
Abstract
Background and Objective
With more research completed using Motor imagery (MI) in people with Parkinson’s disease, this study gathered and synthesized evidence on the use of MI for Parkinson’s disease in improving rehabilitation outcomes.
Methods
Medical Literature Analysis and Retrieval System Online, Embase, Web of Science, The Cochrane Library, PsycINFO, Cumulative Index to Nursing and Allied Health Literature, and Scopus were searched from inception to May 2023. We included randomized controlled trials that examine the effects of MI on individuals with Parkinson’s disease. Two reviewers selected articles and extracted study characteristics and results independently. The Physiotherapy Evidence Database scale was used to assess the methodological quality. Mean differences and 95% confidence intervals were calculated. Heterogeneity was assessed using the I2 statistic.
Results
Thirteen articles with 12 studies were included, involving 320 individuals with Parkinson’s disease, with moderate to high methodological quality (mean = 6.62/10). Compared with the control group, 3 articles reported significant greater improvements in cognitive function, 7 reported significant greater improvement in motor function, 1 article reported significant greater improvement in quality of life, and 1 reported significant greater confidence in daily task performance. No statistically significant effects were found in the meta-analyses. Conclusion. Results of individual articles were in favor of the MI intervention. No statistically significant results were found in the meta-analyses. This might be due to the small number of studies and the heterogeneity of interventions and outcome measures used. MI may be effective in improving some rehabilitation outcomes, but meta-analytic evidence is lacking. More research with larger sample size and less heterogeneous samples, interventions, and outcome measures, is warranted.
Systematic Review Registration
PROSPERO registration number CRD42021230556.
Keywords
Introduction
Parkinson’s disease (PD) is a progressive, neurodegenerative condition affecting motor function including planning and controlling of body movements. 1 With reference to the International Classification of Functioning, Disability and Health (ICF), the motor symptoms of people with PD (PwPD) affect all areas of functioning: body structure and function, and activity and participation, including the ability to perform meaningful activities of daily living (ADL).2,3
Motor imagery (MI) is a suitable non-pharmacologic treatment for functional decline in PwPD. 4 Studies have found improvements in balance and mobility after preliminary MI interventions in PwPD. 5 In a therapeutic context, MI involves a cognitive process whereby a particular motor action or kinesthetic experience is internally reproduced (“imagined”) without any physical movement. 6 MI can also be externally cued, guided by a therapist, or internally cued by the individual themselves. 6 MI is often used in conjunction with actual task practice in rehabilitation.7-10 It has demonstrated benefits in the rehabilitation of individuals post-stroke, including improvements in task relearning and generalization,7-9 and in PwPD. 10 It also shows promising results in the treatment of brain injury, multiple sclerosis, and various other neurological conditions. 11
Imagining an action shares similar neural mechanisms as motor execution in PwPD.6,12 Both neuropsychological and neurophysiological mechanisms are involved in MI. 13 The neuropsychological mechanism is involved in practicing cognitive elements of MI. This can be manifested through breaking an action down into steps to learn the movement strategies.7-9 The neurophysiological mechanisms are proposed to include neural changes in the central nervous system. 14 Research has shown that imagined and executed actions recruit overlapping brain regions and share a similar subcortical network and the same neural structures.15,16 Therefore, PwPD who perform MI in a therapeutic context may experience improvements in motor planning and motor action execution.
There are a handful of studies showing that MI promotes improvements in PD rehabilitation.17,18 These include improved upper limb function, cognition, motivation, and ADL performance. MI is shown to be successful in PD rehabilitation when used in combination with other therapies, including action observation, relaxation and mindfulness, and virtual reality. 5 Silva et al 13 provides a description of MI protocols in their systematic review. MI combined with physical practice might be effective in improving bradykinesia, mobility, and gait speed in PwPD. However, there is no synthesized evaluation of the literature comparing the effectiveness of MI with control interventions in PD rehabilitation. Therefore, the aim of the present systematic review is to investigate the effectiveness of MI in PwPD on body structure and function, and activity and participation.
Methods
The methods were published as a protocol before conducting the review. 19 The protocol was registered in PROSPERO (registration number CRD42021230556). The Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines 20 and recommendations of the Cochrane Collaboration 21 were followed.
Eligibility Criteria
Types of Studies
This review included randomized controlled trials (RCTs). Pilot studies were eligible for inclusion. Articles that were published in English or had available translations into English were eligible. Articles where the full text was not available were excluded.
Participants
Studies including individuals with a diagnosis of PD (any age, sex, or stage of disease progression) were eligible. Studies involving PwPD and other comorbidities, such as dementia, stroke, or multiple sclerosis, were excluded.
Type of Intervention
Studies using MI as a treatment for PwPD were selected. MI refers to the cognitive process of internally reproducing or “imagining” a motor action without any physical movement. Except for use as a feedback mechanism, interventions requiring advanced equipment, such as electro-myographic stimulation or virtual reality technologies, and those combined with medication beyond the participants’ habitual medications were not included. There were no restrictions placed on control groups.
Outcome Measures
Studies that included outcomes on body structure and function (ie, cognition, psychological factors such as confidence in activities, dynamic balance, and gait and leg endurance), and activity and participation (ie, transfers, functional mobility, ADL performance, and quality of life) were included. These categories have been selected according to the ICF 2 and thus have the capacity to represent a holistic perspective on rehabilitation.
Databases and Search Strategy
Electronic searches in the Medical Literature Analysis and Retrieval System Online (MEDLINE), Embase Biomedical Answers (Embase), Web of Science, The Cochrane Library, Cumulative Index to Nursing and Allied Health Literature (via Ebscohost), Scopus, and PsycINFO (via Ebscohost) were conducted. The search strategies were created by considering terms related to the main outcomes of interest (Supplemental Material A). A systematic literature search was conducted from inception until 19 May 2023. We performed a hand search of the reference lists of the studies included in the review to identify any potentially relevant studies not retrieved during the electronic search.
