
Abstract
Background. Contradictory results have been reported for transcranial direct current stimulation (tDCS) as treatment for tinnitus. The recently developed high-definition tDCS (HD tDCS) uses smaller electrodes to limit the excitation to the desired brain areas. Objective. The current study consisted of a retrospective part and a prospective part, aiming to compare 2 tDCS electrode placements and to explore effects of HD tDCS by matched pairs analyses. Methods. Two groups of 39 patients received tDCS of the dorsolateral prefrontal cortex (DLPFC) or tDCS of the right supraorbital–left temporal area (RSO-LTA). Therapeutic effects were assessed with the tinnitus functional index (TFI), a visual analogue scale (VAS) for tinnitus loudness, and the hyperacusis questionnaire (HQ) filled out at 3 visits: pretherapy, posttherapy, and follow-up. With a new group of patients and in a similar way, the effects of HD tDCS of the right DLPFC were assessed, with the tinnitus questionnaire (TQ) and the hospital anxiety and depression scale (HADS) added. Results. TFI total scores improved significantly after both tDCS and HD tDCS (DLPFC: P < .01; RSO-LTA: P < .01; HD tDCS: P = .05). In 32% of the patients, we observed a clinically significant improvement in TFI. The 2 tDCS groups and the HD tDCS group showed no differences on the evolution of outcomes over time (TFI: P = .16; HQ: P = .85; VAS: P = .20). Conclusions. TDCS and HD tDCS resulted in a clinically significant improvement in TFI in 32% of the patients, with the 3 stimulation positions having similar results. Future research should focus on long-term effects of electrical stimulation.
Keywords
Introduction
Subjective tinnitus is the conscious perception of a sound in the absence of an external source. According to a recent large epidemiological study by Bhatt et al, 1 9.6% of adults in the United States have experienced tinnitus that lasted for at least 5 minutes in the past 12 months. Among those who reported tinnitus, 36% had nearly constant symptoms, 7.2% rated their tinnitus as a large or very large problem, and 49.4% had discussed it with a physician. 1 For 2.4% of the adult population, tinnitus severely influences the quality of life because it causes a considerable amount of distress. 2
Although the precise pathophysiological mechanism of tinnitus is not yet fully understood, it is hypothesized that it results from maladaptive plastic changes involving a wide network of cortical areas (eg, central auditory system) and subcortical structures (eg, limbic system), each representing a particular aspect of tinnitus.3-6 Concerning treatment options for tinnitus, there is no one-treatment-fits-all solution. Therefore, a multidisciplinary approach is required to obtain a tinnitus profile of each patient, resulting in an individual treatment plan. Tinnitus retraining therapy and cognitive behavior therapy are widely known as effective tinnitus treatments. Alternatively, neuromodulation techniques, including transcranial direct current stimulation (tDCS), can be used to reduce tinnitus loudness and annoyance by inducing cortical plasticity and modulating the activity of the malfunctioning brain structures.4,7 Vanneste and De Ridder 8 showed that dorsolateral prefrontal cortex (DLPFC) tDCS was able to suppress tinnitus by modulating the parahippocampal area, the pregenual anterior cingulate cortex, and the right primary auditory cortex in a resting-state electroencephalography (EEG) study. These results suggest that DLPFC tDCS not only has an effect on the underlying DLPFC, but also on functionally connected brain areas relevant for tinnitus intensity and tinnitus distress. 8 Nevertheless, the exact mechanism of tinnitus modulation after tDCS is still difficult to predict because of the involvement of multiple brain networks and relatively nonfocal stimulation by tDCS. 9 According to a systematic review by Song et al, 10 39.5% of the tinnitus patients have responded to tDCS, with a mean tinnitus intensity reduction of 13.5% when measured by a visual analogue scale (VAS).
tDCS safely transmits a weak direct electrical current to the brain by means of 2 surface electrodes (ie, anode and cathode).4,11 It is able to influence the resting membrane potential without inducing action potentials. 9 Possible side effects during stimulation are moderate fatigue, mild tingling, and light itching sensations under the electrodes, whereas headache, nausea, and insomnia are possible side effects after stimulation. 12 Because of transient sensations evoked by a few seconds of stimulation, tDCS is effective for sham-controlled trials.9,13
Studies differ considerably with regard to reported effects of tDCS on tinnitus perception. These differences can be assigned to electrode position, electrode size, electric field orientation (defined by the electrodes’ positions and polarities), stimulation duration, and current intensity. 13 The polarity of the stimulation, for example, determines the modulating effect of tDCS. Anodal tDCS increases the excitability of the underlying cortex by depolarizing specific neurons, whereas cathodal tDCS induces inhibition as a result of hyperpolarization.3,4 The left temporoparietal area (LTA) and DLPFC are the most common targets for stimulation, being parts of the neural network that seems to play an important role in tinnitus perception. 14 Previous studies have shown that LTA is overactivated in tinnitus patients, and DLPFC is involved in the integration of sensory and emotional aspects of tinnitus. 15 Cortical stimulation of these 2 sites has showed comparable results with regard to the percentage of responders and the amount of reduction in tinnitus intensity. 10 When the anode was placed at the LTA, the most effective stimulation could be achieved with 2 mA tDCS during 20 minutes. 16 To date, studies do not produce any consistent picture on the target locations for tDCS.
