
Abstract
Objective
Due to variability in reports, the aim of this meta-analysis was to evaluate the incidence and risk factors of post-stroke early seizures (ES) and post-stroke epilepsy (PSE).
Methods
The MEDLINE, EMBASE and Web of Science databases were searched for post-stroke ES/PSE articles published on any date up to November 2020. Post-stroke ES included seizures occurring within 7 days of stroke, and PSE included at least one unprovoked seizure. Using random effects models, the incidence and risk factors of post-stroke ES and PSE were evaluated. The study was retrospectively registered with INPLASY (INPLASY2023100008).
Results
Of 128 included studies in total, the incidence of post-stroke ES was 0.07 (95% confidence interval [CI] 0.05, 0.10) and PSE was 0.10 (95% CI 0.08, 0.13). The rates were higher in children than adults. Risk factors for post-stroke ES included hemorrhagic stroke (odds ratio [OR] 2.14, 95% CI 1.44, 3.18), severe strokes (OR 2.68, 95% CI 1.73, 4.14), cortical involvement (OR 3.09, 95% CI 2.11, 4.51) and hemorrhagic transformation (OR 2.70, 95% CI 1.58, 4.60). Risk factors for PSE included severe strokes (OR 4.92, 95% CI 3.43, 7.06), cortical involvement (OR 3.20, 95% CI 2.13, 4.81), anterior circulation infarcts (OR 3.28, 95% CI 1.34, 8.03), hemorrhagic transformation (OR 2.81, 95% CI 1.25, 6.30) and post-stroke ES (OR 7.24, 95% CI 3.73, 14.06).
Conclusion
Understanding the risk factors of post-stroke ES/PSE may identify high-risk individuals who might benefit from prophylactic treatment.
Introduction
Stroke is the third leading cause of death and a major cause of disability in developed countries, affecting one in six adults, 1 and is the cause of about 55% of newly diagnosed seizures and 10% of epilepsy cases among the elderly.2,3 There is variability in the reported incidence of post-stroke seizures, ranging from 2% to 20%, 3 as well as incidence of post-stroke epilepsy (PSE), ranging from 6% to 15%. 4 Variability in findings may be related to differences in study population, methodology, stroke etiology, when the seizures occur in relation to the stroke, and the definition used for post-stroke early seizures (ES), late seizures, and epilepsy.
The International League Against Epilepsy (ILAE) defines post-stroke ES as seizures occurring within 7 days of an acute stroke. 5 Post-stroke ES are postulated to be related to local cellular biochemical dysfunctions that have not altered neuronal networks. 6 PSE is defined as two unprovoked seizures or a single seizure associated with an enduring condition that increases the chance of future seizures, if the probability of further seizures is similar to the general recurrence risk (at least 60%) after two unprovoked seizures, occurring over the next 10 years. 7 PSE includes late seizures occurring more than 7 days after an acute stroke, 5 and is postulated to be related to gliotic scarring with secondary neuronal excitability and epileptogenesis, with alteration in the neuronal networks. 4 A prior study showed that patients presenting with a single late seizure post-stroke carry a 10-year risk of subsequent seizures of 71.5%. 8 Hence, late seizures are classified as PSE.
Two meta-analyses have evaluated the risk factors for post-stroke ES and PSE. Ferlazzo et al. 9 evaluated the risk of PSE and Zhang et al. 10 assessed risk factors for both post-stroke ES and PSE. Both studies evaluated a number of risk factors, including intracerebral hemorrhage, cerebral infarction with hemorrhagic transformation, stroke severity, cortical involvement and alcoholism. However, additional risk factors, such as age and stroke territories, and the association between post-stroke ES and PSE, have not been evaluated previously. The objective of the present systematic review and meta-analysis was to evaluate the incidence and risk factors relating to post-stroke ES and the development of PSE.
