
Abstract
Background. Multiple sclerosis (MS) can be accompanied by motor, cognitive, and sensory impairments. Additionally, MS patients often report fatigue as one of their most debilitating symptoms. It is, therefore, expected that MS patients will have difficulties in performing cognitive-motor dual tasks (DTs), especially in a fatiguing condition. Objective. To determine whether MS patients are more challenged by a DT than controls in a fatiguing and less-fatiguing condition and whether DT performance is associated with perceived fatigue. Methods. A group of 19 MS patients and 19 age-, sex-, and education-matched controls performed a cognitive task (2-choice reaction time task) separately or concurrent with a low-force or a high-force motor task (index finger abduction at 10% or 30% maximal voluntary contraction). Results. MS patients performed less well on a cognitive task than controls. Cognitive task performance under DT conditions decreased more for MS patients. Moreover, under high-force DT conditions, cognitive performance declined in both groups but to a larger degree for MS patients. Besides a decline in cognitive task performance, MS patients also showed a stronger decrease in motor performance under high-force DT conditions. DT costs were positively related to perceived fatigue as measured by questionnaires. Conclusions. Compared with controls, MS patients performed less well on DTs as demonstrated by a reduction in both cognitive and motor performances. This performance decrease was stronger under fatiguing conditions and was related to the sense of fatigue of MS patients. These data illustrate problems that MS patients may encounter in daily life because of their fatigue.
Introduction
Multiple sclerosis (MS) patients report both motor and cognitive complaints (for a review see Compston and Coles 1 ). The most commonly described cognitive symptoms are those of reduced attention and information processing, which have been shown to be present already at early stages of the disease.2-4 These symptoms may be a result of increased cognitive resources necessary for task performance, as demonstrated by imaging studies in MS patients. These studies show increased cortical activity during the performance of cognitive tasks5-8 as well as during submaximal motor tasks.9-11 If execution of cognitive and motor tasks requires increased cognitive resources, it is expected that the performance of a cognitive task simultaneously with a motor task (cognitive-motor dual task [DT]) would be particularly difficult to master. In a DT paradigm, attention needs to be divided over 2 simultaneously performed tasks, 12 and indeed, MS patients underperformed compared with controls.13-20
We used a cognitive-motor DT to investigate changes in the distribution of attention during development of muscle fatigue in young21,22 and middle-aged 23 participants. In comparison with single task performance, we found decreased cognitive task performance during the DT, with an additional decline in the fatiguing condition. 21 Increasing muscle fatigue, defined as an exercise-induced decline in muscle force,24,25 increases cortical activity (blood oxygenation level detection, BOLD signal) in controls26-28 but not in MS patients. 29 We speculated that this augmented activation in controls reflected increased voluntary activation to compensate for a fatigue-related decline in corticospinal excitability. 30 The lack of this BOLD increase in MS patients was associated with a decline in voluntary activation, 29 suggesting that MS patients indeed had difficulty raising their corticofugal output.
To test whether this decline in cortical activation is confined to motor areas or whether higher-order areas are also affected by muscle fatigue in MS patients, we aimed to repeat the fatiguing cognitive-motor DT experiments in MS patients.21,23 Given that MS patients, besides changes in cognitive, motor, and sensory abilities, 1 almost always report increased levels of perceived fatigue (as quantified by fatigue questionnaires),31,32 it is expected that performing the fatiguing cognitive-motor DT reveals effects of this increased perceived fatigue.
It was the aim of this study to (1) assess the effects of muscle fatigue on the performance of MS patients in a cognitive-motor DT as compared with control participants and (2) explore whether changes in DT performance were associated with perceived fatigue. We expected MS patients to demonstrate decreased cognitive performance when compared with controls even at a single task, which would become more pronounced during the cognitive-motor DT and show an even further decline during the fatiguing DT.
The data collected in controls (17/19) were also used in another study that addressed age effects on cognitive performance in a DT condition. 23
Methods
Participants
In all, 100 patients were screened. We only included those right-handed patients (as assessed by the Edinburgh Handedness Questionnaire 33 ) who were diagnosed with the relapse-remitting form of MS. 34 Additionally, to ensure proper task performance, we only included mildly disabled patients as determined by an experienced neurologist (Expanded Disability Status Scale [EDSS] <5.0 35 ; for information on participants, see Table 1). A total of 52 patients were eligible for participation. Patients were excluded based on the following criteria (some for multiple reasons): having the secondary-progressive form of MS (n = 4), the presence of neurological illnesses other than MS (n = 2), clinical depression (n = 9), other conditions known to influence fatigue (eg, cardiovascular disease, cancer, hypothyroidism; n = 7), and the use of fatigue-modulating medication (amantadine, tricyclic antidepressants, selective serotonin reuptake inhibitors, and muscle relaxants such as baclofen, benzodiazepines, and modafinil; n = 37). MS patients were not included during a relapse or when they had used prednisolone in the preceding 6 weeks.