The main limitation of tDCS is the broad stimulation pattern, especially when there is a large distance between the cathode and anode.14,17 One potential solution is a recent technique called high-definition tDCS (HD tDCS), using 5 small gel electrodes, instead of the conventional 2 large sponge electrodes. Consequently, HD tDCS results in increased focality with limited depth of penetration.18-20 Furthermore, the montage of HD tDCS, with 4 electrodes forming a ring, results in a more unidirectional modulation, such that the polarity of the center electrode determines the change in excitation instead of considering anodal and cathodal effects with conventional tDCS.21,22 Shekhawat et al 14 have investigated HD tDCS effects in 27 tinnitus patients, resulting in a reduction in tinnitus loudness or annoyance of at least 1 point in 78% of the patients. In addition, they have shown that higher intensity (2 mA) and longer duration (20 minutes) were more effective. In a recent study, Shekhawat and Vanneste 23 have confirmed a significant reduction in tinnitus loudness after 15 or 20 minutes of HD tDCS of DLPFC compared with a sham session. Therefore, they suggested a session of 15 minutes as the optimum stimulation duration instead of the conventional 20 minutes. Moreover, they indicated the safety of this electrical stimulation. Tingling, sleepiness, and scalp pain were the most common transient sensations experienced during HD tDCS. 23 In contrast to these promising results, Henin et al 24 found no significant effect of HD tDCS on reducing the tinnitus percept compared with a sham group. However, they used different electrode positions by splitting the current across 2 sets of electrodes. Furthermore, the washout time between the applied treatments within 1 session (tDCS and compensatory auditory stimulation) could have been too short, possibly obscuring some of the potential benefits of HD tDCS. 24
The current article describes a retrospective study on the effects of conventional tDCS at 2 different electrode positions, followed by a prospective study on the effects of HD tDCS. The aim of these studies is threefold. First, therapeutic effects of 2 different electrode placements for tDCS (ie, DLPFC and RSO-LTA tDCS) are compared. Second, the recent technique of HD tDCS is explored with regard to clinical outcomes. Finally, the therapeutic effects of tDCS and HD tDCS are compared.
Methods
The Committee for Medical Ethics UZA-UAntwerp approved the study (File Number: 16/41/415). All participants gave written informed consent prior to any treatment.
Participants
A total of 117 chronic nonpulsatile tinnitus patients were assessed for the current study and screened for eligibility. 20 Patients who underwent another ongoing tinnitus treatment or had a middle ear pathology were excluded. The tinnitus-related details of the patients are summarized in Table 1.
Tinnitus Details of Participants Included in the tDCS and HD tDCS Study.
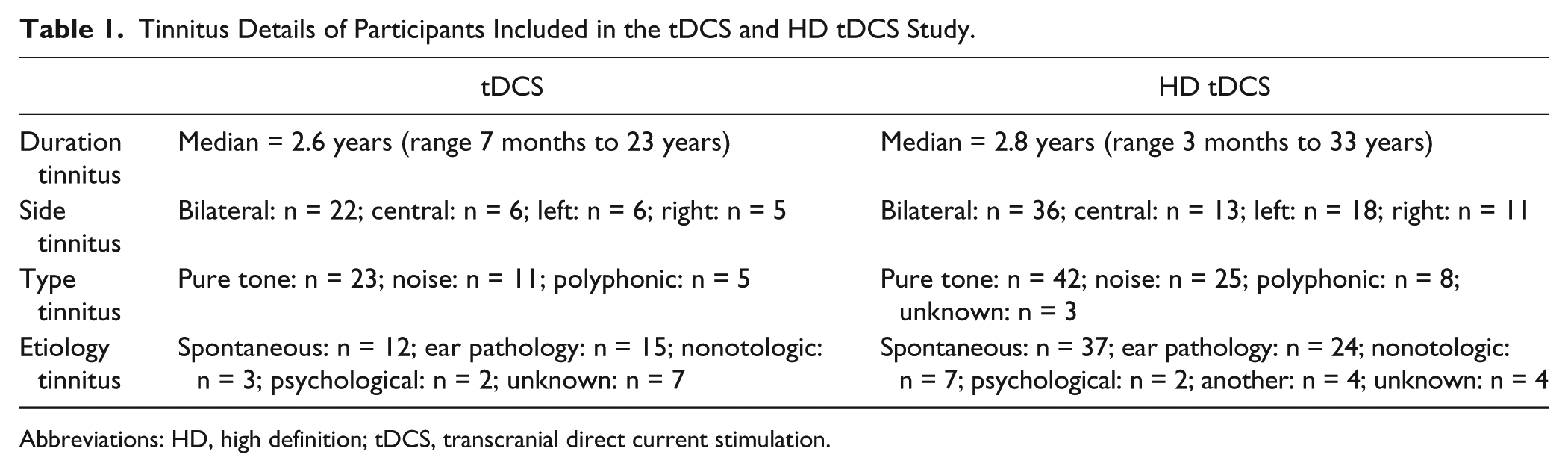
Abbreviations: HD, high definition; tDCS, transcranial direct current stimulation.
The patients of the retrospective study received either tDCS of DLPFC or tDCS of the right supraorbital-left temporal area (RSO-LTA). Two groups were randomly formed based on this electrode placement. Each group contained 39 patients who were matched with regard to gender, hearing thresholds, and age. In total, 16 women and 62 men were included. The median pure tone average for 0.5, 1, and 2 kHz (PTA) was 8 dB Hearing Level (dB HL) for both the right and left ears, within a range of 0 to 120 dB HL and 0 to 48 dB HL, respectively (Figure 1). The median pure tone average for 1, 2, and 4 kHz (PTA HF) was 13 dB HL for the right ear and 15 dB HL for the left ear, varying from 0 to 120 dB HL and 0 to 55 dB HL, respectively (Figure 1). The median age of the participants was 52 years, within a range of 18 to 70 years.