Materials and methods
Search strategy
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guideline. 11 In error, the study was not prospectively registered, but has been retrospectively registered with INPLASY (DOI: 10.37766/inplasy2023. 10.0008; registration No. INPLASY2023 100008). Institutional research ethics board approval was not required for this meta-analysis. The MEDLINE, EMBASE, and Web of Science databases were searched in November 2020 for relevant articles, using the following key terms: (1) stroke, (2) seizure or epilepsy, and (3) incidence, risk factors, and prognosis (Supplementary Table 1). There were no limits placed on publication dates.
The study population included patients who developed post-stroke seizures or epilepsy. Inclusion criteria were primary studies (observational studies), ischemic stroke (both arterial and venous stroke), hemorrhagic stroke, and post-stroke seizures or epilepsy. If there were multiple studies reporting on overlapping patient populations from the same center, the study with the largest population was selected. Exclusion criteria were extra-axial (epidural, subdural and subarachnoid) hemorrhages, patients who had a history of epilepsy before the stroke, studies with less than five patients, non-English language articles, abstracts, conference publications, editorials, and nonhuman studies. Two researchers (AN and PJ) independently screened titles and abstracts following the removal of duplicates, then reviewed the full-text articles for eligibility. Any disagreement was resolved through discussion.
Data extraction
Three researchers (AN, SZ, AW) independently extracted data from eligible studies; any disagreement was resolved by consensus through discussion. A data extraction excel file was used and variables extracted included authors, publication year, country of origin, setting, study design (i.e., prospective versus retrospective), number of participants, age, sex, type of stroke (ischemic versus hemorrhagic) and mean duration of follow-up. An age of 18 years was used as the cut-off to delineate pediatric from adult populations. The incidence of post-stroke ES and PSE was recorded. Additional data on risk factors, such as stroke severity (i.e., the National Institutes of Health Stroke Scale [NIHSS] score), cortical involvement, territories affected, hemorrhagic transformation, presence of post-stroke ES, and alcohol use, were also extracted.
Data analyses
Data are presented as n (%) prevalence or mean ± SD. Meta-analyses were conducted using Comprehensive Meta-Analysis software, version 3 (Biostat; Englewood, NJ, USA) and a P value <0.05 was considered statistically significant. A random effects model was used to calculate the pooled estimates of incidence and risk factors, and 95% confidence intervals (CIs), and was used to account for heterogeneity between studies, assessed using the I2 statistic. Meta-analyses of the pooled incidence rate and 95% CIs for post-stroke ES and PSE were conducted, and the findings were displayed using forest plots. Pooled odds ratios (ORs) and 95% CIs were calculated for the risk factors of post-stroke ES and PSE, including age, stroke type, severity of stroke (based on NIHSS), cortical involvement, territories affected, hemorrhagic transformation, post-stroke ES, and alcohol use. For the risk factor of age, there was variability in the age groupings used by individual studies included in the meta-analysis. For the present study, different age groupings were collapsed and patients aged < 65 years were compared with those aged ≥ 65 years. Similarly, for stroke severity, the definitions of NIHSS categories varied between different studies, so patients were dichotomized for comparison into those with NIHSS score > 15 and those with NIHSS score ≤ 15. For the territories affected, total anterior circulation infarction and partial anterior circulation infarction were combined as anterior circulation infarct.
Subgroup analyses of the incidence and risk factors of post-stroke ES and PSE were conducted in children (aged <18 years) and adults (aged ≥18 years).
Publication bias was assessed using funnel plots. The Duval and Tweedie’s trim and fill test was performed to impute the effect estimates of potentially missing studies.
Quality of evidence
The quality of the observational studies was evaluated using the Newcastle-Ottawa scale. Cohort studies were evaluated on the following criteria: selection of cohorts (i.e., representativeness of the exposed, selection of nonexposed, ascertainment of exposure, and demonstration that outcome of interest was not present at the start of study; maximum score of 4 stars), comparability of the cohorts on the basis of design or analysis (maximum score of 2 stars), and outcomes (assessment of outcome, follow-up period, adequacy of follow up; maximum of 3 stars). Case-control studies were evaluated on the following criteria: selection of studies (adequacy of case definition, representativeness of cases, selection and definition of controls; maximum score of 4 stars), comparability of cases and controls (maximum score of 2 stars), and exposure (i.e., ascertainment of exposure, same method of ascertainment for cases and controls, and non-response rate; maximum score of 3 stars).
