
Abstract
Background and Purpose
Brain stimulation is an adjuvant strategy to promote rehabilitation after stroke. Here, we evaluated the influence of inclusion/exclusion criteria on enrollment in a transcranial direct current stimulation (tDCS) trial in the context of a racially/ethnically diverse acute stroke service at University of Texas Southwestern (UTSW).
Methods
3124 (59.7 ± 14.5 years) racially/ethnically diverse (38.4% non-Hispanic white, (W), Hispanic (H) 22%, African American (AA) 33.5%, Asian (A) 2.3%) patients were screened in the acute stroke service at UTSW. Demographics, stroke characteristics, and reasons for exclusion were recorded prospectively.
Results
2327 (74.5%) patients had a verified stroke. Only 44 of them (1.9%) were eligible. Causes for exclusion included in order of importance: (1) magnitude of upper extremity (UE) motor impairment, (2) prior strokes (s), (3) hemorrhagic stroke, (4) psychiatric condition or inability to follow instructions, and (5) old age, of these (2) and (4) were more common in AA patients but not in other minorities. 31 of the 44 eligible individuals were enrolled (W 1.68%, H 1.37%, AA .77%, A 3.774%). 90.5% of verified stroke patients did not exhibit contraindications for stimulation.
Conclusions
3 main conclusions emerged: (a) The main limitations for inclusion in brain stimulation trials of motor recovery were magnitude of UE motor impairments and stroke lesion characteristics, (b) most stroke patients could be stimulated with tDCS without safety concerns and (c) carefully tailored inclusion criteria could increase diversity in enrollment.
Clinical Trial Registration-URL: http://clinicaltrials.gov. Unique identifier: NCT01007136.
Introduction
The high incidence of disability related to upper extremity (UE) motor impairments due to stroke 1 has led to an increasing number of clinical trials of UE motor interventions. Among the most promising interventions are transcranial magnetic stimulation (TMS) and direct current stimulation (tDCS), which are now being tested in small-scale trials. 2 -22 Trial enrollment criteria typically include isolated unilateral motor impairments, a single acute ischemic stroke with limited co-morbidities, and are specific to the intervention. 4,23 -26 Because these efforts are relatively early in development, little is known about recruitment for brain stimulation trials, 27,28 or about the proportion of clinical stroke patients that could potentially benefit. 29
Although early subacute recovery studies are less affected by some recruitment challenges of the outpatient setting, 30 (eg, transportation, reimbursement, caregiver burden, and community outreach efforts), 31 enrollment criteria is recognized as an important determinant of success of recruitment in both settings. 32,33 Surprisingly, although minority inclusion is an important goal of federally funded research, 34 only about a third of the surveyed prominent stroke researchers reported requiring cultural competency staff training to enhance inclusion of minorities 35 and we found no studies that focus on evaluating the impact of inclusion criteria on participation of women and minorities in noninvasive stimulation studies.
We set out to determine the frequency of stimulation trial candidates in an urban acute stroke population, to evaluate the impact of stimulation-specific exclusion criteria on trial recruitment, and to examine how potential participants differ from the broader stroke population. Using these same data, we also estimate the upper limit of how many stroke patients might qualify for tDCS or TMS, were either found to be useful in UE motor restoration. Lastly, we explored the impact of each exclusion criterion on racial/ethnic/sex groups to improve minority involvement in future research.
Methods
The data that support the findings of this study are available from the corresponding author upon reasonable request. All study procedures were approved by the UTSW Institutional Review Board and a HIPAA waiver was obtained.