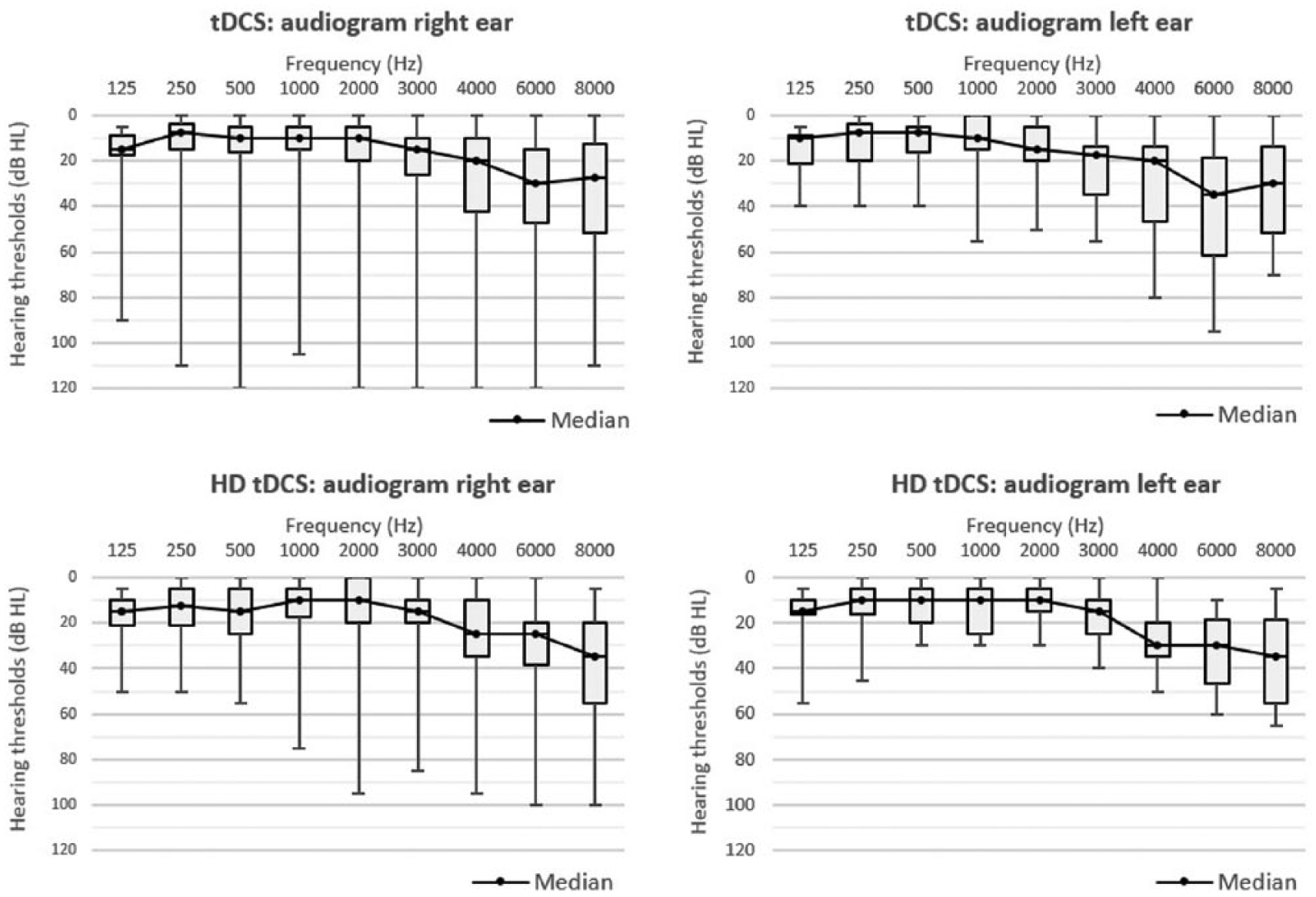
Boxplot (min,Q1,Q3,max) of the air conduction thresholds for the right and left ear of the 78 tDCS patients (upper) and of the 39 HD tDCS patients (bottom). The black solid line represents the median air conduction threshold for each frequency.
The patients of the prospective HD tDCS study and those of the retrospective tDCS study were matched with regard to gender, hearing thresholds, and age. In total, 6 women and 33 men were included in the HD tDCS study. The median PTA was 8 dB HL for the right ear and 10 dB HL for the left ear, within a range of 0 to 75 dB HL and 0 to 28 dB HL respectively (Figure 1). The median PTA HF was 15 dB HL for both right and left ears, varying from 0 to 88 dB HL and 3 to 45 dB HL, respectively (Figure 1). The median age of the participants was 52 years, within a range of 20 to 80 years.
Statistical Analysis
The objective of the first part of the study was (1) to compare the effects of 2 tDCS electrode positions—DLPFC and RSO-LTA—and (2) to determine whether the stimulation led to a significant improvement in the outcome measurements. There were 3 repeated measurements for each individual in the first part of the study, although some of the questionnaires were missing (either post or follow-up). The objective of the second part of the study was (3) to compare the effects of HD tDCS with the 2 previous tDCS electrode positions and (4) to determine whether HD tDCS stimulation led to a significant improvement in the outcome measurements. There were also 3 repeated measurements for each individual in the second part of the study.
