
Abstract
Racial differences have been observed in stroke-related knowledge and knowledge of specific stroke risk factors and stroke prevention practices. Using data from 134 male stroke survivors, racial differences in overall knowledge, risk factor knowledge, and stroke prevention practices were examined using the Stroke Knowledge Test. Knowledge that diabetes doubles ones risk of stroke was present in 48% of the participants, while knowledge of aspirin in the prevention of stroke by stopping blood clot formation was reported in 83% of the participants. Findings indicate participants were knowledgeable that obesity increased risk of stroke (71%) and high blood pressure was the most important stroke risk factor (70%). Participants indicated knowledge that diet, exercise, and controlling blood pressure and cholesterol reduces risk of stroke (86%). In regression models, there were no significant race differences in overall stroke knowledge or the odds of knowledge of information related to stroke risk factors and stroke prevention practices after adjusting for age, education, and marital status. Although stroke-related knowledge did not differ by race, stroke survivors exhibited gaps in stroke knowledge particularly of knowledge of common risk factors. These factors should be considered in approaches to improve stroke-related knowledge in all stroke survivors.
Background
Annually approximately 795,000 individuals experience a stroke in the United States and at a cost of approximately $19 billion (Roger et al., 2012). These estimates represent only a fraction of the estimated 15 million individuals who suffer strokes worldwide (World Health Organization, 2012). Sadly, five million individuals who suffer a stroke will die and five million more will be left with permanent disability (World Health Organization, 2012). Those who do survive face a 3% to 10% short-term risk of recurrent stroke within 2 days of their initial stroke and a 9% to 17% risk within the first 30 days after their stroke (Giles & Rothwell, 2007; Wu et al., 2007).
Recently there has been a decrease in overall stroke incidence in the United States. However, the same has not been observed for minorities (Kleindorfer et al., 2010). At the same time, racial minorities experience strokes at younger ages and have greater stroke-related death rates, greater initial stroke severity, and greater residual impairments (Gaines & Burke, 1995; Gillum, 1999; Green & King, 2010; Horner, Swanson, Bosworth, & Matchar, 2003; Jha, Shlipak, Hosmer, Frances, & Browner, 2001; Jones et al., 2000; Kleindorfer, 2009; Kuhlemeier & Stiens, 1994; Shen, Washington, & Aponte-Soto, 2004). Additionally, those racial minorities who do survive strokes are more likely to have negative outcomes compared with their nonminority counterparts (Horner et al., 2003; Shen et al., 2004). Unfortunately, the specific reasons for racial differences in stroke incidence, mortality, and outcomes are unknown (Cruz-Flores et al., 2011).
Because of the significant risk of initial and recurrent stroke, particularly among racial minorities, health care providers are challenged to emphasize primary and secondary prevention in this high-risk population. According to the American Heart Association, modest lifestyle changes can substantially reduce the risk of stroke and other cardiovascular diseases (Artinian et al., 2010). Stroke risk factors and strategies to reduce them are well established (Artinian et al., 2010).
A key first step in stroke prevention is sufficient stroke-related knowledge. The current literature suggests that stroke-related knowledge may not be optimal even among stroke survivors. Sloma, Backlund, Strender, and Skaner (2010) examined stroke-related knowledge in a sample of 182 patients with a history of stroke or transient ischemic attack and reported that <50% knew that diabetes was a risk factor for stroke. Koenig et al. (2007) also identified large deficiencies in stroke-related knowledge in a sample of 130 stroke survivors undergoing inpatient rehabilitation. Similarly, Slark, Bentley, Majeed, and Sharma (2012) reported that only 22% of stroke survivors could identify four stroke risk factors and 8% could not identify any stroke risk factor in a study of 622 stroke survivors. Finally, Sullivan and Waugh (2005) reported no difference in stroke-related knowledge between stroke survivors and a matched community-dwelling sample. Because stroke-related knowledge is a key component of adequate stroke risk management, it can be hypothesized that many stroke survivors continue unhealthy prestroke lifestyles because of incomplete or unclear knowledge of their condition (Cheng, Jolly, Jones, & Cohen, 2005; Qureshi, Suri, Guterman, & Hopkins, 2001).
Racial and ethnic differences have been reported in baseline stroke-related knowledge in the general population (Biederman et al., 2012). Biederman et al. identified knowledge deficits that were more pronounced among Hispanics residing in two North Carolina counties in the “stroke belt.” To date, it is unclear if racial or ethnic disparities also exist in stroke-related knowledge in stroke survivors or whether such disparities are potential contributors to differences in stroke risk factor management. As a critical first step, the objective of this study was to examine stroke-related knowledge in a sample of Black and White male stroke survivors and to determine whether stroke-related knowledge differed between two race groups. Stroke-related knowledge was examined using the Stroke Knowledge Test (SKT) with emphasis on five specific questions designed to further examine each participant’s knowledge of key stroke risk factors and stroke prevention practices. The primary hypothesis of this study was that race disparities in stroke-related knowledge would exist in stroke survivors with lower stroke-knowledge present among Blacks compared with Whites.
