
Abstract
Background
Mobility and cognitive impairments are often associated with increased fall risk among people with multiple sclerosis (PwMS). However, evidence on the concurrent assessment of gait or balance and cognitive tasks (dual-task) to predict falls appears to be inconsistent.
Objective
To summarize the ability of gait or balance dual-task testing to predict future falls among PwMS.
Methods
Seven databases including PubMed, Embase, Web of Science, Scopus, CINHAL, SPORTDiscuss, and PsycINFO were searched from inception to May 2022. Two independent reviewers identified studies that performed a dual-task testing among adults with multiple sclerosis and monitored falls prospectively for at least 3 months. Both reviewers also evaluated the quality assessment of the included studies.
Results
Eight studies with 484 participants were included in the review. Most studies (75%) indicated that dual-task testing and dual-task cost did not discriminate prospective fallers (⩾1 fall) and non-fallers (0 fall) and were not found as predictors of future falls. However, dual-task cost of walking velocity (OR = 1.23, 95% CI 0.98-4.45, P = .05) and dual-task of correct response rate of serial 7 subtraction (OR = 1.34, 95% CI 1.04-3.74, P = .02) were significantly associated with increased risk of recurrent falls (≥2 falls). Pattern of cognitive-motor interference was also associated with an increased risk of falling. All studies presented with strong quality.
Conclusion
The scarce evidence indicates that dual-task testing is not able to predict future falls among PwMS. Further research with more complex motor and cognitive tasks and longer-term fall monitoring is required before dual-task testing can be recommended as a predictor of future falls in this population.
Introduction
Approximately 60% of ambulatory and 75% of non-ambulatory people with multiple sclerosis (PwMS) experience at least 1 fall in a period of 6 to 12 months.1,2 Falls may lead to physical injuries (eg, lacerations and fractures),3,4 psychological concerns (eg, fear of falling), 5 hospitalizations, 6 and in the worst cases death. 7 Therefore, the clinical utility and importance of fall risk screening among PwMS are well recognized among researchers and clinicians working in the field. While recent studies have focused on fall risk predictors in this population,8,9 clinical recommendations of the appropriate fall risk screening procedures are limited. A broad range of clinical signs and symptoms are associated with elevated fall risk among PwMS.8 -10 Among them, mobility and cognitive impairments are frequently reported.11,12 Therefore, it seems logical that the impairments associated with the interaction between mobility and cognition (motor-cognitive dual-task) may lead to a more accurate detection of fall risk among PwMS. 13
Dual-task testing of gait and balance is a common procedure used in neurorehabilitation to estimate the ability to perform multiple tasks simultaneously. 14 Dual-tasks often occur in daily life (eg, walking while talking) but their execution is more demanding for clinical populations such as PwMS. 15 Although studies have reported similar dual-task cost between PwMS and healthy adults,16,17 the impact is greater among PwMS which may affect their daily living activities. 18 Indeed, evidence indicates that dual-task walking is affected among PwMS due to the result of a divided attention deficit.13,19 Other factors including muscle fatigue, poor coordination, and spasticity resulting from the variability in lesion load and gray matter atrophy, have also been highlighted as contributors to dual-task deficits among PwMS.15,20,21 Dual-task cost refers to the decline in performance (eg, reduced walking speed) under dual-task condition (eg, walking while talking) relative to single-task condition (eg, walking only). 22 Among older adults aged 60 years or more, evidence suggests that those with poor dual-task performance are at increased risk of future falls. 23 However, this association is not clear among PwMS and conflicting findings have been reported. 24 For example, Wajda et al 25 and Etemadi 26 indicated that, among PwMS, dual-task cost of walking is associated with fall risk and prospective falls, respectively. Meanwhile, Tajali et al 27 and Quinn et al 28 reported no association between dual-task cost of walking and prospective falls in the same population. These inconsistent findings hinder the evidence-based practice of dual-task testing focusing on gait or balance and cognitive tasks to predict future falls in multiple sclerosis (MS).
The conflicting findings may be due to the different methodologies of fall tracking utilized in the studies. While Wajda et al 25 used the Physiological Profile Assessment (PPA) to estimate fall risk, other studies utilized retrospective or prospective fall status in their analyses.27,29 Also, the reviews by Rooney et al 24 and Postigo-Alonso et al 30 highlighting inconsistent associations between dual-task and falls included studies that evaluated falls prospectively and retrospectively. However, it is well-known that retrospective fall reporting is subject to recall bias and has been shown to be inaccurate to determine fall status of PwMS. 31 Therefore, a summary of the findings from studies that have utilized prospective fall monitoring as suggested by the International MS Research Network might provide a better insight into the associations between dual-task testing and falls among PwMS. 32 This summary will also help guide clinicians in their decision-making of using dual-task testing to predict falls in MS.
