients with a sense of empowerment in changing and sustaining health risk behaviors. When patients are engaged in their own health care, health care spending decreases, health outcomes improve, and patients feel they have had a better experience, 17 a strong strategy for the triple aim. With the cost of health care shifting directly to the patient, patient engagement should not only be promoted but also actively offered.
Since 1991, the Institute for Healthcare Innovation (IHI) has been influencing the redesign of health care delivery, specifically in 2007 with the introduction of the triple aim: essentially enhancing patient experience, improving outcomes, and reducing costs. This has been improved on by adding an additional aim to become the quadruple aim: improving the work life of health care providers, noting that provider burnout imperils the triple aim. 18 When patients are engaged in their own health care, providers are likely to be happier. ITLCs have the potential to help providers work to the level of their licensure. Physicians will have more time for difficult decision making and relationship building, two key components of the value of the doctor and enhancing the patient–doctor relationship.
We are ready for a revolution of health care delivery, which includes health promotion embedded and valued in primary care. Continuing to value and pay for primary care has been shown to create a 6-fold annual return in the Medicare population through simulations done by the Commonwealth Fund. 19 ITLCs have a valuable place in this system. What will get us to a sustainable model of health care will be a focus on primary, secondary, tertiary, and quaternary prevention as opposed to our current system that drives disease care.
Conclusion
The health expenditures by sponsor in 2012, according to the Centers for Medicare and Medicaid Services (CMS), 20 noted that 44% of health care was being paid by the government, 28.4% by households, 6.9% by other (such as philanthropy), and 20.7% by businesses. Please keep in mind that the government and the insurers do not generate the revenue to pay for health care. They are adjudicators. So in actuality, it is individuals and corporations in the United States who pay for health care. We should have a strong voice in what we value in health care, but what are we willing to pay for? This is a critical conversation as we transform to a value-based care system.
A significant landmark in treatment legitimacy for ITLCs happened in 2010 with the passage by Medicare of the Undo It Program by Dr Dean Ornish. He lobbied for 16 years with evidence-based science and data. Medicare valued the outcomes and evidence of this ITLC. This is something of value that government and insurance sponsors are now willing to pay for.
Evidence-based medicine algorithms overwhelmingly promote lifestyle change as the initial intervention. Offering effective evidence-based ITLCs should be considered as the basis for standard clinical care. ITLCs satisfy the goals of the quadruple aim. ITLCs will further increase patients’ access to preventative services in health counseling.
In health care reform, we need to promote low-cost, high-impact interventions that affect the majority of the population. ITLCs meet this goal. This has been the recent focus of CMS, IHI, and the PPACA. If we do not continue to promote and create the environment for covered ITLCs, we will have lost one of the greatest interventions for shifting the health of this nation. This is our responsibility as lifestyle medicine providers and our responsibility as consumers of health care in the United States. It is also our responsibility to provide a better future.
Footnotes
Authors’ Note
This study was presented at Lifestyle Medicine 2014, San Diego, CA, October 19-22, 2014.