All research questions listed above were addressed using linear mixed models to account for the nonindependence between the observations taken from the same individual. All models included a random intercept for individuals. As dependent variable, either VAS, HQ, TFI, TQ, or HADS was entered.
To test the first research question, we entered time, treatment, and their interaction as fixed effects. Significance of the interaction indicated if the change in outcome between 3 visits differed between the 2 electrode positions. A nonsignificant interaction term implied that the change in outcome over time was not significantly different between the 2 electrode positions. To test the second research question, separate models were fit for the 2 electrode positions with time as fixed effect. For all models of the third research question, we started with a model including fixed effects for time (categorical, 3 levels), therapy (=treatment, 3 levels; DLPFC tDCS, RSO-LTA tDCS, HD tDCS), and their interaction. This model was simplified using stepwise backward elimination. The fourth research question was addressed by fitting linear mixed models with time as fixed effect.
In case the effect of time was significant, a post hoc analysis with Tukey correction for multiple hypothesis testing was carried out. The significance of the fixed-effect terms was tested using an F-test with Kenwardroger correction for degrees of freedom. Across all models, the significance level was set at P ≤.05.
Part I: Retrospective tDCS Study
Transcranial Direct Current Stimulation
Each patient received 2 sessions of tDCS weekly and a total of 8 sessions (Figure 2). In the DLPFC stimulation, the anode and cathode were placed on the right and left DLPFC, respectively (Figure 3 A1), whereas in the RSO-LTA stimulation, the anode was placed on the right supraorbifrontal area and the cathode on the LTA (between C3 and T5; Figure 3 A2). Only limited evidence exists on the neurophysiological basis of tDCS. It might be that anodal tDCS of the LTA also activates surrounding cortical areas that, by inhibitory connections or competition, decrease the increased activity of tinnitus-related areas. 25 Furthermore, it has been suggested that DLPFC tDCS strengthens deficient inhibitory top-down mechanisms in tinnitus, inducing auditory sensory gating in the anterior cingulate cortex. 10 The positioning was according to the 10/20 international system for EEG electrode placement. A constant current of 2 mA was applied for 20 minutes with a fade-in and fade-out of 10 s. The direct current was transmitted by means of 2 saline-soaked pairs of surface sponge electrodes (35 cm3) and delivered by a battery-driven constant current stimulator (Neuroconn, Ilmenau, Germany), with a maximum output of 10 mA.
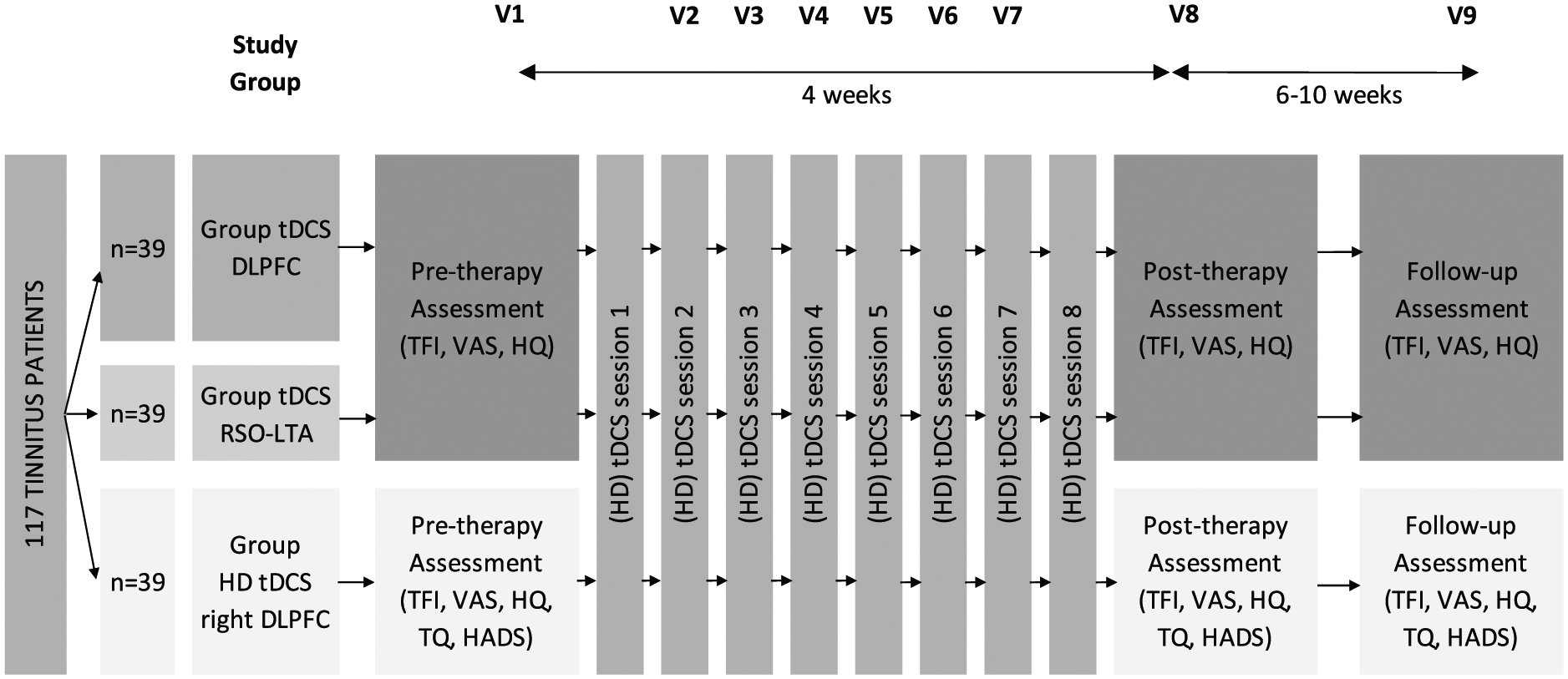
Patient flow diagram of the tDCS and HD tDCS study with each patient receiving eight sessions of tDCS or HD tDCS. Tinnitus perception is assessed at three visits: pre-therapy (V1), post-therapy (V8) and follow-up (V9).
