
Abstract
Background. Tinnitus is the phantom perception of sound and can have negative effect on the quality of life. Transcranial direct current stimulation (tDCS) is a noninvasive neuromodulation technique, which can increase or decrease the cortical excitability in the brain region to which it is applied. tDCS has been used for tinnitus research since 2006. Objective. To investigate whether tDCS affects tinnitus perception, related emotion, or both, and the potential implications for tinnitus management. Methods. A scoping review was undertaken using the methods proposed by Arksey and O’Malley. After initial consideration of title relevance and reading abstracts, 15 studies were included in this review. The data from these studies were charted to investigate the impact of tDCS on tinnitus perception and emotions. Results. tDCS results in transient suppression of tinnitus loudness and annoyance; however, it does not lead to long-term impact on tinnitus related emotion. Local stimulation of different sites of stimulation (left temporoparietal area, dorsolateral prefrontal cortex, and auditory cortex) might modulate tinnitus perception (loudness) and emotions differently; however, further research is needed to explore this hypothesis. This review has identified aspects of methodologies that require attention in upcoming tinnitus and tDCS trials to offer better insights. Conclusions. tDCS is an effective research tool for transient tinnitus neuromodulation. However, efforts should be invested in designing clinical trials using local and multiple sites of stimulation, optimized parameters, and objective outcome measures before it can be translated in to a clinical tool for tinnitus management.
Introduction
Tinnitus is the perception of a phantom sound 1 often associated with emotional symptoms. Tinnitus perception is comprised of the psychophysical properties of pitch, loudness, and location. Tinnitus sounds do not appear extreme, such that they should be unbearable 2 ; although normally matched to sounds lower than 20 dB sensation level, it can have negative emotional consequences. 3
The emotional consequences of tinnitus sound perception can be low-mood, annoyance, anger, anxiety, depression, reduced attention, and poor sleep.4-8 Catastrophic effects on the overall quality of life occur in approximately 5% of the tinnitus population.4-8 Sanchez and Stephens 9 identified 5 major categories of problem among people with tinnitus: psychological (30.1%), hearing difficulties (23.5%), health (20.7%), sleep (14.6%), and situational difficulties (11.1%).
Tinnitus has been hypothesized to be the weighted mean of 3 external and internal components: the tinnitus signal, background sound, and residuals; the sum of factors such as past experience (ie, memory), physiological state (arousal), and personality. 10 The tinnitus signal may arise from compensatory mechanisms following sensory deafferentation, with cochlear hair cell loss resulting in reduced spontaneous firing rate of the auditory nerve fibers. 11 Reduction in afferent activity may lead to hyperactivity in the auditory cortex through reductions in cortical inhibition.12,13 Emotion and other residuals have been linked to the various cortical and subcortical networks of the brain. The major networks proposed to be involved in the perception of tinnitus are: a perception network (prefrontal cortex, parietal cortex, precuneus, posterior cingulate cortex, subgenual, and dorsal anterior cingulate cortex), salience network (dorsal anterior cingulate cortex and anterior insula), distress network (anterior cingulate cortex, anterior insula and amygdala), and memory network (parahippocampal area, amygdala, and hippocampus).14,15 The majority of research is consistent with increased connection between auditory cortex, attention, memory, and limbic systems in tinnitus patients using functional magnetic resonance imaging (fMRI).16-19
Neuromodulation techniques can be divided into 2 categories: noninvasive (neurofeedback, transcranial magnetic stimulation [TMS], transcutaneous electrical nerve stimulation [TENS], transcutaneous vagus nerve stimulation [TVNS], and transcranial direct current stimulation [tDCS]) and invasive neuromodulation involving epidural stimulation or electrode implants to stimulate the auditory cortex, dorsolateral prefrontal cortex (DLPFC), subcutaneous occipital nerve stimulation, and deep brain stimulation). The scope of this review is limited to investigating the impact of tDCS on the perception and emotions associated with tinnitus.