Patient Characteristics. a
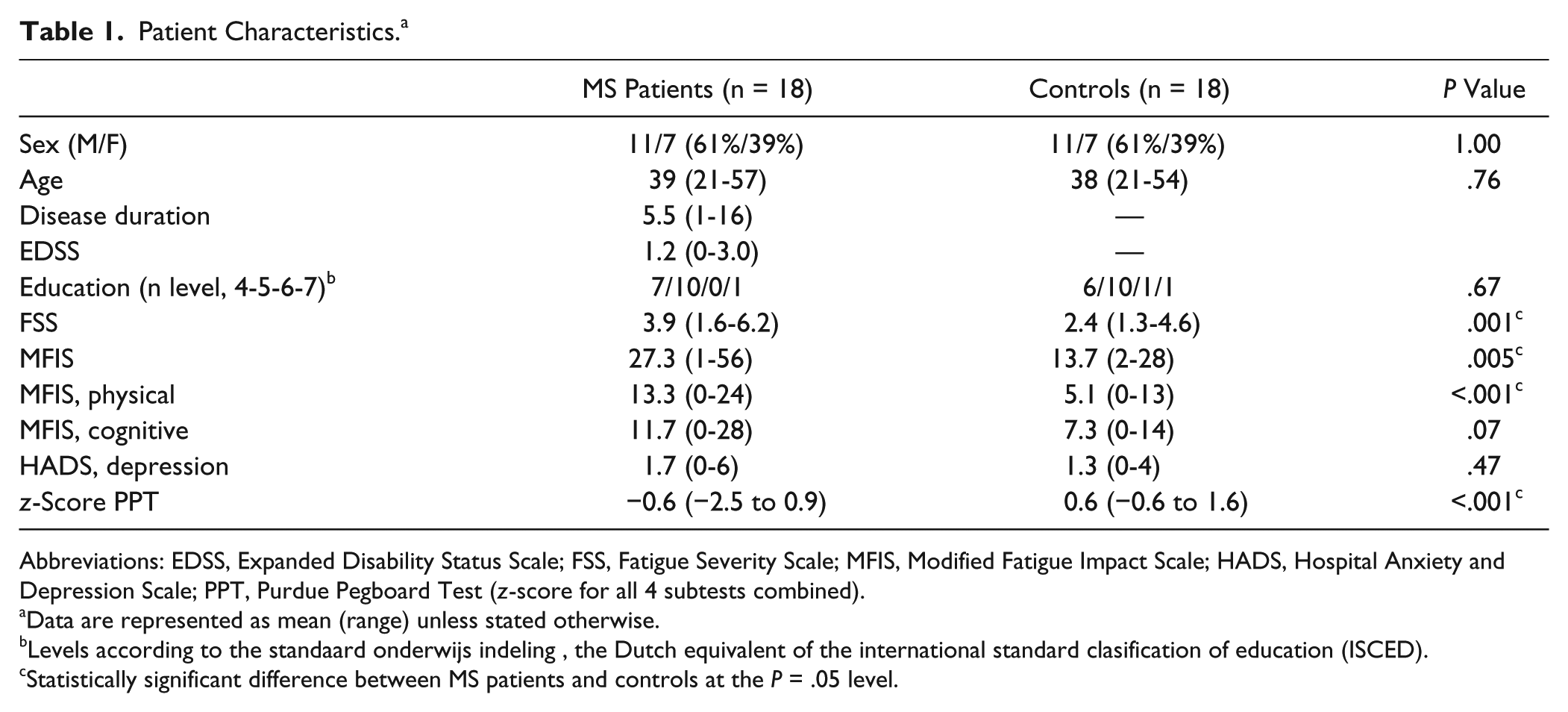
Abbreviations: EDSS, Expanded Disability Status Scale; FSS, Fatigue Severity Scale; MFIS, Modified Fatigue Impact Scale; HADS, Hospital Anxiety and Depression Scale; PPT, Purdue Pegboard Test (z-score for all 4 subtests combined).
Data are represented as mean (range) unless stated otherwise.
Levels according to the standaard onderwijs indeling , the Dutch equivalent of the international standard clasification of education (ISCED).
Statistically significant difference between MS patients and controls at the P = .05 level.
In all, 20 individuals agreed to participate. Common reasons not to do so were time investment and logistics. A total of 19 MS patients (1 patient relapsed after the first measurement and was excluded) and 19 controls, matched on a subject-by-subject basis for sex, age, and education, were included.
All participants were able to survey the visual feedback and auditory stimuli presented in this study without problems. Participants gave their informed consent before participation. The study was approved by the medical ethical committee and was performed to conform to the Declaration of Helsinki.
General Information
At the start of the experiment, participants completed the validated Dutch versions of 2 questionnaires regarding fatigue: the Fatigue Severity Scale (FSS) and the Modified Fatigue Impact Scale (MFIS).36-39 The FSS is a general fatigue questionnaire, whereas the MFIS distinguishes between cognitive and physical fatigue. Furthermore, participants filled out the Hospital Anxiety and Depression Scale (HADS). 40 To determine dexterity, all participants performed the Purdue Pegboard Test (#32020 Lafayette Instruments, Lafayette, IN).
Experimental Setup
The experimental setup and tasks are similar to those described by Lorist et al 21 and Wolkorte et al. 23
Force and Electromyography Recording During the Motor Task
The motor task consisted of isometric right index finger abduction. Participants sat with their arms resting on a table with their right forearm stabilized halfway between pronation and supination. On the right hand, digits 3 to 5 were constrained with a plastic plate, and the thumb was fixed with a Velcro strap. The proximal interphalangeal joint of the index finger was taped to a force transducer (Figure 1). 41 After amplification, the force signal was collected (500 Hz) with a PC equipped with a data-acquisition interface and accompanying software Spike2 v7 (1401 Power, Cambridge Electronic Design, Cambridge, UK).