Method
This was a cross-sectional pilot study of stroke-related knowledge among a sample of male stroke survivors. The study was approved by the Medical University of South Carolina institutional review board. Data were collected and analyzed from a sample of male stroke survivors. This data were completed in 2011-2012 as part of a larger study of race differences in stroke-related outcomes. Data were collected at the Medical University of South Carolina (MUSC) and the MUSC affiliated Charleston, SC VA Medical Center (VAMC). All participants had experienced an ischemic stroke within 2 years of participation in the study. Participants recruited at MUSC were patients identified by the outpatient stroke clinic staff. Ninety percent (95) of eligible patients agreed to participate during their clinic visit. Participants recruited at the VAMC were patients identified based on ICD-9 codes for stroke and receiving care for stroke within the prior 2 years. A letter signed by their primary care physicians was sent to those patients explaining the study and providing a telephone number to call if they were interested in participating. Approximately 75% (39) of patients who were sent letters responded and agreed to participate in the primary study. The author obtained written consent from all participants regardless of site.
Outcome Variables
Demographics
Demographic data were collected and included the following: age, age at time of stroke onset, education, marital status, and usual source of care. Race was identified as follows: non-Hispanic White (Whites) and non-Hispanic Black (Blacks). Education was measured using three levels of education: less than high school graduate, high school graduate, more than high school graduate. Marital status was defined as married and not married. Usual source of care was defined as having a usual primary care provider or not having a primary care provider.
Stroke-Related Knowledge
Stroke-related knowledge and knowledge of specific stroke risk factors and stroke prevention practices were measured using the SKT. The SKT is a 20-item multiple-choice test designed to measure knowledge and understanding of stroke, stroke risk, stroke risk factors, and stroke prevention practices (Sullivan & Dunton, 2004). The SKT is a valid and reliable tool for assessing stroke knowledge. Psychometric analysis of the test demonstrated good construct validity (scores increased after stroke education) and reliability (internal consistency and test–retest reliability; Sullivan & Dunton, 2004). One question related to stroke incidence was adapted to reflect the current incidence of stroke in the United States. In addition to calculating a SKT total score, five specific questions were used for further examination of each participant’s knowledge of specific stroke risk factors and stroke prevention practices. The five selected questions were the following: (a) Which of the following will double your risk of stroke? (if you are asthmatic, diabetic, exercise too much or all of the above); (b) Taking aspirin assists in preventing stroke by (stopping the formation of blood clots, getting rid of a headache, settling your stomach, relieving stress or I don’t know); (c) You are at greater risk of stroke if (you are obese, exercise regularly, give up smoking, all of the above or I don’t know); (d) The most important known risk factor for stroke is (genetic, heart attack, high blood pressure, old age or I don’t know); and (e) To reduce the risk of stroke you need to (eat well and exercise regularly, ensure your blood pressure is not too high, monitor your cholesterol levels, all of the above or I don’t know). The test was administered in the same manner in both research sites.
Data Analysis
PASW Statistics (formerly SPSS) 18 was used for statistical analyses (SPSS, 2007). Descriptive statistics and knowledge of stroke risk factors were reported as means (SD) or frequencies stratified by race. Linear regression was used to evaluate the total SKT score by race adjusted for age, education, and marital status. Similarly, logistic regression was used to evaluate the knowledge of risk factors for stroke by race adjusted for age, education, and marital status.