Depending on the polarity of the stimulation, tDCS can increase or decrease the cortical excitability in the brain region to which it is applied. Anodal stimulation leads to an excitatory effect due to neuronal depolarization and cathodal stimulation leads to inhibitory effect on the cerebral cortex due to neuronal hyperpolarisation.20-22 tDCS has the ability to influence the resting membrane potential, but without inducing action potentials as is the case in TMS.23,24 The current intensity, duration, and location of electrodes are important parameters in determining the impact of tDCS.20,23 tDCS has been applied safely without any significant adverse effect to more than 3000 individuals.22,23,25 However, it is common to observe mild tingling and light itching sensations under the electrodes, during the stimulation.24,26 These sensations are mostly transient and can be induced during sham stimulation by few seconds of stimulation, making tDCS effective for sham-controlled trials. 25
Understanding of the neurophysiological basis of tDCS is limited. The aftereffects of anodal tDCS can be explained based on effects during and after stimulation. During stimulation, anodal tDCS leads to depolarisation of the resting membrane potentials in neurons. There is no change in the synaptic strength during stimulation.
27
After stimulation, there are 3 possible mechanisms for associated effects: activation of NMDA receptors (N-methyl-
The aim of this scoping review was to investigate whether tDCS affects the tinnitus perception, emotion, or both, and the potential implications for tinnitus management.
Methods
A scoping review
34
was undertaken using the methods proposed by Arksey and O’Malley.
35
According to Mays et al
36
scoping reviews: aim to map rapidly the key concepts underpinning a research area and the main sources and types of evidence available, and can be undertaken as standalone projects in their own right, especially where an area is complex or has not been reviewed comprehensively before.36(p194)
The 4 reasons for which a scoping review might be undertaken are
to examine the extent, range, and nature of research activity
to determine the value of undertaking a full systematic review
to summarize and disseminate research findings
to identify research gaps in the existing literature.35(p21)
The following databases (Scopus, Google Scholar, Springer link, and PubMed) were searched with the combination of following key words “tinnitus,” “tDCS,” “tinnitus intervention,” and “neuromodulation.” Studies published before August 1, 2014, were included in this review. After initial consideration of title relevance to the present review 24 articles were shortlisted and after reading the abstracts, 15 studies were included (9 studies were excluded as they were not investigating tinnitus). The data from these studies were charted to investigate the impact of tDCS on tinnitus perception and emotions.
Studies were divided into 3 groups: group 1—assessing the impact of tDCS on tinnitus perception (5 studies), group 2—assessing the impact of tDCS on both tinnitus perception and related emotion (10 studies), and group 3—assessing the long-term impact of tDCS on tinnitus related emotion (4 studies). The 4 studies investigating the long-term impact of tDCS on tinnitus related emotions (group 3) overlapped with group 1 (2 studies) and group 2 (2 studies). Group 1 and group 2 investigated the immediate impact of tDCS on tinnitus perception and emotion; however, group 3 looked at the long-term impact of tDCS on tinnitus emotions (follow-up ranging from 2 weeks to 6 months). ‘Tinnitus perception” refers to tinnitus loudness and “emotions” refers to annoyance and distress associated with tinnitus.
Results
The first published evidence of tinnitus suppression by tDCS came in 2006 by Fregni et al. 37 It took 4 years for the second publication to arrive in 2010 and every year since then 3 studies have been published, illustrating an increase in interest in tDCS for tinnitus. All the published studies37-46 have supported small degrees of transient tinnitus suppression with tDCS, except Vanneste et al. 47 The criterion used for “tinnitus suppression” across all the studies included in this scoping review was either a minimum of 1 point or any reduction in the tinnitus loudness and annoyance rating. Charted data of these studies are presented in Table 1.
