
Abstract
Background. Stroke is one of the most common causes of physical disability worldwide. The majority of survivors experience impairment of movement, often with lasting deficits affecting hand dexterity. To date, conventional rehabilitation primarily focuses on training compensatory maneuvers emphasizing goal completion rather than targeting reduction of motor impairment. Objective. We aim to determine whether finger dexterity impairment can be reduced in chronic stroke when training on a task focused on moving fingers against abnormal synergies without allowing for compensatory maneuvers. Methods. We recruited 18 chronic stroke patients with significant hand motor impairment. First, participants underwent baseline assessments of hand function, impairment, and finger individuation. Then, participants trained for 5 consecutive days, 3 to 4 h/d, on a multifinger piano-chord-like task that cannot be performed by compensatory actions of other body parts (e.g., arm). Participants had to learn to simultaneously coordinate and synchronize multiple fingers to break unwanted flexor synergies. To test generalization, we assessed performance in trained and nontrained chords and clinical measures in both the paretic and the nonparetic hands. To evaluate retention, we repeated the assessments 1 day, 1 week, and 6 months post-training. Results. Our results showed that finger impairment assessed by the individuation task was reduced after training. The reduction of impairment was accompanied by improvements in clinical hand function, including precision pinch. Notably, the effects were maintained for 6 months following training. Conclusion. Our findings provide preliminary evidence that chronic stroke patient can reduce hand impairment when training against abnormal flexor synergies, a change that was associated with meaningful clinical benefits.
Introduction
Stroke is one of the leading causes of death and disability globally,1,2 resulting in a wide range of physical, emotional, and cognitive consequences. 3 Among the most common physical sequela of stroke are hemiparesis and spasticity, two forms of motor impairment that affect daily living and overall quality of life in approximately 80% of survivors. 3 Hand impairment, in particular, is often present in the chronic stage after stroke, frequently manifesting itself as both a decrease in finger strength, loss of dexterity (negative signs), and abnormal hand flexion synergy, characterized by a pattern of involuntary motor activation resulting in finger and hand flexion (positive signs).4,5 Indeed, one of the most prominent deficits in hand dexterity is increased finger enslaving, or unintended force produced by the uninstructed fingers. This hand function abnormality is thought to be a direct result of lesions to the motor cortex and corticospinal tract,5,6,7,8,9 as these are known to be critical for the control of independent finger movements (i.e., finger individuation).5,10-13
Previously, we have shown that stroke patients recover both finger individuation and strength relying on separable recovery processes. 5 Recovery asymptotes after the first 3 to 6 months, although typically remains far from the level of performance of healthy individuals, especially for the individuation component. Over the past few years, different training and rehabilitation strategies have assessed the effect of finger and hand training as well as virtual reality environments in chronic stroke patients in an attempt to improve deficits in dexterous movement.14-20 Some of these works reported positive gains in clinical measures of hand dexterity. However, these studies cannot distinguish between compensatory maneuvers versus true impairment reduction as the mechanism underlying clinical benefits. Specifically, these studies did not fully assess force control in the finger individuation tasks,14,18-20 used gross measures of hand dexterity and did not report a detailed individuation metric,14,16 and/or did not report post-training long-term retention of clinical outcomes or retention of improvement in finger individuation.14,18,20 In the present study, we use a direct and quantitative measure of finger dexterity 5 .
The goal of this study was to discern whether true hand motor impairment can be reduced in the chronic phase after stroke following personalized multidimensional training targeting finger dexterity that minimizes the use of compensatory maneuvers to facilitate performance. To this end, we modified a previously published piano-chord-like task13,21 to train finger dexterity by asking participants to practice in an intense manner against their baseline flexion synergy. Task difficulty during practice was adjusted for each participant based on baseline ability, controlling for individual differences in initial weakness and performance. Participants cannot perform this task by recruiting actions beyond their fingers. We tested both the short- and long-term retention of trained and nontrained hand-chord postures. We quantified hand dexterity by measuring finger individuation and also gauged the impact of the training on clinical outcome measures of impairment, activity, and participation. We hypothesized that intensive training focused on moving fingers against abnormal synergies while minimizing compensatory movements, would improve the ability of patients with chronic stroke to individuate their fingers and perform functional tasks better.
Materials and Methods
Participants
We recruited a cohort of eighteen participants with ischemic stroke and hemiparesis (5 female, 13 male; age 61.3 ± 2.1 years, mean ± SEM). We administered multiple screening assessments during the pretest session to determine participant eligibility. We included participants if they met the following inclusion criteria: (1) age 21 years and older; (2) ischemic stroke at least 6 months prior (time poststroke of 49.7 ± 11.4 months, mean ± SEM), confirmed by computed tomography, magnetic resonance imaging, or neurological report; (3) residual unilateral upper extremity weakness; (4) ability to give informed consent and understand the tasks involved; (5) appearance of flexion synergy in the hand, evaluated by observation of a trainee and/or neurologist; and (6) the ability to extend fingers ≥5° from resting position, as evaluated by a stroke specialist. We excluded participants with one or more of the following criteria: (1) cognitive impairment, as seen by a score of <20/30 on the Montreal Cognitive Assessment (MoCA); (2) history of a physical or neurological condition that interferes with study procedures or assessment of motor function (e.g., severe arthritis, severe neuropathy, Parkinson’s disease); (3) inability to sit in a chair and perform upper limb exercises for one hour at a time; (4) participation in another upper extremity rehabilitative therapy study during the study period; (5) terminal illness; (6) social and/or personal circumstances that interfere with the ability to return for therapy sessions and follow-up assessments; (7) pregnancy; and (8) severe visuospatial neglect, as seen by a score of <44/54 on the Star Cancellation Test. Among the screened patients, 3 patients were excluded from the study. One participant had hemorrhagic stroke, one showed cognitive-related issues in understanding the task and could not sign the informed consent, and the third patient did not show residual unilateral upper extremity weakness. For detailed participant characteristics, see Table 1.