Subjects
Patients were evaluated for possible stroke at an academic, urban stroke service UTSW Medical Center, that covers 3 hospitals on the Dallas, TX campus: Parkland Memorial Hospital that provides care primarily for the urban, underserved population, and 2 smaller private University Hospitals. A total of 3124 patients were evaluated and screened for participation in the Eunice Kennedy Shriver National Institute of Child Health and Human Development sponsored study “Transcranial Direct Current Stimulation Enhanced Stroke Recovery and Cortical Reorganization” (Clinical trials.gov identifier: NCT01007136) during 2009–2012. Inclusion criteria were the following: 18–80-years old, an ischemic stroke 5–15 days prior to enrollment with resultant mild to moderate UE weakness (UE Fugl-Meyer scale <60), able to activate their wrist or hand muscles (Medical Research Council Scale [MRC] 1), and able to give informed consent and follow study procedures. Subjects were excluded from participation if they had severe medical or psychiatric illness, recent (within 3 months) substance abuse as determined from history and drug screen, bilateral weakness or prior strokes, or contraindications to stimulation. Stimulation-related safety reasons for exclusion included seizures, pacemaker, cranial surgery or skull defect, skin disease at the stimulation site, metal in the skull, pregnancy, and unstable thyroid disease. Neuromodulatory effects of prescribed and illicit drugs can be a significant confounder. 36,37 We used adaptive randomization to control for the inhibitory or facilitatory effects of medications on neuroplasticity, and when it was feasible we discontinued these drugs. 37 In addition, we excluded illicit drug users to limit the confounding effects of these substances and to improve compliance with study procedures.