Transcranial Direct Current Stimulation (tDCS) and Tinnitus Studies Done in the Past Looking at the Impact of Direct Current Stimulation on Tinnitus Perception or Emotions. a
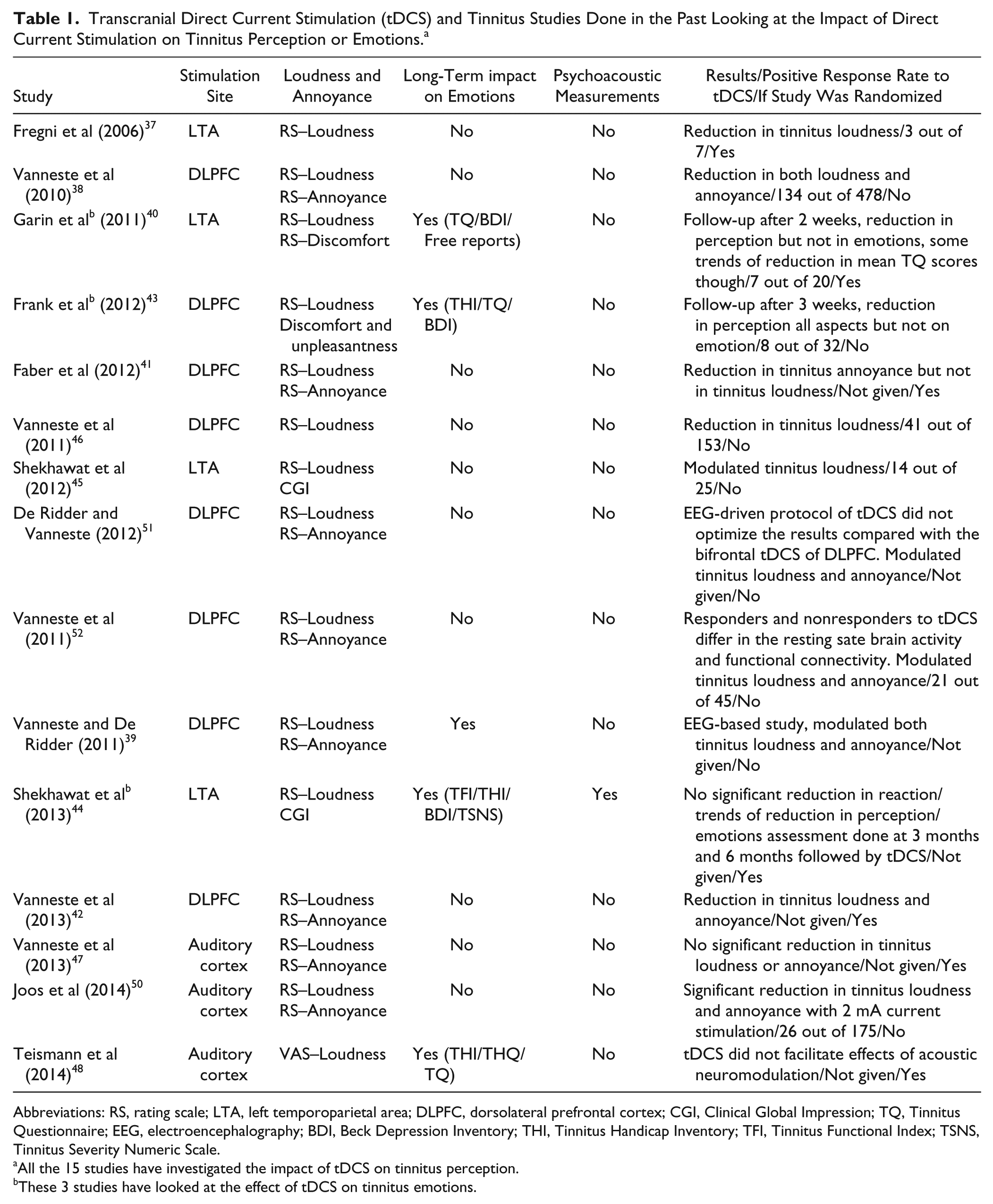
Abbreviations: RS, rating scale; LTA, left temporoparietal area; DLPFC, dorsolateral prefrontal cortex; CGI, Clinical Global Impression; TQ, Tinnitus Questionnaire; EEG, electroencephalography; BDI, Beck Depression Inventory; THI, Tinnitus Handicap Inventory; TFI, Tinnitus Functional Index; TSNS, Tinnitus Severity Numeric Scale.
All the 15 studies have investigated the impact of tDCS on tinnitus perception.
These 3 studies have looked at the effect of tDCS on tinnitus emotions.
All the studies presented in Table 1 have used numeric rating scales of various types for assessing tinnitus perception (intensity) and/or emotions (handicap/severity) (groups 1 and 3). Only 3 studies40,43,44 used questionnaires to assess the long-term impact on tinnitus emotions (group 2), 2 weeks to 6 months after administering tDCS. None of these studies used matching comparisons to external sounds. The 15 studies included in this scoping review have used both within- and between-subject design.
Transcranial direct current stimulation parameters and protocol details of all the studies included in the present review are documented in Table 2.
Transcranial Direct Current Stimulation (tDCS) Parameters and Methodological Details of Research Studies Included in This Scoping Review.