Additionally, the recognition of the role of mobility and cognition in fall risk, the growing interest in dual-task testing among clinicians and researchers, and the lack of evidence-based recommendations for clinical practice, warrant a systematic review on dual-task testing to predict falls among PwMS. Therefore, the purpose of this review was to summarize the evidence on the ability of dual-task testing of gait and balance to predict future falls among PwMS. This review specifically examined: (1) the ability of dual-task testing of gait and balance to discriminate between fallers and non-fallers and (2) the clinical utility of dual-task testing of gait and balance (sensitivity, specificity, odds ratio) to predict future falls.
Methods
This systematic review was conducted according to the Cochrane Handbook 33 and the reporting of the study followed the instructions suggested by the 2020 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guideline. 34 The review protocol was prospectively registered on PROSPERO, the International Prospective Register of Systematic Reviews (Registration number: CRD 42022302910).
Data Sources and Search Strategy
A comprehensive systematic search was conducted on the following databases from inception to May 2022: MEDLINE via PubMed, Embase, Web of Science, Scopus, CINHAL, SPORTDiscuss, and PsycINFO. A combination of MeSH terms, Emtree terms, keywords, and their synonyms was used to develop a search strategy that was adjusted for the various databases. The search strategy included terms such as (“dual-task” OR “motor-cognitive” OR “psychomotor performance”[MeSH] OR “divided attention”) AND (“Accidental Falls”[MeSH] OR fall) AND (“Multiple Sclerosis”[MeSH] OR MS). The full search strategy for each database is provided in Supplemental Appendix A.
Two reviewers (LA) and (JP) independently conducted the searches and screened all titles and abstracts for study eligibility. Both reviewers compiled a list of potentially eligible studies. Next, full texts of the potential eligible articles were obtained and independently screened according to the eligibility criteria of the review. Disagreements were discussed between the 2 reviewers until a consensus on the final studies included in the review was reached. A manual search of articles that cited the articles included in this review was performed to further identify potential articles of interest (forward search). A manual search in the reference lists of included articles was also performed to further identify potential articles of interest (backward search).
Selection Criteria
Studies that met the following eligibility criteria were included in the review. Inclusion criteria were developed based on Population, Intervention or Exposure, Comparators, Outcomes, and Study designs (PICOS) framework. Studies including (1) Participants: adults (>18 years) with a diagnosis of MS; (2) Exposure: cognitive-motor dual-task assessment focusing on the concurrent assessment of cognitive tasks and gait or balance as motor tasks (eg, concurrent assessment of a walking test using the 10 MWT and a subtraction test); (3) Comparators: single-task (motor or cognitive) or no task; (4) Outcomes: future falls measured prospectively for at least 3 months and included the analysis of fallers (at least 1 fall) or recurrent fallers (≥2 falls) 32 ; and (5) Study design: only prospective cohort studies were included. Studies that included similar definition of falls as follow were included: “an unexpected event in which you come to rest on the ground, floor, or lower level.” 35 Studies that examined retrospective falls, used the PPA as fall risk, or conducted an intervention during a prospective falls tracking that might affect participant’s falls status were excluded.
Data Extraction and Data Synthesis
Data extraction was carried out by one reviewer (JP) and checked by another (LA). The following data were extracted from the included studies: authors, year of publication, and country where study was conducted, setting, sample characteristics (number of participants, % female, age, EDSS-Expanded Disability Status Scale, disease duration, and fall history), methods of fall tracking, duration of fall tracking, and fall outcomes and rate. In addition, motor tasks, cognitive tasks, testing procedures, test outcome of interest, and a summary of dual-task association with falls were also extracted from the included studies. The summary included difference (P-values) between fallers (at least 1 fall) or recurrent fallers (≥2 falls) and non-fallers and evidence of clinical utility of dual-task or dual-task cost to predict falls (sensitivity, specificity, and/or odds ratio).
Data were summarized and presented qualitatively. A meta-analysis was not conducted because of the heterogeneity of the data among the included studies (eg, different measures of dual-task). Mann–Whitney U tests or independent samples t-tests were carried out to examine differences between fallers and non-fallers when median and IQR or mean and SD, respectively, were reported in the studies without further comparison. The analyses were performed using SPSS Version 25.0, SPSS Inc. Chicago, IL. Significant difference was set at P < .05.