Procedures
Research staff was trained in study procedures; they screened the electronic medical records of patients evaluated by the UTSW stroke service. Weekly contacts were made with the UTSW-affiliated inpatient and outpatient rehabilitation services for any eligible stroke patients referred from outside institutions, but no eligible candidates were identified by this mechanism. Once a potential candidate was identified, a research assistant and the principal investigator verified eligibility and obtained informed consent. Study staff received cultural competency education, we addressed patients’ concerns about reimbursement issues (all study-related procedures were free of charge, subjects received a small incentive payment to offset travel expenses for follow-up visits), and whenever possible, patients were approached by a team member from the same racial/ethnic group to improve participation of patients from all racial/ethnic and socioeconomic background. De-identified demographics (age, sex, and self-identified race/ethnic background) and exclusion criteria were recorded for each screened individual in a study log for the study, and those older than age 90 were recorded as 90 *.
Statistical Analysis
Descriptive statistics were used to characterize demographic information. Data are presented as mean ± standard deviation (SD). An association between racial background, eligibility, and enrollment was assessed with Fisher’s exact test. Variation in age between sex and race was assessed with 2-way analysis of variance (ANOVA). P < .05 was considered significant. R statistical software version 3.0.2 (R core team 2013) was used for the calculations.
Results
Demographics
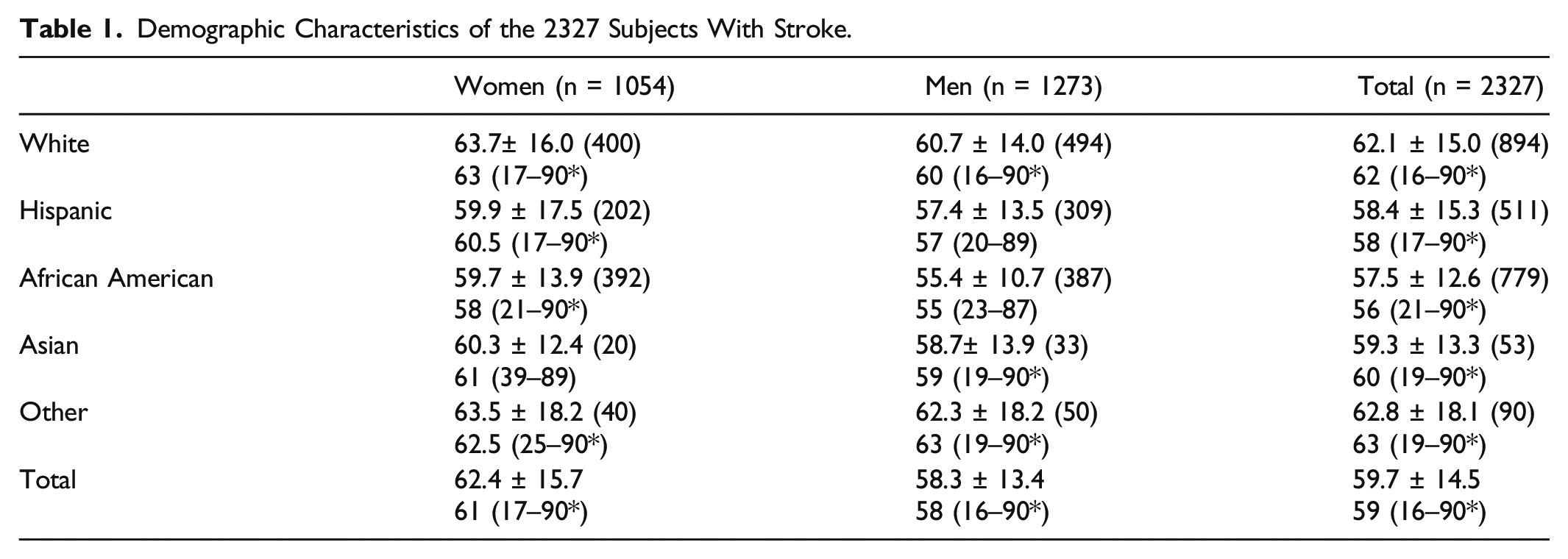
Demographic Characteristics of the 2327 Subjects With Stroke.
Impact of Exclusion Criteria on Study Recruitment
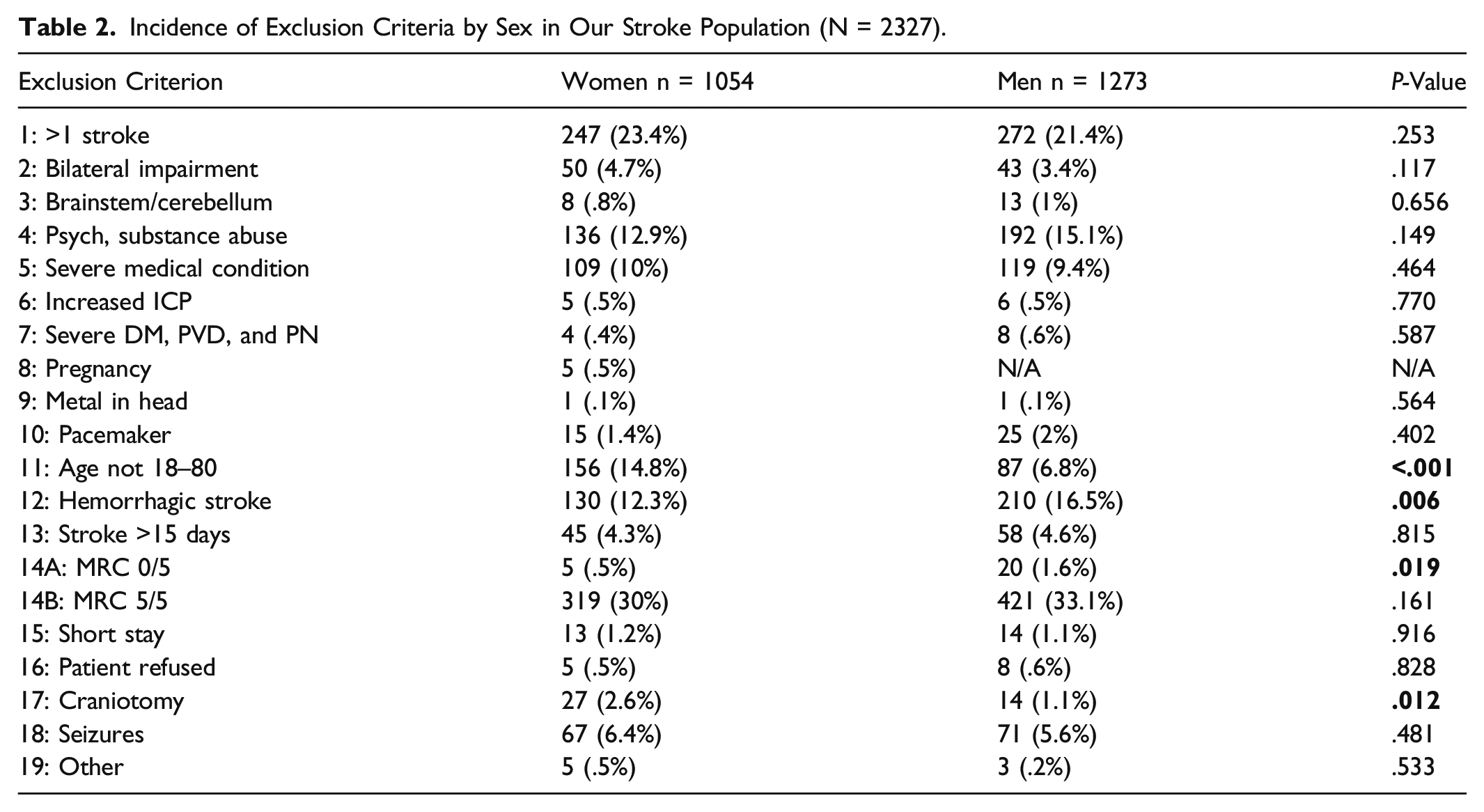
Of the 2327 patients with stroke, only 44 subjects met eligibility criteria (1.9%). The vast majority of patients were not excluded because of safety concerns related to tDCS; rather, they were due to study-specific criteria. The 5 most common causes for exclusion were (in descending order) the following: (1) No suitable UE motor impairment (31.8%), (2) prior strokes (22%), (3) hemorrhagic strokes (15%), (4) psychiatric conditions (active drug abuse and psychosis) or inability to give consent or perform study procedures (severe aphasia or dementia) (14%), and (5) old age (10%). (Of note, if a subject met more than 1 exclusion criteria then each was counted; therefore, the sum of these will be more than 100%.)
Incidence of Exclusion Criteria by Sex in Our Stroke Population (N = 2327).
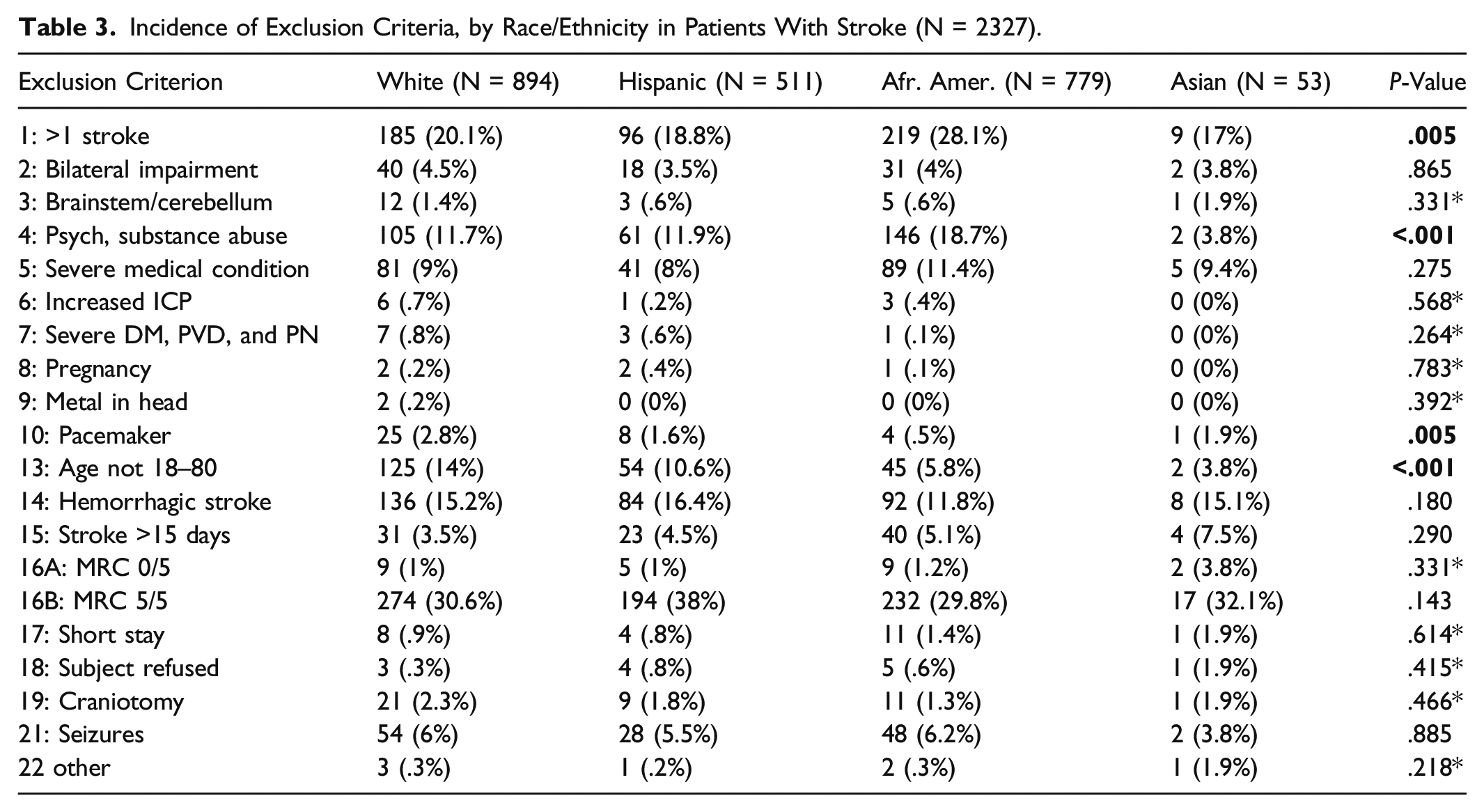
Incidence of Exclusion Criteria, by Race/Ethnicity in Patients With Stroke (N = 2327).
Impact of Stimulation-Specific Exclusion Criteria on the Study Population
Only 3.6% of stroke patients were excluded solely due to stimulation safety. An additional 5.9% met multiple exclusion criteria, including stimulation-related criteria. The majority (90.5%) of stroke patients met safety criteria for the stimulation. Although more W patients had pacemakers, and more women had craniotomies, the overall