Results
Search results
Following removal of duplicates, a total of 5946 records were screened, resulting in 566 full-text articles that were reviewed for eligibility (Figure 1). Of these, 438 studies were excluded for the following reasons: the incidence, risk factors, or prognosis of post-stroke seizures or PSE were not reported (n = 258); not original research (n = 43); less than five participants in the sample (n = 8); the study focused on stroke patients with extra-axial hemorrhages (n = 37); overlapping patient populations from the same center (n = 76); post-stroke seizures were evaluated after surgical procedures (n = 12); or the study used animal models (n = 4). Finally, 128 studies were included in the qualitative and quantitative synthesis (Supplementary Table 2).12–139
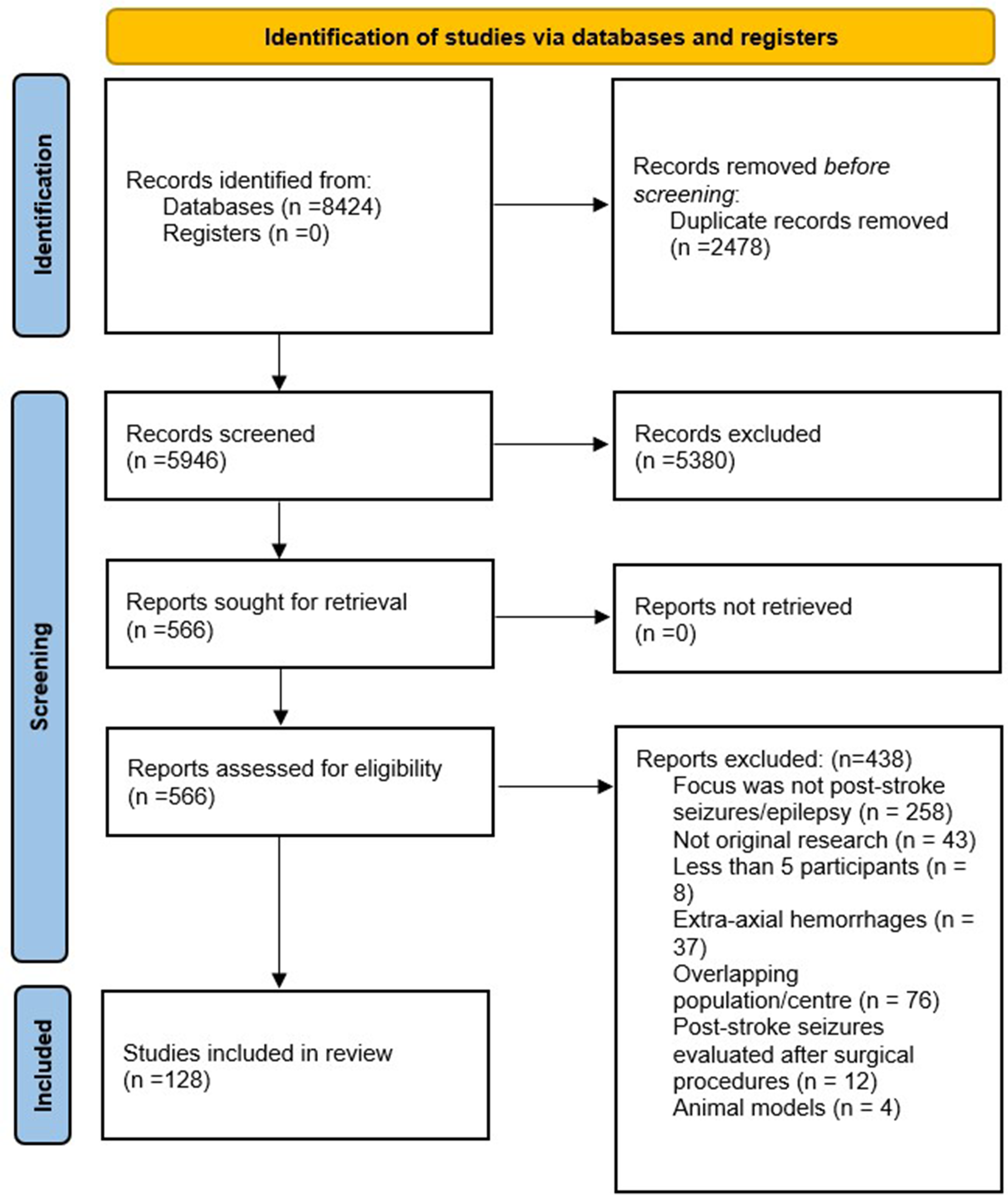
Prisma flowchart of study selection.