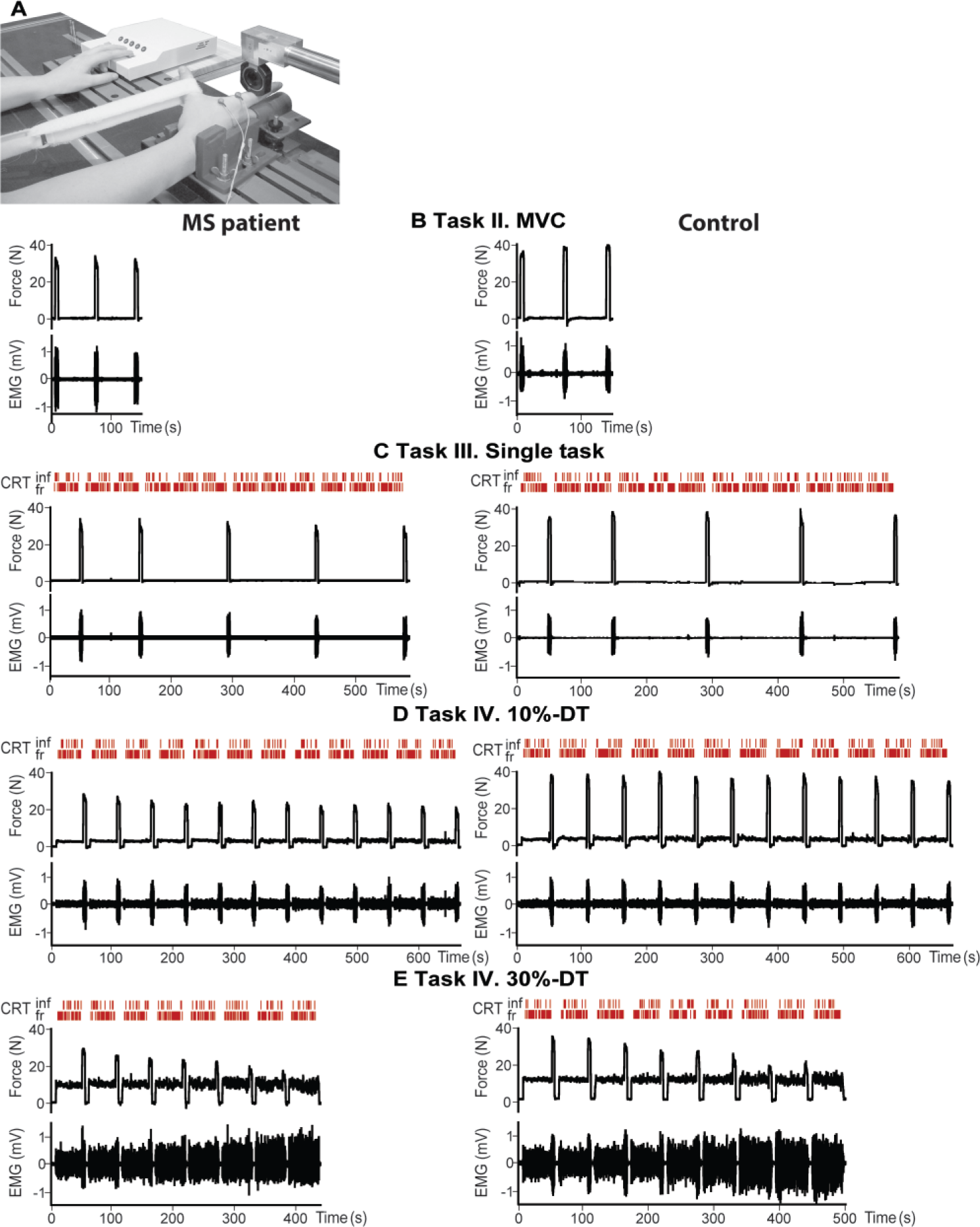
Illustration of the tasks. A. Setup: right index finger is attached to a force transducer, left hand is placed on a serial response box. B-E. Raw data for an MS (left) and control (right) participant, for task II (B), task III (C), and task IV 10% DT (D) and 30% DT (E). Top 2 rows show responses to the frequent and infrequent cognitive stimuli, followed by force and EMG recordings. Task I, the training of the cognitive task, is not shown.
Electromyographic activity (EMG) of the right first dorsal interosseus muscle (FDI) was recorded with sintered Ag/AgCl electrodes taped above the muscle and the first metacarpophalangeal joint. EMG signals were amplified, filtered (8-1000 Hz), and collected (2000 Hz) together with the force data. Participants received force feedback on a computer screen located approximately 1 m in front of them. One line showed the target force and a second line, in different color, the produced force in real time.
Setup of the Cognitive Task
A response box was placed in front of the participants at a comfortable position, so that participants could respond with their left hand while their right index finger was placed in the force setup (Figure 1A). The cognitive task consisted of an auditory choice reaction time task (CRT). E-Prime software presented the stimuli and collected the responses (Psychology Software Tools, Inc, Sharpsburg, PA).
Loudspeakers in front of the participant produced either a low- (500 Hz) or a high- (900 Hz) pitched tone (50 ms) at 70 dBA. The interstimulus interval varied between 1100 and 1300 ms. One tone occurred more frequently (70%) than the other tone (30%). Participants responded to the low- or high-pitched tones by pressing a button on the response box with either their left index or middle finger as quickly and as accurately as possible. The tone that was presented more frequently and the associated response (left index or middle finger) were randomized between participants. Participants were informed that the first stimulus of every block was the frequent stimulus.
Experimental Tasks
Participants came to the lab at the same time of the day for 3 sessions, separated by 1 week. The first session was a practice session to become familiar with the task and to minimize training effects. In the second and third session, either a low-force (10%-DT) or a high-force DT (30%-DT) was performed. Each session (~1 hour) consisted of 4 tasks (Figure 1).
Task I, practice of the cognitive task: Responding to 150 stimuli (task Ia), followed by 3 blocks of 50 stimuli, with 5 s between the blocks (task Ib).
Task II, maximal voluntary contraction (MVC): Assessment of maximal isometric index finger abduction force (~5 s), 3 attempts with 60 s of rest between attempts. The maximal force was taken as the control MVC (cMVC). EMG of the FDI was rectified and maximal EMG was determined for a 100-ms time window around the maximal force.
Task III, single cognitive task: 12 CRT blocks of 33 stimuli (~40 s). After the 1st, 3rd, 6th, 9th, and 12th blocks, participants performed a 5-s MVC to get acquainted with the timing of the DT.
Task IV, DT: Participants produced a force (~44 s) at either 10% (10%-DT) or 30% (30%-DT) cMVC. Then, 4 s into the contraction, the cognitive stimuli started. Again, as in the single task, blocks of 33 stimuli were presented. After the cognitive task, participants performed an MVC (5 s), followed by 5 s of rest. This sequence was repeated for 12 blocks for 10%-DT and until task failure for 30%-DT. Task failure was defined as being unable to maintain force at 30% cMVC for more than 5 s or when the MVC did not exceed 30% cMVC. Participants were instructed to prioritize the motor task over the cognitive task.
Outcome Measures
Descriptive information included scores on the fatigue and the depression questionnaires. the outcomes of the fatigue questionnaires were further used as a measure of perceived fatigue. The main outcome measures of the force task were the following: (1) MVCs obtained during task II; (2) submaximal force (percentage cMVC), EMG (percentage maximal EMG), and force variability (standard deviation [SD]/force) during the submaximal part of the DT; and (3) MVCs during the DT (percentage cMVC).
Cognitive outcome measures consisted of the percentage of incorrect responses and reaction times. The first 2 responses of each block were discarded. Responses faster than 100 ms were counted as incorrect; only reaction times to correct responses were used in the analyses. Furthermore, we calculated variability of reaction times (SD/mean). To minimize the influence of outliers, 20% trimmed means were used for calculating the means and the variability of the reaction times—that is, the 10% highest and 10% lowest scores per participant per task were disregarded.