Patient Characteristics in the Trained Cohort. a
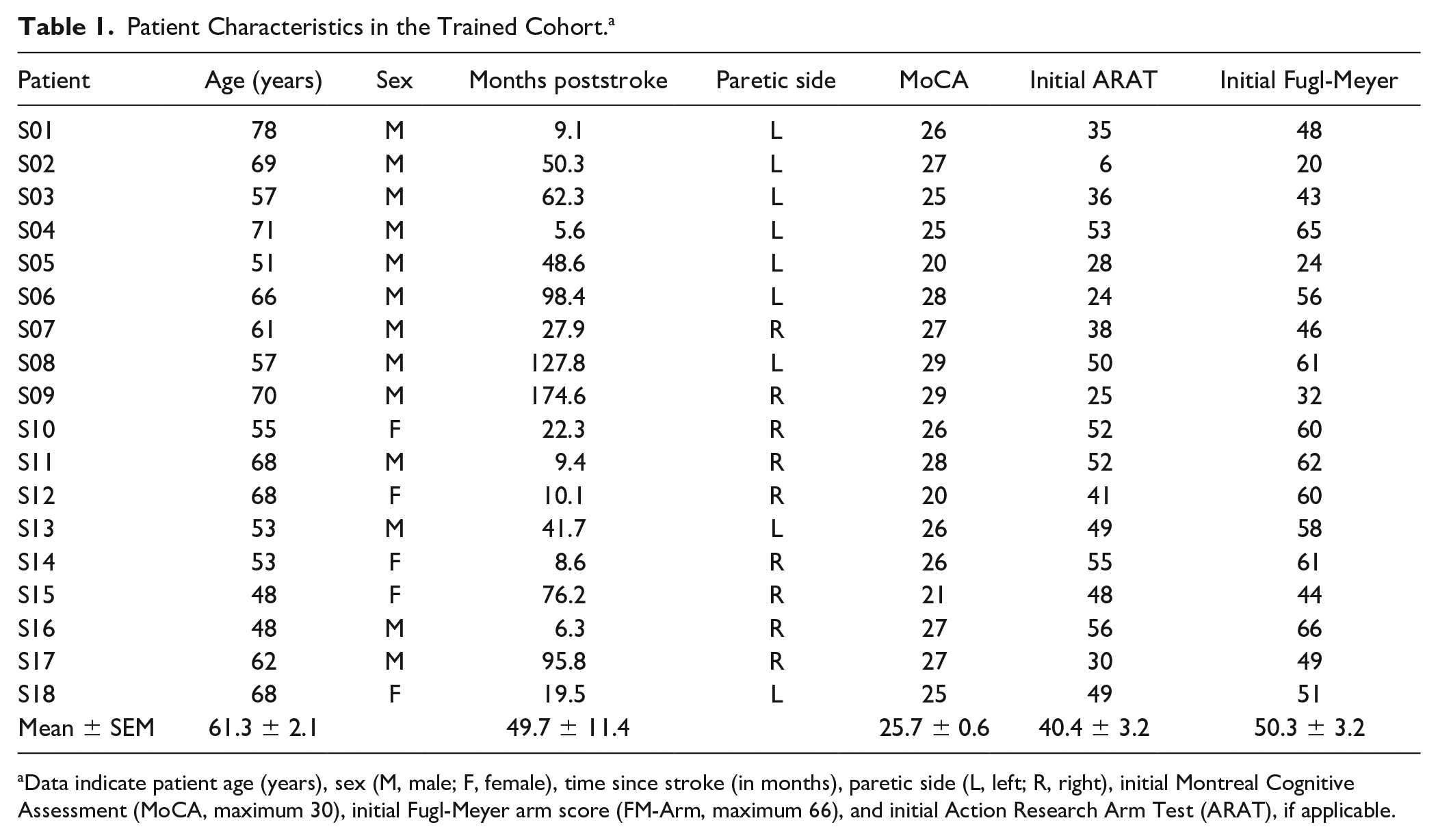
Data indicate patient age (years), sex (M, male; F, female), time since stroke (in months), paretic side (L, left; R, right), initial Montreal Cognitive Assessment (MoCA, maximum 30), initial Fugl-Meyer arm score (FM-Arm, maximum 66), and initial Action Research Arm Test (ARAT), if applicable.
Apparatus to Measure and Train Finger Dexterity
We tested participants’ hand function using an ergonomic device, designed and published previously5, that measures isometric forces produced by each finger (Figure 1A). The hand-shaped keyboard was comprised of 10 keys with force transducers (FSG-15N1A, Honeywell; dynamic range 0-50 N) underneath each key at the position of the fingertips. Downward flexion force exerted at each fingertip was measured at a sampling rate of 200 Hz. The data were digitized using National Instruments USB-621x devices interfacing with MATLAB (The MathWorks, Inc) Data Acquisition Toolbox. Visual stimuli were presented on a computer monitor (22 inches), run by custom software written in MATLAB environment using the Psychophysics Toolbox (Psychtoolbox). 22
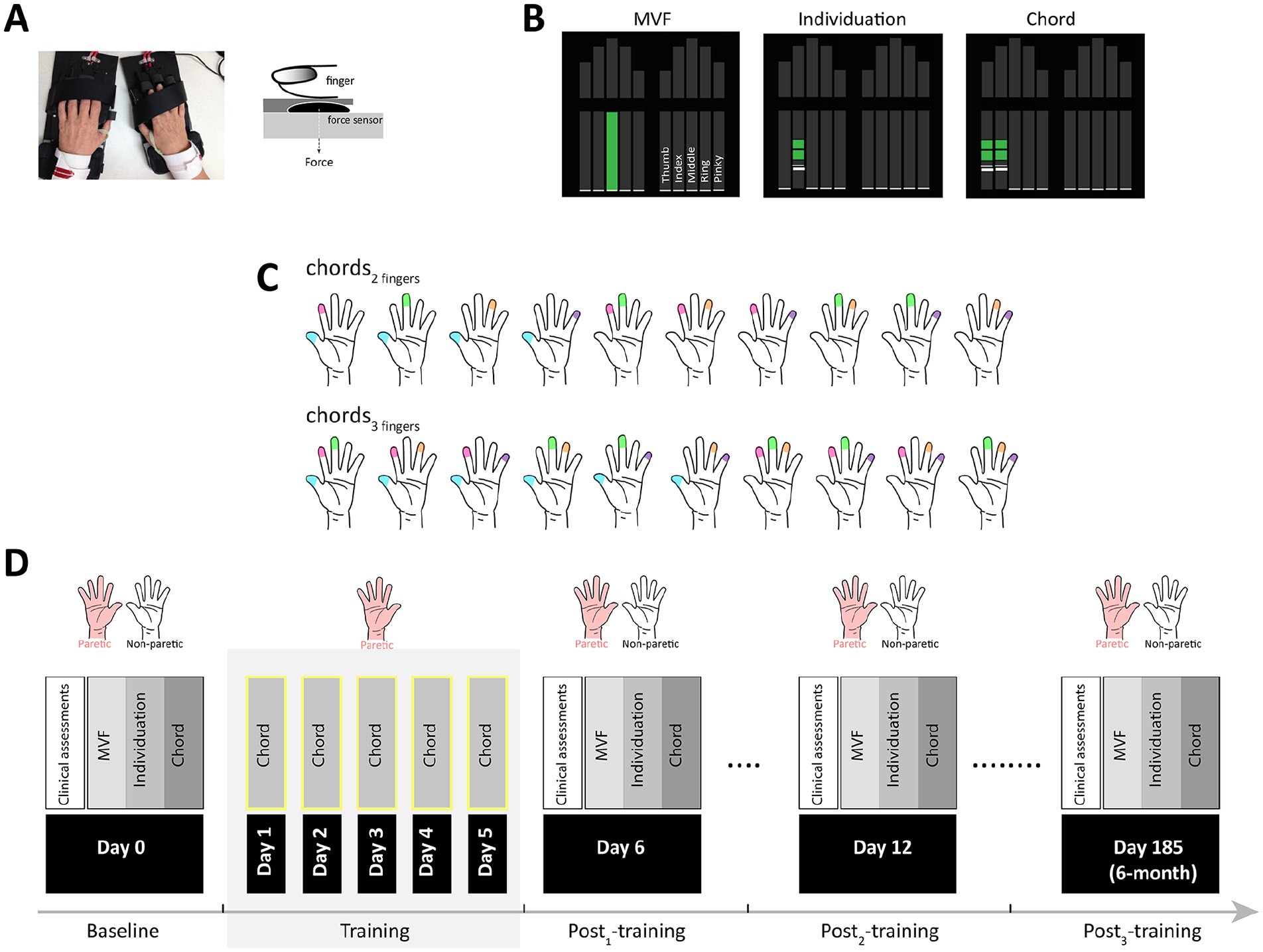
Experimental apparatus and protocol. (A) Ergonomic hand device. Force sensors beneath each key measured the force exerted by each finger in real time. (B) Computer screen showing the instructional stimulus, which indicates both which fingers to press and how much force to produce (height of the green bar). (C) All possible combinations of 2-finger and 3-finger chords tested at baseline and in all post-training sessions. (D) Experimental protocol. During the pre-test, clinical assessments and baseline performance on maximal voluntary contraction force (MVF), individuation, and chord tasks (all possible combinations) were assessed in both hands. During the 5 days of training, participants practiced 6 chords (3 two-finger and 3 three-finger) with the paretic hand (420 trails per day). During post-tests, clinical assessments and performance were reassessed in both hands.
