
Abstract
Background. Simultaneous execution of motor and cognitive tasks can result in worsened performance on one or both tasks, indicating cognitive-motor interference (CMI). A growing amount of research on CMI in persons with multiple sclerosis (pwMS) is observed. However, psychometric properties of dual-task outcomes have been scarcely reported. Objective. To investigate the between-day test-retest reliability of the motor and cognitive dual-task costs (DTCs) during multiple CMI test conditions with various task complexities in pwMS and matched healthy controls (HCs). Methods. A total of 34 pwMS (Expanded Disability Status Scale score 3.0 ± 0.8) and 31 HCs were tested and retested on 3 single cognitive, 4 single motor, and 12 cognitive-motor dual tasks. Cognitive tasks included serial subtraction by 7, titrated digit span backward, and auditory vigilance. Motor tasks were walking at self-selected speed, over obstacles, crisscross, and while carrying a water-filled cup. Outcome measures were cognitive and motor DTC, calculated as percentage change of dual-task performance compared with single-task performance. Intraclass correlations (ICCs) and Spearman correlation coefficients were calculated as appropriate. Results. For DTCmotor of gait speed, ICCs ranged from 0.45 to 0.81 and Spearman correlations from 0.74 to 0.82. For DTCcognitive, ICCs ranged from −0.18 to 0.49 and Spearman correlations from −0.28 to 0.26. Reliability depended on the type of motor and cognitive task. Conclusion. Reliability of the DTCmotor was, overall, good, whereas that of the DTCcognitive was poor. The “walking” and “cup” dual-task conditions were the most reliable regardless of the integrated cognitive task.
Introduction
Dual tasking, such as walking while talking or browsing a smart phone while walking, is a common everyday act that can be defined as “the concurrent performance of two tasks that can be executed independently, measured separately and have distinct goals.” 1 However, simultaneous performance of a motor (eg, walking) and a cognitive (eg, talking) task may be difficult and lead to worsening in performance on one or both tasks. Such deterioration in performance has been conceptualized as cognitive-motor interference (CMI).
CMI is usually investigated with a dual-task paradigm in which a motor task (eg, walking, balance) and a cognitive task (eg, subtracting, word list generation) are performed separately and concurrently. The dual-task cost (DTC) quantifies this interference and is the percentage change of dual-task performance compared with single-task performance. 2 In healthy individuals and elderly people, CMI assessment during walking is a common way to gauge the interaction between cognition and mobility in daily life. 3 Difficulties with dual tasking during walking were associated with a higher fall risk in elderly people.4,5 Also, in persons with multiple sclerosis (pwMS), fall risk may be related with DTC of walking (velocity, stride length, and cadence)6,7 and with DTC of standing balance. 8 These consequences highlight the need to assess and treat CMI.
Walking and cognitive impairments are common features in pwMS, with prevalence rates ranging between 41% and 75%, 9 and 43% and 70%,10,11 respectively. Because of impaired sensory and motor system functions, walking may become less automatic and require increased attention, whereas at the same time, pwMS suffer from reduced attentional and executive function, possibly leading to worsening in dual-task (DT) performance. 11 Recent reviews in MS reported diminished performance on motor performance (DTCmotor) and on cognitive performance (DTCcognitive) under DT conditions, ranging from ~6% to ~27%2,12 and from ~6% to ~16%, 12 respectively. It is unclear to what extent CMI in pwMS deviates from that of healthy controls (HCs). Contradictory results were found in different reviews on whether pwMS showed greater decrements compared with HC in walking or balance2,12,13 or in cognitive tasks performance14-17 under DT conditions. Across studies, however, diverse combinations of cognitive-motor DTs have been used, hampering direct comparisons of results. Moreover, cognitive tasks from various cognitive domains may result in different DTCs in persons with and without MS.13,18 Additionally, it is scarcely investigated whether the DTC is dependent on the complexity of the motor task.
Despite the increasing interest in DTC as a new ecological disease outcome measure, reported psychometric properties (reliability, validity, and responsiveness) are still rare, halting the use of DTC as an experimental outcome measure. 19 As shown by 2 recent reviews, conducted in individuals with diverse neurological conditions and in elderly people, absolute measures of gait parameters (velocity, stride length, double support time, etc) under DT conditions can be reliably measured.19,20 In the cognitive domain, cognitive performances under DT conditions and cognitive DTCs have, conversely, shown lower reliability values than gait parameters did in stroke and Parkinsonian patients. 19 In pwMS, the reliability of absolute gait parameters under DT conditions was investigated during normal walking 21 and walking over a narrow pathway. 22 In daily life, however, various complex motor tasks such as walking over obstacles or carrying a cup with water are common acts. Therefore, there is a need to investigate the reliability of DT outcomes in more complex motor tasks as well. Most notably, although Prosperini et al 23 reported excellent test-retest reliability for outcomes of dual-task balance and cognition, reliability of relative CMI outcome measures, such as DTCmotor and DTCcognitive, during walking is still unknown in pwMS. 19
It is important to study the psychometric properties of the motor and cognitive DTCs to ensure accurate measurements and to be able to allow for sound interpretations of (change) scores of CMI in pwMS for clinical purposes or for research. The aim of the present study was to examine the between-day test-retest reliability of CMI of both motor and cognitive performance during different DT conditions, with motor and cognitive tasks of various task complexities, in pwMS and age- and gender-matched HCs. We hypothesized the reliability of the motor DTC to be good and expected lower reliability values for the cognitive DTC compared with the motor DTC. 19
Method
Participants
Between September 2016 and April 2017, 34 pwMS and 31 age- and gender-matched HCs participated in the study in the Masku Neurological Rehabilitation Centre (Finland) and the Centre Hospitalier Universitaire de Liège (Belgium). The sample was a convenience sample. Prospective participants were recruited among the patients from the participating centers and via the Neuro Society in South-Western Finland. Inclusion criteria for pwMS and HCs were age between 18 and 65 years and minimal cognitive function as measured with the Mini Mental State Examination ≥26. 24 Inclusion criteria for pwMS were as follows: diagnosis of MS according to McDonald criteria, Expanded Disability Status Scale (EDSS) ≥2 and ≤5, 25 no relapse within the past 30 days, no changes in immunomodulatory disease treatment and no corticoid-therapy within the past 50 days, and presence of DT interference (DT screening list ≥1). 26 Participants were excluded if there were other medical conditions interfering with mobility, other neurological diagnoses, or MS-like syndromes such as neuromyelitis optica or when participants were not able to understand instructions or had major problems with hearing or vision. The study size was based on Hobart et al 27 who reported that sample sizes of a minimum of 20 persons provided robust reliability estimates. The study was approved by the ethical committees of the Centre Hospitalier Universitaire de Liège, Hasselt University and Hospital District of Southwest Finland and executed according to the Helsinki declaration. All participants received written information and signed informed consent.