Selection of Studies
Two independent reviewers (TS and KL) screened the titles and abstracts of the publications retrieved based on the eligibility criteria. Potentially relevant studies then underwent full-text analysis. The entire selection process was performed by consensus. Covidence Review was used during the selection of the studies (www.covidence.org).
Data Extraction
The same 2 reviewers (TS and KL) developed the data extraction form (Supplemental Material B). They independently piloted the data extraction form on 10% of the identified studies and modified as required prior to use. They then independently extracted the required information from each article, including study design, country/setting, sample size, mean age and sex of participants, mean stage of PD, and mean disease duration. Study characteristics were also extracted, including details of the experimental and control interventions, number of sessions and frequency of treatment, outcome measures, and major findings. The medication “OFF” phase data were included if available. Disagreements concerning data extraction were resolved through discussion.
Appraisal of Methodological Quality
The Physiotherapy Evidence Database (PEDro) scale was used for the individual appraisal of the studies included. The PEDro was scored out of 10, though item 1 is not included in the score calculation as it represents external validity. 22 Studies with a total score between 6 and 8 are regarded as having “good” methodological quality and a score of 9 to 10 is equivalent to “excellent.” 23
Synthesis and Analysis of Data
Study design, country/setting, participant, sample size and characteristics, intervention, outcome measures, and major findings were extracted from the selected studies and analyzed qualitatively. Two reviewers (TS and KL) independently categorized the outcome measures used in each article into body structure and function (cognition, psychological factors such as confidence in ADL performance, dynamic balance, or gait and leg endurance), or activity and participation (transfers, functional mobility, ADL performance, or quality of life). Any discrepancies were resolved through discussion.
The common outcome measures used in PD, such as the Unified Parkinson’s Disease Rating Scale (UPDRS), Timed Up and Go Test (TUG), were selected for the meta-analysis. The summary statistics provided were extracted from the included studies. Authors were contacted for those studies with insufficient data. One reviewer (TS) entered the data into the metafor-package in R software. 24 Another reviewer (PF) checked the entries to ensure accuracy. Any discrepancies were resolved through discussion. Where identical measurement scales were used by all studies, pooled effect sizes were reported as mean differences (MD) between experimental and control groups. The difference in post-intervention mean scores of the outcome measures were pooled in the analysis. Statistical significance is summarized as P values and 95% confidence intervals (95% CI). P-values less than 0.05 were interpreted as statistically significant. Heterogeneity was assessed using the I2 statistic. Studies with an I2 > 50% were considered to have substantial heterogeneity. The analysis was performed using a random-effects model, with results presented as forest plots. 24
Results
Description of Studies
The electronic search of the databases led to the retrieval of 1,073 publications (Figure 1). Thirteen articles were selected,25-36 involving a total of 320 PwPD (163 in experimental groups, 157 in control groups). No additional articles were found through hand searching of the reference list of included articles. Two included articles26,33 used the same participant group, and are represented accordingly as 1 study in the present review. Therefore, this review included 13 articles with 12 studies.
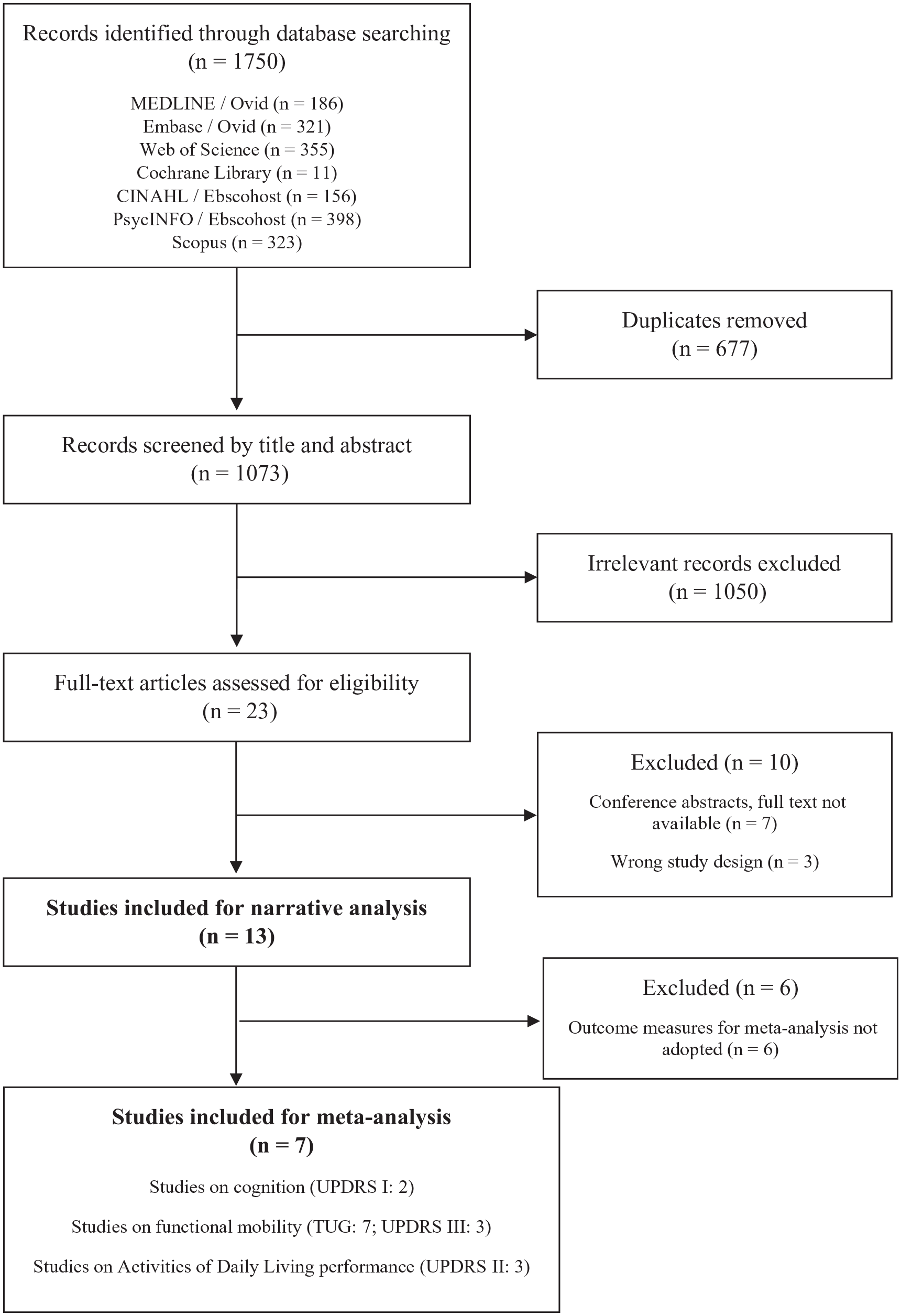
Flow diagram of the study selection process based on the PRISMA guidelines.