Results
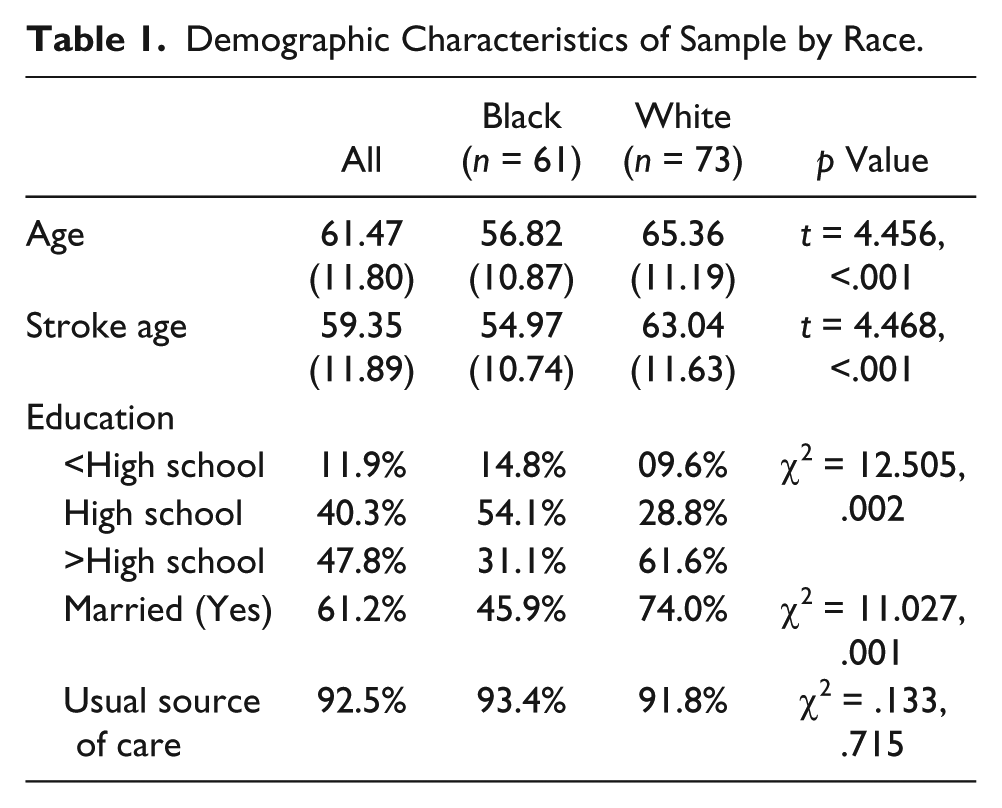
The sample consisted of 134 adult male stroke survivors. Of these 73 (54%) were White and 61 (46%) were Black. The age of the overall sample was 61 (±11.8) years. Black participants were significantly younger than the White participants at both the time of stroke onset and time of participation in the study (t = 4.456, p < .001). The majority of the total sample had a high school education or greater and educational levels differed by race (χ2 = 12.505, p = .002). Racial differences were reported in the number of participants who were married (χ2 = 11.027, p = .001) and the majority (93%) of the participants reported having a usual source of care (see Table 1).
Demographic Characteristics of Sample by Race.
Race Differences in Stroke-Related Knowledge and Knowledge of Stroke Risk Factors and Stroke Prevention Practices
The mean total SKT score was 11.6 of a possible 20.0 for all participants. White participants had higher mean scores (12.27) when compared with Blacks (10.75) (t = 2.655, p = .009) (see Table 2). Specific questions related to stroke risk factor knowledge showed that awareness that diabetes doubles ones risk of stroke was present in 48% (65) of the sample, that aspirin prevents stroke by stopping the formation of blood clots in 83% (111), that obesity doubles your risk of stroke in 71% (95), that high blood pressure was the most important stroke risk factor in 70% (94), and awareness that diet, exercise, and controlling blood pressure and cholesterol reduces your risk of stroke was present in 86% (115) of the sample. More Whites (89%) than Blacks (75%) reported that aspirin prevents stroke by stopping the formation of blood clots (χ2 = 4.343, p = .037), but more Blacks (79%) than Whites (63%) reported that high blood pressure was the most important risk factor for stroke (χ2 = 3.899, p = .048).
Stroke-Related Knowledge and Knowledge of Stroke Risk Factors and Stroke Prevention Practices by Race.

Race Differences in Overall Stroke-Related Knowledge and Odds of Knowledge of Stroke Risk Factors and Stroke Prevention Practices by Race
Table 3 reports the contribution of race to total stroke knowledge and the odds of knowledge of information related to stroke risk factors and stroke prevention practices by race. After adjusting for age, education, and marital status, there were no race differences in overall stroke knowledge. Similarly, with Whites as the comparison group and adjusting for age, education, and marital status, there were no significant race differences in knowledge of stroke risk factors or stroke prevention practices.
Odds of Knowledge of Stroke Risk Factors and Stroke Prevention Practices.

Note. CI = confidence interval. White race is comparison group. Odds ratio adjusted for age, education, and marital status.