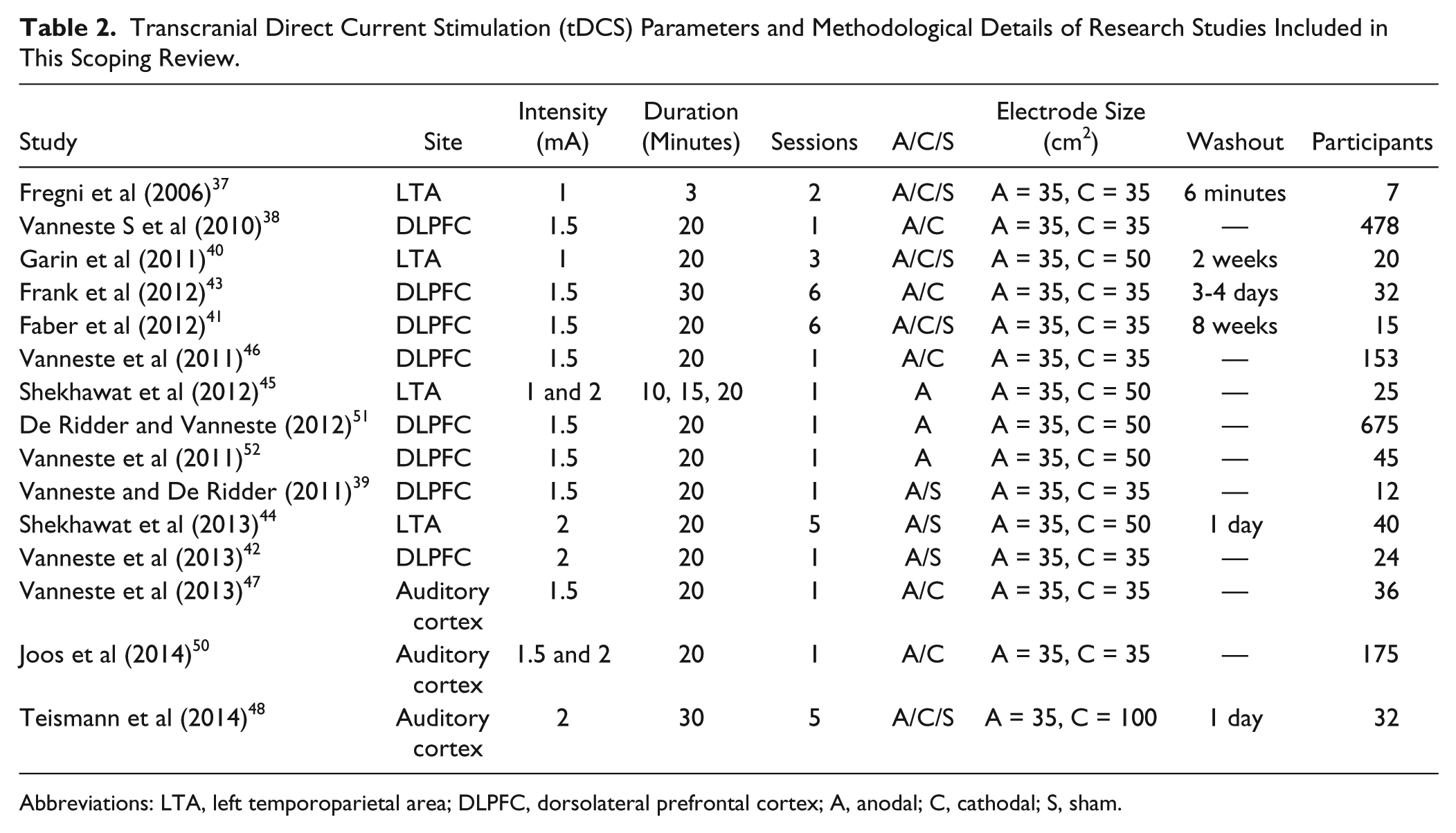
Abbreviations: LTA, left temporoparietal area; DLPFC, dorsolateral prefrontal cortex; A, anodal; C, cathodal; S, sham.
Group 1: Immediate Impact of tDCS on Tinnitus Perception
Five studies37,44-46,48 looked at the immediate impact of tDCS on tinnitus perception (loudness) using rating scales. All these studies documented the effectiveness of tDCS in transient tinnitus suppression lasting from a few minutes to up to a day. The study by Shekhawat et al 44 and Teismann et al 48 also investigated the long-term impact of tDCS on tinnitus-related emotions using questionnaires and will be presented under group 2. The summary of the other 3 studies is presented next.