Appraisal of Methodological Quality
Nine of the 13 articles were indexed in the PEDro database. The mean score of all studies was 6.62 (range 3-8; Supplemental Material B, Table 1). Eleven of the 13 articles were considered to have good methodological quality.10,25,27,28,30-36 All articles scored 0 in items 5 and 6 (participant and therapist blinding).
Characteristics of Included Articles.
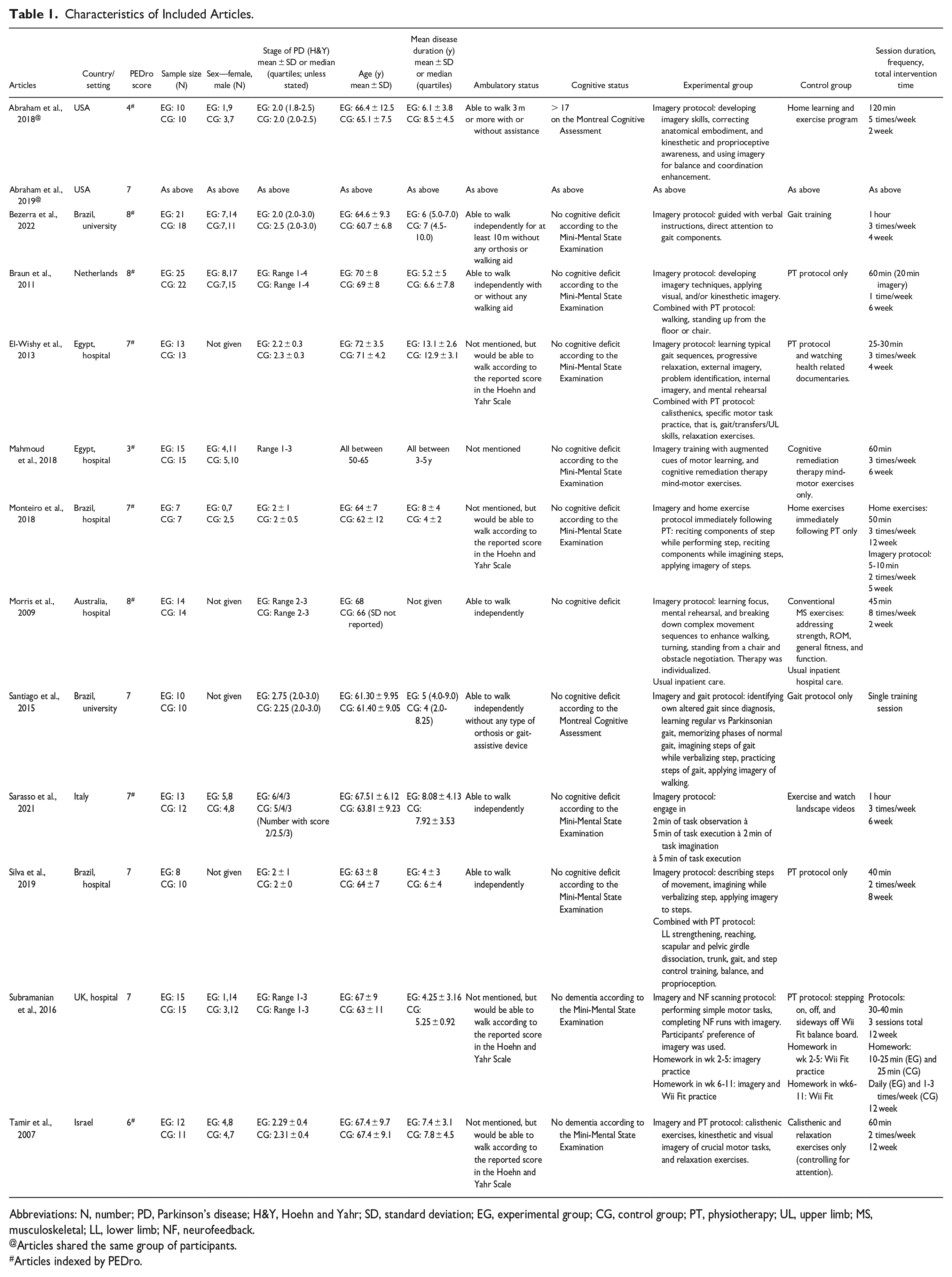
Abbreviations: N, number; PD, Parkinson’s disease; H&Y, Hoehn and Yahr; SD, standard deviation; EG, experimental group; CG, control group; PT, physiotherapy; UL, upper limb; MS, musculoskeletal; LL, lower limb; NF, neurofeedback.
Articles shared the same group of participants.
Articles indexed by PEDro.