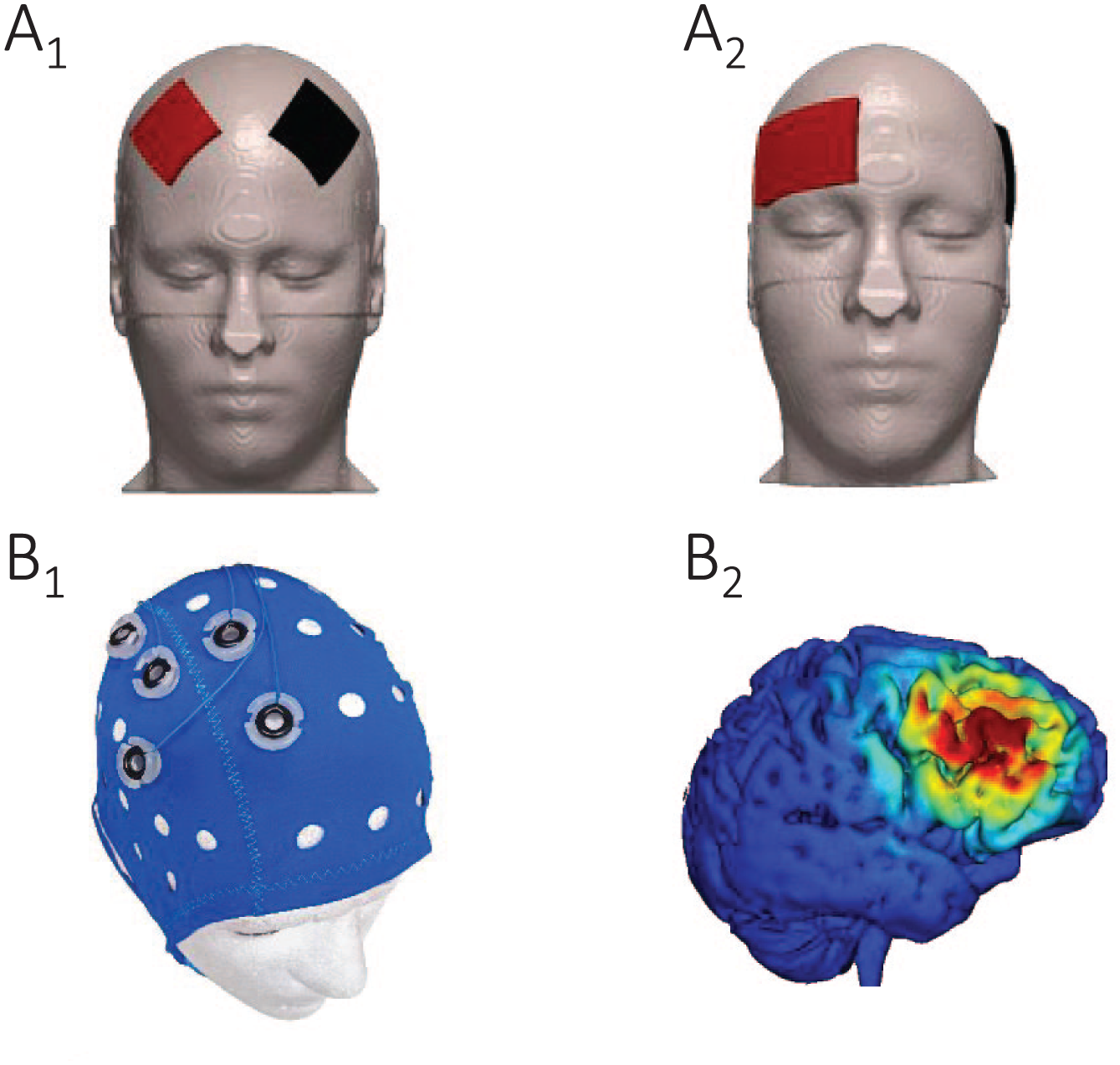
Electrode positioning of tDCS: bifrontal dorsolateral prefrontal cortex (DLPFC) (A1) and right supraorbital-left temporal area (RSO-LTA) (A2). Electrode positioning of HD tDCS at the right DLPFC (B1) and a simulation of the current flow with HD tDCS at the right DLPFC with Soterix HD-Explor TM 4 (B2).