Fregni et al 37 studied 7 patients with chronic tinnitus who underwent anodal, cathodal, and sham tDCS of left temporoparietal area (LTA) with a 6-minute interval between sessions. Three participants (42%) experienced transient tinnitus suppression following anodal tDCS of LTA. There were no positive responders after cathodal and sham tDCS. Responders had less hearing loss compared with nonresponders. Fregni et al 37 hypothesized that a higher degree of hearing loss was associated with more profound plastic changes and may require higher intensity and duration stimulation for noticeable tinnitus relief. Vanneste et al 46 conducted a retrospective study investigating the mechanism of effect of tDCS compared with TMS and TENS. A positive response rate (reduction in tinnitus loudness) of 27% was found with tDCS. This study revealed that responsiveness of 1 neuromodulation technique can be predicted by others (tDCS predicts TMS and vice versa, TENS predicts the response of tDCS and TMS) and the mechanism of effect of tDCS appears to be dual (directly modulating the auditory and DLPFC area and indirectly influencing the somatosensory pathway as used by TENS via cervical nerve–cochlear nucleus interaction 49 ). Shekhawat et al 45 conducted a dose-response optimization trial for tDCS and found that 56% participants (n = 14) experienced transient tinnitus suppression. This study revealed that it was the 2 mA current intensity and 20 minutes’ duration that was most effective stimulus combination for tinnitus suppression. This study was the first attempt to optimize current intensity and duration for tinnitus suppression, however the study design was not sham controlled and it was not possible to rule out the cumulative impact of stimulation intensity due to a short washout period of 10 minutes between stimulations.
Group 2: Impact of tDCS on Both Tinnitus Perception and Related Emotion
Ten studies38-43,47,50-52 have investigated the combined impact of tDCS on both tinnitus perception and emotion using rating scales. One study conducted by Vanneste et al 47 showed that tDCS did not modulate tinnitus loudness or annoyance. The rest of the studies38-43,50-52 supported the effectiveness of tDCS in transient tinnitus reductions of related annoyance and/or loudness. Faber et al 41 proposed tDCS of the DLPFC modulated tinnitus annoyance but had no impact on tinnitus loudness. However, the hypothesis of difference in loudness and annoyance has been contradicted by other studies.39,42,51,52
Vanneste et al 38 found a significant reduction in tinnitus intensity and distress for 29.9% (n = 134) of patients with anode on right and cathode on left DLPFC. The amount of improvement was unrelated to factors such as age, gender, tinnitus type, tinnitus laterality, and duration of tinnitus. Faber et al 41 proposed that bifrontal tDCS may modulate tinnitus distress but not necessarily tinnitus loudness. Irrespective of anodal position, tDCS lead to a reduction in tinnitus annoyance but no change was observed in tinnitus loudness as measured with rating scales. Recently, Vanneste et al 42 compared tDCS of DLPFC with transcranial alternating current stimulation (tACS) of DLPFC. They found tACS to have no effect on tinnitus loudness or annoyance, unlike tDCS of DLPFC, which led to suppression of tinnitus annoyance, as well as loudness; contrary to the findings of Faber et al. 41 In a head-to-head comparison of 3 neuromodulation techniques: tDCS, tACS, and transcranial random noise stimulation (tRNS), Vanneste et al 47 demonstrated the effectiveness of tRNS in suppressing tinnitus loudness and annoyance; the use of tDCS and tACS did not lead to any significant effects. Vanneste and De Ridder 39 investigated the underlying mechanisms behind bifrontal tDCS in a sham-controlled study. Significant suppression of tinnitus perception (41.67%) and tinnitus-related distress (43.20%) was observed after real tDCS and no significant effects were seen for the sham condition. Electroencephalographic (EEG) analysis revealed a significant increase of alpha 1 activity in the pregenual anterior cingulate cortex, a significant decrease of activity for beta 3 and gamma in the right primary auditory cortex and inferior primary somatosensory cortex post tDCS as compared to pre tDCS. However, no such changes were seen after the sham tDCS. This study provides some evidence that bifrontal tDCS not only modulates the area under DLPFC but also indirectly affects the functionally connected brain areas related to perception of tinnitus and its distress. However, EEG-driven tDCS did not improve the tDCS protocol for tinnitus modulation. 51 Further work conducted by Vanneste et al 52 has shown that responders to tDCS differ from nonresponders in their resting-state brain activity and functional connectivity.