Study Design
We aimed to investigate whether movement control and finger dexterity in the chronic stage of stroke can improve with impairment following intensive training. We evaluated movement quality and finger dexterity by measuring various clinical outcomes, finger strength, individuation, and coordination at multiple time points before (day 0) and after training (1 day, 1 week, and 6 months post-training). For training, we used a novel and challenging piano-chord-like motor task that directly engaged simultaneous coordination of multiple fingers.21,23,24 Participants trained on a subset of possible finger combinations (i.e., chords) with the paretic hand for 5 consecutive days (day 1–day 5). In addition, we quantified generalization and transfer of training to untrained chords and the nonparetic hand, respectively (Figure 1B-D).
Finger Strength and Individuation Task
We used a previously published finger individuation and strength task5. Briefly, participants sat in a comfortable chair facing a computer monitor. Throughout the experiment, participants rested their hands on the keyboards with each finger slightly touching a key, their wrists strapped and fixed on a wrist-rest, and forearms supported by foam armrests. Importantly, given the position of the arms and device the only way to exert isometric forces in the finger tips is by activating finger muscles. In other words, proximal forearm, arm, or trunk movements could not trigger detectable forces. We tested participants’ finger strength and individuation using a finger individuation task that involved pressing a specific key with an instructed finger to match a required force level. Participants could monitor the force exerted by all 10 fingers in real time by the heights of 10 small white horizontal lines moving along the vertical force bars (Figure 1B).
We assessed two separate aspects of finger function, maximal voluntary contraction force (MVF) and individuation5. During each MVF trial, we instructed participants to press one finger at a time with maximum strength as fast as they could 25 and maintain this force level for 2 seconds. The participants could press with the other fingers as much as they wanted as long as maximal force from the instructed finger was achieved. In this manner, we measured MVF three times per finger. In each individuation trial, we asked participants to press only one finger at a sub-MVF force level, while keeping other fingers immobile on the keys. Four target force levels were tested for each finger: 20%, 40%, 60%, and 80% of MVF, and each level was repeated four times. For each trial, we asked participants to bring the corresponding white line up to the force target line (black line in the middle of green region, representing the 25% upper and lower bounds of target force level) (Figure 1B), and maintain the force level for 0.5 seconds. Participants had to complete each trial within 5 seconds. After force release, the bars turned gray again, and the next trial started after a 2-second intertrial interval (ITI). If participants could not cross the force threshold of 1.5 N within 3 seconds, the trial was terminated.
Finger Strength
To obtain a measure of MVF for each digit, we calculated the 95th percentile of the force traces produced across all sampled force data points during the finger-pressing period in each trial and then averaged across the three MVF trials. If the force achieved on 1 of the 3 trials was less than 60% of that produced on the other trial, only the larger force was taken as the MVF measure (6.14% of trials were excluded). The overall strength was then calculated by averaging across all 5 digits.
Individuation Index
To assess participants’ ability to individuate their fingers, we calculated the Individuation Index (the primary outcome measure), which accounts for the relationship between force deviations of the noninstructed fingers and the force produced by the instructed finger. 5 For each trial, we obtained the mean deviation from the baseline force (before Go cue onset) of each uninstructed finger by averaging over all time bins (5 ms) over the entire force trace. A positive linear relationship between the mean deviation of the enslaved noninstructed fingers and the instructed finger force is captured by the slope of the regression line of these two variables. To represent the data in a more intuitive manner we then calculated the negative log of the slope for each of the instructed fingers and averaged across all fingers. In this way, a higher value of this index indicates better individuation (ie, less enslaving, Figure 2A).
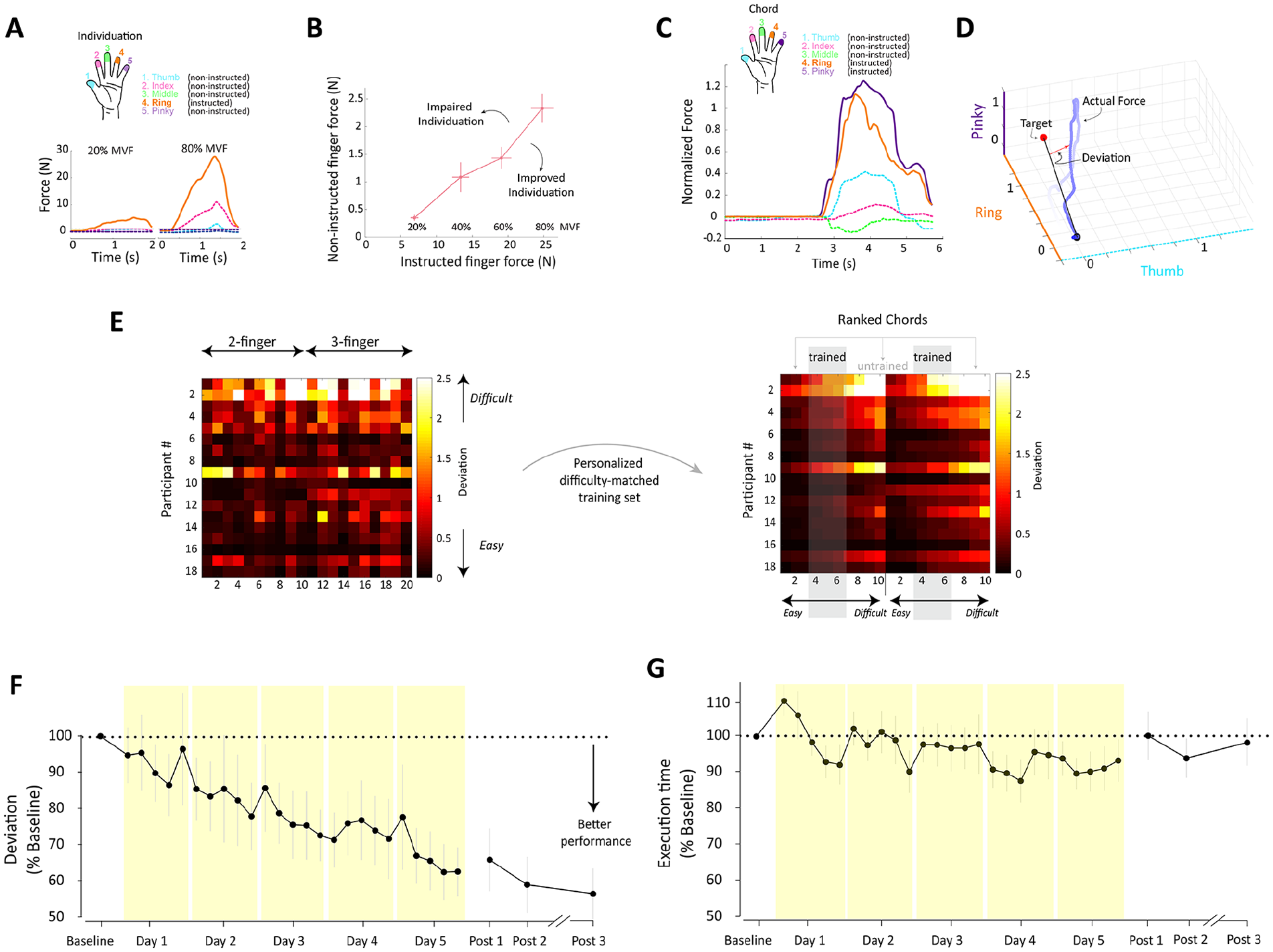
Individuation index, deviation measure, personalized training, and performance during training. (A) Example trials during the individuation task for a single participant. In these particular trials, the fourth finger (inset, orange) was the instructed finger that had to reach a force level of 20% (left panel) and 80% (right panel) of maximum voluntary contraction force (MVF). Note the higher level of enslaving of the uninstructed fingers for higher instructed finger force level. (B) Mean deviation from baseline in the uninstructed fingers plotted against the force generated by the instructed finger for the example in A. (C) Example trial during the chord task for a single participant. Forces exerted by all 5 fingers were sequentially adjusted until the required chord was achieved. (D) Corresponding force trajectories (blue line) in a 3-dimensional finger space consisting of two active fingers (ring and pinky) and one passive digit (thumb). The deviation from this straight-line trajectory (red arrow), averaged across the entire execution phase (initiation to release) was used to quantify accuracy (ie, mean deviation). (E) Mean deviation in all possible combinations of 2-finger and 3-finger chords in the chord task at baseline for all subjects (left panel). Personalized difficulty-matched training set (right panel). (F) Average mean deviation of the trained chords during training and post-training sessions, normalized to baseline performance (in %). (G) Same as F but for execution time. Error bars indicate ± SEM across panels.