Studies Quality Assessment
Methodological quality assessment of the included studies was performed independently by 2 review authors (LA) and (JP) using the Standard Quality Assessment Criteria for quantitative studies. 36 Any discrepancies between the assessments were discussed among both authors until consensus was reached. The Standard Quality Assessment Criteria for quantitative studies is a 14 items checklist that captures the range of methodologies and risk of bias. The 14 items of the checklist can be answered with 4 options: Yes (2 points), Partial (1 point), 0 (0 point), and N/A (does not count toward the final score). The final score is calculated as follows: Final score = Total sum/Possible sum where Total sum = (number of “Yes” × 2) + (number of “Partial” × 1) and Possible sum = 28 – (number of “N/A” × 2). Higher final scores indicate higher methodological quality. 36 Studies with total scores <0.7 were considered to have low quality, between 0.7 and 0.79 were considered to have good quality, and ≥0.8 were considered to have strong quality. 37
Results
Study Selection
The literature search yielded a total of 5639 articles. After removing duplicates, 3230 articles were screened based on titles and abstracts. The full screening led to a final list of 8 articles that were included in the review. Three studies used data from the same study sample; therefore, the search yielded studies from 6 independent samples. Forward and backward searches yielded no additional studies that could be included in this review. The flow diagram of the study selection is presented in Figure 1.
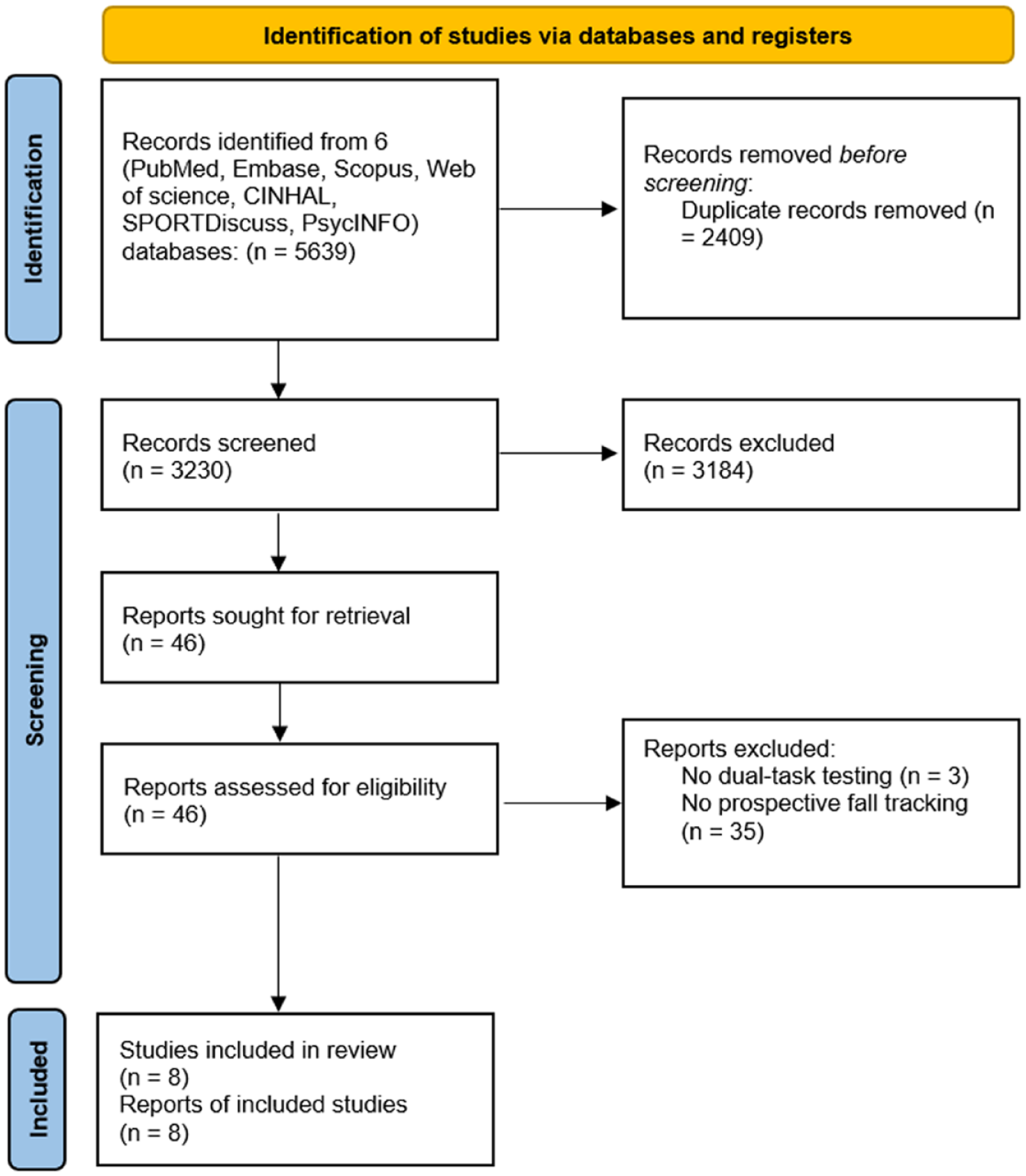
PRISMA flow chart.