Statistics
Based on a pilot study, 24 patients were required (power = 0.8; α = .05; effect size = 0.27). To ensure sufficient power for all analyses 40 participants were included. From a previous study, 23 we learned that age had significant effects on reaction times. Therefore, we included age (centered grand mean) as a covariate in all statistical analyses.
Differences in patients and control characteristics were tested with independent t tests. The MVC between groups was tested with a univariate ANOVA with MS and Sex as between-subjects factors; sex was added to correct for force difference between the sexes.
Training Effects
To investigate within-session training effects, repeated measures (RM) ANOVAs were performed with Task (task Ia, task Ib, task III) and Probability (frequent, infrequent) as within-subjects effects and MS as between-subjects effects. To investigate between-session training effects, we used task III of the 3 sessions. RM-ANOVAs were performed with Session (1, 2, and 3) and Probability (frequent and infrequent stimuli) as within-subject factors and MS as the between-subject factor.
Dual-Task Analyses
To compare the two sessions (ie, 10%- and 30%-DT), all data were averaged for the same number of blocks. Thus, if a participant could maintain the 30%-DT for 10 blocks, output measures (reaction times and accuracy) obtained during tasks III and IV were also averaged for 10 blocks. This was not possible for 2 MS patients and 1 control, who maintained 30%-DT for 13, 14, and 17 blocks. For these participants, 12 blocks of the 10%-DT task were used. Analyses were performed for accuracy, reaction times, and variability of reaction times. RM-ANOVAs were performed with Task (single task, DT), Session force (10% or 30%), and Probability (frequent, infrequent) as within-subject factors and MS as a between-subject factor.
To evaluate time-related changes in motor performance, data during 10%- and 30%-DT were averaged over the first and second half of the number of blocks that a participant could maintain during 30%-DT. A RM-ANOVA with Force (10% or 30%) and Time (first and second half) as within-subject factors and MS as a between-subject factor were used for statistical analysis.
Relationship Between Perceived Fatigue and DT Costs
We calculated DT costs—that is, DT minus single task—to investigate the relationship between perceived fatigue as measured with the MFIS questionnaire cognitive subscale and DT costs. Because no interaction effects of MS and Probability were found, data from frequent and infrequent stimuli were pooled. We also included a linear regression model as proposed by Steens et al 42 to associate perceived fatigue (FSS) with the HADS depression score, MVC, and fatigability.
Results
The MS patients reported more fatigue than age- and sex-matched controls (Table 1). Based on the FSS, using a cutoff point of 4.0, 43 9 of 18 MS patients and 1 of 18 controls were fatigued. The EDSS scores (Table 1, median = 0.0) indicated that patients were only mildly affected by MS. Still, MS patients had reduced fine motor skills as shown by their performance on the Purdue Pegboard Test (Table 1).