Personalized Chord-Like Skill Task
In the chord-like task, we modified a previously published piano-chord-like task13,21,23,24 and instructed participants to simultaneously press 2 or 3 fingers (instructed fingers) of the paretic hand to reach a target force level while maintaining the rest of the fingers (noninstructed fingers) within the resting force range (≤5% MVF). On each chord trial, we instructed participants to bring the corresponding white lines up to the force target level (defined as 20% of MVF for each instructed finger) represented as a black line in the middle of the green region (representing the 25% upper and lower bounds of target force level; Figure 1B). In order to perform an accurate and successful movement, participants had to meet two conditions: (1) to hit the force target using the instructed fingers and (2) to control the forces of the noninstructed fingers and to keep them as low as possible.
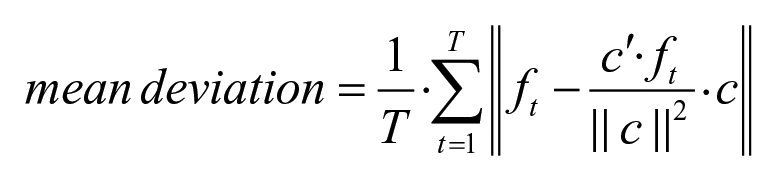
Finger forces (in newtons) were normalized to the baseline force which corresponded to force levels during presentation of the go signal before the movement onset (ie, the resting force). The accuracy during each chord trial was assessed by evaluating the force trajectory in 5-dimensional digit space, which started at the origin (trial initiation) and progressed to the desired chord and returned to the origin. If a chord was generated with perfect simultaneity and no passive finger coactivation, the force trajectory corresponded to a straight line (Figure 2D, black line) toward the goal chord (red sphere). Contrarily, increased involuntary flexion coactivation of passive fingers caused deviation from this straight-line trajectory. We quantified accuracy as the multidimensional Euclidian distance between the actual force (ft) and the projection of the produced force onto the target trajectory (c).21 This distance was averaged over all time points from force initiation (t = 1) to termination (T) to produce the “mean deviation” (Figure 2C and D) as follows:
Since chord difficulty is idiosyncratic to the individuals, we carefully selected a subset of chords for training based on each participant’s performance at baseline. In other words, we personalized the training to the individual. We used mean deviation to rank baseline performance of all possible combinations of 2-finger (rank 1:10) and 3-finger chords (rank 1:10) for each individual. We assumed that the larger the deviation for a given chord, the more difficult to execute that chord. Based on the baseline ranking, we then selected 6 chords (3 for each type) in the mid-range of difficulty (ranks 4, 5, 6 out of 10) for training (trained chords) (Figure 2E). On each training day, participants practiced 5 blocks of 84 trails (14 repetitions × 6 selected chords, randomly interleaved), yielding 420 trials per day (completed in 3.5-4 hours) and 2100 for the 5-day training. The duration of each chord trial was 5 seconds. In addition, we tested generalization by measuring performance with the paretic hand in the untrained chords after each training session.
Clinical Outcome Measures
In order to track changes in clinical metrics of impairment, objective measures of function, and self-reported measures of function over the course of the study, we included a battery of clinical assessments. A licensed physical therapist performed these assessments in the pre- and post-test sessions.
Clinical Measures of Impairment
Upper extremity motor impairment was quantified using the arm subscale of the Fugl-Meyer test (FM-UE). 26 This test includes 33 items scored on an ordinal scale (0-2) with a total of 66 points, with higher scores representing less impairment. The Modified Ashworth Scale measures resistance during passive soft tissue stretching and is used as a simple measure of the spasticity of the elbow, wrist, thumb, and finger joints. 27 Scores for each joint range from 0 (no increase in muscle tone) to 4 (affected parts rigid in flexion or extension). We used Semmes-Weinstein Monofilament testing 26 to assess the light touch sensation of each digit of the paretic hand. To complete this testing, a participant closed his or her eyes and verbally responded “yes” each time he or she perceived the monofilament on the pad of a finger. Monofilaments (sizes 4.31, 3.61, and 2.83) were applied to the test site perpendicularly until they bent for 1 second. For each monofilament, 6 test probes were applied to each finger in a randomized order for a total of 30 probes per monofilament. Sensation scores are expressed as the number of correct positive responses out of 30.
Clinical Measure of Function
To assess upper limb function, we used the Action Research Arm Test (ARAT). ARAT assesses the ability to grasp and manipulate objects of different sizes, shapes, and weights and is considered a measure of upper limb and hand function and activity. Improvement on this scale, therefore, provides evidence supporting the hypothesis that the chord training implemented here can lead to a meaningful improvement in upper extremity motor function. This test includes 19 items divided into 4 subcategories (grasp, grip, pinch, gross movement). It is scored on an ordinal scale (0-3) with a total of 57 possible points and higher scores representing better function. 29
Self-Reported Measures of Functional Use
Last, we included the Motor Activity Log (MAL). The MAL is a structured interview used to assess real-world upper extremity activity. 30 An individual is asked to rate his/her performance on how much (Amount of Use subscale, AOU) and how well (Quality of Movement subscale, QOM) the paretic upper extremity is used during a variety of activities typically completed in daily life. Each of 30 items is rated from 0 to 5 and scores for each scale are calculated as the mean of the scored items attempted with the paretic arm. Averages closer to 5 indicate better quality of movement and more use of the paretic arm/hand.
We also reported the minimal clinically important difference (MCID) of each clinical measure as defined by the 10% of the measure’s total range (eg, 5.7 points MCID in ARAT test). 31
Statistical Analysis
We implemented a linear mixed-effects model using the lme4 package in R 32 with time point as a fixed effect and participant as a random effect and calculated the χ2 to assess the significance of the fixed effect. The estimated mixed-effects model deals with cases of incomplete and unbalanced data in a statistically efficient way. Any differences were explored post hoc using 2-sample paired t-test, implemented in Prism software (GraphPad Software Inc), with statistical significance considered at P < .05. For the training data set, we first averaged performance (ie, mean deviation, execution time) across the 5 blocks of each day and then compared the average value across days. For the pre- and post-training data set, we estimated the mixed-effects model and compared the scores across time points.