Characteristics of Participants
The mean participant age was 66.2 years (range 50-72 years) in the experimental groups and 63.3 (range 50-71) in the control groups (Table 1). The sex of participants was available in 8 articles,10,26,27,29,31,34-36 with the majority being male participants (range 61.5%-100% in the experimental groups and 61.1%-80% in the control groups). The mean duration of the disease ranged from 3.0 to 13.1 years in the experimental groups and from 3.0 to 12.9 years in the control groups. Using the Hoehn and Yahr 37 scale, the stage of disease was 2 in 3 participant groups,26,28,31,33 ranged from 2 to 3 in 7 groups,10,25,27,30,32,34,35 ranged from 1 to 3 in 1 group, 29 and from 1 to 2 in 1 group. 36 Except in 1 study, 29 participants were reported to be able to walk. Participants in all selected studies reported no cognitive deficits or dementia. Two studies included a screening of their imagery ability.31,34
The minimum number of participants among the studies was 14, 31 the maximum was 47, 27 and the mean considering all studies included was 29.9.
Intervention
The selected studies reported using visual, auditory, and kinesthetic modalities during MI (Table 1). Seven of the studies included a physiotherapy protocol in the intervention.10,25,27,28,30,31,34 One included cognitive remediation therapy, 29 1 involved MI training using attention to compensate for movement difficulties, 32 1 included neurofeedback, 36 and 1 involved dual tasks. 35 The duration and frequency of the sessions ranged from 30 to 120 minutes and from 1 to 5 times per week. The total duration of the interventions ranged from 1 day to 12 weeks. One study provided only a single treatment session. 30 Aside from one article, 36 all MI protocols were supervised by therapists.
Participants in the control groups received active controls, including musculoskeletal exercises, physiotherapy protocol, Wii Fit training, cognitive remediation therapy, dual-task training, and health education.
The participants in 7 studies received the experimental or control therapy in the “ON” phase of medication.10,26,27,29-31,33,36 Other studies did not provide the information.
Evaluation Measures and Outcomes
Body structure and function were evaluated in 10 articles (9 studies),10,26,29-36 and activity and participation were also evaluated in 10 articles (Table 2).10,25-28,30-32,35,36
Major Findings of Included Articles.
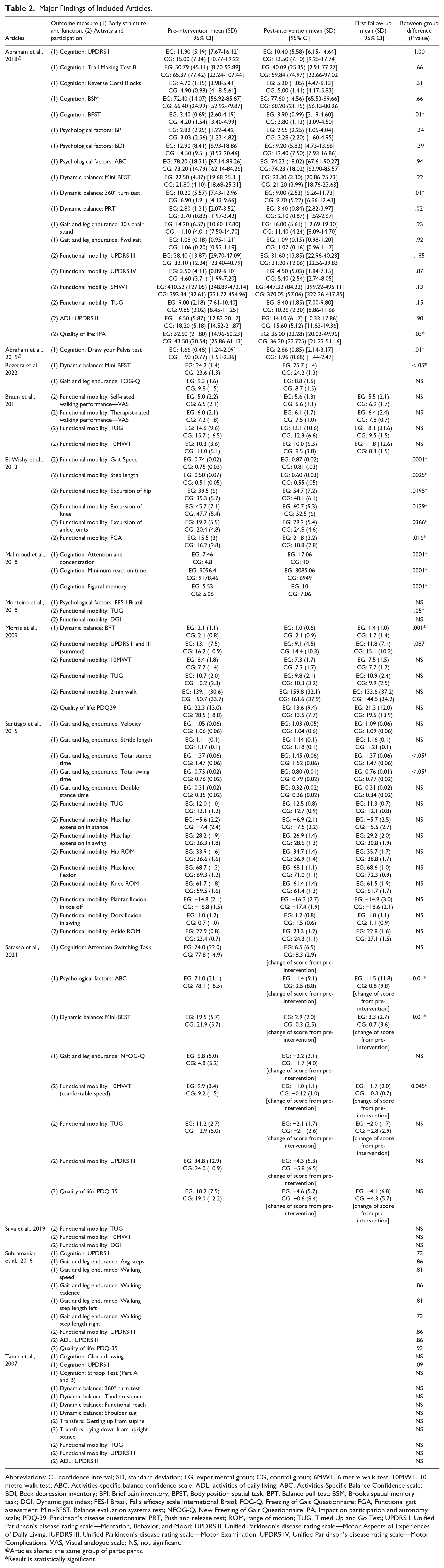
Abbreviations: CI, confidence interval; SD, standard deviation; EG, experimental group; CG, control group; 6MWT, 6 metre walk test; 10MWT, 10 metre walk test; ABC, Activities-specific balance confidence scale; ADL, activities of daily living; ABC, Activities-Specific Balance Confidence scale; BDI, Beck depression inventory; BPI, Brief pain inventory; BPST, Body position spatial task; BPT, Balance pull test; BSM, Brooks spatial memory task; DGI, Dynamic gait index; FES-I Brazil, Falls efficacy scale International Brazil; FOG-Q, Freezing of Gait Questionnaire; FGA, Functional gait assessment; Mini-BEST, Balance evaluation systems test; NFOG-Q, New Freezing of Gait Questionnaire; PA, Impact on participation and autonomy scale; PDQ-39, Parkinson’s disease questionnaire; PRT, Push and release test; ROM, range of motion; TUG, Timed Up and Go Test; UPDRS I, Unified Parkinson’s disease rating scale—Mentation, Behavior, and Mood; UPDRS II, Unified Parkinson’s disease rating scale—Motor Aspects of Experiences of Daily Living; IUPDRS III, Unified Parkinson’s disease rating scale—Motor Examination; UPDRS IV, Unified Parkinson’s disease rating scale—Motor Complications; VAS, Visual analogue scale; NS, not significant.
Articles shared the same group of participants.
Result is statistically significant.