Characteristics of Included Studies
Table 1 depicts the characteristics of the included studies. In total 484 individuals with MS participated in the included studies. The mean age of participants varied from 30.3 to 59.0 years. Most participants were female with the percentage of female varying from 50% to 85%. Participants’ EDSS varied from 3.0 to 6.5 indicating no impairment in walking to requirement of bilateral support to walk about 20 m without resting. 38 Participants’ mean disease duration varied from 3.78 to 14 years. Two studies did not report participants’ disease duration.39,40 Prospective fall tracking in the included studies varied from 3 to 6 months. All included studies used validated methods for fall tracking (monthly fall diaries without or with reminder phone call). Fall definition was similar across included studies. Most studies classified participants based on fall status as fallers (1 or more falls) and non-fallers (0 fall). One study classified participants as non-fallers (0-1 fall) and recurrent fallers (≥2 falls). 26
Summary of Included Study Details and Fall Outcome.
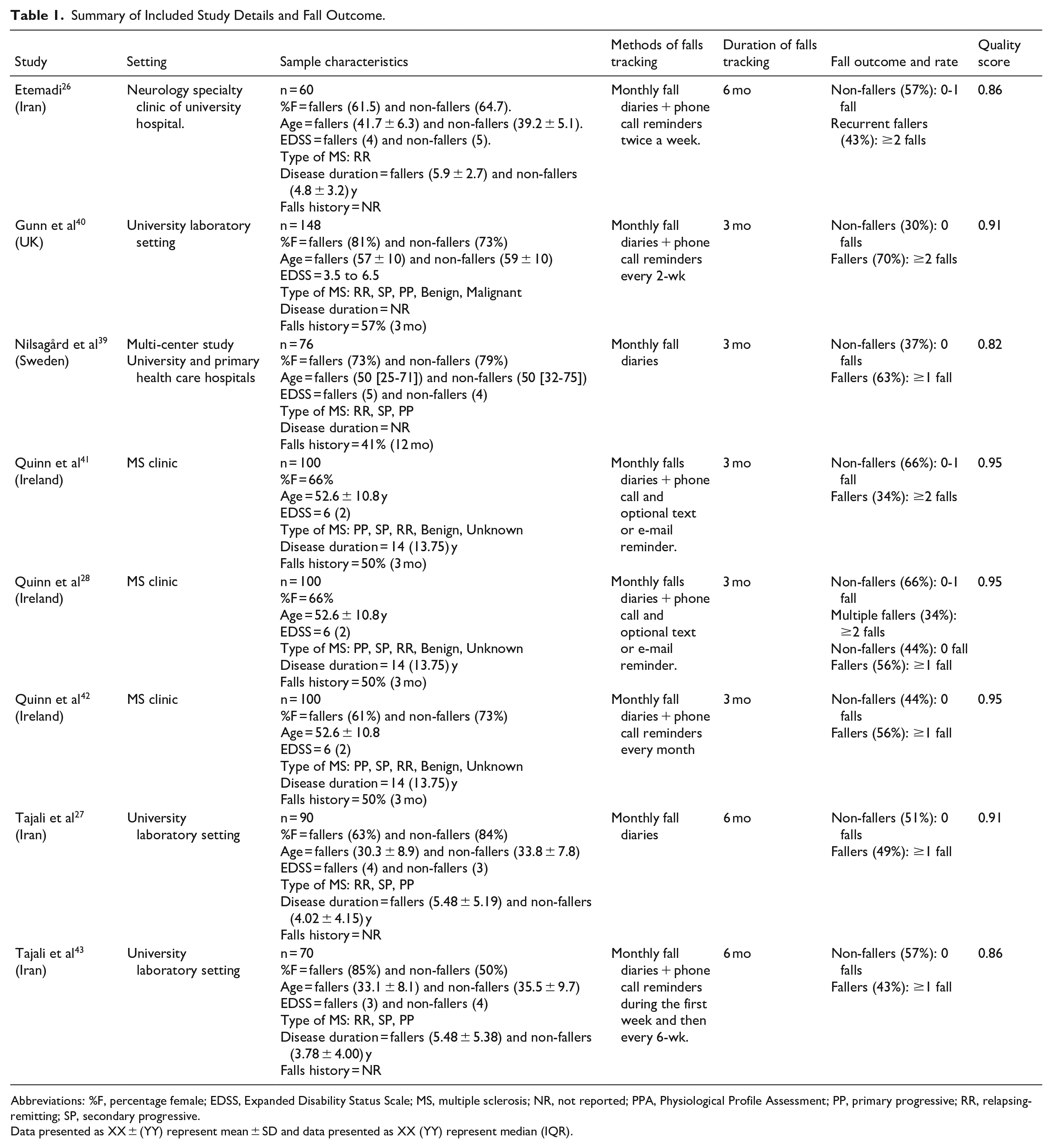
Abbreviations: %F, percentage female; EDSS, Expanded Disability Status Scale; MS, multiple sclerosis; NR, not reported; PPA, Physiological Profile Assessment; PP, primary progressive; RR, relapsing-remitting; SP, secondary progressive.