Results
In our data set, Individuation Index, Strength, ARAT, and FM-UM were completed for all participants for the pre, post 1-, and post 2-training time points. Clinical assessment of participation as measured by MAL was incomplete and had missing values for some participants. For the 6-month follow-up session (ie, post 3-training), we obtained data of all assessments from 13 participants (72.2%). Patient characteristics and the percentages of successfully measured sessions for the different tests are reported in Tables 1 and 2, respectively.
The Percentages of Successfully Measured Sessions for the Different Tests. a
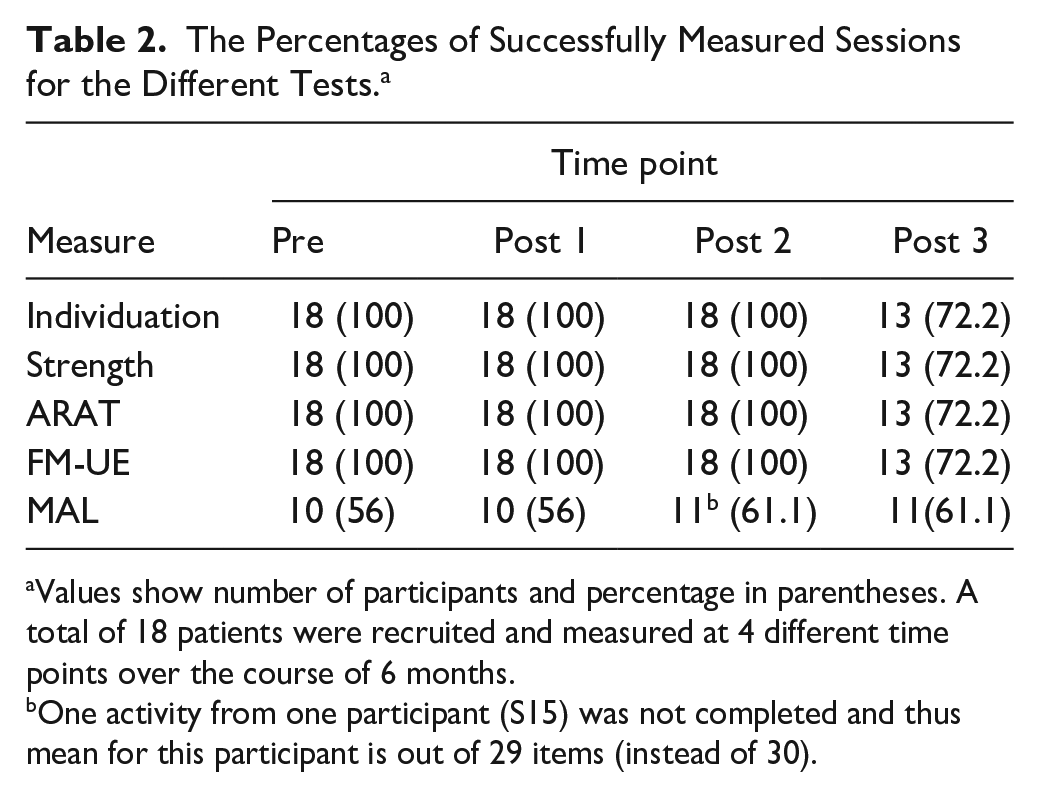
Values show number of participants and percentage in parentheses. A total of 18 patients were recruited and measured at 4 different time points over the course of 6 months.
One activity from one participant (S15) was not completed and thus mean for this participant is out of 29 items (instead of 30).
Training Led to Improvements in Chord-Like Skill Performance
The first objective of this study was to determine whether patients with chronic stroke can improve finger dexterity when training on a task that requires coordinated movements in a direction opposite to the typical abnormal flexion synergy. We hypothesized that training would lead to improvements in force accuracy (i.e., reduced force deviation in all fingers) and, to some extent, faster execution (i.e., reduced execution time).
We found that participants were able to synchronously engage correct combinations of fingers to perform accurate force patterns during training. The linear mixed-effect model revealed that participants significantly improved their force accuracy and reduced deviation (of the non-instructed fingers) over the course of the training (χ2 = 19.20, P = 1.18e-05). By the end of training, participants reduced their baseline deviation by ~38% ± 6.8% (mean ± SEM). The post-training (post 1, post 2, and post 3) skill assessments revealed similar effects. Post hoc comparison between performance on day 5 and each post-training session showed that training effects on deviation did not significantly decline by day 1 (t(17) = 0.39, P = .70); week 1 (t(17) = 1.24, P = .23); and 6 months (t(12) = 1.01, P = .34) (Figure 2F).
Since accuracy and speed might be inherently linked, a confound arises when comparing the accuracy of force patterns performed at different speeds. This limitation makes it difficult to interpret cases where participants improve their accuracy yet decrease their speed. Our data showed that this was not the case. Our participants did not sacrifice speed for accuracy (Figure 2G). Although we expected to see some improvement on execution speed, there was no significant change in execution time across training days (χ2 = 0.10, P = .75).
Training Improved Hand Dexterity in Both the Paretic and the Nonparetic Hands
Next, we determined whether the accuracy gain observed in the trained chord-like task led to a general improvement of finger dexterity, beyond the trained task. To this end, we first examined before and after changes in individuation index and found that participants experienced significant improvements in this metric (χ2 = 14.09, P = .00017; Figure 3A). Post hoc analysis showed that individuation improved relative to baseline by 10.3% ± 4.55% in post 1-training (t(17) = 2.36, P =.031); 12.9% ± 5.80% in post 2-training (t(17) = 2.43, P = .027); and 11.71% ± 9.31% in post 3-training (t(12) = 2.72, P = .018) (Figure 3A).