Study characteristics
All of the included studies were observational (80 [62.50%] were retrospective and 48 [37.50%] were prospective). Studies were from the USA (n = 22; 17.19%), Canada (n = 4; 3.13%), Europe (n = 50; 39.06%), Australia (n = 1; 0.78%), China (n = 16; 12.50%), Japan (n = 5; 3.91%), Middle Eastern countries (n = 15; 11.72%), and others (n = 15; 11.72%).
Regarding the quality of cohort studies, the mean scores were 2.90 ± 0.30 for selection, 1.21 ± 0.77 for comparability, and 2.69 ± 0.66 for outcome, with a mean total score of 6.77 ± 0.98. Regarding case–control studies, the mean scores were 3.00 ± 0.00 for selection, 1.86 ± 0.38 for comparability, and 2.71 ± 0.49 for exposure, with a mean total score of 7.43 ± 0.79. Thus, overall, the studies were considered to be of good quality based on the rating criteria.
Incidence of post-stroke early seizures and epilepsy
A total of 58 studies, comprising 204 434 participants, reported the incidence of post-stroke ES. Meta-analysis revealed that the pooled estimate for ES was 0.07 (95% CI 0.05, 0.10; I2 = 98.96; Figure 2). There was evidence of publication bias with fewer studies on the left of the funnel plot and the observed effect size was greater than the imputed effect size (0.07 versus 0.02, respectively; Figure 3).

Forest plot showing meta-analysis of the incidence of post-stroke early seizures.

Funnel plot of standard error by logit event rate for the incidence of post-stroke early seizures.