numbers were low. Other stimulation-specific exclusion criteria occurred equally in the different racial and ethnic groups and between sex groups. Taken together, in our patient population, the maximum possible recruitment of stroke patients for motor impairment studies using methods other than non-invasive stimulation is estimated to be 67% and adding brain stimulation decreases this number only slightly, to 60%.
Enrollment
Enrolled patients were the same age and sex as the UTSW stroke population (61.0 + 11.0 years, 48.4% female), and participation rates of the various racial/ethnic groups did not differ significantly. We observed a trend for lower enrollment of AA patients compared to other racial or ethnic groups (W 1.68%, H 1.37%, AA .77%, A 3.774%, P = .17), but this was not statistically significant. African American patients were more likely to have had prior strokes causing weakness compared to other patients (28.1% vs 19.9%, P < .001), and this was the most common cause of their exclusion if they had an eligible hand weakness.
Refusals
Thirteen individuals refused participation (3 W, 4 H, 5 AA, and 1 A). Non-white groups tended to be more likely to refuse participation than W patients; however, their total numbers were low (P = .073). Refusal was most prominent with AA patients, where 45.5% refused compared to 24.2% of patients of any other racial/ethnic background.
Discussion
In this urban, mixed race, and ethnic population, we found that strokes occurred at a younger age than in previously reported United States population based studies. 38 -40 The patients enrolled in our study were representative of the UTSW stroke service patient demographic.