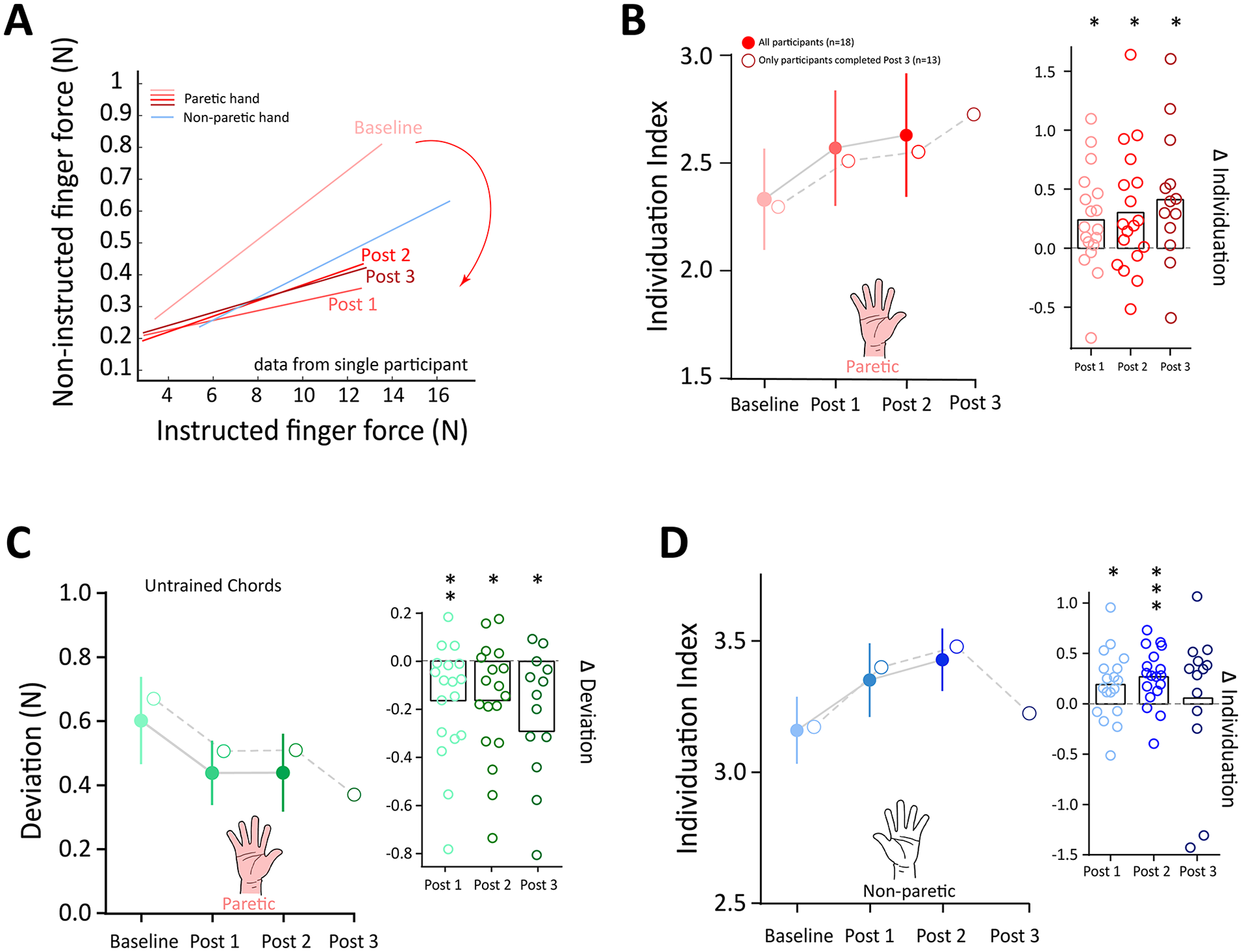
Training effect on finger individuation generalized to untrained task and transferred to untrained hand. (A) Training reduced the enslaving in the individuation task. Forces of the noninstructed fingers as a function of the forces in the instructed fingers in a single participant for baseline, post 1-training, and post 2-training sessions. For comparison, data from the nonparetic hand is also shown (blue line). The log slope of each subject at each time point constituted the Individuation Index. (B) Mean data of the Individuation Index during baseline and post-training sessions. Solid line and solid marks show the data from all participants (n = 18) who completed post 2 session and dashed line and open marks show the data from participants (n = 13) who completed post 3 session. Inset shows individual data for the change (relative to baseline) in the Individuation Index in the paretic hand in post-training tests. (C) Improved performance (ie, reduced deviation) generalized to the untrained chords in the paretic hand. (D) Finger individuation transfer to the untrained nonparetic hand. Error bars indicate ±SEM across all panels. Significance levels are as follows: *P < .05, **P < .01, and ***P < .001.
Given that increased individuation ability reflects improvement of finger dexterity, we predicted that the improved finger dexterity should also be reflected in better performance of untrained chords. Indeed, when comparing pretraining deviation with that of post-training, we found that participants also exhibited significant reduction in deviation (of the noninstructed fingers) for the untrained chords (χ2 = 17.44, P = 2.97e-05; Figure 3B).
To ascertain whether training effects on chord learning were effector specific, we examined performance of the untrained (nonparetic) hand before and after training. We found that training effects were not limited to the trained hand. Improvements in individuation were significantly present in the untrained, nonparetic hand up to 1 week (χ2 = 12.49, P = .0004; Figure 3C). Post hoc analysis showed that individuation of the untrained hand improved by 6% (t(17) = 2.394, P = .0285) and 8.5% (t(17) = 4.039, P = .0009) in post 1-training and post 2-training, respectively. This effect, however, was not present at 6 months (t(12) = 0.29, P = .78).
Training Led to Meaningful Clinical Changes in Impairment, Function, and Hand Use
In order to determine whether the impairment reduction in hand dexterity had meaningful clinical effects, we assessed and tracked changes in function, impairment, and self-reported measures of functional use. At baseline, participants were moderately impaired, with a mean ARAT score of 40.4 and mean total FM-UE score of 50.3 (Table 1).
Hand function as measured by ARAT improved significantly post-training (χ2 = 18.88, P = 1.39e-05; Figure 4A). Post hoc analysis showed that total ARAT score improved by 5.60 ± 0.8 points in post 1-training (t(17) = 6.37, P < .0001); 6.0 ± 0.90 points in post 2-training (t(17) = 6.48, P < .0001); and 4.54 ± 1.14 points in post 3-training (t(12) =3.99, P = .0018). ARAT subscales revealed that the majority of the improvement occurred in the pinch precision domain (48%, 53% and 49% of the total improvements for post 1, post 2, and post 3-training, respectively). The ARAT grip subscale showed the second greatest improvement (32%, 25%, and 28% for post 1, post 2, and post 3-training, respectively; Figure 4B). Notably, the differences in ARAT up to 1 week after training exceeded the reported MCID for chronic stroke patients (5.7 points). 33