In one MS patient, we measured reaction times that were more than 3 SDs from the average response. We excluded this patient and the matched control from all our analyses. During the 30%-DT, one MS patient produced less than 30% MVC, and a second MS patient could not maintain 30% MVC for 40 s. We excluded these patients and their matched controls from the DT analyses.
Training Effects
Within the first session, an interaction effect of Task (task Ia, Ib, and CRT) by MS was present for accuracy (F1.3,43.9 = 5.1, P = .021); MS patients reduced their errors from task Ia to task Ib (10.5%, 5.0%, 5.0%), whereas controls did not (3.7%, 3.3%, 3.1%; F1,33 = 5.1; P = .021; Figure 2). Overall, MS patients made more errors than controls (F1,33 = 6.2; P = .018). Reaction times did not show training effects within the session, but overall, MS patients were slower than controls (F1,33 = 20.3; P < .001).
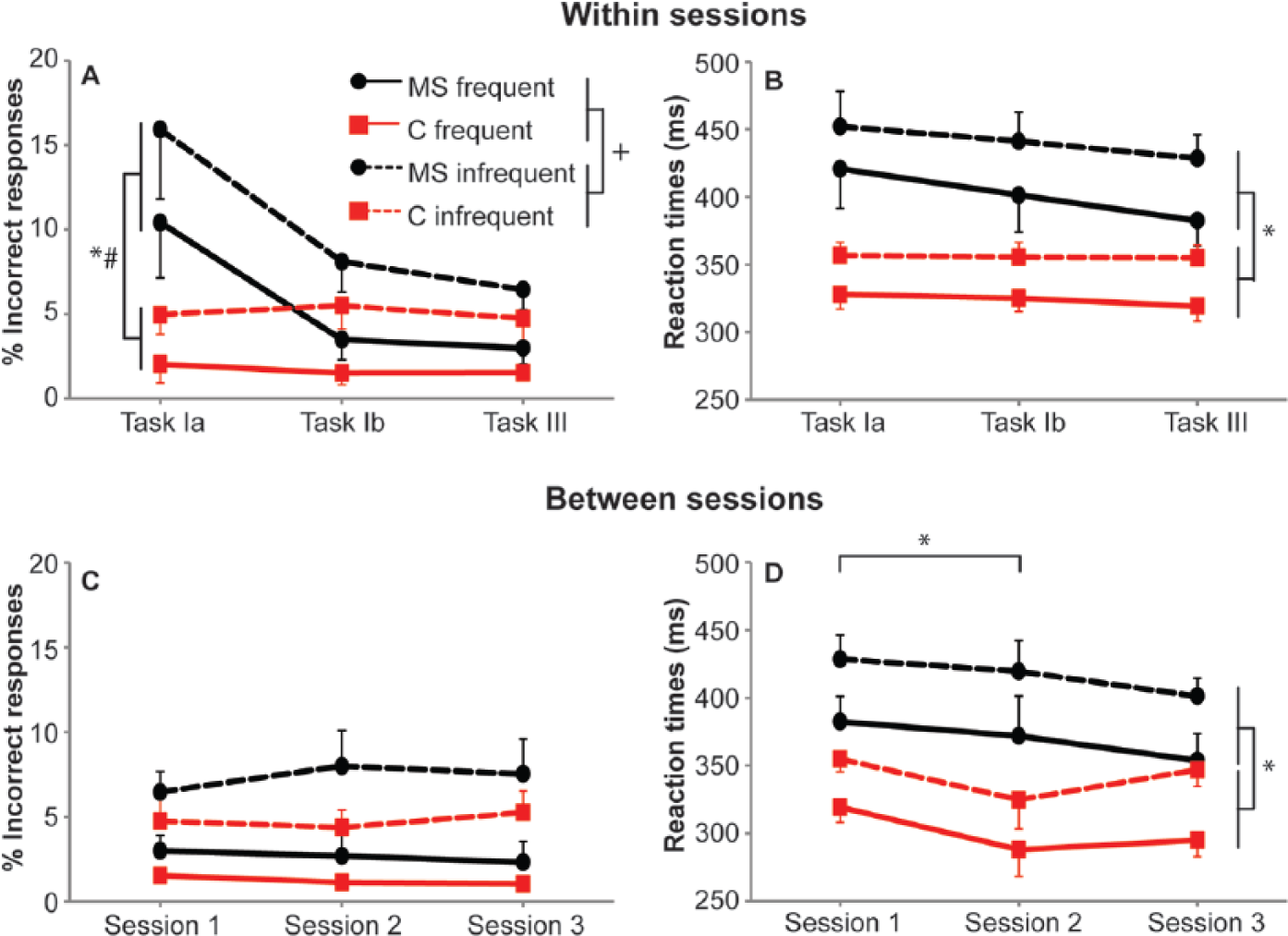
Training effects: Within-session (A, B) and between-session (C, D); training effects for accuracy (left panels) and reaction times (right panels). Task Ia, practice of the cognitive task with 150 stimuli. Task Ib, practice of the cognitive task with 3 × 50 stimuli. Task III, single cognitive task with 6 × 33 stimuli.a
Between sessions, an effect of Session was found for reaction times (373, 350, 343 ms; F2,64 = 11.49, P < .001; Figure 2). Post hoc analysis revealed a significant decrease in reaction times only from session 1 to session 2 (F1,32 = 11.1; P = .002). Overall, MS patients were slower than controls (F1,33 = 19.6; P < .001). Nevertheless, there were no interaction effects with MS; hence, training effects resulting in faster reaction times were similar for both groups (Figure 2). In general, more errors and slower reaction times were recorded on infrequent as opposed to frequent stimuli, but no interaction effects with MS were found.
Motor Data and the Effect of Fatigue on Force During the DT Performance
No difference was found in MVC between sessions (T(31) = 0.86; P = .93) or between patients (40 N, SD = 18) and controls (45 N, SD = 11; F1,28 = 1.18, P = .29). However, one patient was very strong (97 N). If this patient was excluded, controls were stronger than MS patients (36 N, SD = 9; F1,27 = 7.27, P = .012). Men (49 N) were stronger than women (34 N; F1,28 = 10.69, P = .003).
The number of blocks until fatigue did not differ between patients (7.5 blocks, SD = 4.1) and controls (8.0 blocks, SD = 2.4; P = .673). The data showed that participants maintained target force (Table 2, Figure 3D), but intermittent MVCs decreased during 30%-DT (P < .001; Figure 3E). EMG remained stable during 10%-DT but increased during 30%-DT (P < .001; Figure 3G). Interestingly, force variability increased for both groups during 30%-DT, but MS patients showed a greater increase (P = .042; Figure 3F). Patients produced less force during intermittent MVCs of 10%-DT (P < .001; Figure 3E), but not during 30%-DT. This was mostly because 2 MS patients had lower MVCs during 10%-DT.
Motor Data. a
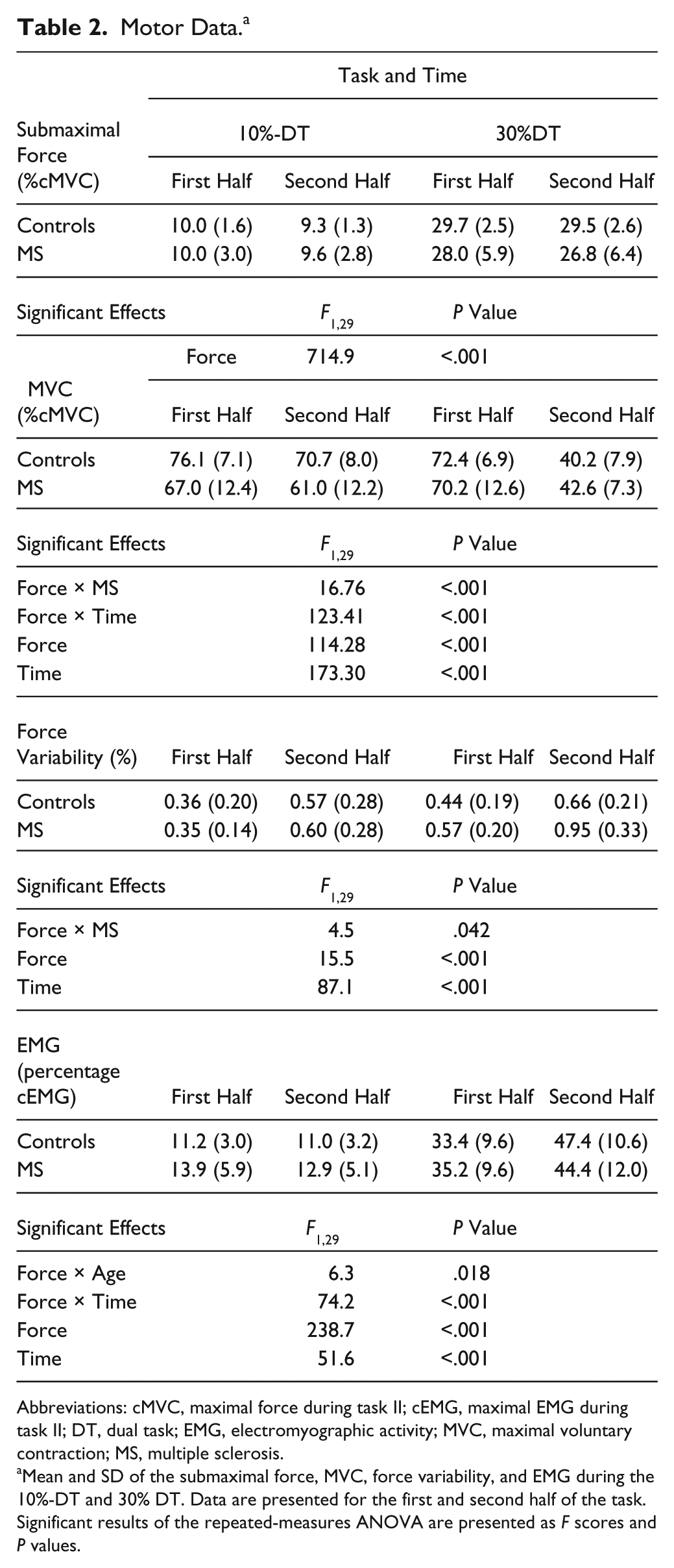
Abbreviations: cMVC, maximal force during task II; cEMG, maximal EMG during task II; DT, dual task; EMG, electromyographic activity; MVC, maximal voluntary contraction; MS, multiple sclerosis.