Data presented as XX ± (YY) represent mean ± SD and data presented as XX (YY) represent median (IQR).
Assessment of Motor and Cognitive Tasks and Dual-Task
The most common motor tasks assessed among the studies included Timed Up and Go (TUG) over 3 m28,39,41,42 and the 10 m walking test (10MWT).26,40 A walking test on a treadmill at a self-selected speed, 43 a 2-minute walking test (2MWT), 27 and the Timed 25-foot walk (T25FW) test 27 were also used as motor tasks to assess gait function. Only 1 study evaluated balance using a force plate as the motor task. 26
Cognitive tasks included activities that involved counting backward in multiples of 3 from a random number,27,44 a number between 20 and 100, 39 a number greater than 50, 42 or a number between 200 and 300. 43 Cognitive activities also involved counting backward in multiples of 7 from a random number.26,40 Details of motor and cognitive assessments are presented in Table 2.
Summary of Dual-Task Testing Protocols, Outcomes of Interest, and Association With Future Falls Among Studies Included.
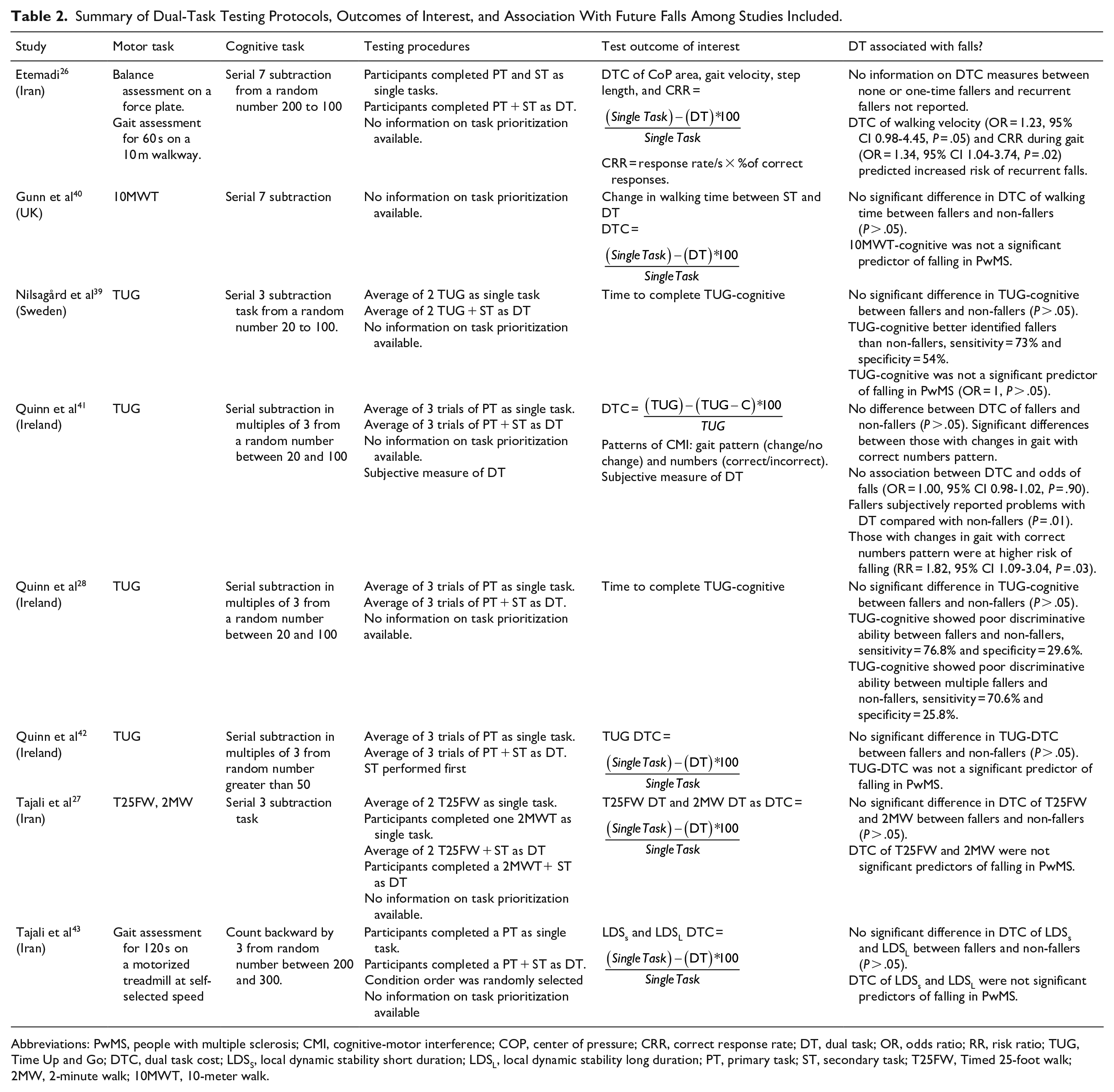
Abbreviations: PwMS, people with multiple sclerosis; CMI, cognitive-motor interference; COP, center of pressure; CRR, correct response rate; DT, dual task; OR, odds ratio; RR, risk ratio; TUG, Time Up and Go; DTC, dual task cost; LDSS, local dynamic stability short duration; LDSL, local dynamic stability long duration; PT, primary task; ST, secondary task; T25FW, Timed 25-foot walk; 2MW, 2-minute walk; 10MWT, 10-meter walk.