Procedure
Testing was divided over 3 days. On day 1, descriptive outcomes (demographics, cognition, mobility, quality of life measures, and a DT screening list) were assessed. On the second and third (test-retest) days, the participants performed the experimental CMI assessments. A time window of 3 to 5 days between the testing days was chosen to balance between minimizing practice effects from the first to the second test day and minimizing time in-between test sessions to avoid the possibility of changes in the patient’s functioning while fitting practical organization of scheduling tests.
Instruction booklets with a lot of details and internal agreements were provided, and pilot trials with new equipment were conducted before the actual start of study. Measures were assessed according to a standardized test protocol, including detailed test procedures, verbal instructions, and level of encouragement during testing, besides standardized electronic files to collect and transfer data. Data quality control was performed by the study coordinator.
Descriptive Outcome Measures
Data on age, gender, disease duration since diagnosis, type of MS, and disability level (EDSS) were collected. Cognition, mobility, and quality of life measures are described below.
Cognitive Function
The Brief Repeatable Battery of Neuropsychological Tests 28 was used to assess participants’ cognitive function. This is a set of 5 tests in different cognitive domains: (1) the Selective Reminding Test measuring verbal learning and delayed recall; (2) the 10/36 Spatial Recall Test to assess visuospatial learning and delayed recall; (3) the Symbol Digital Modalities Test and (4) the Paced Auditory Serial Addition Test (PASAT), which are 2 tests of sustained attention, concentration, and information processing speed; and (5) the Word List Generation, or fluency task to measure semantic word retrieval.
Motor Function
Motor function was assessed using the Timed 25 Foot-Walk, 29 with maximal walking speed; the Timed-Up-and-Go test 30 ; the Dynamic Gait Index 31 ; and the 2-minute walking test. 32 The Multiple Sclerosis Walking Scale–12 33 and Falls Efficacy Scale 34 were completed to measure perception of the limitations in walking ability caused by MS and the concern about the possibility of falling, respectively.
Quality of Life, Perceived Fatigue, and Daily Life Dual Tasking
The Multiple Sclerosis Impact Scale–29 35 and the Modified Fatigue Impact Scale 36 were used to record participants’ perceived impact of MS on day-to-day life and of fatigue on daily functioning, respectively. Furthermore, the Dual Task Questionnaire of Evans et al 37 asked how often participants experienced problems with DTs (eg, needing to stop an activity to talk) over the past 2 weeks.
Experimental Outcome Measures
Three single cognitive-, 4 single motor-, and 12 integrated cognitive-motor DTs were performed twice. All tasks had a duration of 1 minute. The order in which the blocks of single-cognitive, single-motor, or cognitive-motor DTs were performed was computer randomized between participants as well as the sequence of each separate task within 1 block. The sequence of the tasks performed was the same during the test and retest session for a participant.
Cognitive Tasks
The cognitive tasks used were the following: the titrated digit span backward, 38 the serial 7 subtraction test, 39 and the auditory vigilance with alphabets task. These cognitive tasks were chosen based on pilot studies, and compatibility with walking and on the cognitive domains, because information processing speed, attention, and working memory are among the most affected cognitive domains in pwMS. 40 Cognitive stimuli were delivered by auditory speech via a headset microphone with noise cancelling while participant responses were noted by the assessor and audiorecorded on a specifically developed tablet application. For all cognitive tasks, an example was given by the researcher, and participants practiced with a short example before the test to make sure the participants fully understood the task.
The digit span backward loads working memory. Participants listened to a titrated string of digits (eg, 5-3-1-8), at the presented rate of 1 number per second and repeated them in the reverse order. The individual sequence length was assessed for each participant on the first CMI test day, before the first trial, to determine the participant’s digit span. Participants started at a digit length of 3 numbers, and length was increased by 1 digit. CMI of the participant was tested with the last sequence length at which 3 of 4 trials were performed correctly. Performance on the digit span task was quantified as “number of correct answers.”
The serial 7 subtraction test loads working memory and information processing speed. Participants had to count backward from a given number (between 152 and 198). Performance of this task was determined as “number of correct subtractions.” Answers were counted as correct each time there was a subtraction of 7 from the previous number.
The auditory vigilance task is a test of sustained attention. Vigilance refers to a state of readiness to detect and respond to certain small changes occurring at random time intervals.41,42 Participants listened to letters presented at the rate of 1 letter per 2.5 s and said aloud “yes” every time they heard 1 of the 2 target letters (eg, “L” or “R”) and were asked not to respond when another letter was heard. Then, 24 letters were randomly presented, including 10 target letters. Performance of this task was determined as “number of correct answers” because the reaction time could not be calculated as a result of technical problems.
Motor Tasks
Walking was performed on a 30-m, free-of-obstacles, quiet walkway that was marked with 80 cm start and 80 cm turning lines. Four different motor tasks were performed: (1) walking at self-selected speed (“walk”), (2) walking while carrying a cup filled with water (“cup”), (3) walking while stepping over obstacles (10 cm height and width) placed every 3 m (“obstacles”), and (4) walking crisscross from cone to cone every 2 m with 80 cm fixed width in between (“crisscross”) (Figure 1). For all motor tasks, the researcher demonstrated how to walk over the walkway, and participants walked a part of it. All tasks were performed for 1 minute at a self-selected, comfortable speed. For safety reasons, the examiner always walked close to but behind the participant. The motor tasks were chosen based on the criterion that they are all common walking activities carried out in daily life but differing in motor complexity and required attention or adaptation. Besides, the motor tasks were based on previous studies investigating reliability in persons with neurological conditions during various walking tasks.21,43 Spatiotemporal gait parameters were recorded by 3 wearable APDM sensors placed on each foot and in the lower lumbar region, with the respective Mobility Lab Software (Portland, OR). For the walking, cup, and obstacles conditions, these parameters were gait speed (m/s), cadence (steps/min), double support time (percentage), and stride length (m), and for the crisscross conditions, this was turn velocity (degrees/s).