Outcome Measurements
Tinnitus intrusiveness, tinnitus loudness, and the presence of hyperacusis were evaluated at the start of the therapy (pre), after 8 sessions of tDCS (post), and ±6 to 10 weeks poststimulation (follow-up) by means of the tinnitus functional index (TFI),26,27 VAS, 28 and the hyperacusis questionnaire (HQ; Figure 2).29,30 TFI is a self-report questionnaire consisting of 25 questions measuring the severity and negative impact of the tinnitus and is divided into 8 subscales (ie, intrusive, sense of control, cognitive, sleep, auditory, relaxation, quality of life, and emotional). The patient has to answer each question on a Likert scale from 0 to 10. One purpose of TFI is assessing treatment-related changes in tinnitus. A reduction of 13 points or more in TFI is considered as a meaningful reduction to the patient (ie, clinically significant).26,27 For VAS, patients score the mean loudness of their tinnitus on a scale from 0 to 100 with the help of a ruler, with 0 meaning no audible tinnitus and 100 indicating extremly loud. 28 When patients had bilateral tinnitus, the maximum score of both ears was taken into account for statistical analysis. HQ consists of 14 self-rating items, rating oversensitivity to sounds. Answers to each question are given on a 4-point scale, with a total score greater than 28 representing strong auditory hypersensitivity. 29
Part II: Prospective HD tDCS Study
High-Definition Transcranial Direct Current Stimulation
Each patient received 2 sessions of HD tDCS weekly and a total of 8 sessions (Figure 2). The electrodes were positioned at the right DLPFC. The positioning was according to the 10/20 international system for EEG electrode placement, with the central anode at F4 and the adjoining cathodes at F2, F6, FC4, and AF4 (Figure 3 B1 & B2). A constant current of 2 mA was applied for 20 minutes with a fade-in and fade-out of 20 s. The direct current was transmitted by means of 5 sintered silver/silver chloride (Ag/AgCl) ring electrodes with an inner radius of 6 mm and an outer radius of 12 mm and delivered by a battery-driven 1 × 1 tDCS low-intensity stimulator and 4 × 1 multichannel stimulation adaptor (Soterix Medical Inc, New York, NY), with a maximum output of 2 mA, following the guidelines for HD tDCS stimulation. 20
Outcome Measurements
The patients had to fill out the TFI,26,27 VAS, 28 HQ,29,30 tinnitus questionnaire (TQ),31,32 and hospital anxiety and depression scale (HADS)33,34 before, immediately after, and ±6 to 10 weeks after 8 sessions of HD tDCS (Figure 2). TQ scores the tinnitus handicap by assessing emotional and cognitive distress, intrusiveness, auditory perceptual difficulties, sleep disturbances, and somatic complaints using 52 self-rating questions. Answers should be given on a 3-point scale. An improvement of 10 points or more in TQ is in general considered as a clinically significant improvement. 35 HADS is a 14-item self-report screening scale using 4 answer possibilities for each question and consisting of 2 subscales: anxiety and depression. A cutoff score of 8 points or more can be used to diagnose anxiety or depression disorders. 36
Results
In general, tDCS and HD tDCS were well tolerated, yet there were fewer sensations experienced during HD tDCS. A minority of the participants complained about warmth or tingling feelings during HD tDCS.
Comparison of 2 Electrode Placements for tDCS
The effect of time was highly significant in both tDCS groups for TFI total score (DLPFC: P < .01; RSO-LTA: P < .01; Figure 4 A1 & A2). A post hoc analysis showed that TFI scores at posttherapy and follow-up were significantly better compared with pretherapy, for both stimulation sites (DLPFC post-pre: P = .02; DLPFC follow-up–pre: P < .01; RSO-LTA post-pre: P = .02; RSO-LTA follow-up–pre: P < .01), whereas the posttherapy and follow-up visit were not significantly different from each other (DLPFC follow-up–post: P = .65; RSO-LTA follow-up–post: P = .08). Moreover, 38% of the participants receiving tDCS of DLPFC and 27% of the participants receiving RSO-LTA tDCS improved clinically significantly. However, the analysis of the effect over time on VAS loudness score (DLPFC: P = .49; RSO-LTA: P = .06) and HQ score (DLPFC: P = .71; RSO-LTA: P = .31) showed no significant effects for both tDCS stimulations.