The procedures for evaluating the concurrent effect of motor and cognitive tasks varied across the included studies. Time to complete the TUG-cognitive test in seconds was used in 2 studies as test outcome to evaluate future fall risk.28,39 Dual-task cost was the test outcome reported in most studies. Patterns of cognitive-motor interference as well as a subjective measure of difficulty with dual-task were also used in 1 study. 41 Dual-task cost of TUG, CoP area, gait velocity, walking time, step length, correct response rate, dynamic stability were all used in the included studies. All studies but one 40 completed the motor task as a single task activity before assessing the simultaneous performance of both tasks (motor and cognitive). None of the studies provided information on task prioritization during the dual-task testing protocol and therefore, primary and secondary tasks could not be determined.
Association Between Dual-Task Testing and Future Falls
Six out of the 8 included studies (75%) reported no difference between dual-task and dual-task cost performance of fallers and non-fallers.27,28,39 -43 Quinn et al 41 reported significant difference between fallers and non-fallers among individuals using a specific pattern of cognitive-motor impairment (changes in gait with correct numbering). The remaining study by Etemadi 26 that evaluated dual-task cost measures between none or one-time fallers and recurrent fallers (≥2 falls) did not provide information on this comparison and data were not available to estimate the difference. Also, 6 out of the 8 included studies (75%) reported no ability of dual-task and dual-task cost to predict future falls among adults with MS.27,28,39,40,42,43 However, Quinn et al, 41 indicated that a specific pattern of cognitive-motor interference (changes in gait with correct numbering) is associated with higher risk of falling (RR = 1.82, 95% CI 1.09-3.04, P = .03). Also, Etemadi 26 reported that dual-task cost of walking velocity (P = .05, OR = 1.23, 95% CI 0.98-4.45) and dual-task cost of correct response rate (P = .02, OR = 1.34, 95% CI 1.04-3.74) as significant predictors for increased risk of recurrent falls among adults with MS. However, the study failed to reveal an association between dual-task cost of balance (CoP area) and future falls in adults with MS. 26
Quality Assessment of the Included Studies
The quality assessment of included studies is summarized in Table 1. Detailed scores of each item are presented in Supplemental Appendix B. Overall, all included studies were considered to have strong quality (>0.8). Total scores for the quality assessment varied from 0.82 to 0.95 (mean = 0.90). All studies scored lower on the “sample size appropriate?” item because appropriate sample sizes were not estimated. The inter-rater agreement between both reviewers of the methodological quality assessment was 92%. Studies where the reviewers disagreed were re-read and discussed until a consensus was reached.
Discussion
This review demonstrated limited evidence of the association between gait or balance dual-task testing and future falls among adults with MS. Only 8 studies (6 with independent data) were identified in the literature on this topic. The scarce evidence indicated that dual-task testing and dual-task cost of gait and balance are not able to differentiate between adult fallers and non-fallers living with MS. In addition, the findings indicated that dual-task testing and dual-task cost do not predict future falls of adults with MS who fall at least once in a period of 3 to 6 months. Nevertheless, a study by Etemadi 26 demonstrated that the dual-task cost of walking velocity and dual-task cost of correct response rate of a cognitive test (serial subtraction of 7) predicted those who will experience multiple falls (≥2 falls) in the next 6 months. Also, patterns of cognitive-motor interference may be associated with future falls in MS. Despite the significant contributions of mobility and cognitive impairments (as independent factors) on falls among adults with MS, current evidence suggests that additional investigations are required before the motor-cognitive dual-task testing can be recommended for use as a clinical tool for predicting future fall risk. Further prospective studies with longer follow up times are needed to test the ability of gait or balance dual-task assessment to predict future falls in MS.