Enrolled W patients were slightly overrepresented and AA patients were slightly underrepresented compared to the UTSW stroke population, but this difference was not statistically significant due to the low number of enrolled patients. The slightly lower participation of AA patients in the study could be due to a combination of factors, including the multiple strokes experienced by this group and the reluctance on their part to participate in a research protocol. The finding of increased psychiatric disease burden, including substance abuse, in AA patients compared to other racial and ethnic groups requires further study and targeted intervention. Public health efforts targeting psychiatric disease including substance abuse and access to affordable preventive care options to mitigate the effects of stroke risk factors such as diabetes or hypertension to lessen disease burden could help increase AA participation. If our results are generalizable, future studies will have to adjust for the lower eligibility of AA subjects perhaps by allowing the enrollment of patients with previous non-motor strokes, and have plans in place to encourage their participation. Interestingly, we found that other minority groups, such as H and A patients, were recruited at a similar rate as W subjects.
Increasing the age limit of enrollment may increase participation in the study, in particular of W patients and of women, as these groups presented at a later age with stroke. Brain plasticity is diminishing with advancing age 41,42 ; however, evidence for life-long neuroplasticity is mounting, 43,44 suggesting that older patients might also benefit from an effective non-invasive stimulation. Enrolling patients with hemorrhagic strokes and severe UE weakness could preferentially enhance the participation of men. In our study, hemorrhagic strokes were excluded because of their different pathology and early recovery patterns; however, many of these subjects could be safely included in future larger studies. 29 For example, deep hemorrhagic strokes at the thalamus/internal capsule carry minimal risk for seizures, and might behave similarly in the post-edema phase as ischemic lesions in the same location. The somewhat higher risk of seizures in patients with cortical hemorrhages will have to be balanced against the potential benefit of brain stimulation.
Enrollment in this stimulation trial (1.9%) was similar to other early stroke recovery trials in acute hospital setting, where the recruitment rate was 3–4%. 24,45,46 Most stroke patients (90.5%) were eligible for stimulation in this urban sample, supporting the wider applicability of brain stimulation methodology once well-designed, sham controlled, blinded studies confirm it to be an effective treatment. The impact of stimulation-related exclusion criteria on recruitment was minor (3.6%), as most of the subjects that met safety exclusion criteria for stimulation met additional exclusion factors (5.9%).
Additional subgroups of patients with multiple strokes or certain co-morbidities may also benefit from such interventions if they can be safely stimulated. Prior “clinically silent” strokes or symptomatic strokes involving non-motor regions (such as temporal or occipital lobe) identified by admission notes and imaging may be considered. Although expensive, brain mapping for careful planning of electrode placement might further expand the applicability to the most complex patients with multiple prior strokes. Involvement of these more complex patients in the initial, stringent, proof-of-concept studies is impractical, but if pilot studies have promising results, complex patients should be included in subsequent studies.
Limitations of the study include that although medical personnel was instructed to ask patients about their self-identified racial/ethnic identity, it is possible that in some cases racial/ethnic background was recorded based on medical personnel assumption, when we worked with medical records collected by non-research personnel. It is also possible that despite our efforts to record all exclusion criteria in each subject during screening, we could have missed some of those that were not recorded in the first notes. Generalizability of our findings to chronic stroke recovery studies requires caution as the percentage of excluded patients may reflect the subacute setting, for example, the degree of motor impairment. Lastly, in our study we did not record the availability or lack of third party reimbursement to address co-morbidities; therefore, the role of this important factor in inequalities needs further study.
Conclusions
Safety concerns did not represent a significant recruitment limitation. Results inform appropriate estimation of sex and racial/ethnic group participation in future stroke recovery studies. Given slow recruitment in neurorehabilitation in general, this planning is crucial to avoid poor or unrealistic trial designs. Consideration of the impact of relaxation of different exclusion criteria on recruitment could further increase participation across racial/ethnic groups. Tailoring recruitment efforts to disadvantaged racial and ethnic communities could enhance participation in neurorehabilitation trials.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health (grant no. 5K23HD050267) and University of Texas Southwestern Department of Neurology.