Discussion
The findings of this study did not support the primary hypothesis that lower stroke-knowledge would be present among Black stroke survivors when compared with Whites. Although such findings have been previously reported (Biederman et al., 2012), no such disparities existed in this sample. Despite a lack of racial differences in stroke-related knowledge, two key findings did emerge that are important to understanding poststroke knowledge. The first key finding was that stroke-related knowledge was limited in the overall sample. Finding limited stroke-related knowledge among male stroke survivors was not entirely surprising. The mean stroke-related knowledge score of the participants in this study (11.58) was slightly higher than previously reported in sample of stroke survivors (10.78; Sullivan & Waugh, 2005). In addition, less than 50% of the sample knew diabetes doubles the risk of stroke and more than 25% of the sample did not know obesity doubles the risk of stroke and that high blood pressure was an important risk factor for stroke. Similarly, more Whites than Blacks knew that aspirin prevents stroke by stopping the formation of blood clots and more Blacks than Whites knew that high blood pressure was the most important risk factor for stroke.
Limited stroke knowledge among stroke survivors is a concern because adequate knowledge is considered necessary for behavior change particularly among individuals with chronic diseases (Maasland, Brouwer-Goossensen, den Hertog, Koudstaal, & Dippel, 2011). It is unclear why stroke-related knowledge is not optimal in this high-risk population. Some stroke-related information (warning signs, risk factors, and prevention/risk reduction strategies) appears more salient, thereby facilitating greater understanding and recall. In either case, improving stroke-related knowledge is critical to facilitating compliance of health behaviors and reduction of overall stroke risk. Improving stroke-related knowledge among stroke survivors is not without its unique issues. According to Maasland et al. (2011), special consideration must be given to stroke survivors due to: (a) older age, (b) poststroke disability and handicaps that limit some physical behavioral changes, and (c) cognitive impairments that reduce their ability to understand, retain, and apply information. In addition, stroke survivors must be willing to initiate behavior changes to reduce their risk of recurrent stroke.
The second key finding was that in our study of Black stroke survivors were younger and less educated than Whites, thereby raising concern about the role of demographic characteristics in stroke education and risk factor management. Experiencing a stroke at a younger age among Blacks compared with Whites has been established in the literature (National Stroke Association, 2013). Similarly, it is well known that the prevalence of stroke is highest among Blacks, those less educated, and those residing in the southeastern United States or “Stroke Belt” (Centers for Disease Control and Prevention, 2012). However, it is unclear how younger age influences stroke risk or risk factor education in this high-risk group. Understanding which variables influence the success of educational programs is important because many health professionals educate patients based on what they think the patient should know (Maasland et al., 2011). Consequently, this belief may contribute to limited presentation of critical information as well as patients being dissatisfied with the quality of stroke education that they are receiving (Maasland et al., 2011). Limited education and subsequently reduced knowledge of critical information is at least one contributor to poor poststroke risk factor management (Cadilhac et al., 2011).
It is also important to note that knowledge alone will not facilitate optimal poststroke risk factor management. Knowledge is only one critical component of poststroke management programs that must also emphasize setting goals, practicing skills critical to the poststroke management of risk factors, and empowerment of the individual with the necessary problem-solving skills needed to live well with chronic disease (Cadilhac et al., 2011; Lorig et al., 1999; Lorig & Holman, 2003; Lorig, Ritter, Laurent, & Plant, 2006). Such programs must also promote the necessary self-efficacy for self-management of risk factor management strategies (Cadilhac et al., 2011; Lorig et al., 2006; Lorig, Ritter, & Plant, 2005). Finally, information should be tailored to unique patient issues, needs, and concerns while also being patient centered, interactive, personalized, and repetitive (Maasland et al., 2011; Sloma et al., 2010).
There are a few limitations to report. The small sample size of this pilot study may have contributed to the lack of significant differences between Blacks and Whites and preclude generalization to larger populations. It is possible that other variables not collected could have significant contributions to knowledge. Time since the occurrence of stroke was variable. It can be argued that those who were closer to 2 years poststroke may have had greater opportunities to obtain stroke-related knowledge than those experiencing their stroke more recently. Knowledge was only examined in men, and including women in future studies is warranted. Knowledge data was collected using a quantitative approach. Examining knowledge using a qualitative approach could potentially yield a greater understanding of stroke-related knowledge (O’Connell & Hartigan, 2011). Validity and reliability of the extraction and analysis of data on the five specific questions has not been established in the literature and the results of these outcomes should be considered with some caution.
Conclusions
In spite of these limitations, this study offers insights into stroke-related knowledge in stroke survivors. Age and educational attainment are variables that may be variables that should be give greater consideration in the educational process of stroke survivors. Similarly, health care providers that provide care at each stage in the post-stroke care continuum have an important opportunity to facilitate stroke-related knowledge and potentially decrease the stroke survivor’s risk of stroke.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by a pilot grant from the Medical University of South Carolina Center for Health Disparities Research and a VA HSR&D Career Development Award (CDA-1 #07-012-3).