Walking over obstacles and walking crisscross.
Dual Cognitive-Motor Task Performance
Participants performed the motor and cognitive tasks described above simultaneously in 12 different DT conditions and were instructed to perform both tests at their best level (to avoid any task prioritization). The same procedures as described above for the single cognitive and single motor task conditions were used. To examine DT performance, DTCs were calculated for the diverse parameters for each DT condition as follows:


Statistical Analysis
All analysis were conducted with IBM SPSS Statistics 25 and performed for pwMS and HC separately. Outliers were analyzed with the DTCs of gait speed (walk, obstacles, cup), turning velocity (crisscross), and number of correct answers. DTCs were defined as outliers when they were more than or less than 3 SDs from the mean on test or retest moment and excluded from further analysis per DT condition. Normality of the data was assessed with the Shapiro-Wilk test.
Test-retest reliability was examined for all 12 DT conditions for the DTCs of 1 cognitive parameter (number of correct answers) and 5 motor parameters (gait speed, cadence, double support time, stride length, and turn velocity). To assess reliability, intraclass correlation coefficients (ICCs) for single measurements with a 2-way random effect with absolute agreement (ICC2,1) and Spearman correlation coefficients were calculated, for normally and nonnormally distributed data, respectively. For ICC values, reliability was categorized according to Shrout and Fleiss’ cutoffs as follows: >0.75 excellent, >0.6 good, >0.4 fair, or ≤0.4 poor. 44 Landis and Koch’s cutoffs categorizing reliability as excellent >0.8, good >0.6, fair >0.2, or poor ≤0.2 were used for Spearman correlation coefficients. 45 Listwise deletion was used in the case of missing data, meaning that a participant was excluded from data analyses only for the DT condition in which a DTC value was missing.
Agreement between repeated measures was analyzed using Bland-Altman plots. The mean difference between the 2 test moments was plotted against the mean of the 2 test moments. 95% Limits of Agreement (LOAs) were defined as 1.96 × SD greater than and less than the mean difference. The plots were only given for pwMS for the motor DTCs of gait speed over the 9 diverse dual walk, cup, and obstacles conditions and for the cognitive DTCs in the dual walk conditions.46,47