The incidence of PSE was reported by 51 studies, comprising 262 334 participants, and the pooled estimate for PSE was 0.10 (95% CI 0.08, 0.13; I2 = 99.26; Figure 4). There was evidence of publication bias with a higher number of studies on the right of the funnel plot and the observed effect size was higher than the imputed effect size (0.10 versus 0.06, respectively; Figure 5).
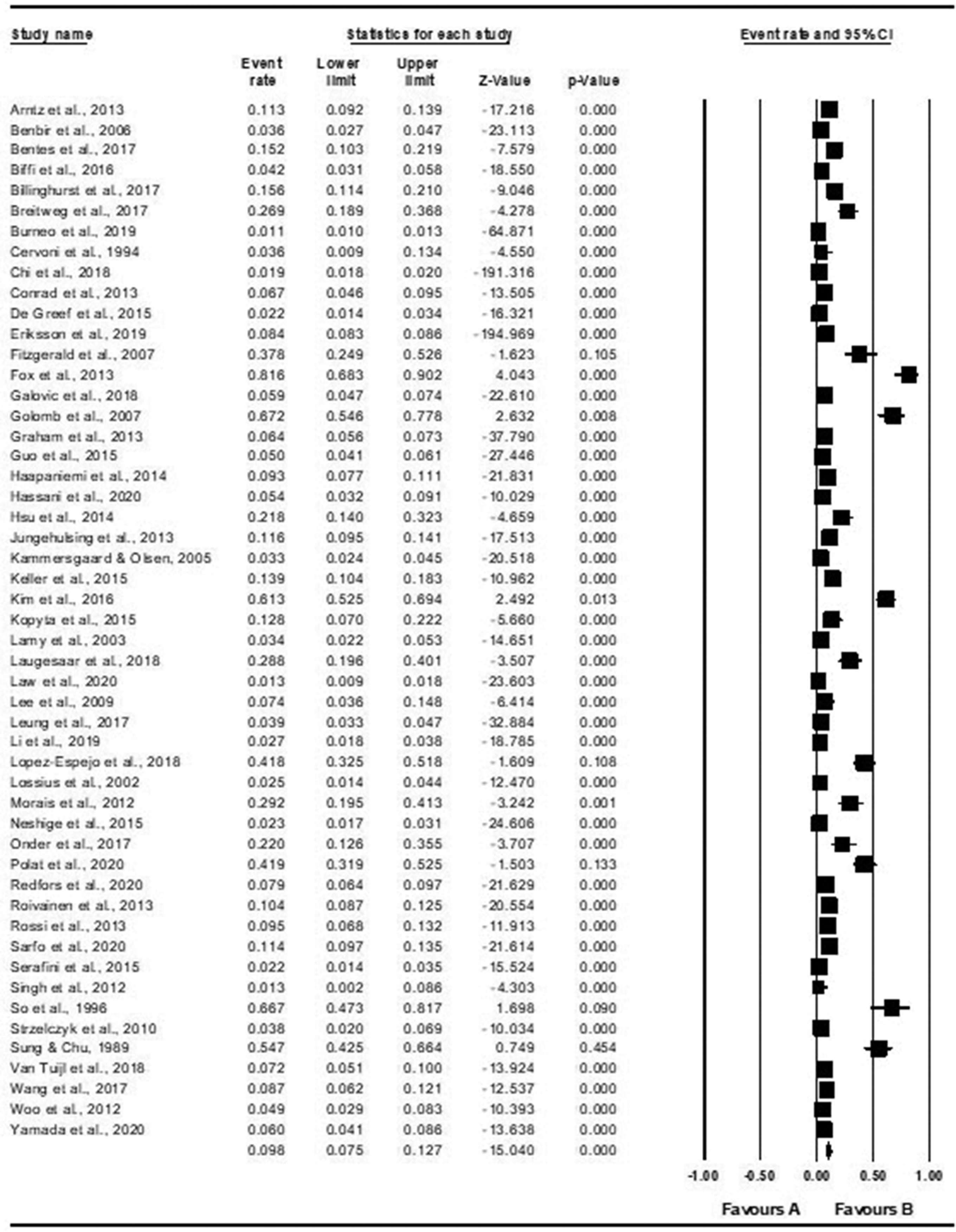
Forest plot showing meta-analysis of the incidence of post-stroke epilepsy.

Funnel plot of standard error by logit event rate for the incidence of post-stroke epilepsy.
Incidence for subgroups
A total of 49 studies in adults (n = 203 368 participants) and nine studies in children (n = 1066 participants) investigated the incidence of post-stroke ES. The pooled estimate for ES in adults was 0.05 (95% CI 0.04, 0.07; I2 = 98.74) and in children was 0.30 (95% CI 0.20, 0.42; I2 = 92.53).
The incidence of PSE was reported by 38 studies in adults, comprising 261 219 participants, and 13 studies in children, comprising 1115 participants. The pooled estimate for PSE in adults was 0.07 (95% CI 0.05, 0.09; I2 = 99.37) and in children was 0.29 (95% CI 0.19, 0.41; I2 = 91.97).
Risk factors
Early seizures
The risks of post-stroke ES were higher in those with hemorrhagic stroke compared with ischemic stroke (OR 2.14 [95% CI 1.44, 3.18], P < 0.001), more severe stroke compared with less severe stroke (OR 2.68 [95% CI 1.73, 4.14], P < 0.001), cortical involvement versus without cortical involvement (OR 3.09 [95% CI 2.11, 4.51], P < 0.001) and hemorrhagic transformation versus without hemorrhagic transformation (OR 2.70 [95% CI 1.58, 4.60], P < 0.001). Alcohol use and stroke territories affected were not associated with increased risk of post-stroke ES (Table 1).