Group 3: Long-Term Impact of tDCS on Tinnitus-Related Emotion
Four studies40,43,44,48 investigated the long-term impact of tDCS on tinnitus-related emotions using questionnaires. All the studies overlapped with group 144,48 and group 2.40,43 None of the studies showed that tDCS was effective in modulating long-term tinnitus-related negative emotions. However, all the studies documented the reduction in tinnitus loudness and/or annoyance immediately after tDCS on rating scales. Garin et al 40 did not find any significant reduction in tinnitus emotion (handicap/severity) scores measured by the Tinnitus Questionnaire (TQ) and Beck Depression Inventory (BDI); however, some patients reported tinnitus loudness suppression lasting for up to 15 days. Garin et al 40 suggested the need for the optimization of tDCS parameters for tinnitus relief. Frank et al 43 found scores on the Tinnitus Handicap Inventory (THI), TQ, and BDI remained unchanged 3 weeks after stimulation; however, positive results were seen in numeric rating scores for tinnitus loudness, discomfort, and unpleasantness. This was one of the first studies to report the effect of gender on the treatment response. Women reported more positive results than men on the THI. Shekhawat et al 44 investigated whether priming the LTA with multisession tDCS would enhance the benefits of hearing aids for tinnitus management and observed significant reductions in the tinnitus handicap after 3 and 6 months of hearing aid use; however, the benefits of hearing aids were independent of the tDCS. Although there was some preliminary evidence supporting the effectiveness of tDCS on transient tinnitus loudness suppression and change in minimum masking levels at 3-month follow-up, tDCS on its own did not lead to any significant change in tinnitus-related handicap. Teismann et al 48 investigated whether tDCS could modulate the efficacy of tailor-made notched music training (TMNMT) for tinnitus management. TMNMT resulted in a significant reduction of Tinnitus Handicap Questionnaire (THQ) scores after 5 days of treatment and the treatment effect lasted for 31 days following treatment. tDCS on its own did not facilitate the efficacy of TMNMT, thus Teismann et al 48 and Shekhawat et al 44 failed to find that tDCS augmented sound-based therapy.
Discussion
Transcranial direct current stimulation results in transient suppression of tinnitus loudness and annoyance; however, it does not lead to long-term impact on tinnitus-related emotion. All the 15 studies reviewed37-48,50-52 explored the effect of tDCS on tinnitus perception and 14 of them37-46,48,50-52 using rating scales showed that tDCS resulted in transient loudness suppression. A possible reason for temporary suppression of loudness perception could be due to the reduction of abnormal hyperactivity in the cortex via inhibitory networks and competition due to the stimulation of various cortical and subcortical regions underlying different sites of stimulation (LTA, DLPFC, and auditory cortex).37,45 Vanneste et al 47 undertook the only study that tDCS did not result in tinnitus modulation; however, Joos et al 50 could modulate the tinnitus loudness and annoyance using slightly higher current intensity (2 mA) than Vanneste et al 47 stimulating the auditory cortex. It is possible that the 1.5 mA current intensity used by Vanneste et al 47 was insufficient to stimulate the neural networks responsible for tinnitus. Further optimization of tDCS parameters for tinnitus loudness suppression via auditory cortex stimulation is recommended.
Four studies40,43,44,48 out of 15 have made an attempt to investigate the long-term effect of tDCS on tinnitus emotions (handicap/severity) using questionnaires (TQ, BDI, THI, THQ, Tinnitus Functional Index [TFI], and Tinnitus Severity Numeric Scale [TSNS]). All these studies documented that tDCS provided transient tinnitus modulation (loudness and emotion) immediately after tDCS. However, none of these studies showed tDCS to be effective in long-term reduction of tinnitus related emotions (handicap/severity). A potential reason for not having a long-term impact on emotions includes the possibility of tDCS modulation (duration and intensity) being insufficient to influence the long-term emotions associated with tinnitus. 40 It is also difficult to rule out the possibility of the suitability and sensitivity of the questionnaires used to measure the long-term impact of tDCS on emotions.
Song et al 53 conducted a systematic review (6 studies) and meta-analysis (2 studies) investigating the impact of tDCS in tinnitus patients. According to this review, LTA and DLPFC stimulation revealed comparable results and tDCS appeared to be a promising tool for tinnitus management; however, they could not confirm the efficacy of tDCS due to the small number of studies. Our scoping review supports and extends the findings of Song et al. 53 We have identified aspects of tDCS tinnitus treatment methodologies that require further attention, including use of psychoacoustic tinnitus assessment, electrophysio-logical assessment, evaluating different sites of stimulation, larger sample sizes, standardized criteria for positive response, evaluation of differential impact on tinnitus loudness/emotions, polarity of stimulation, placement of the reference electrode, and candidacy for tDCS.