Means and SDs of absolute cognitive and motor performance during the single and dual walk conditions and DTCs were provided for gait speed and number of correct answers as supplementary data. A paired t-test or the Wilcoxon signed rank test was executed to assess systematic differences between both test sessions for normally and nonnormally distributed data, respectively. The standard error of measurement [SEM = SDpooled × √(1-ICC)] was calculated to provide an absolute value of reliability to be able to quantify the precision of individual scores on a test. 48 The minimal detectable change (MDC = SEM × 1.96 × √2) was calculated to be able to determine whether a change in score can be considered without measurement error. 48
Results
Descriptive Characteristics
Descriptive data of the participants are presented in Table 1. In total, 35 pwMS and 33 HCs were recruited to participate in the study. One of the pwMS and 2 HCs did not perform the retest because of sickness and lack of interest. Therefore, 34 pwMS and 31 HCs completed the whole study. Age and gender distribution were equal in the 2 groups, with around two-third being female participants. For pwMS, disease duration was on average 11.9 ± 10.6 years, with most of them having a relapsing remitting disease form (82.4%). HCs and pwMS did not perform differently on the Selective Reminding, Spatial Recall, Word List Generation, and PASAT 2-s tests. pwMS performed worse on all other tests of cognition and mobility and on the questionnaires for quality of life and dual tasking in daily life.
Descriptive Data of pwMS and HCs.
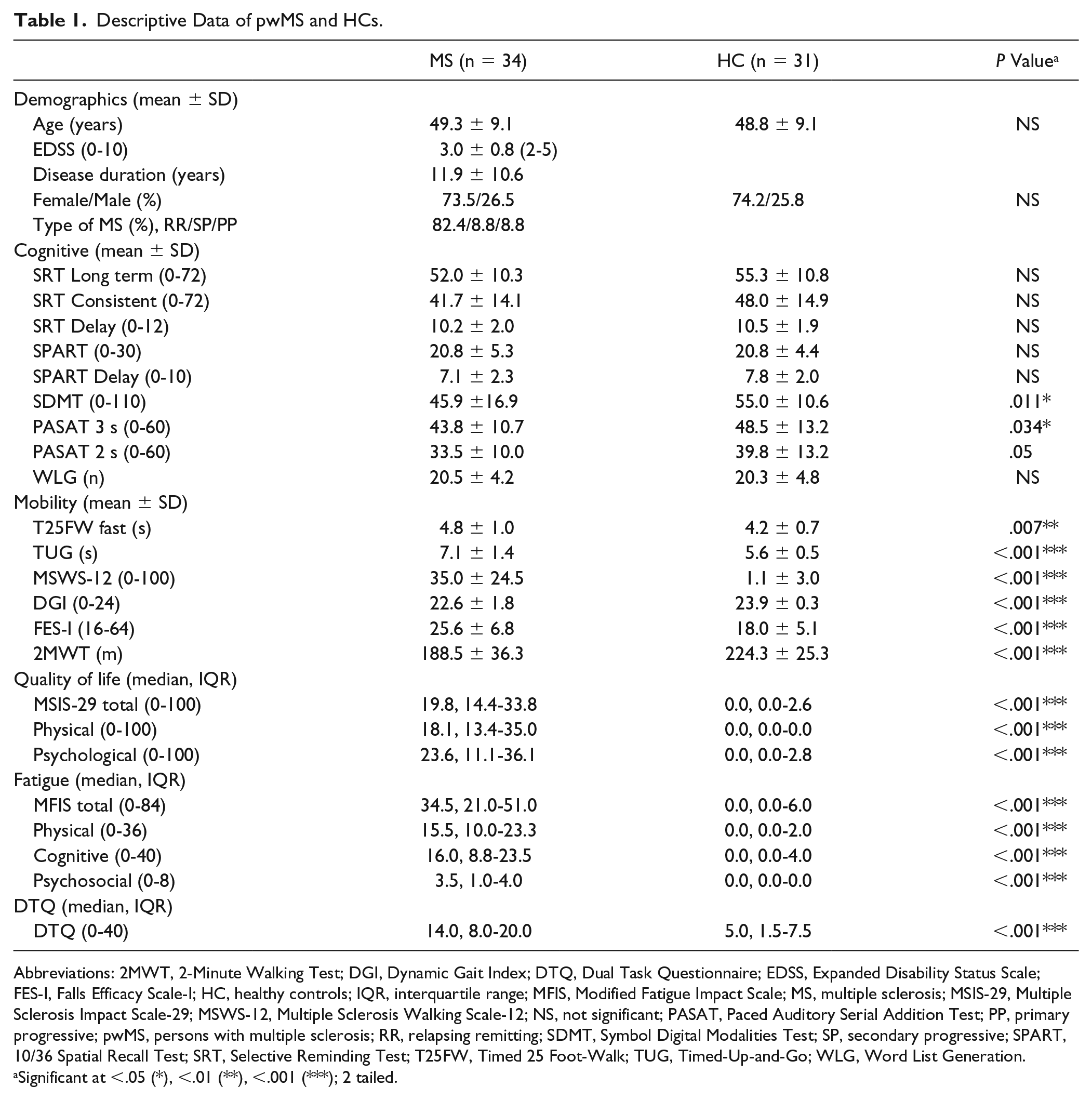
Abbreviations: 2MWT, 2-Minute Walking Test; DGI, Dynamic Gait Index; DTQ, Dual Task Questionnaire; EDSS, Expanded Disability Status Scale; FES-I, Falls Efficacy Scale-I; HC, healthy controls; IQR, interquartile range; MFIS, Modified Fatigue Impact Scale; MS, multiple sclerosis; MSIS-29, Multiple Sclerosis Impact Scale-29; MSWS-12, Multiple Sclerosis Walking Scale-12; NS, not significant; PASAT, Paced Auditory Serial Addition Test; PP, primary progressive; pwMS, persons with multiple sclerosis; RR, relapsing remitting; SDMT, Symbol Digital Modalities Test; SP, secondary progressive; SPART, 10/36 Spatial Recall Test; SRT, Selective Reminding Test; T25FW, Timed 25 Foot-Walk; TUG, Timed-Up-and-Go; WLG, Word List Generation.
Significant at <.05 (*), <.01 (**), <.001 (***); 2 tailed.
Table 2 shows the motor and cognitive DTCs on test and retest for all DT conditions for the parameters gait speed (walk, obstacles, cup), turning velocity (crisscross) and number of correct answers. The DTCmotor ranged from 8.7% to 15.8%, from 11.6% to 18.1%, and from 3.7% to 12.1% in the digit span, subtraction, and vigilance DT conditions, respectively. The DTCcognitive ranged from −0.8% to 18.2% on the digit span task, from −5.0% to 16.9% on the subtraction task, and from −0.0% to 3.9% on the vigilance task.
DTCs of Gait Speed, Turn Velocity, and Number of Correct Answers During Dual-Task Conditions on Test and Retest.
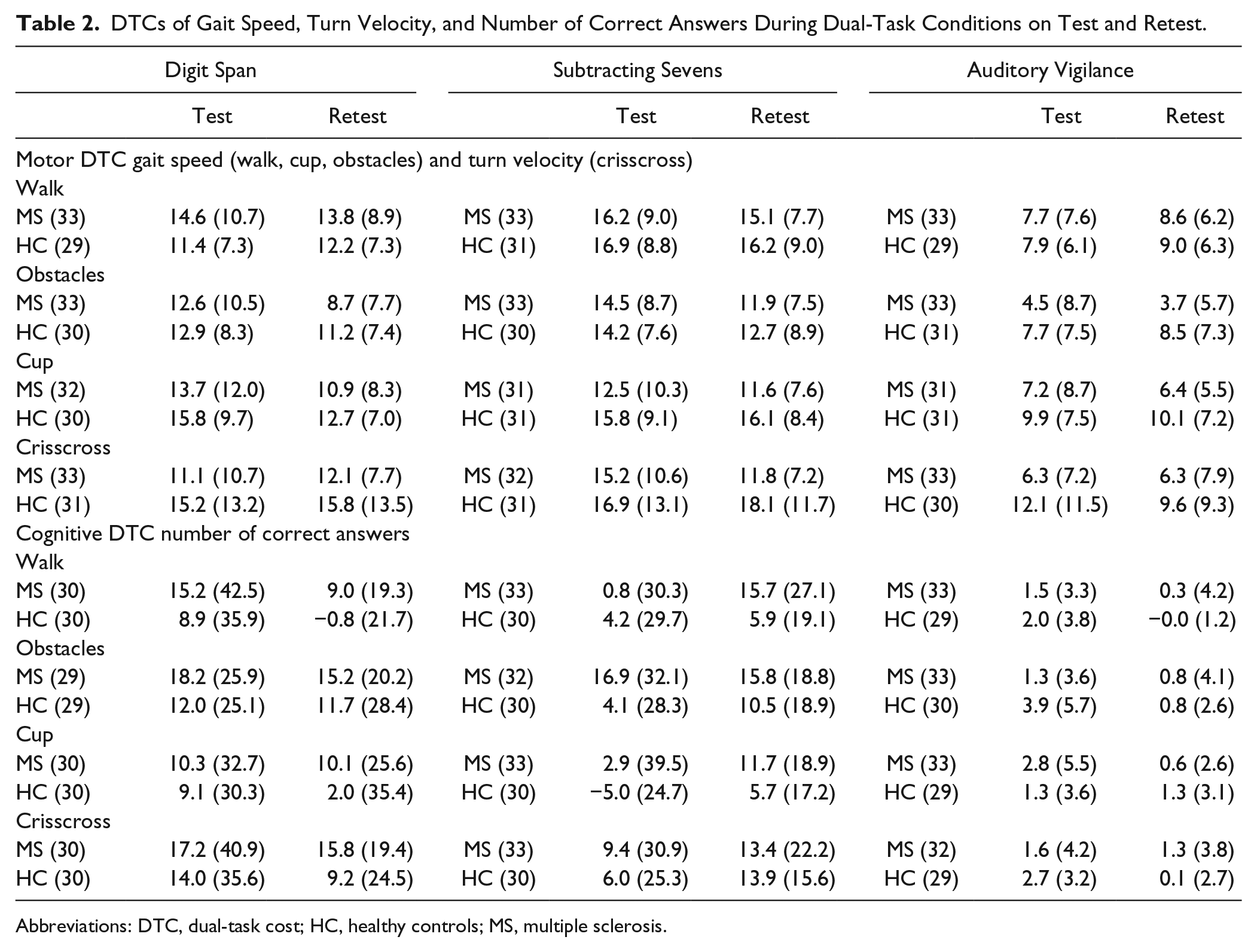
Abbreviations: DTC, dual-task cost; HC, healthy controls; MS, multiple sclerosis.