The lack of associations between dual-task and future falls in this population is somewhat surprising because mobility and cognitive impairments have been independently identified as strong predictors of future falls in this population.11,12 Evidence indicates that the concurrent assessment of motor and cognitive tasks among PwMS increases the difficulty of the execution and leads to a decrease in the performance of the primary task (eg, gait). 17 Therefore, individuals with poor gait performance during a dual-task activity may be at high risk of falls. Rooney et al 24 also presented similar results regarding the uncertainty of an association between dual-task and clinical features including falls among PwMS. Our findings are however different from the results of fall research among community dwelling older adults (≥60 years) where authors have argued through a systematic review that dual-task testing was found as a strong predictor of future falls. 23 The discrepancy observed between the findings in older adults and adults with MS may be due to methodological differences between the studies included in the reviews. In the review by Muir-Hunter and Wittwer 23 among older adults, most included studies conducted prospective falls monitoring for at least 12 months after the dual-task testing while the studies included in our review monitored those falls for only 3 to 6 months. A short duration of fall tracking may be insufficient to fully capture fall status of study participants. Research indicates that significant differences exist between fall-related outcomes after a short-term and longer-term fall follow-up. 45 In addition, a longer-term follow-up whenever possible has been suggested for fall prevention studies by the International MS Falls Prevention Research Network. 32 Therefore, future studies may benefit from including a longer prospective fall tracking (eg, ≥12 months) after dual-task testing to better identify fall status within PwMS.
The absence of associations between dual-task testing and future falls may also be associated with the classification of fall status used as an outcome in the included studies, fallers (≥1 fall) versus non-fallers (0 fall) and recurrent fallers (≥2 falls) versus infrequent fallers (0-1 fall). Recurrent falls have been more attributed to intrinsic factors of falls (eg, disease-specific impairments such as loss of balance, spasticity, cognitive motor interaction, or fatigue) compared with isolated falls. 46 In fact, only 1 study included in our review examined recurrent falls and indicated significant association between the dual-task cost of walking velocity and future falls status. 26 This association needs to be further examined. Examining recurrent falls in future studies may be more important and clinically useful for identifying individuals at high risk of future falls.
The nature of the motor tasks assessed in the studies included in this review may also influence the findings. All the studies analyzed a series of forward walking tests as motor tasks and most tests such as 10 MWT and TUG were shorter than the 60 second walking test used by Etemadi. 26 These motor tasks may not be complex or long enough to elicit motor-cognitive impairments during a dual-task testing. Indeed, none of the studies included in this review compared the dual-task performance of their samples at baseline with reference values (cut-off scores) to indicate whether motor-cognitive impairments were present. Evidence suggests that motor-cognitive interference is affected by the difficulty of the dual-task. 17 Additionally, motor tasks such as walking on a treadmill, obstacle crossing, or backward walking may be more challenging than a simple forward walking. Walking on a treadmill combined with a cognitive task might be more challenging to elicit motor-cognitive impairments. Malcay et al 47 reported that modification of normal walking pattern existed when PwMS walked at a fixed speed on treadmill while performing a cognitive task. However, Tajali et al 43 indicated that dual-task treadmill walking was not associated with future falls in MS. As only 1 study examined the ability of dual-task treadmill walking to predict future falls in MS, 43 more studies are needed to compare this approach with over-ground walking. Furthermore, dual-task obstacle crossing is ecologically valid and has been associated with fall risk in PwMS. 48 Also, dual-task backward walking was more sensitive than dual-task forward walking in detecting fallers with MS. 29 In this later study, fall was measured retrospectively at 6 months, highlighting the potential of including dual-task backward walking in fall risk assessments. 29 Still, it must be noted that backward walking is rarely completed in the real-world and may not be ecologically valid. Therefore, more studies analyzing the associations between dual-task backward walking and prospective falls are needed to confirm this observed relationship. According to Dibble et al, 31 retrospective falls (as used by Edwards et al 29 in their analysis) may not be an accurate assessment of fall risk in an MS sample. Nonetheless, the potential of obstacle crossing and backward walking to detect adult fallers and non-fallers with MS might be a solution for evaluating fall risk based on dual-task costs.
Similarly, the nature of the cognitive tasks evaluated in the studies included in this review may also influence the findings. A more challenging arithmetic subtraction may be more sensitive to detect dual-task impairment and subsequently falls. Etemadi 26 who reported ability of dual-task cost to detect future falls used an arithmetic subtraction by 7 which is more challenging than the arithmetic subtraction by 3 used in the remaining studies included in this review. Also, a cognitive task that is more challenging than an arithmetic task and ecologically relevant, such as working memory tasks, information processing speed task, verbal fluency, or a task switching test might be more sensitive in detecting impairments. Indeed, Leone et al 16 indicated that during dual-task assessments, a Digit Span backward was the most interfering cognitive task over gait velocity and accuracy when the authors compared 16 different cognitive tasks including arithmetic tasks. Also, tests of processing speed like the Symbol Digit Modalities Test have been recommended for cognitive screening and management in MS care, 49 though its combination with over-ground walking is challenging. By combining a more challenging cognitive task (eg, Digit Span backward) with a more complex motor task (eg, obstacle crossing over 60 second walking test), and monitoring fall prospectively for at least 12 months, future studies may be able to better assess the ability of dual-task methods for predicting future falls. With better insight, clinicians may also gain better tools for screening this population’s fall risk in the clinical setting.