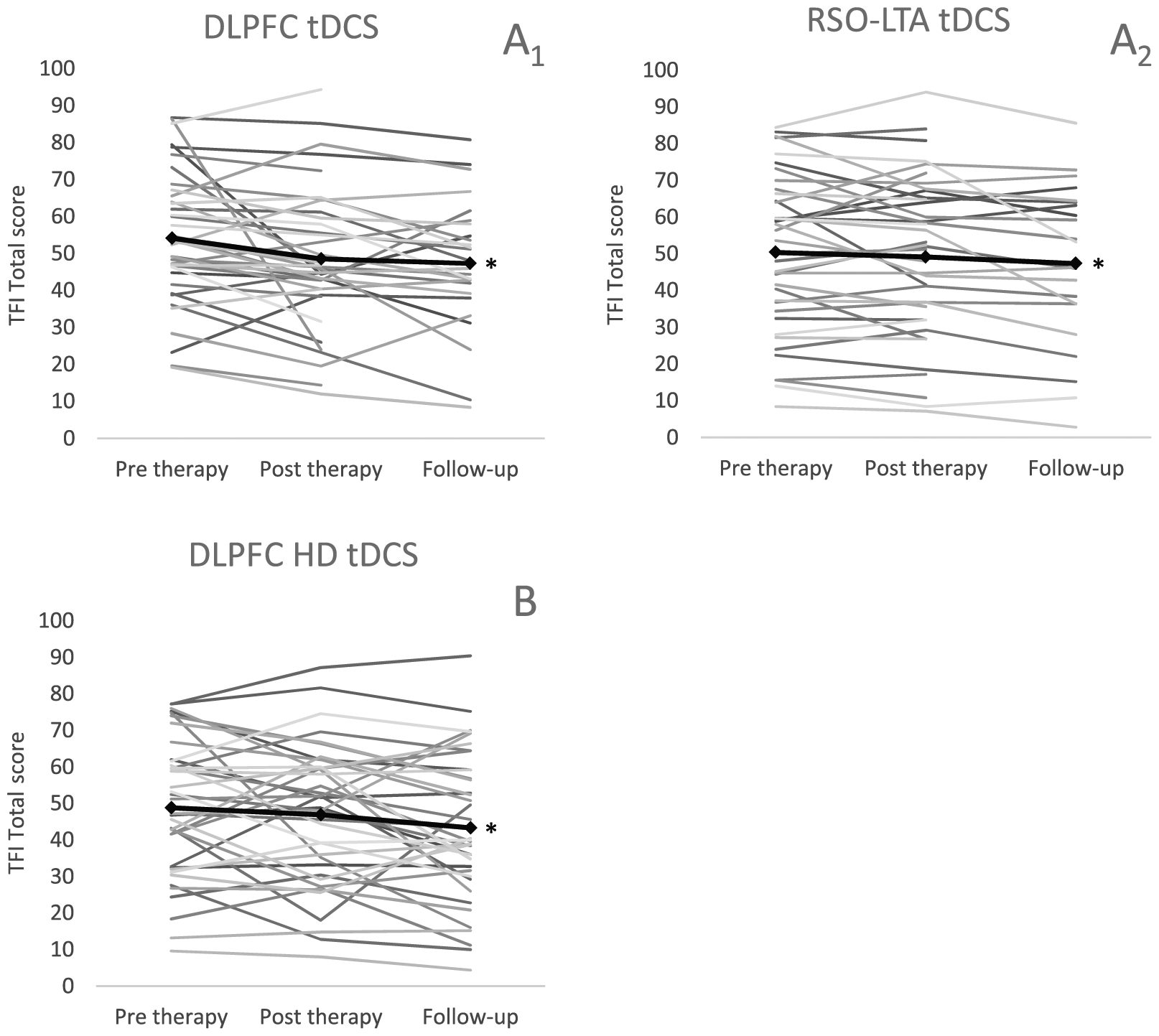
The evolution of the TFI total score over time at pre therapy (before the first tDCS session), post therapy (after the last tDCS session) and follow-up (± 6-10 week after the last tDCS session) for each individual for A1: dorsolateral prefrontal cortex (DLPFC) tDCS, A2: right supraorbital-left temporal area (RSO-LTA) tDCS (nDLPFC=39; nRSO-LTA=39) and B: for right DLPFC HD tDCS (n=39). The black solid line represents the mean TFI total score. Significant changes (p<.05) over time are indicated with an asterisk (*).
Furthermore, linear mixed model analysis showed no statistically significant interaction between electrode positioning and time with regard to TFI total score (P = .16; Figure 4), VAS loudness score (P = .07), and HQ score (P = .85). These results suggest that there was no difference in therapy effect between the 2 electrode positions.
HD tDCS of the Right DLPFC
The analysis of the therapy effect over time for HD tDCS of the right DLPFC showed a significant improvement in TFI total score (P = .05; Figure 4B). A post hoc comparison between the 3 visits revealed a significant difference between the pretherapy and follow-up visits (P = .04). Moreover, 31% of the participants showed a clinically significant improvement. On the other hand, the other outcomes (ie, TQ, VAS, HQ, HADS) did not improve significantly over time (TQ: P = .36; HADS fear: P = .42; HADS depression: P = .71; HQ: P = .56; and VAS: P = .64).
In addition to TFI and TQ total score, the subscales of these questionnaires were analyzed. First, the following TFI subscales showed a significant evolution: sense of control (P = .02), cognitive interference (P = .01), quality of life (P < .01), and emotional distress subscale (P < .01; Figure 5). Because of these subscales, TFI total score improved significantly from pretherapy to follow-up visit. Nevertheless, the sense of control subscale also differed significantly between posttherapy visit and follow-up (P = .05). Second, the TQ subscales showed no significant evolutions over time.