Reliability of Motor Dual-Task Costs
Table 3 and Figure 2 show the test-retest reliability of the DTCs for all motor and cognitive outcome parameters in all DT conditions for both pwMS and HC (Figure 2 visualizes the reliability of the various DTCs). In total, 0.90% of the 6630 DTCs are missing because of technical errors or a zero score on the cognitive single task. In pwMS, the reliability of the DTCmotor for all gait parameters in the walk conditions was mostly excellent and in the cup conditions mostly good. In the obstacles conditions, the reliability of the motor DTCs was mostly fair and ranged from poor to good. In the crisscross conditions, the reliability of the DTCmotor of turn velocity was mostly poor for pwMS.
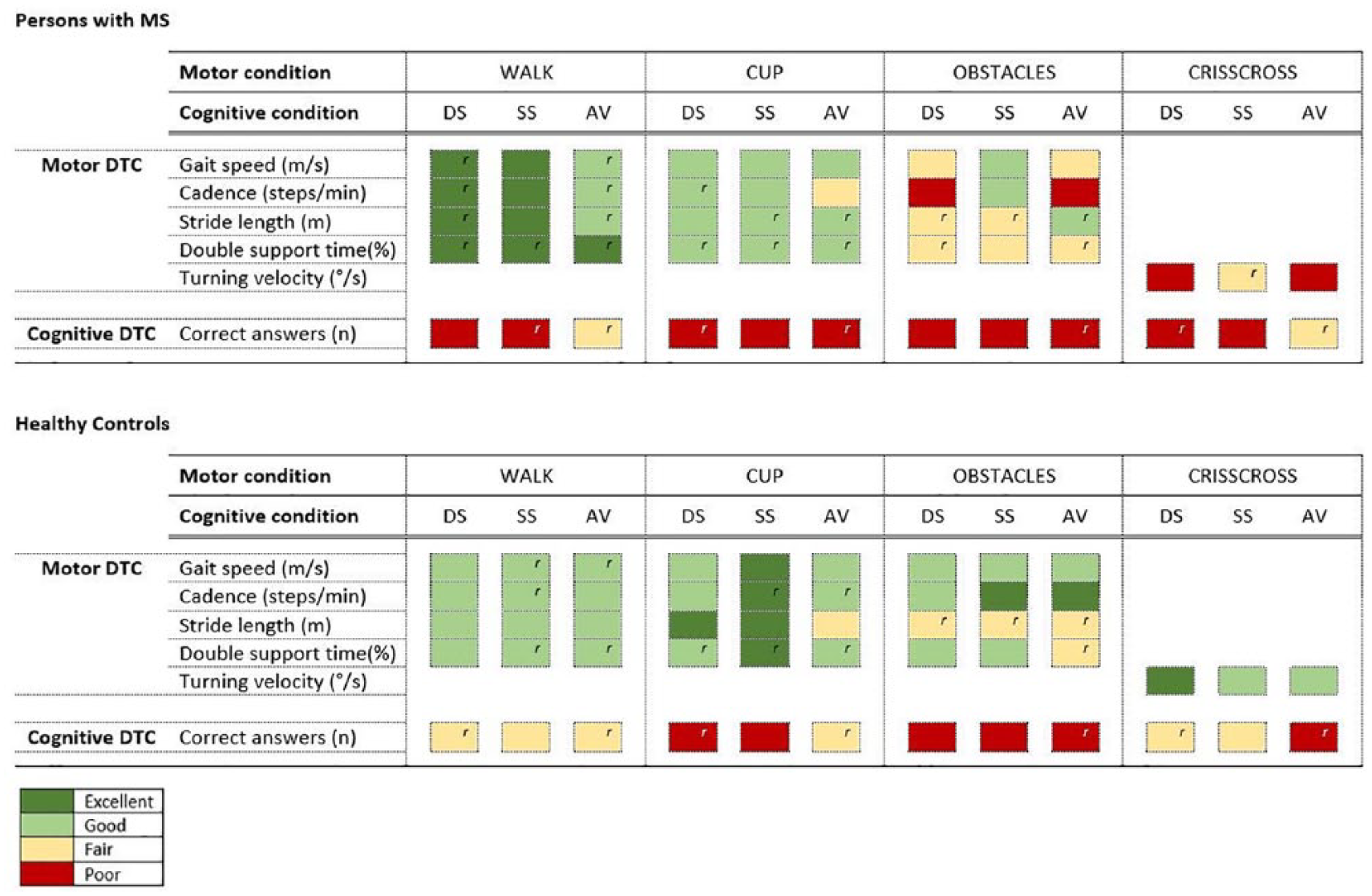
Test-retest reliability (ICC or Spearman r) of the dual-task costs (DTCs) for motor and cognitive measures for pwMS (upper figure) and HCs (lower figure). Reliability is categorized as excellent >0.75, good >0.6, fair >0.4, or poor ≤0.4 for ICC values and as excellent >0.8, good >0.6, fair >0.2, or poor ≤0.2 for Spearman correlations.