Mean and SD of the submaximal force, MVC, force variability, and EMG during the 10%-DT and 30% DT. Data are presented for the first and second half of the task. Significant results of the repeated-measures ANOVA are presented as F scores and P values.
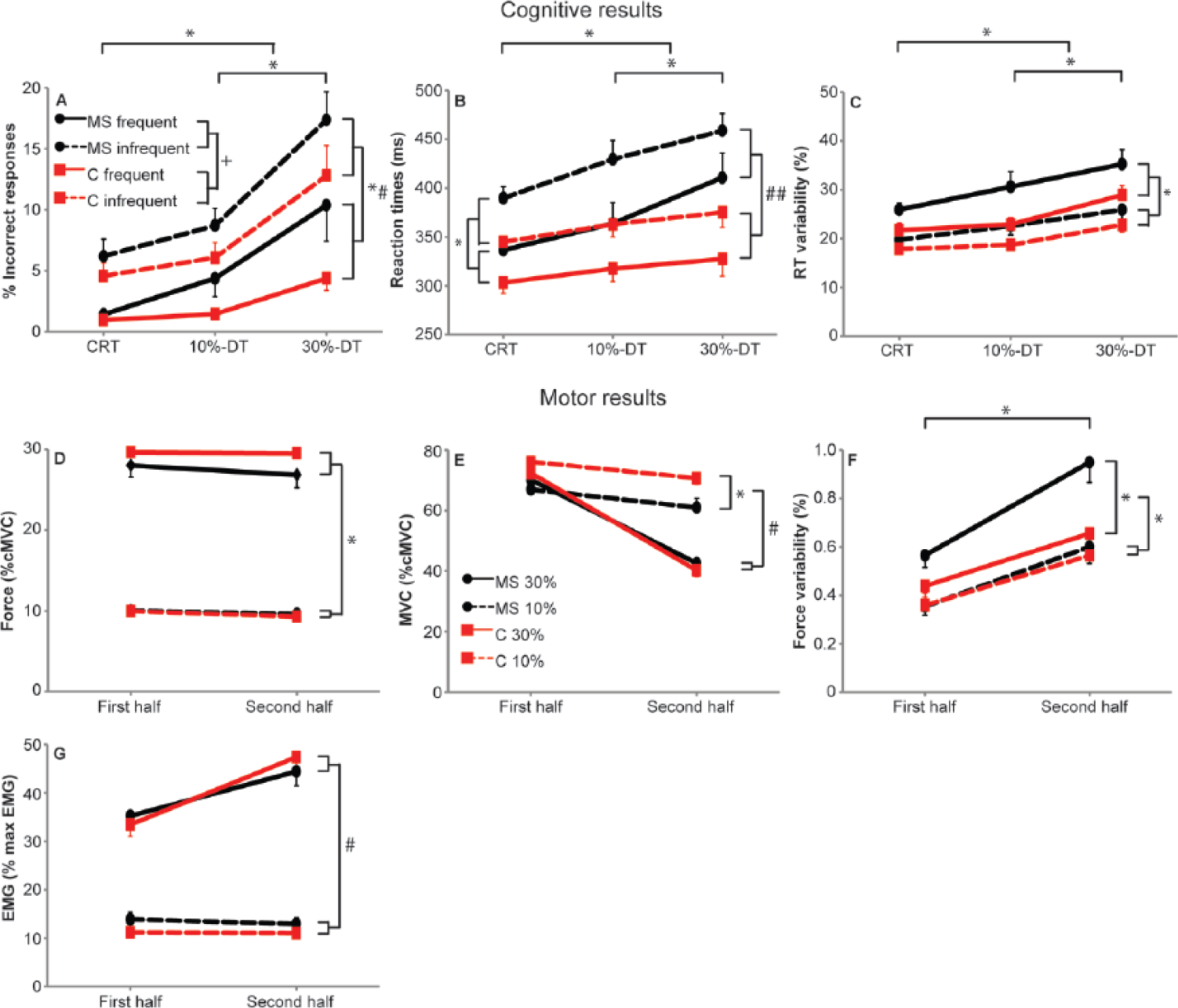
Dual task data. Top panels: cognitive data. Accuracy (A), reaction times (B), and reaction times variability (C) for the single task, 10%-DT, and 30%-DT. Note the decrease in performance with increasing task difficulty and the additional increase in reaction times for MS patients. Lower panels: motor data obtained during the dual task. Submaximal force (D), MVC (E), force variability (F), and EMG (G). Note the increased force variability during 30%-DT in MS patients.a
Effect of Task and Force on Cognitive Performance
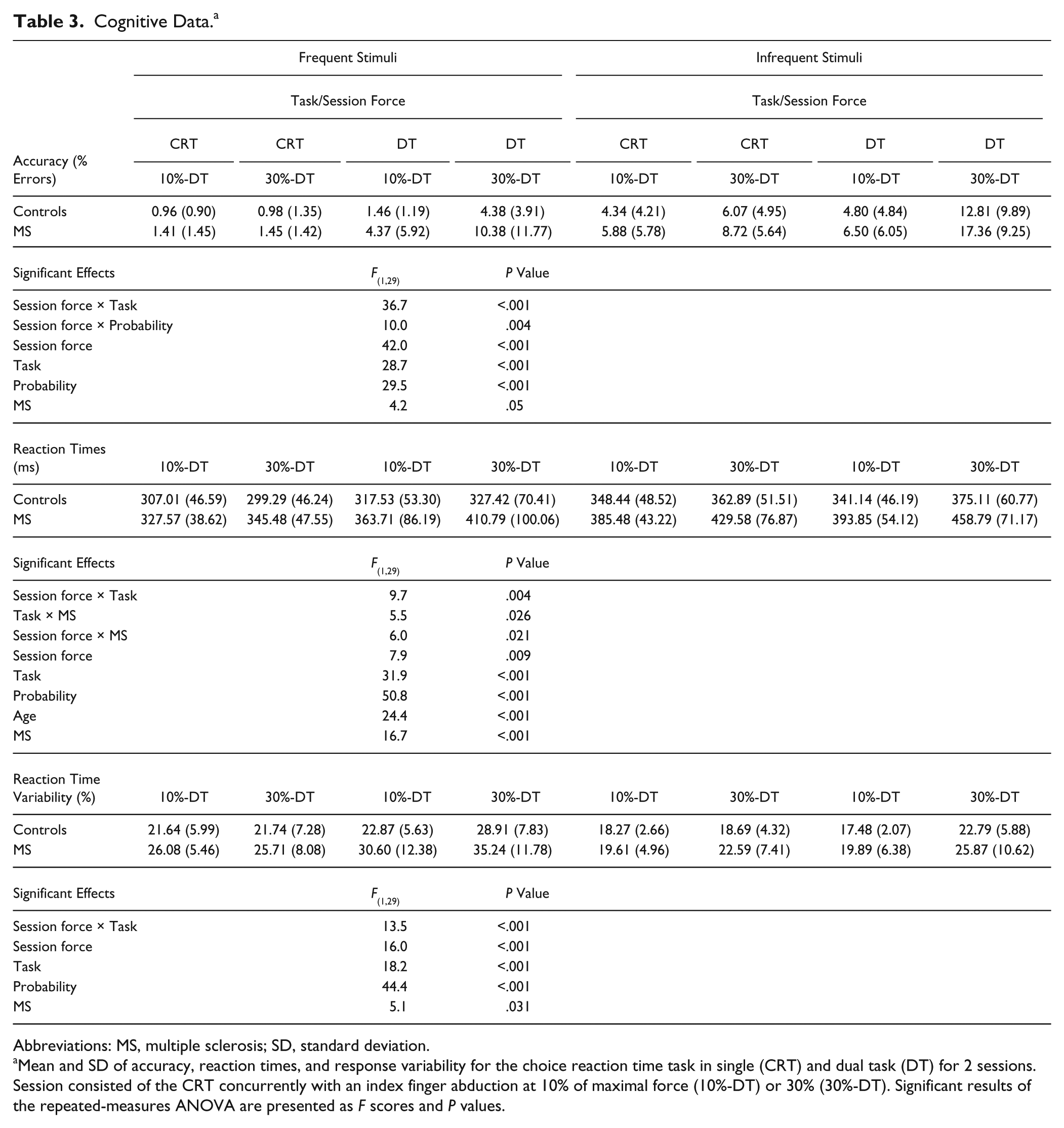
Statistical analysis revealed main effects of Task, Probability, Session force, and MS on accuracy, reaction times, and variability (Table 3, Figure 3). The effect of Task demonstrated longer reaction times (P < .001), more errors (P < .001), and more variability (P < .001) in responses obtained in the dual- versus single-task condition. Furthermore, significant interaction effects were found for Task by Session force, indicating that the increase from a single to a DT in reaction times (P = .004), errors (P < .001), and variability (P < .001) was larger during the more effortful 30%-DT (Table 3, Figure 3).
Cognitive Data. a
Abbreviations: MS, multiple sclerosis; SD, standard deviation.
Mean and SD of accuracy, reaction times, and response variability for the choice reaction time task in single (CRT) and dual task (DT) for 2 sessions. Session consisted of the CRT concurrently with an index finger abduction at 10% of maximal force (10%-DT) or 30% (30%-DT). Significant results of the repeated-measures ANOVA are presented as F scores and P values.