For the body structure and function outcome category, cognition was evaluated most (in 6 articles),26,29,33,35,36 followed by gait and leg endurance (5 articles)26,30,34-36 and dynamic balance (4 articles).10,26,32,35 In the activity and participation outcome category, functional mobility was evaluated in 10 out of the 13 selected articles. The most commonly reported outcome measures used were the TUG,10,26-28,30-32,35 UPDRS,26,32,35 and 10 m walk test (10MWT).10,27,28,32,35,36
Comparing the experimental and control groups, 9 articles reported significantly better improvement in the experimental group in at least 1 component of body structure and function evaluated. In cognition, statistically significant better performances in the experimental group were found in the body position spatial task, 26 the draw your pelvis test, 33 and attention and concentration, minimum reaction time, and figural memory. 29 Regarding dynamic balance, the experimental group showed statistically significant better results in the 360° turn test, push and release test, 26 balance pull test, 32 and overall balance evaluation.34,35 One article showed a significantly better improvement in the experimental group in stance time and total gait swing time in walking. 30 One study reported statistically significant results for confidence in ADL in the experimental group. 35 Four articles reported significant improvements in functional mobility in the experimental group, with gait speed, step length, hip, knee, ankle excursion, functional gait assessment, 25 and TUG. 31 Quality of life showed statistically significant better improvements in the impact on participation and autonomy scale in the experimental group. 26 Only 3 articles measured ADL,10,26,36 but none showed a significant difference between experimental and control groups.
Meta-Analyses
The meta-analyses included 8 articles on cognition with a total of 202 participants,26-28,30-32,35,36 using the outcome measure UPDRS I, functional mobility including TUG and UPDRS III, and ADL performance using UPDRS II.
Results on Body Structure and Function: Cognition
The pooled data of cognitive outcome measures using the UPDRS I with 25 participants in the experimental groups and 22 in the control groups26,36 showed no statistical evidence in favor of MI (MD = −1.99; 95% CI, −4.82-0.85; P = .17; I2 = 0.0%; Figure 2).
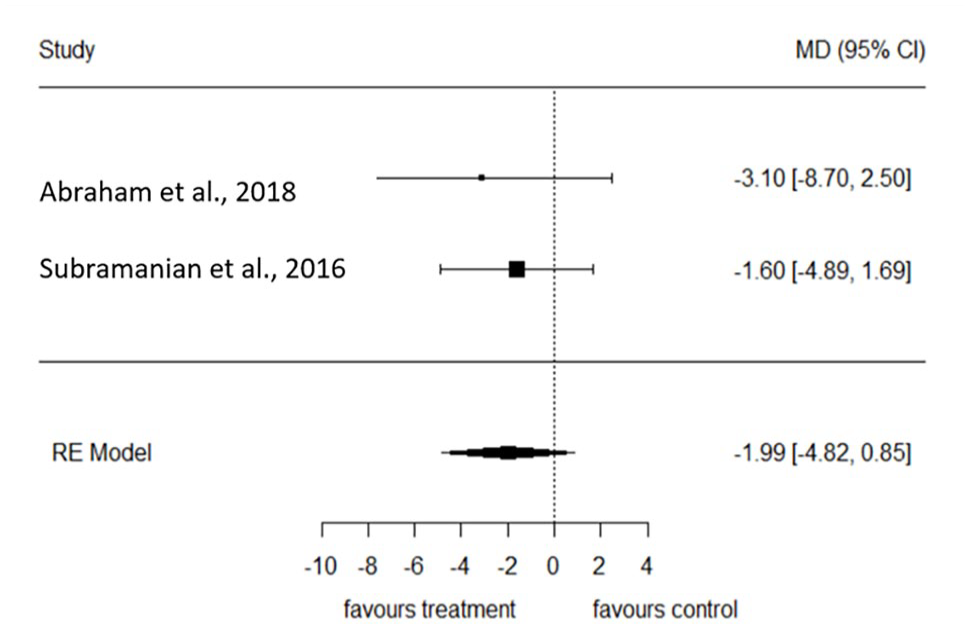
Forest plot of the effect of motor imagery on UPDRS I measure compared to control.
Results on Activity and Participation: Functional Mobility
For articles assessing functional mobility, the pooled data of the TUG26-28,30-32,35 (with 87 participants in the experimental groups and 90 in the control groups) and the UPDRS III26,36 (with 38 participants in the experimental groups and 34 in the control groups) showed non-significant results on improving mobility (MD = −0.56; 95% CI, −1.23-0.07; P = .10; I2 = 8.4% and MD = 1.46; 95% CI, −2.06-4.98; P = .42; I2 = 0.0% respectively; Figures 3 and 4).
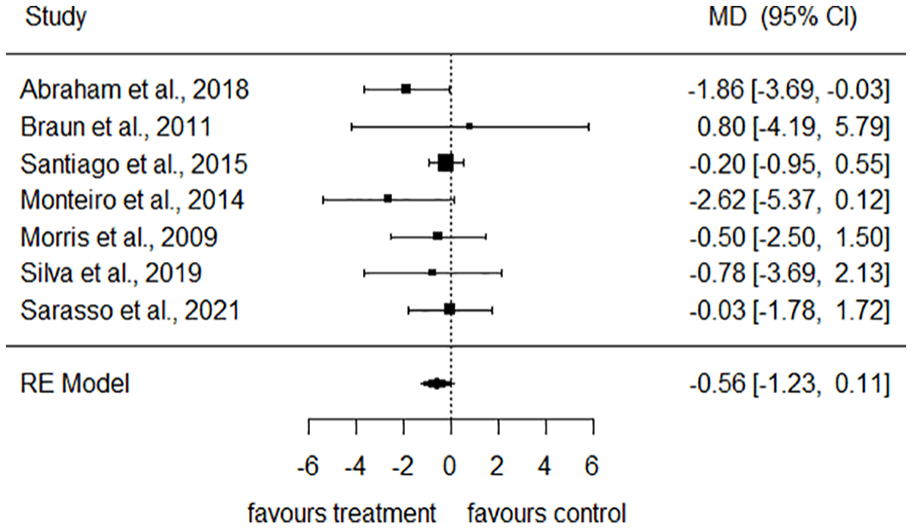
Forest plot of the effect of motor imagery on TUG measure compared to control.