Test-Retest Reliability of Motor and Cognitive DTC per Outcome Parameters in All Dual-Task Conditions for pwMS and HCs. a
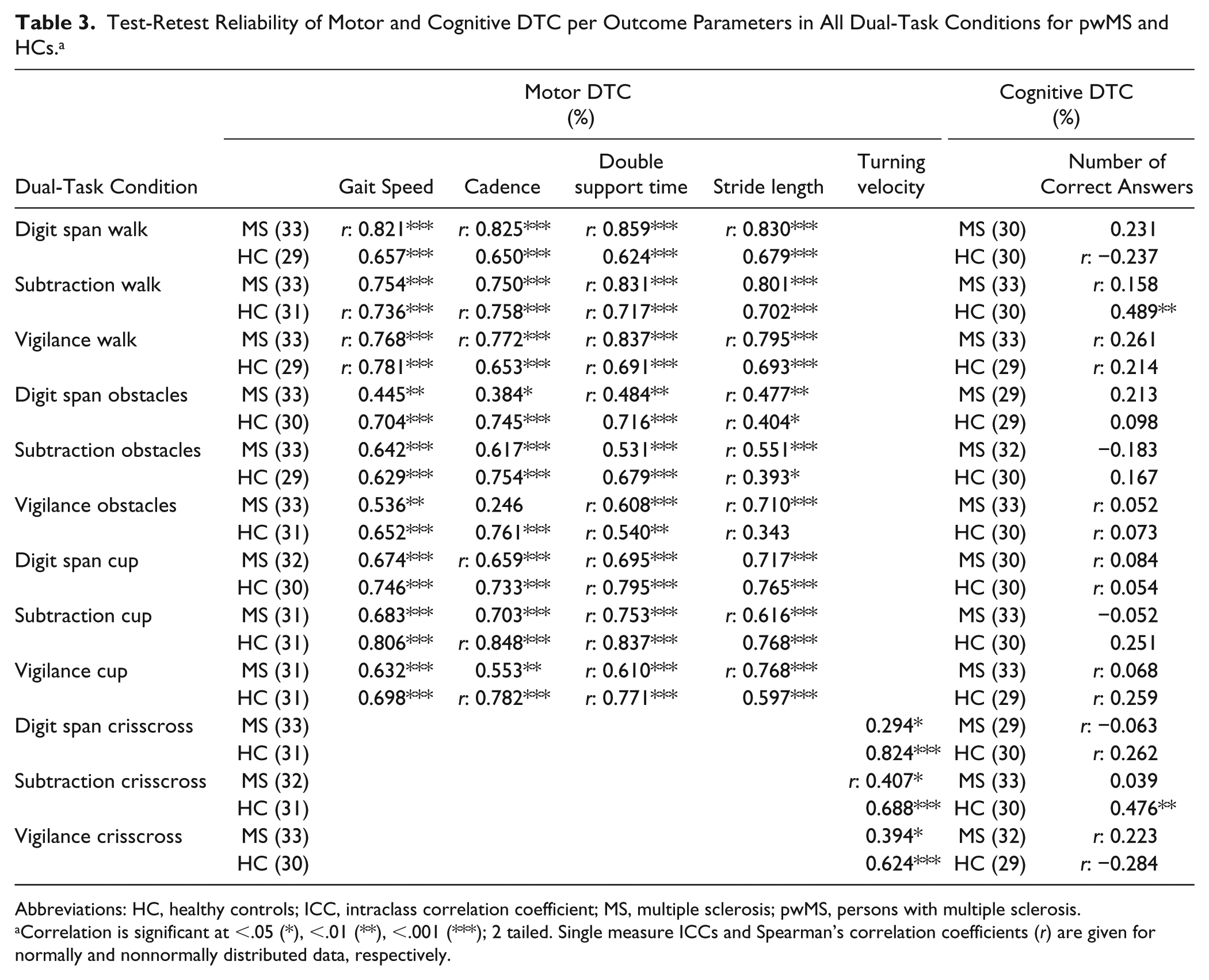
Abbreviations: HC, healthy controls; ICC, intraclass correlation coefficient; MS, multiple sclerosis; pwMS, persons with multiple sclerosis.
Correlation is significant at <.05 (*), <.01 (**), <.001 (***); 2 tailed. Single measure ICCs and Spearman’s correlation coefficients (r) are given for normally and nonnormally distributed data, respectively.
For HCs, the reliability of the DTCmotor was good for all gait parameters in the walk conditions and mostly good to excellent in the cup conditions. In the obstacles conditions, the reliability of the DTCmotor of gait speed, cadence, and double support time was mostly good to excellent, whereas the reliability of the DTCmotor of stride length was fair. The reliability of the DTCmotor in the crisscross conditions was good to excellent for HCs.
Bland-Altman plots for DTCmotor of gait speed for pwMS are presented in Figure 3. LOAs for DTCmotor gait speed were ±8.6% to ±11.5% in the walk, ±12.3% to ±15.8% in the cup, and ±12.9% to ±18.6% in the obstacles conditions. Points were equally distributed around zero for most conditions. However, the digit span obstacles and subtraction obstacles conditions showed a general pattern of decrease in DTCmotor with repeated measurements of −3.9% and −2.6%, respectively. Furthermore, the vigilance obstacles and all dual cup conditions showed a trend of dependence of the difference scores on the magnitude of the DTCmotor. It seems that pwMS with a low mean DTCmotor had a greater DTCmotor on retest- than on test-moment, whereas in contrast, pwMS with a high mean DTCmotor showed smaller DTCmotor on retest- than on test-moment.