In general, MS patients responded significantly slower (P < .001), made more errors (P = .050), and showed greater variability in their reaction times (P = .031; Figure 3). Interaction effects of MS by task were only found for reaction times (P = .026), showing a greater increase in dual- versus single-task conditions for MS patients than age-, education-, and sex-matched controls. Additionally, an interaction effect of Session force and MS was found. This indicated longer reaction times during 30%-DT compared with 10%-DT, particularly in MS patients.
Relationship Between Perceived Fatigue and DT Costs
In MS patients, significant associations were found between the MFIS cognitive subscale and DT costs of 30%-DT accuracy scores (after correction for age; rpartial = 0.60; P = .019), 30%-DT reaction times (rpartial = 0.67; P = .007), and 10%-DT variability (rpartial = 0.52; P = .045). Participants with higher perceived cognitive fatigue presented more DT costs, mainly during the fatiguing, 30%-DT.
The number of blocks for which a person maintained target force during 30%-DT gives an indication of the fatigability of the FDI. A model as proposed by Steens et al 42 that includes HADS depression, fatigability, and MVC could significantly explain the differences in FSS score in the MS group (R2 = 0.53, P = .026; HADS depression: rpartial = 0.66, P = .011; fatigability: rpartial = 0.60, P = .024; MVC: rpartial = −0.43, P = .127). Participants with higher FSS scores had higher HADS scores, and were more fatigable (lower number of blocks, after correcting for their MVC 42 ).
Discussion
This study showed that MS patients performed a cognitive task slower, with more errors, and with a greater variability in their responses compared with controls matched for age, sex, and education. Compared with controls, MS patients’ reaction times increased to a greater extent when going from a single task to a DT. Furthermore, muscle fatigue resulted in an additional decline in cognitive performance of MS patients, albeit only of their reaction times. Increased levels of cognitive fatigue (MFIS scores) in MS patients were associated with increased cognitive DT costs. A model that included depression, fatigability, and MVC was associated with a general sense of fatigue (FSS score).