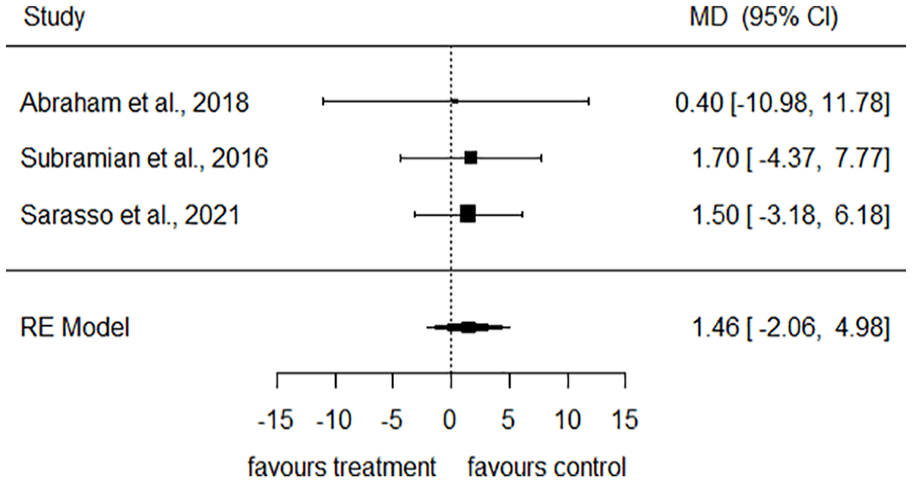
Forest plot of the effect of motor imagery on UPDRS III measure compared to control.
Results on Activity and Participation: ADL Performance
The pooled data of the UPDRS II26,35,36 (with 38 participants in the experimental groups and 34 in the control groups) showed non-significant effects on improving ADL performance (MD = 0.38; 95% CI, −2.95-3.71; P = .82; I2 = 2.1%; Figure 5).
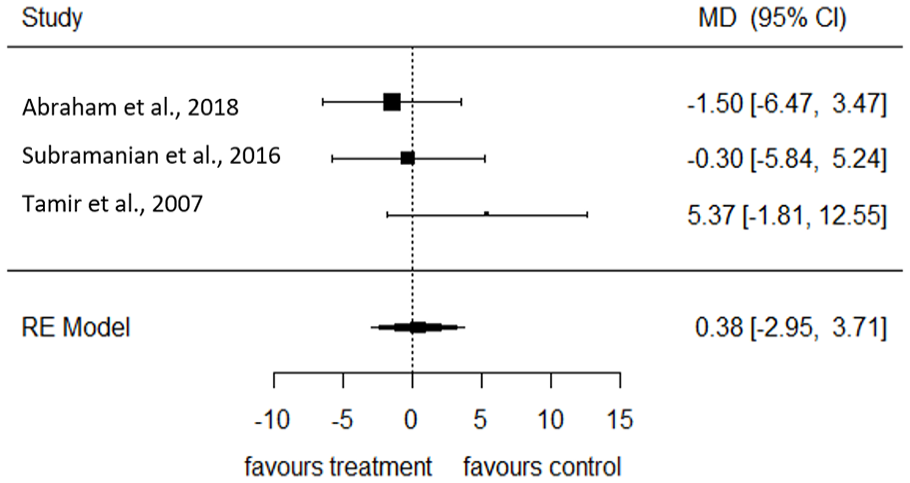
Forest plot of the effect of motor imagery on UPDRS II measure compared to control.
Discussion
The purpose of the present systematic review was to investigate the effects of MI on body structure and function, and activity and participation in PwPD. The results of the meta-analyses did not reveal statistically significant effects of MI in UPDRS I (representing cognition), TUG and UPDRS III (representing functional mobility), and UPDRS II (representing ADL performance) although individual articles reported statistically significant effects on body structure and function (cognition, dynamic balance, and gait and leg endurance) and activity and participation (functional mobility and quality of life). However, the objectively measured cognitive outcomes did show improvement in individual articles, which could yield significant effects if there were sufficient studies using each measure to include in a meta-analysis. No evidence has been found in individual articles on MI to improve other components of body structure and function (psychological factors such as confidence in activities), and activity and participation (ADL performance and transfers). Based on the PEDro scale, the average methodological quality of the included articles was rated as good (ranging from poor to good). With differences in outcome measures and inadequacies in result reporting, only a small number of articles could be included in the meta-analyses, which might have resulted in non-significant findings in the meta-analyses. Ryan and Cochrane Consumers and Communication Review Group 38 reported that 2 studies are sufficient for meta-analytic purposes, provided the 2 trials can be meaningfully pooled and their results are sufficiently similar. Zhou and Shen 39 commented that sample sizes for a study to be included in a meta-analysis would be ideally greater than 30 per group or the number of studies to be included should be more than 5. Except for the meta-analysis on the effect of MI using the TUG that included 7 studies, none of the meta-analyses in this systematic review fulfilled the recommendation. Therefore, the findings of the meta-analyses in this review should be analyzed with caution, as the real effect may be different from the estimated effect.
In body structure and function, the outcomes on cognition, psychological factors such as their confidence in activities, dynamic balance, and gait and leg endurance were included in the articles. Only 2 articles were included in the meta-analysis. This meta-analysis did not find a statistically significant effect in favor of the intervention on cognition measures. Individual study results in 3 articles reported improvements in at least 1 cognition outcome measure.26,29,33 Treatment was conducted 3 to 5 times per week in these articles. Tamir et al 10 conducted treatments twice per week only and did not report any statistically significant results in cognition (in UPDRS I, Stroop Test, and clock drawing). More frequent treatment might lead to a greater effect on cognition. Additionally, these studies only included a sample size of 10 to 15, which might limit the results.