Psychoacoustic measurement of tinnitus (tinnitus pitch, loudness, minimum masking level—the minimum level of sound needed to mask or cover the tinnitus) forms an integral part of a comprehensive tinnitus assessment battery and can provide useful information about tinnitus management. 54 The study conducted by Shekhawat et al 44 was the only study that included psychoacoustic assessment (pitch, loudness, minimum masking level, refer Shekhawat et al 44 for the details on psychoacoustic measurements and their assessment). All the studies included in this review used rating scales. The limitation of rating scales is the difficulty in quantifying what respondents are actually reporting, as loudness may be interpreted in different ways (Tinnitus Magnitude Index 55 ). Tinnitus Magnitude Index represents a single domain that includes tinnitus loudness, participant’s reports of severity of tinnitus, and percent of time aware of tinnitus. 55 According to adaptation level theory, magnitude ratings may be strongly influenced by emotion and residuals, meaning intensity matches and loudness ratings are very different constructs. 10 Psychoacoustical measurements pre and post tDCS may be a more objective means of determining the influence of tDCS on a loudness match, but these suffer from poor reliability. 56 Both psychoacoustical matching and loudness ratings may be needed to appropriately measure tinnitus.
The effects of tDCS on electrophysiological measures were explored in only 3 studies39,51,52 out of 15 undertaken thus far. Responders to tDCS tend to have higher gamma band activity in the right primary auditory cortex, secondary auditory cortex, and right parahippocampus compared with nonresponders in their resting-state brain activity, and increased functional connectivity between right DLPFC and right parahippocampus/subgenual anterior cingulate cortex. 52 All these studies were limited to DLPFC as the site of tDCS stimulation. It is strongly recommended to include electrophysiological measures such as EEG or other objective measures such as fMRI to assess the impact of tDCS on tinnitus. Such measurements would provide greater insight into the physiological changes resulting from tDCS.
We are limited in our knowledge regarding the exact distribution of electric field and current density over the various cortical and subcortical areas. 57 Heschl’s gyrus, which is buried in the Sylvian fissure, has an oblique course and plays an important role in pitch discrimination. 58 None of the studies included in this review have attempted to explore the impact of Heschl’s gyrus stimulation on tinnitus modulation. All the studies included in this scoping review have limited themselves to one site of stimulation (LTA [defined as half way between C3/T5], DLPFC [F3 or F4], or auditory cortex [either C3 or C4]). Considering the big size of electrodes (35-50 cm2) there may not be a little difference between LTA and auditory cortex. None of them have attempted to explore multiple sites of stimulation and their impact on tinnitus perception and emotion. Our understanding of tinnitus has evolved tremendously in the past 2 decades from it being a problem of the auditory periphery, to a complex dynamic, network of brain areas. 14 It may be more appropriate to target multiple sites to modulate the perception and/or emotions associated with tinnitus. We need to ascertain the best sites for stimulation and the specific and cumulative impact of tDCS on tinnitus perception and emotion.
The majority of the studies undertaken in tinnitus and tDCS have used small sample sizes (11 studies37,39-48,52 used n = 7-45) and 4 studies38,46,50,51 used sample size ranging from 153 to 675 participants. The studies using large sample size were not strong in their research design (they were not sham controlled, and used retrospective analysis of the data). More double blind, sham controlled, randomized clinical trials with larger sample size are needed.
Tinnitus characteristics such as quality of tinnitus (tonal, narrow band noise, etc), duration, severity, and laterality require further attention while planning tDCS trials. Some of the studies39,45,48,51,52 included in this scoping review have provided details about the tinnitus quality; however, publications investigating the relationship between tinnitus characteristics and responsiveness to neuromodulation are still awaited.
The positive response rate of participants toward tDCS has been defined differently by researchers. A minimum 1 point reduction on rating scales has been used by some researchers37,40,44,45 and others defined it as any reduction on rating scales.38,39,42,47,50-52 This small and transient reduction may not have an immediate clinical implication for tinnitus management. Hence tDCS is still a research tool and further investigation is needed to explore ways to convert the transient relief into long-lasting, sustainable benefits which may have clinical significance to the process of tinnitus management. The reported responsiveness toward tDCS has also varied among studies (ranging from 29.9% to 56%) and this difference could be attributed toward the different response criteria, research design, protocol, washout period, stimulation parameters, and potentially in many studies placebo effect. Gender may also have an effect. Frank et al 43 reported gender differences in the responsiveness toward tDCS. Females reported more positive results than males on the THI. The reason proposed for this was the difference between males and females in the neural activity of orbitofrontal and anterior cingulate cortex 59 and neural responses 60 during emotional processing.