Risk factors for developing post-stroke ES or PSE.

ES, early seizures; PSE, post-stroke epilepsy; NIHSS, National Institute of Health Stroke Scale.
Epilepsy
The odds of developing PSE were higher in those with more severe stroke compared with less severe stroke (OR 4.92 [95% CI 3.43, 7.06], P < 0.001), anterior circulation infarcts compared with posterior circulation infarcts (OR 3.28 [95% CI 1.34, 8.03], P = 0.009), cortical involvement versus without cortical involvement (OR 3.20 [95% CI 2.13, 4.81], P < 0.001), hemorrhagic transformation versus without hemorrhagic transformation (OR 2.81 [95% CI 1.25, 6.30), P = 0.01), and in those with post-stroke ES (OR 7.24 [95% CI 3.73, 14.06], P < 0.001). Age, alcohol use, and stroke type were not associated with increased risk of PSE (Table 1).
Risk by subgroup
In adults, the risk of post-stroke ES was higher in those with hemorrhagic stroke compared with ischemic stroke, more severe stroke, cortical involvement, and hemorrhagic transformation (Supplementary Table 3). In adults, the risk of PSE was higher in those with more severe stroke, those with hemorrhagic stroke compared with ischemic stroke, those with anterior circulation infarcts compared with posterior circulation infarcts, those with cortical involvement versus without cortical involvement, those with hemorrhagic transformation versus without hemorrhagic transformation, and those with post-stroke ES versus without post-stroke ES.
In children, the risk of PSE was higher in those with cortical involvement than without cortical involvement.
Discussion
The present meta-analysis assessed the incidence of post-stroke ES and PSE using a large number of studies from multiple countries, including North America, Europe, Asia, and Africa, which enhanced the generalizability of study findings. Overall, the rate of PSE was found to be higher than the rate of post-stroke ES, and rates of ES and PSE were higher in children than in adults. Risk factors for post-stroke ES included hemorrhagic strokes, severe stroke, cortical involvement, and hemorrhagic transformation, while risk factors for PSE included stroke severity, anterior circulation infarcts, cortical involvement, hemorrhagic transformation, and the presence of ES. Older age and alcohol misuse were not found to be associated with increased risk of post-stroke ES or PSE.
The present systematic review improves on previously published reviews by using definitions of ES and PSE that are consistent with ILAE guidelines, by including more studies in the analysis, and analyzing risk factors, such as age, stroke territories, and whether post-stroke ES were associated with PSE, and by conducting subgroup analyses of incidence and risk factors in adults and children.
A prior meta-analysis identified 32 studies reporting the incidence of post-stroke ES (0.04), late seizures (LS: 0.05) and PSE (0.05). 140 In the present systematic review, many more studies reporting on the incidence of PSE were identified, and the incidences of post-stroke ES and PSE were higher than those reported by the previous study. 140 There is huge variability in the reported incidence of ES, LS, and PSE in individual studies, which may be related to the population studied, methodology, country, and type and extent of stroke, with a higher incidence in hemorrhagic stroke than ischemic stroke. 140 The risk of ES is greatest in the first 24 h after stroke.58,141 The risk of PSE is highest in the 6–12 months following a stroke, 142 and 84% of those who develop PSE do so within the first 2 years after a stroke. 58 In the present study, a more detailed timing of ES or PSE was not considered.
Previous meta-analyses have evaluated the risk factors for different categories of post-stroke seizures and PSE. For example, a previous study evaluating the risk factors of PSE, in which PSE was defined as seizures occurring more than 7 days after stroke, found that cortical involvement, hemorrhagic stroke, and ES were risk factors for PSE. 9 An evaluation of risk factors for ES (i.e., seizures occurring less than 7 days after stroke) and LS (i.e., seizures occurring more than 7 days after stroke), reported that hemorrhagic stroke, hemorrhagic transformation of infarct, severe stroke, and alcoholism were associated with increased risk of ES, while cortical involvement and severe stroke were associated with PSE. 10 The present study identified further risk factors for both ES and PSE compared with the previous meta-analyses.9,10 In contrast to the study by Ferlazzo et al., 9 but similar to the meta-analysis by Zhang et al., 10 hemorrhagic stroke was not identified as a risk factor for PSE. Differences in findings may be related to the fact that Ferlazzo et al., 9 combined primary hemorrhage and hemorrhagic transformation of ischemic stroke in their definition of hemorrhagic stroke.