Moreover, given the findings of previous studies indicating that history of previous falls is a strong predictor of future falls8,50 and that self-reported measures are stronger fall risk predictors than performance-based measures, 27 it is important to examine whether dual-task testing provides any added value to clinicians when identifying PwMS who are at risk of future falls. None of the included studies in this review compared the predictive ability of dual-task testing with history of falls, self-reported measure (eg, Activities-specific Balance Confidence scale), or any single-task walking test (eg, TUG). Only Tajali et al 27 indicated that single-tasks of T25FW and 2MWT significantly discriminated between fallers and non-fallers while dual-task costs of the same tasks were not able to discriminate both groups. A direct comparison of the ability of dual-task testing with falls history, self-reported measures, or single-task performance-based measure may provide a better insight on the added value of dual-task testing to clinical practice. Such comparisons will help clinicians to choose the most accurate fall risk tool to identify PwMS at high risk of falls and refer them to fall prevention programs.
Limitations
There are limitations associated with this review. First, the literature search yielded only 8 studies with 6 independent datasets. We limited our search to only studies that evaluated prospective future falls to provide a true state of the art of the current evidence of dual-task testing to predict future falls. Retrospective falls have been shown to be inaccurate 31 and were therefore excluded from our analysis. Therefore, the number of studies on dual-task testing and prospective falls among PwMS is much smaller when compared to other populations (eg, older adults) limiting our ability to provide firm conclusions. In addition, the included studies were mostly conducted by the same research groups in selected countries (Ireland, Iran, Sweden, and UK). This indicates that more diversity and possible multicenter research are needed in this field of study. Also, all studies included in this review evaluated individuals with EDSS between 3 and 6.5 who are ambulatory, and no study was found evaluating dual-task testing among non-ambulatory individuals who use a wheelchair for their daily mobility. Furthermore, all studies but one 26 included all subtypes of MS (relapsing-remitting, primary progressive, and secondary progressive) in their analyses. The inclusion of PwMS with relapsing and progressive in the same analysis may also justify the lack of associations between dual-task testing and prospective falls. Future studies should analyze people with relapsing and progressive MS separately to achieve more sensitive and accurate results. Lastly, we were unable to provide any clinical recommendations on the use of dual-task testing focusing on gait or balance and cognitive tasks to predict future falls based on the current findings, however, the lack of association observed in the included studies is informative for future studies.
Conclusion
Evidence on the association between gait or balance dual-task testing and future falls among PwMS is still scarce. Our findings highlight no association between gait or balance dual-task testing and future falls when comparing fallers (at least 1 fall) and non-fallers (0 fall) between 3 and 6 months. The analysis of individuals who fall recurrently (≥2 falls) over a period of at least 6 months might provide better insight on the true fall status of this population. Gait or balance dual-task testing requires further research before it can be recommended as predictor of future falls among adults with MS in clinical settings.
Supplemental Material
sj-docx-1-nnr-10.1177_15459683221131791 – Supplemental material for Motor Cognitive Dual-Task Testing to Predict Future Falls in Multiple Sclerosis: A Systematic Review
Supplemental material, sj-docx-1-nnr-10.1177_15459683221131791 for Motor Cognitive Dual-Task Testing to Predict Future Falls in Multiple Sclerosis: A Systematic Review by Libak Abou, Joseph Peters, Nora E. Fritz, Jacob J. Sosnoff and Anna L. Kratz in Neurorehabilitation and Neural Repair
Supplemental Material
sj-docx-2-nnr-10.1177_15459683221131791 – Supplemental material for Motor Cognitive Dual-Task Testing to Predict Future Falls in Multiple Sclerosis: A Systematic Review
Supplemental material, sj-docx-2-nnr-10.1177_15459683221131791 for Motor Cognitive Dual-Task Testing to Predict Future Falls in Multiple Sclerosis: A Systematic Review by Libak Abou, Joseph Peters, Nora E. Fritz, Jacob J. Sosnoff and Anna L. Kratz in Neurorehabilitation and Neural Repair
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Mentor-Based Postdoctoral Fellowship Program in Rehabilitation Research (MB-1706-27943; PI: Kratz) from the National Multiple Sclerosis Society.
Ethical Approval
Not required.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.