Polarity of stimulation, size, and placement of the reference electrode requires further attention. It is impossible to rule out the stimulation of areas underlying the reference electrodes. 61 None of the studies included in this scoping review have attempted to investigate the impact of reference electrode size and placement on tinnitus modulation.
There is preliminary evidence that tDCS of DLPFC modulated annoyance and not loudness 41 and LTA might modulate loudness but not tinnitus annoyance.53,56 However, this view was challenged by Vanneste et al.38,42,50-52 It is probably too early to reject or accept the possibility of neuromodulation of different areas. It will not be surprising if different sites of stimulation might modulated tinnitus loudness and emotions in slightly different manner and such results would support network models such as that proposed by De Ridder et al. 14 However, tDCS uses large rubber electrodes (35-50 cm2) and research by Parazzini et al 57 has shown that the distribution of electric field and current density is not only limited to target site of stimulation but also reaches other adjoining cortical and subcortical areas making tDCS a relatively nonfocal neuromodulation technique. Modulation of tinnitus intensity and annoyance may occur irrespective of the site of stimulation (LTA or DLPFC). Further research is needed using relatively more local stimulation techniques such as high-definition tDCS (HD-tDCS)62-64 to investigate if different site of stimulation can modulate tinnitus intensity and emotions differently.
The network model proposed by De Ridder et al 14 is a plausible model proposing the involvement of several parallel, simultaneously overlapping networks (a perception network, salience network, distress network, and memory network) leading to tinnitus perception. It may be useful to conduct clinical trials investigating independent and focal stimulation of these networks and its impact on tinnitus using HD-tDCS. Further research in this direction would be helpful in understanding the physiological basis of neuromodulation for tinnitus suppression.
Future Direction of tDCS and Tinnitus Research
There has been an increased interest in the use of tDCS for tinnitus research; however, tDCS has yet to be proven to be a standalone clinical treatment. Research needs to be undertaken to investigate ways to prolong the current transient aftereffects of tDCS. New techniques such as HD-tDCS and tRNS may offer advantages. HD-tDCS has been proposed to be more local stimulation and have longer lasting after effects compared with tDCS 62 and a comparison between the effectiveness of tDCS, tACS, and tRNS has shown the superiority of tRNS compared with tDCS and tACS in transient tinnitus suppression. 47 Adding the random noise through tRNS possibly disrupts ongoing hypersynchronization in the auditory cortex due to tinnitus, resulting in transient relief. 47 However it is possible that even optimized electrical neuromodulation will only ever provide transient suppression. If so tDCS (and similar) techniques utility may be in diagnosis than treatment, or alternatively it may need to be combined with another treatment as a “primer” of neuroplasticity. 44
There has been preliminary evidence based on animal studies that different genotypes may respond differently toward neuromodulation. 65 Vanneste et al 52 documented that responders to tDCS differed from nonresponders in the resting-state brain activity and functional connectivity. There is some early research speculating roles for brain-derived neurotrophic factor (BDNF) gene in tinnitus-related plasticity changes. 66 A nucleotide polymorphism (BDNF Val66Met) is linked with differences in hippocampal volume and memory 67 and tinnitus has been linked with altered structural volume as well. 68 Identifying biomarkers or endophenotypes that predict the responsiveness toward neuromodulation may be possible in future research and identify those individuals likely to be successful candidates for tDCS.69,70
Conclusions
Transcranial direct current stimulation is effective in transient modulation of tinnitus loudness or annoyance, but it does not lead to any long-term change in emotions associated with tinnitus. Local stimulation of different sites of stimulation (LTA, DLPFC, and auditory cortex) might modulate tinnitus loudness and emotions differently; however, further research is needed to explore this hypothesis. tDCS appears to be a promising technique for tinnitus modulation; however, we are yet to completely understand the underlying mechanisms of tDCS and efforts should be invested in addressing this by designing future clinical trials using local multiple sites of stimulation, optimized parameters, and objective outcome measures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.