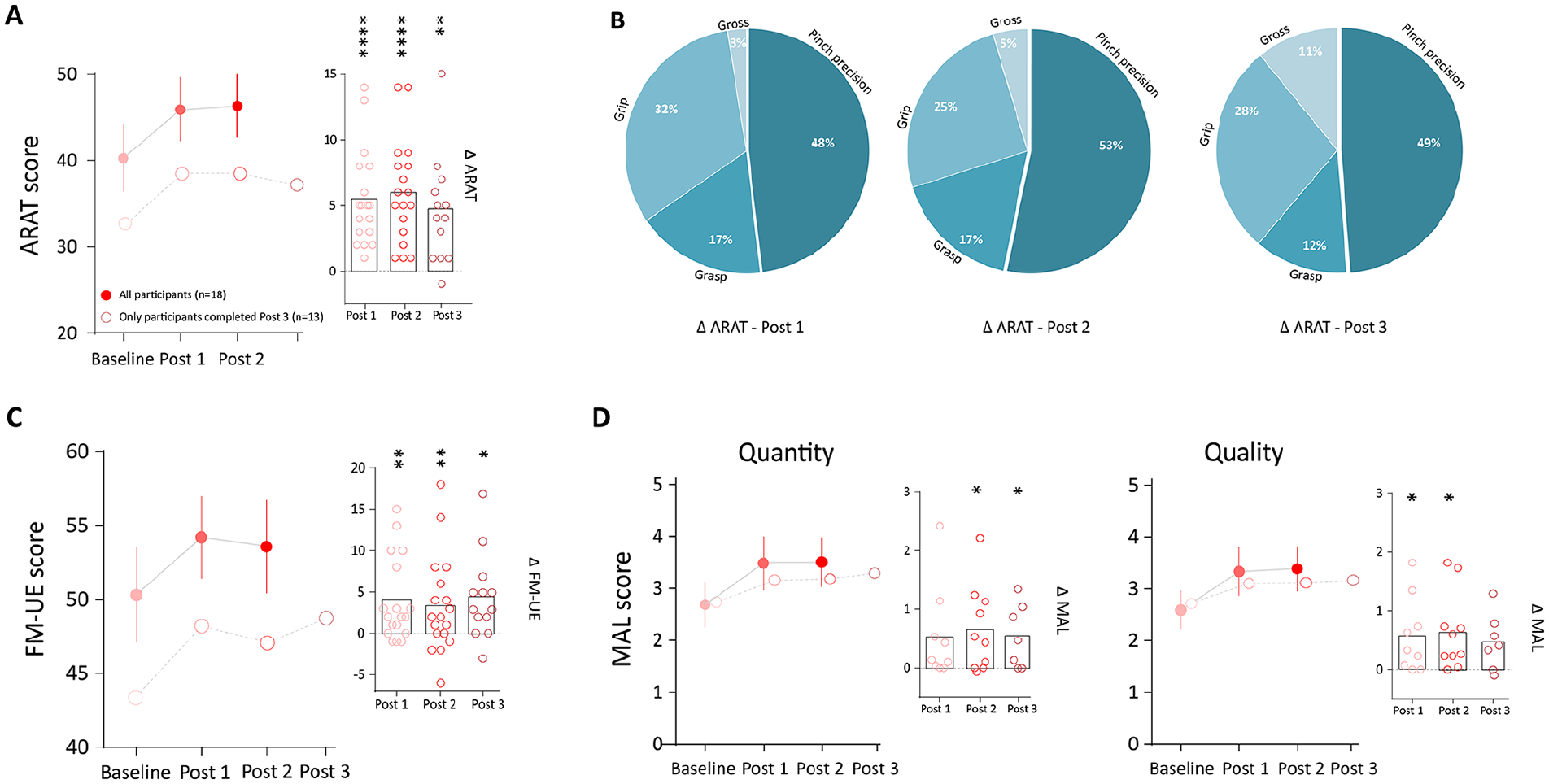
Non-task-oriented generalization and retention. (A) Action Research Arm Test (ARAT) improved significantly post-training. Inset shows individual data for the change (relative to baseline) in the ARAT score in post-training tests. Solid line and solid marks show the data from all participants (n = 18) who completed post 2 session and dashed line and open marks show the data from participants (n = 13) who completed post 3 session. (B) Inspection of ARAT subscales revealed that the majority of improvement occurred on the Pinch Precision domain. (C) Fugl-Meyer assessment of upper extremity (FM-UE) also showed statistically significant improvement post-training. (D) Training improved the amount of use (left panel) as well as the quality of the executed movement (right panel) in Motor Activity Log (MAL). MAL score was not available in post 3 session. Error bars indicate ±SEM across all panels. Significance levels are as follows: *P < .05, **P < .01, and ****P < .0001.
In terms of overall clinical impairment, FM-UE also showed statistically significant improvement post-training (χ2 = 10.77, P = .001). FM-UE score improved by 3.90 ± 1.2 points in post 1-training (t(17) = 3.28, P = .0044); 3.30 ± 1.30 points in post 2-training (t(17) = 2.42, P = .0269); and 4.39 ± 1.43 points in post 3-training (t(12) = 3.07, P = .0098) (Figure 4C). This significant improvement, however, did not exceed the MCID for this measure in chronic stroke (5.25 points). 31
In terms of AOU and QOM in MAL, we found that participants reported an overall improvement in AOU (χ2 = 10.01, P = .0015), as well as QOM (χ2 = 3.90, P = .048) (Figure 4D). The significant improvement in MAL exceeded previous definition of MCID, set at 10 % of the total scale range on the basis of clinical experience, and MCID for similar measures (0.5 points). 34
Last, we assessed the cross-sectional relationships of Strength and Individuation, and the clinical measures of function (ie, ARAT) and impairment (ie, FM-UE) obtained from the paretic hand across all time points (ie, data from all sessions were included in this analysis). Overall, all correlations were high and significant (Table 3A). However, since Strength and Individuation were correlated (r = 0.484, P < .001), we calculated the partial correlations between Individuation and clinical measures after controlling for Strength, and vice versa. While Individuation remained highly correlated with the clinical measures after controlling for Strength, Strength was not correlated with clinical measures after controlling for Individuation (Table 3B).
(A) Cross-Sectional Correlation Between Strength, Individuation, ARAT, and FM-UE a and (B) Partial, Cross-Sectional, Correlation Between Strength and Individuation With Clinical Measures After Controlling for the Internal Variable (Individuation and Strength, Respectively).
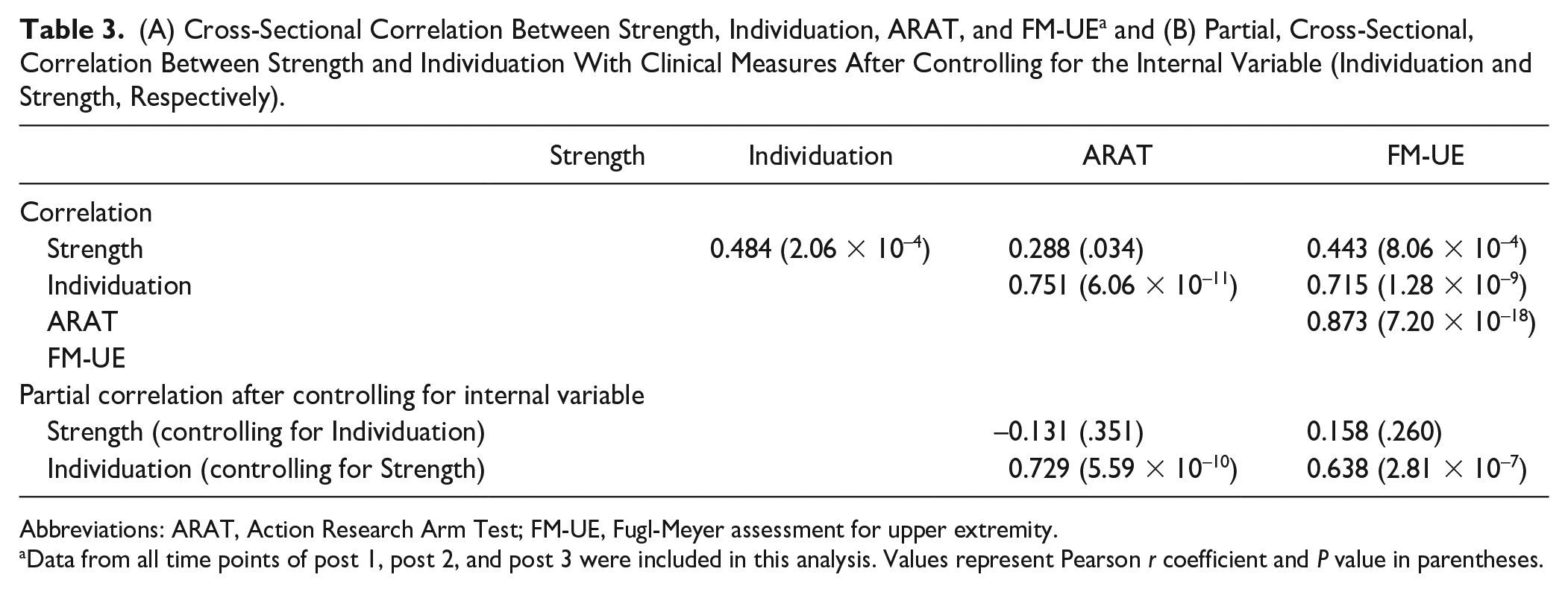
Abbreviations: ARAT, Action Research Arm Test; FM-UE, Fugl-Meyer assessment for upper extremity.
Data from all time points of post 1, post 2, and post 3 were included in this analysis. Values represent Pearson r coefficient and P value in parentheses.