MS Patients Responded Slower, With More Errors and Higher Variability
In agreement with the existing literature, MS patients reacted slower than controls.3,14,44-48 Increased reaction times are thought to be a sign of attentional deficits,45-47 with decreased information processing speed 3 possibly accompanied by a slowing of the motor response. 44 Included patients were only mildly affected by MS, and all but 3 were still employed or worked as volunteers. Hardly any medication was taken, except immune-modulating medication. The fact that increased reaction times were found in these participants indicates that attentional deficits can already be present in the mild stages of MS. 4
Accuracy scores were lower in MS patients (conforming with some studies,14,45,48 although others did not find effects3,44,46). Previous studies used relatively simple tasks, resulting in few errors (less than 10%). This may explain why some studies were not able to distinguish between patients and controls. Additionally, we found an effect of task and force level, with more errors in the DT and in the 30%-DT, indicating that task complexity affected response accuracy. 14
Variability of reaction times is used as a measure of information processing speed, and an increase points to decreased ability to sustain attention.49,50 The greater variability48,51,52 suggests that MS patients had problems with sustained attention and were less able to respond consistently.
Response Preparation During Cognitive Task Performance Was Not Affected by MS
Task difficulty was manipulated by using different stimulus probabilities; that is, stimuli were presented with a probability of 70% or 30%. After a practice session, participants prepared preferentially for the frequent stimulus.21-23,53,54 This was visible by faster reaction times on frequent stimuli and more errors on infrequent stimuli (Table 3, Figure 3). The present data did not show an interaction effect between stimulus probability and MS (Table 3), implying that MS patients prepared as well as their age-matched controls. 23 Additionally, this result indicates that performance of MS patients did not further deteriorate when the task became more difficult; responses to the 2 stimuli differed in reaction times and accuracy but were similar for both groups. 14 Other studies that changed task difficulty did find differences between patients and controls.45,47,48,52 It is conceivable that because our MS patients were only mildly affected, increased difficulty did not result in overt performance deficits. 14
Reduced DT Performance With an Additional Decrease With Muscle Fatigue in MS
Studies using relatively simple cognitive-motor DTs 20 or cognitive-cognitive tasks14,16 did not find reduced performance in MS patients. Conversely, more demanding paradigms resulted in DT interference in MS: on cognitive-walking tasks,13,15 cognitive-posture tasks,17,18 and cognitive-cognitive tasks. 20 These results, combined with our findings, indicate that MS patients are able to perform demanding DTs, but at greater DT costs.
Studies in controls using the same cognitive-motor DT as the current study showed decreased cognitive performance in the DT, with an additional decline with muscle fatigue.21,23 The present study extended this observation to MS patients who demonstrated an additional performance decline, albeit only in their reaction times, both from a single task to a DT and from a low-force to a high-force DT.
Functional MRI data show increased activity during submaximal motor tasks in MS patients, not only in motor areas but also in areas involved in attention, such as prefrontal and parietal areas.9-11,55 A DT requires participants to divide attention between tasks. 12 If our motor task demanded increased attention in patients, fewer resources could be allocated to the cognitive task, resulting in a reduced performance. Moreover, during fatiguing motor tasks, MS patients have difficulty increasing their voluntary drive to compensate for fatigue-related changes downstream of the motor cortex.29,42,56-58 This deficient voluntary activation is accompanied by a smaller increase in BOLD activity. 29 In that experiment, force output did not differ between controls and MS patients. However, it can be surmised that a smaller increase in cortical motor activity with fatigue could be responsible for the greater force variability observed during the 30%-DT task in MS patients.
Perceived Fatigue Was Associated With Performance Decrease of the DT
We found associations between task performance and measures of perceived fatigue. Although these associations should be treated cautiously, because of the small number of participants, it is a novel and intriguing observation. Nevertheless, these associations do not provide us with the direction of the relation. DTs are often performed during everyday situations, and participants with higher DT costs might display higher levels of cognitive fatigue. 13 Conversely, it is conceivable that participants perceiving high levels of cognitive fatigue perform less well on cognitive tasks, especially in effortful conditions.
The association between the FSS score and HADS depression score, MVC, and muscle fatigue confirms an earlier model, 42 referring to the multidimensionality of MS-related fatigue.
Limitations of the Study
Our patient group was atypical, in that we included more men than women, whereas it is commonly accepted that women are more often affected by MS. 59 We believe that this is a consequence of the criterion that patients were not allowed to take fatigue-modulating medication, which seemed to be used more often by women than men. However, we do believe that the data found in this study apply to both sexes. This is supported by preliminary investigations where sex, added as a between-subjects factor in the analyses, did not reveal any effects.
Knowledge about information processing speed as measured by the symbol digit modality task or by the paced auditory serial addition task (PASAT) would have added to the interpretation of the results of the DT costs.
Conclusions and Implications
DT situations in daily life may prove challenging for MS patients, especially under fatiguing circumstances. Our results showed that fatigue effects are not confined to the motor system but also affect cognitive parameters. The fact that these cognitive effects are already present in patients who have only mild symptoms stresses the importance of further research on how to counteract these effects with medication or rehabilitation therapies (eg, Kramer et al 60 ), especially because the consequences of reduced attention can be serious (eg, errors in decision making, stumbling, or falling). Further information of possible interactions between motor and cognitive tasks is also essential for patients and caregivers in organizing their daily activities.
In conclusion, MS patients perform less well on a cognitive task compared with controls, and although the cognitive performance of all participants deteriorates under DT conditions, the decrease is stronger in MS patients. Muscle fatigue leads to a further deterioration in cognitive performance, which is again stronger in MS patients. These results point to problems that patients may encounter in the present society, where attentional demands and DT performance become increasingly common because of widespread use of electronic devices. The observation that DT costs are positively associated with perceived fatigue could reflect effects of these increased cognitive demands in everyday life.
Footnotes
Acknowledgements
We thank Tjalling Nijboer, Cobi Bolwijn, Marina Kaspar, and Christine Sanserino for help with the experimental setup, patient inclusion, data collection, and editing of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.