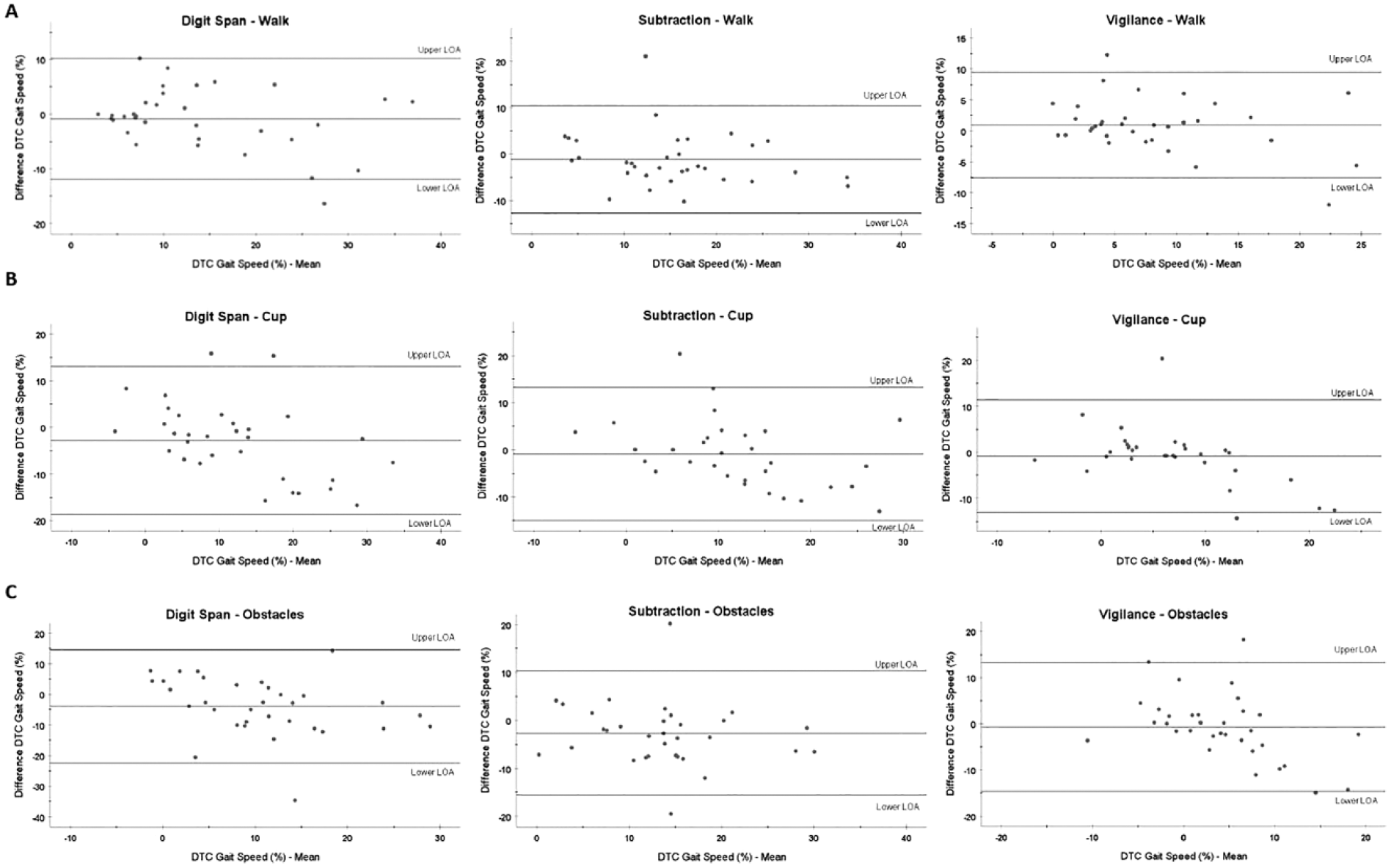
Bland-Altman plots for persons with MS for the DTCmotor of gait speed in the (A) walk conditions, (B) cup conditions, and (C) obstacles conditions for all cognitive tasks. It should be noted that the axes are different per plot.
Reliability of Cognitive Dual-Task Costs
Table 3 and Figure 2 show the test-retest reliability of the cognitive DTCs in all DT conditions. For pwMS, reliability of the DTCcognitive was mostly poor, independent of the DT condition. For HCs, the reliability of the DTCcognitive was fair in the walk conditions, poor in the obstacles conditions, and poor to fair in the cup and crisscross conditions. Bland-Altman plots for DTCcognitive are presented in Figure 4. LOAs were ±80.3%, ±78.3%, and ±9.6% in the digit span, subtraction, and vigilance dual walk conditions, respectively.

Bland-Altman plots for persons with MS for the DTCcognitive of number of correct answers in the walk conditions for all cognitive tasks. It should be noted that the axes are different per plot.
Absolute Motor and Cognitive Performance in Walk Conditions and Its Reliability
Supplementary Table 1 shows absolute single- and dual-task performance and reliability of the absolute measures during the walk conditions. For pwMS, significant differences between test and retest in number of correct answers were found for performance on the digit span in the single and DT conditions and for subtraction in the single-task condition. For HCs, significant differences between test and retest in number of correct answers were found for performance on the subtraction task in the single-task condition and on the digit span, subtraction, and vigilance tasks in the DT conditions. In all these cases, scores were higher on retest- than on test-moment (Supplementary data, Table 1).
Reliability of single-task and DT gait speed (absolute value) was excellent for both groups (MS: ICC = 0.87-0.94; HC: ICC = 0.88-0.93). The SEM for gait speed during single-task and DT performance ranged from 0.04 to 0.07 m/s, resulting in a MDC ranging from 0.12 to 0.20 m/s for pwMS and HCs.
For performance on the cognitive tasks (number of correct answers), reliability in the single-task conditions was poor to fair for vigilance (MS: Spearman’s r = 0.05; HC: Spearman’s r = 0.55), fair to good for digit span (MS: ICC = 0.71; HC: ICC = 0.60), and excellent for subtraction (MS: Spearman’s r = 0.82; HC: ICC = 0.79). In the dual walk conditions, reliability for the digit span and subtraction tasks was good for pwMS (ICC = 0.63-0.64) and excellent for HCs (ICC = 0.77-0.77). Reliability of the vigilance task under dual walk conditions was poor (MS: Spearman’s r = 0.31; HC: r = 0.09). The SEM for number of correct answers on the digit span task during single-task and DT performance ranged from 1.29 to 1.63, resulting in a MDC ranging from 3.58 to 4.52 for pwMS and HCs. For number of correct answers on the subtraction task during single-task and DT performance, it ranged from 3.36 to 3.89, resulting in a MDC ranging from 9.32 to 10.79 for pwMS and HCs.
Discussion
This study, in persons with MS, is the first to show that the reliability of the DTCs, especially DTCmotor, depends strongly on the type and complexity of the motor DT and to some extent on the choice of gait parameter, regardless of the cognitive task. In contrast, the DTCcognitive showed poor test-retest reliability in pwMS and HCs.
The walk and cup, but not the obstacles and turning conditions, were shown to be reliable dual-task conditions to measure the DTCmotor in pwMS. None of the cognitive tasks used in the DT conditions resulted in a systematic higher or lower reliability of the DTCmotor. For pwMS, reliability of the DTCmotor seemed to decrease with increasing motor task complexity because reliability was the highest in the walk and cup, and the lowest in the obstacles and crisscross DT conditions. This pattern was not clearly observed in HCs. This pattern was also confirmed by inspecting B-A plots because the walk conditions showed acceptable agreement, whereas a learning effect was present in the obstacles conditions, and agreement tended to depend on the magnitude of the DTCmotor in the cup conditions. The significantly higher motor impairment in pwMS compared with HCs may have resulted in less confidence in DT conditions with larger motor complexity, leading to higher variation in motor performance and consequentially to a lower reliability. For example, turn parameters have been found to be important markers for self-perceived balance confidence of pwMS. 49 Whereas in HCs motor performance on the crisscross DT conditions could be reliably measured, this was not true in pwMS.