Hemorrhagic transformation was found to be associated with increased risk for ES and PSE in the present analyses. Hemorrhagic transformation may result in the ischemic penumbra tissue becoming more excitable, 16 and this, along with the increased irritability caused by blood degradation products on cortical neurons, 109 may predispose individuals to developing post-stroke seizures. Zhang et al., 10 did not assess whether hemorrhagic transformation increased the risk of PSE. However, hemorrhagic transformation of acute ischemic stroke has been shown to be associated with increased risk of ES and PSE. 143 In addition, ES was found to be higher among those with symptomatic hemorrhagic transformation, but not among those with asymptomatic hemorrhagic transformation. 143
Stroke is rare in children compared with adults. The prevalence of pediatric stroke is reported to be 5–25/100 000 with an incidence of 1.2–13/10 000.144–146 In the present study, the rates of post-stroke ES and PSE were higher in children compared with adults, which may be related to greater vulnerability of the developing brain to biochemical dysfunction in acute stroke, and to the generation of abnormal neural networks and epileptogenesis. Few studies have assessed the risk factors for PSE in children compared with adults. The present meta-analysis showed that cortical involvement was associated with increased risk of PSE, but hemorrhagic stroke was not associated with increased risk of PSE compared with ischemic stroke in children. More studies are needed to assess the risk factors of post-stroke seizures and PSE in children.
The results of the present systematic review and meta-analysis may be limited by several factors. First, the definition of post-stroke ES differs between published studies, varying from 1 week to 4 weeks. The present study defined ES as occurring within 7 days following a stroke, aligned with the ILAE definition of post-stroke ES, and therefore did not include seizures occurring outside this time frame in the incidence of post-stroke ES. Despite this, the present investigation included a large number of studies to assess the incidence of acute seizures post-stroke. Some studies have separated late seizures from PSE, while others have used the term LS interchangeably with PSE. In the present study, post-stroke late seizures were considered under the definition of PSE, in line with the ILAE definition of PSE.
Conclusions
In summary, this meta-analysis showed that the incidence of PSE was higher than post-stroke ES. A broad range of risk factors were also evaluated, and while some risk factors were shown to be associated with increased risk of both ES and PSE (e.g., higher stroke severity, cortical involvement, and hemorrhagic transformation), other risk factors (e.g., hemorrhagic stroke) were associated with increased risk of ES but not PSE. Understanding the risk factors of post-stroke ES and PSE will improve prognosis and may help to identify high risk individuals who might benefit from prophylactic treatment. Children (aged < 18 years) were also found to have higher rates of ES and PSE compared with adults. However, few studies have evaluated the risk factors for post-stroke ES and PSE in children, highlighting an important gap in the literature.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231213231 - Supplemental material for Incidence and risk factors of post-stroke seizures and epilepsy: systematic review and meta-analysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605231213231 for Incidence and risk factors of post-stroke seizures and epilepsy: systematic review and meta-analysis by Aathmika Nandan, Yi Mei Zhou, Lindsay Demoe, Adnan Waheed, Puneet Jain and Elysa Widjaja in Journal of International Medical Research
Footnotes
Author contributions
Aathmika Nandan: study design; data acquisition, analysis and interpretation; article drafting; and article critical revision. Yi Mei Zhou: data acquisition and article critical revision. Lindsay Demoe: data acquisition and article critical revision. Adnan Waheed: data acquisition and article critical revision. Puneet Jain: data acquisition and article critical revision. Elysa Widjaja: study design; data acquisition, analysis and interpretation; article drafting; and article critical revision.
Data accessibility
The data that support the findings of this study are available from qualified authors upon reasonable request.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.