Three included articles assessed for psychological factors (including fear of falls, confidence in activity performance, mood, and pain).26,31,35 A meta-analysis could not be performed due to the use of different outcome measures. No statistically significant improvements were reported. This could also be due to the small sample size (summed sample size of 49). There is some evidence, however, that certain psychological factors such as pain and confidence can improve in PwPD after MI.35,40
Of the 5 articles that reported outcomes in dynamic balance, 4 reported improvements after treatment with MI.26,32,34,35 A meta-analysis to investigate the effects of MI on dynamic balance was not conducted due to the dissimilarity of the relevant outcome measures in the included articles. When reviewing the MI interventions, the short protocols adopted in 2 of the articles (2 weeks) were able to promote an improvement in balance for PwPD.26,32 Muscle strength is associated with balance, 41 and postural control is linked to muscle strength. 42 Interestingly, the control groups of the articles engaged in conventional musculoskeletal exercise. Therefore, we cannot state that the improvement in dynamic balance was due to an improvement in muscle strength, but rather from the comprehensive and intensive MI protocol of the intervention, such as imagery and practice of turning, standing and the movement sequences to enhance balance and walking in Morris et al. 32 The natural progression of PD leads to a reduction in various aspects of body structure and function, including postural balance. 3 It may, therefore, be difficult for PwPD to perform ADL involving balance, such as ambulating, transfers, navigating obstacles, ascending/descending stairs, or any activities performed while standing. Therefore, improvement in these outcomes can translate to important improvements in daily task performance in this population.
Like dynamic balance, no meta-analysis was conducted for outcome measures of gait and leg endurance because of the heterogeneity of the outcome measures. Among 5 articles that had outcomes on gait and leg endurance, only 1 article showed significant improvement in the experimental group in the total stance time and total swing time of these outcomes. 30 This article utilized a gait protocol in the experimental and control groups. The experimental group also received MI training and identified their own gait changes. The addition of MI and education on their own gait improved participants’ gait and leg endurance through total stance time and total swing time in gait. It did not, however, result in statistically significant improvements for other measures including gait velocity, stride length, double stance time, and functional mobility measures. It is of note that the duration of the protocol in this article was a single session, while longer protocols26,34-36 did not report statistically significant improvements in gait and leg endurance. The mechanisms involved in the improvement of gait in PwPD are unknown. However, experiments with animal models suggest that it may be linked to a dopaminergic pathway of the brain involved in movement 43 as well as cortical and striatal function. 44 Improvements in gait and leg endurance are of significant clinical relevance, as many PwPD experience muscle weakness in the lower limbs and therefore decreased gait and leg endurance, which is associated with difficulties in daily task performance and a lower quality of life. 45
In the category of activity and participation, the outcomes from the articles that reported on transfers, functional mobility, ADL performance, and quality of life were included. Only 1 article reported outcomes for transfers as a standalone measure, and the results did not show a statistically significant improvement. 10 The result of the meta-analysis on the mobility measure TUG did not achieve statistical significance. The other mobility measure, UPDRS III, did not show statistically significant results. However, the substantial heterogeneity of the outcome measures used may indicate excessive clinical diversity in the included articles. For example, for functional mobility, besides UPDRS and TUG as the common outcome measures, other outcome measures like walk tests with different distances, gait speed, Functional Gait Assessment, Dynamic Gait Index, and self-rated and therapist-rated walking performance were used. The clinical foci in functional mobility in the selected articles were different, and there was a lack of unified assessment in functional mobility. The small number of studies using a specific outcome measure could be the cause of the non-significant findings. Of the 10 articles which assessed functional mobility, 3 articles reported an improvement after the intervention with MI.25,31,35 It should also be pointed out that in one of the articles that did not find an improvement in mobility, 32 the individuals had a good performance at baseline, which may have limited the gains after treatment.
The meta-analysis evaluating ADL performance using UPDRS II did not show statistically significant results. Despite favoring the intervention, individual articles also did not find statistically significant results in measures assessing ADL.
Four articles reported quality of life outcomes,26,32,35,36 and 1 reported an improvement after the intervention. 26 The study also demonstrated significant improvement in dynamic balance and cognition after the intervention. 26 It appears that an improvement in at least 1 domain of body structure and function may exert a positive effect on the quality of life of PwPD.
Reviewing articles with positive results indicated that the MI protocol might matter. For example, Abraham et al 26 and Morris et al 32 involved breaking down the steps of movements into smaller tasks, Bek et al 40 provided social support and heightened self-awareness for participants. Studies using a strategy called self-regulation on people with stroke were demonstrated to enhance one’s self-awareness.46-48 These MI protocols involving people with stroke to analyze task steps also showed effectiveness in improving rehabilitation outcomes.7-9 Drawing participants’ attention toward task performance may enhance their use of MI. Future MI studies for PwPD could consider building up the attention components in the intervention protocol.
One of the strong points of the present review was the classification of outcomes based on the domains of the ICF, which provides a holistic approach to rehabilitation outcomes for PwPD. The inclusion of RCTs only is important, as this study design is considered the “criterion standard” for evaluating treatments and decision-making in health. Moreover, the studies’ methodological quality was evaluated according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and resulted in an average score of moderate to high. Although no statistical significance was found in the outcomes, the inclusion of the meta-analysis enhances the precision of treatment effects and demonstrates the benefits of the intervention, if any.