Multiple spatiotemporal gait parameters were measured in the present study. For the calculation of a DTCmotor, the choice of spatiotemporal gait parameter seems to have some influence on its reliability. For both groups, reliability of the motor DTCs of gait speed, cadence, stride length, and double support time was mostly good to excellent in the walk and cup conditions. Conversely, for the obstacles conditions, the reliability of the DTCmotor varied according to gait parameter. For example, in the obstacles conditions, stride length has to be adapted to the encountered obstacles; this probably leads to more variability and a lower reliability of the DTC on stride length. Only 1 study explored the reliability of DTC in an obstacle course and showed a low reliability of the DTC of walking time in stroke patients. 43
To our knowledge, this is the first study evaluating the reliability of the DTCcognitive during walking in pwMS. The poor reliability of the DTCcognitive is in accordance with a previous study in people with stroke. 43 Factors such as fatigue, psychological state, and attention may affect cognitive performance more than gait performance. 19 Learning effects were greater for cognitive tasks than for gait tasks because gait is more habitual behavior. Indeed, pwMS performed significantly better on the subtraction and digit span backward tasks during retest assessment than during the first assessment. This is in accordance with Strouwen et al, 44 who also found the digit span task to be subject to learning effects. The lack of sufficient practice might have led to a more pronounced learning effect over the 2 sessions and a lower reliability for the DTCcognitive of number of correct answers.
The low test-retest reliability of the DTCcognitive may also relate to methodological factors. First, the number of correct answers was used in the present study as cognitive performance outcome. Among other possible parameters are accuracy, error rate, correct response rate, and reaction time. In previous studies, fair to moderate reliability has been found for absolute DT error rate in Parkinson disease and MS,22,44 fair to excellent reliability for absolute DT correct response rate in chronic stroke, 43 and excellent reliability for absolute DT reaction time in Parkinson disease. 44 Including reaction time in cognitive performance measures seems to enhance reliability. Especially for the vigilance task, reaction time could be of more value because almost none of the participants made any or more than 1 error during the task. Second, the lower reliability of especially the cognitive DTCs may also be related to the instructions given to the participants. In the current study, the instruction was to perform both tasks at best levels to prohibit task prioritization. However, previous studies in pwMS comprising both cognitive and motor DTCs showed different prioritization strategies when no instruction to prioritize one of the tasks was given.14,15,50 Various task- and patient-related factors may affect prioritization strategies,14,51-54 illustrating the importance of measuring both the motor and cognitive DTC. 55 The present sample showed motor impairments in walking but no clear cognitive impairment except for processing speed.
For both motor and cognitive measures, absolute DT performance was shown to be more reliable than DTC. Absolute measure of gait speed under DT conditions demonstrated excellent reliability in pwMS and HCs, which is in accordance with 2 previous studies on DT reliability in pwMS showing excellent reliability for various absolute spatiotemporal gait parameters.21,22 Also comparable to previous findings,22,43,44 good to excellent reliability was found for the absolute cognitive performance under DT conditions for the digit span and subtraction tasks. However, large SDs and very broad ranges in the ICC 95% CIs were found, indicating large variability in cognitive performance. When calculating the DTC, measurement errors inherent to the single and the DT condition were both taken into account. This could partly explain the lower reliability of the DTCs. However, as Plummer and Eskes 55 described, it is important to take both absolute and relative measures into account to be able to conclude improvement in overall dual-task performance. For example, gait speed might improve in both single and DT conditions, resulting in the same DTC despite improvements. Notwithstanding, DTCs are relevant to compare different populations and diverse DT paradigms. Moreover, as described previously, to be able to analyze whether someone has improved in dual tasking, both a motor and cognitive DTC are needed to determine whether a new strategy—that is, gait priority or cognitive priority trade-off—has occurred or whether indeed an overall improvement has taken place. 55
Limitations
There are some limitations to this study. First of all, the sample size of 31 pwMS might be insufficient to arrive at generalized conclusions. The results are, therefore, confined to mildly motor and cognitive impaired pwMS. Second, one may comment on limited sample size. We are, however, confident in the observed results because our sample size matches previous studies on dual-task walking reliability in persons with MS21,22 and recommendations on reliability in neurological patients made by Hobart et al. 27 Importantly, current results are comparable to those of previous studies in neurological populations. The 3 cognitive tasks used in the current study were based on the cognitive domains involved—namely, information processing speed, working memory, and attention because these are frequently impaired in pwMS 40 —and on previous studies. Tasks of executive functioning such as the Stroop color word task and verbal fluency tasks have, however, also been shown to be promising concurrent cognitive tasks in pwMS13,56 and showed excellent test-retest reliability in a dual balancing task. 23
Conclusion
The present study provides valuable information on CMI assessments for further studies. It was shown that motor DTCs and absolute DT performance of various spatiotemporal gait parameters can be reliably measured in pwMS with motor impairments, if the complexity of the dual motor task is not too difficult. Walking and cup conditions were shown to be the most reliable DT conditions regardless of the integrated cognitive task. Cognitive performance during DT could not reliably be measured in pwMS and HCs, but the cognitive DTC is important for a complete understanding of DT performance. Testing multiple cognitive-motor dual-task combinations reliably is viable in pwMS and gives a better understanding of the dual-task performance when including both absolute and relative measures.
Supplemental Material
Supplementary_data_table_1_manuscript_test-retest_reliability_of_CMI-assessments_in_pwMS – Supplemental material for Test-Retest Reliability of Cognitive-Motor Interference Assessments in Walking With Various Task Complexities in Persons With Multiple Sclerosis
Supplemental material, Supplementary_data_table_1_manuscript_test-retest_reliability_of_CMI-assessments_in_pwMS for Test-Retest Reliability of Cognitive-Motor Interference Assessments in Walking With Various Task Complexities in Persons With Multiple Sclerosis by Renee Veldkamp, Anders Romberg, Paivi Hämäläinen, Xavier Giffroy, Lousin Moumdjian, Carmela Leone, Peter Feys and Ilse Baert in Neurorehabilitation and Neural Repair
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by RIMS by Novartis AG, MS Society Flanders, Swedish Promobilia Foundation, and SailingChallenge4MS.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.