Discussion
In this longitudinal, nonrandomized, single-group chronic stroke cohort study, we tested whether training requiring fingers to move independently and against the frequently observed abnormal flexion synergies could reduce hand impairment as depicted by an improvement in finger dexterity. In addition, we assessed whether these changes had a clinically meaningful impact on overall motor function and impairment beyond finger individuation ability. We found that patients with stroke in the chronic phase were able to reduce their impairment in finger movement accuracy, coordination and individuation following intensive training. Importantly, training not only improved in the trained task but also ameliorated overall finger dexterity and movement quality (e.g. MAL and ARAT measures). These effects remained present at 6 months following the training period.
A recent longitudinal study on hemiparetic stroke patients showed that finger individuation and strength recovery dissociate, with most of the finger individuation improvements occurring within the first 3 months after stroke, and nonsignificant changes for the remainder of the first year. 5 Critically, this recovery pattern indicated that patients do not fully recover under current standard of care, consistent with other classic reports of the natural history of stroke recovery.35-39 This recovery limitation in motor impairment has led to many rehabilitation programs in the chronic phase after stroke to focus the efforts on compensation interventions rather than reducing neurological deficits. Thus, current therapeutic approaches are based on task-oriented motor training primarily focusing on task or goal accomplishment, rather than reduction of impairment.38-42 However, recent studies in human and animal models of stroke provide new evidences suggesting that in order to truly recover from impairment, and possibly impact disability, the focus of training should be on movement quality and that practice should be delivered at high intensity.8,41-46 For example, Murata et al 42 reported in monkey models of stroke that deficits in finger dexterity due to lesions in the digit representation in the primary motor cortex (M1) recovered to the same level as those in the prelesion period when they received intensive daily training for 1 to 2 months.
Here we designed a personalized training approach with a high number of repetitions (480 repetitions per session, total of 2100 repetitions) at high intensity (1 session of 3-4 hours per day, for 5 days) in a challenging piano-chord-like task focused on breaking the flexion synergy, while minimizing the use of compensatory movements. The task was derived from prior studies of motor control in healthy humans21,23,24 and nonhuman primates. 12 Successful performance in this task requires coordination and synchronization of multiple fingers and the ability to move against the flexor synergy. Unlike other motor sequence tasks, this piano-like chord task requires the participants to learn how to efficiently adopt a range of hand configurations activating some fingers and relaxing others. Learning finger configurations is a basic step to develop hand dexterity, and becomes essential in diverse motor skills such as activities of daily living. Recent psychophysical studies showed that chord learning has a substantial generalization effect to untrained chords and the untrained hand.23,24 In support of this, our data in patients with chronic stroke revealed similar effects in chord learning, and notably, the gains in motor function observed in the ARAT test were mostly driven by improvement in the pinch precision domain.
Improvement in finger dexterity and motor functions in the chronic stage of stroke following intensive practice are indicative of “residual capacity,” which refers to the finding that additional movement practice can improve motor function, including dexterity and strength.47-50 Although motor recovery of upper extremities following a stroke reaches an apparent plateau, or even deteriorates in the first year after the initial incident,35-51 some studies have suggested that high dose of intensive movement practice can tap into the residual capacity leading to overall improvement in upper extremity motor function in both the subacute and chronic phases following a stroke.8,52-54 The limitation of these prior studies, however, is that compensation could not be ruled out as the mechanism underlying the observed improvement. Unlike those investigations, the apparatus, the individuation outcome metric and the trained task used in this study does not permit the use of compensatory movements. Therefore, the gains observed here have to be due to a reduction of impairment.
What is the neural substrate that underlies the recovery of finger dexterity in stroke? Work in human and in animal models of stroke demonstrated the contribution of the corticospinal tract (CST) to finger dexterity and recovery. In 1968, Lawrence and Kuypers8,55 reported systematic studies of the effects of lesions to the corticospinal tract and found that the capacity for precise control of fingers was lost after a complete, bilateral lesion of the pyramidal tract; while strength was severely impaired after bilateral disruption of the reticulospinal tract. Consistent with this idea, Xu and colleagues 5 analyzed diffusion tensor imaging data of stroke while tracking recovery of finger individuation and strength and found that lesions in the hand areas in M1, as well as the CST, correlated more with impaired individuation than with strength in humans with stroke. This study was more recently followed by another investigation demonstrating the reliance of finger individuation recovery on the presence of motor-evoked potentials in the hand. 56 Based on these observations, we speculate that the residual CST of the ipsilesional side was most likely involved in the finger individuation recovery observed in our study.
The multifinger motor action during the chord/piano-like training task resembles to some extent the action performed during music playing on a piano. Previous work evaluated the effect of a real music-supported training provided some evidences for positive gains in motor function 57 that was accompanied with electrophysiological changes in M1. 58 We therefore think it is possible that adding musical cues during the piano-like task might be an interesting approach that could be considered in future studies to boost training effects.
This study has some limitations. First, there is no control group for the specific training regimen used in our research. Thus, it is not possible to conclude that all the gains found in hand dexterity are due to the training intervention. It is possible that other non-specific effects such as motivation in research participation or passage of time led to some of the changes. Nonetheless, the demonstration of effectiveness of a specific training protocol was not the focus of our study. Rather, we aimed to determine whether it is possible to change hand impairment in patients with chronic stroke. In our study, this was accomplished by a training regimen focused on moving against flexor synergies that does not permit for compensatory maneuvers and based on motor learning principles (high intensity and repetition). This work provides evidence that hand motor impairment can be reduced in the chronic phase after stroke. This opens up the opportunity to test the effects of behavioral training interventions following similar principles used here (focus on reducing impairment without permitting the use of compensatory maneuvers, with high number of repetitions) through formal randomized controlled trials. The second limitation to consider is that while ARAT and Individuation Index were correlated across all post-training sessions, these correlations do not mean causality. In other words, we cannot conclude that changes in hand function and impairment are due to the improvements in individuation itself.
In conclusion, we provide evidence that patients in the chronic phase following stroke can reduce hand impairment and improve finger dexterity. This was observed by direct quantitative measurement of dexterity following training on a multiday skill task focused on moving fingers against abnormal synergies without allowing other compensatory movements (ie, from proximal upper extremity or trunk). Since this is a single cohort group, we cannot determine whether this effect was purely the result of the training paradigm or other nonspecific effect, such as passage of time or research participation. This study shows that chronic stroke patients are able to learn new patterns of multidimensional finger postures against abnormal flexor synergies; an improvement at the impairment level that correlated with meaningful functional changes. Of note, the improvement was sustained, and transferred to some extent to the nonparetic hand and generalized to untrained chords. The present findings are important because they show that patients may have residual capacity to change impairment, even in the chronic stage following stroke, leading to meaningful clinical impact. If the present findings are corroborated in future controlled clinical trials, then stroke rehabilitation programs in the chronic phase will need to reconsider changing the focus from mostly compensatory to also include intensive training to reduce impairment.
Supplemental Material
NNR_34_8 – Supplemental material for Pushing the Rehabilitation Boundaries: Hand Motor Impairment Can Be Reduced in Chronic Stroke
Supplemental material, NNR_34_8 for Pushing the Rehabilitation Boundaries: Hand Motor Impairment Can Be Reduced in Chronic Stroke by Firas Mawase, Kendra Cherry-Allen, Jing Xu, Manuel Anaya, Shintaro Uehara and Pablo Celnik in Neurorehabilitation and Neural Repair
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Institutes of Health/National Institute of Child Health and Human Development Grants R01HD053793 (PC) and R01HD073147 (PC).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.