We included 13 articles with 12 RCTs in the present review. The most critical points regarding methodological quality were related to allocation concealment, and blinding. Only 8 of the articles concealed the allocation of the individuals to the different groups.25,27,28,31-35 The lack of concealment can lead to a higher risk of bias, which can skew results to either an overestimation of the treatment or mask a possible effect. 49 Therefore, allocation concealment is a criterion that needs to receive greater attention on the part of researchers to reduce the risk of bias. Nine articles described the blinding of the assessors.10,27,28,30,32-36 However, blinding of the participants and therapists was not performed in any of the included articles. RCTs without blinding may yield inaccurate, biased results. 50 Although double blinding is ideal in RCTs, it may not be feasible in clinical studies of this nature. Intention-to-treat analysis was performed in 8 of the included articles, enhancing the external validity of the study.25,27,30-34,36 Regarding the selection criteria, only 2 studies included screening of the participants’ imagery ability.31,34 Participants completed the Kinesthetic and Visual Imagery Questionnaire—20 31 or the Movement Imagery Questionnaire—Revised. 34 Those who were able to perform MI were included. Another study suggested including testing participants’ imagery ability in future studies. 27
Study Limitations
Most of the articles included had a relatively small sample size of PwPD and did not present the effect size. All of the included articles utilized MI as part of a combined intervention. Two studies included non-exercising control intervention.10,29 The effect or absence of effect could be attributable to the combined treatment with MI in the experimental group. Methodological limitations include selecting articles published in English only, not investigating publication bias, excluding studies using MI with advanced equipment, and not including the percentage of agreement between the reviewers in both study selection and data extraction. Furthermore, the variety of MI and control interventions, variation in outcome measures, selection of common outcome measures for meta-analyses, incomplete reporting of results, and small sample sizes to date make it difficult to quantify the possible benefits of MI.
Implications for Practice and Research
MI is a low-cost intervention, and it can apply to individuals with varying levels of physical ability. MI is, therefore, considered a highly feasible intervention in clinical practice. It can be successfully delivered in person or through a virtual telerehabilitation service, allowing individuals the autonomy of choice and for remote communities where in-person resources are limited. MI for functional mobility, gait and leg endurance, and cognition from 20 to 60 minutes, 2 to 3 times a week for a total of 2 to 12 weeks were the most reported. Regarding body structure and function, the benefits reported in cognition and dynamic balance were observed in a protocol as short as 2 weeks (5-8 times/week); whilst benefits were reported in a protocol as short as a single training session for gait and leg endurance. Regarding activity and participation, benefits were reported on mobility in a protocol as short as 4 weeks (3 times/week); for quality of life, benefits were reported in a protocol as short as 2 weeks (5 times/week). However, this systematic review provided information on the frequency and duration of MI in only a few studies. It is unclear if intensive exposure to MI may also result in increased neuroplasticity and improved performance of motor skills through exerting a “priming” effect on the brain. 51 Based on the present findings, there was no evidence for significant improvement in other aspects of body structure and function (psychological factors such as their confidence in activities), or other aspects of activity and participation (transfers and ADL performance) associated with the practice of MI.
Further research may consider reviewing the MI protocol to add components to draw participants’ attention to their task performance as well as investigating the optimal frequency and duration of MI. MI can also be incorporated into a range of existing activities and interventions for PwPD, such as music 52 and dance. 53 Incorporating creative and enjoyable activities could enhance adherence and long-term engagement with MI training. 52 Further research should consider increasing the number of PwPD in the samples, using uniform outcome measures for PwPD, screening the imagery ability of participants and including outcome measures related to body structure and function, and activity and participation. Besides focusing on motor outcomes, further studies can be done on the effects of MI on non-motor outcomes. With more research done in the area, further systematic review can also consider using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach to summarize the evidence for making clinical practice recommendations. 54
Conclusions
MI was shown in individual articles to promote improvements in body structure and function (cognition, dynamic balance, and gait and leg endurance) and activity and participation (functional mobility and quality of life). However, the evidence to support using MI for PwPD has not been established, as the meta-analyses did not show statistically significant results. Practitioners are suggested to refer to the individual study’s specific MI protocol when considering implementing MI for PwPD.
Supplemental Material
sj-docx-1-nnr-10.1177_15459683241246493 – Supplemental material for Effectiveness of Motor Imagery in the Rehabilitation of People With Parkinson’s Disease: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-nnr-10.1177_15459683241246493 for Effectiveness of Motor Imagery in the Rehabilitation of People With Parkinson’s Disease: A Systematic Review and Meta-Analysis by Tabitha Singer, Paul Fahey and Karen P. Y. Liu in Neurorehabilitation and Neural Repair
Supplemental Material
sj-docx-2-nnr-10.1177_15459683241246493 – Supplemental material for Effectiveness of Motor Imagery in the Rehabilitation of People With Parkinson’s Disease: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-nnr-10.1177_15459683241246493 for Effectiveness of Motor Imagery in the Rehabilitation of People With Parkinson’s Disease: A Systematic Review and Meta-Analysis by Tabitha Singer, Paul Fahey and Karen P. Y. Liu in Neurorehabilitation and Neural Repair
Supplemental Material
sj-docx-3-nnr-10.1177_15459683241246493 – Supplemental material for Effectiveness of Motor Imagery in the Rehabilitation of People With Parkinson’s Disease: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-3-nnr-10.1177_15459683241246493 for Effectiveness of Motor Imagery in the Rehabilitation of People With Parkinson’s Disease: A Systematic Review and Meta-Analysis by Tabitha Singer, Paul Fahey and Karen P. Y. Liu in Neurorehabilitation and Neural Repair
Supplemental Material
sj-docx-4-nnr-10.1177_15459683241246493 – Supplemental material for Effectiveness of Motor Imagery in the Rehabilitation of People With Parkinson’s Disease: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-4-nnr-10.1177_15459683241246493 for Effectiveness of Motor Imagery in the Rehabilitation of People With Parkinson’s Disease: A Systematic Review and Meta-Analysis by Tabitha Singer, Paul Fahey and Karen P. Y. Liu in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
The authors acknowledge Lily Collison, Librarian, Western Sydney University, for her assistance in developing the search strategy.
Author Contributions
Tabitha Singer: Data curation; Formal analysis; Investigation; Methodology; Writing—original draft; Writing—review & editing. Paul Fahey: Data curation; Formal analysis; Methodology; Supervision; Writing—review & editing. Karen P. Y. Liu: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Supervision; Writing—original draft; Writing—review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.