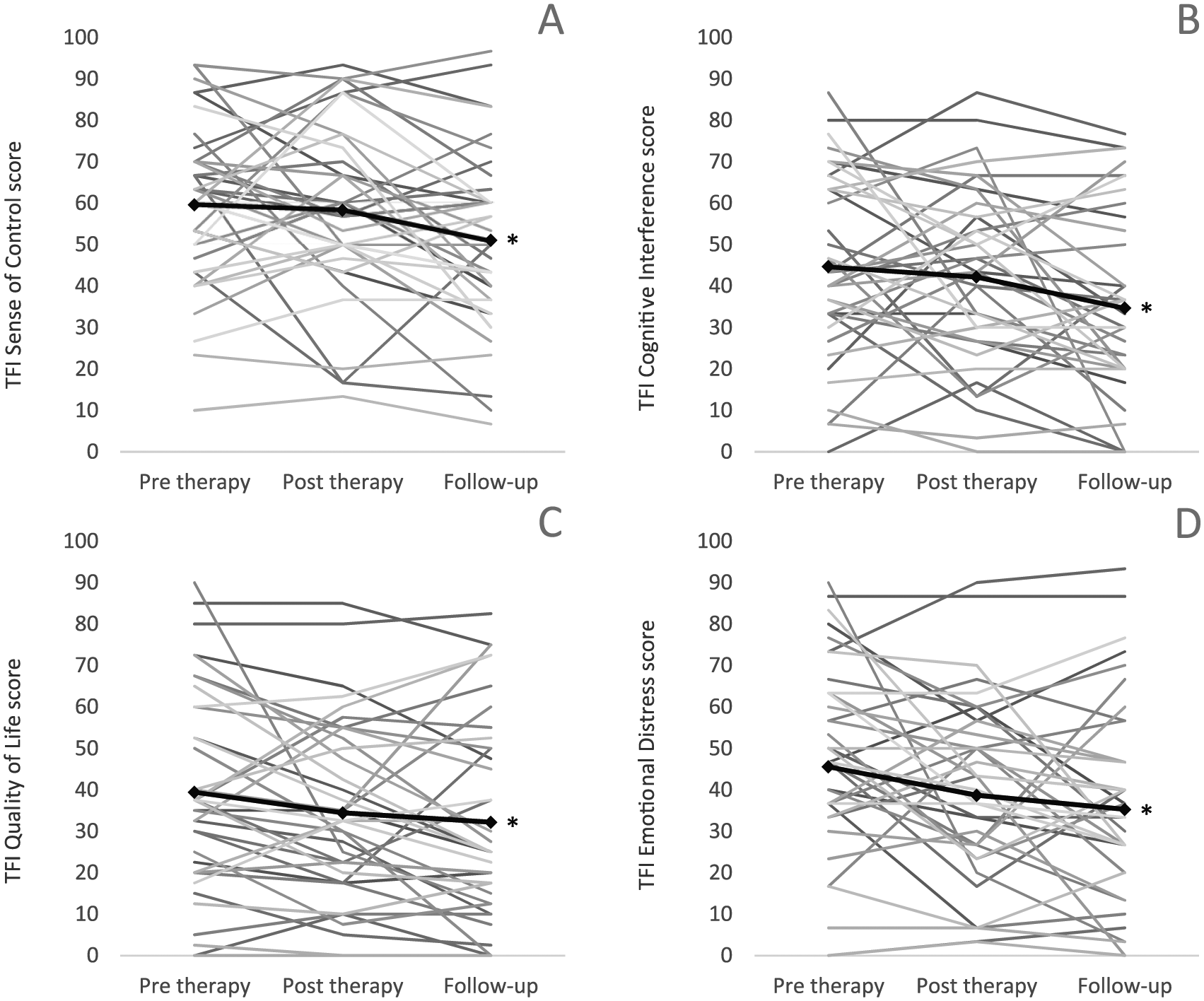
Evolution of the following TFI subscales - sense of controle (A), cognitive interference (B), quality of life (C) and emotional distress (D) - over time at pre therapy (before the first HD tDCS session), post therapy (after the last HD tDCS session) and follow-up (± 6-10 week after the last HD tDCS session) for each individual (n=39). The black solid line represents the mean TFI subscale score. Significant changes (p<.05) over time are indicated with an asterisk (*).
Comparison Between tDCS and HD tDCS
The analysis of the therapy effect over time for the 3 different stimulations (ie, tDCS DLPFC, tDCS RSO-LTA, and HD tDCS right DLPFC) showed no significant differences between these stimulation sites and/or modes with regard to TFI total score (P = .49), VAS score (P = .20), and HQ score (P = .94).
Discussion
Concerning the comparison of DLPFC and RSO-LTA tDCS, the previously mentioned systematic review by Song et al 10 concluded that there was no difference between tDCS targeting LTA and DLPFC with regard to the percentage of responders and the amount of reduction in tinnitus intensity. However, the current study aimed to perform an in-depth assessment of the therapeutic effects of 8 sessions of tDCS in the long term (ie, with 3 questionnaires filled out at 3 visits) and with matched participants. Second, the effects of the recently developed HD tDCS was explored because previous studies evaluating HD tDCS have observed inconsistent results.14,24 Finally, the therapeutic effects of tDCS and HD tDCS were compared because no data were found in the literature on the comparison between these 2 electrical stimulation treatments.
The current study showed that tDCS of DLPFC does not differ from tDCS of RSO-LTA with regard to TFI, VAS, or HQ, confirming the meta-analysis by Song et al. 10 However, both treatments resulted in a significant improvement in TFI total score, which was clinically significant in 27% to 38% of the participants. Song et al 10 focused on tinnitus loudness and demonstrated an average responder rate of 39.5%, ranging from 29.9% to 46.7%, with a mean reduction in tinnitus intensity of 13.5%, whereas the current study found no significant change in VAS for loudness. Tinnitus impact, measured with TFI, decreased significantly in the current study, in contrast to a previous study by Rabau et al, 37 in which 8 sessions of DLPFC tDCS did not render any tinnitus reduction. This inconsistenty cannot be explained by differences in study design. In the present study, tinnitus burden was altered after tDCS treatment, whereas hyperacusis sensation was not changed. An implication of this is the possibility that not all the additional symptoms, such as sound hypersensitivity, change with electrical stimulation. However, loudness of tinnitus did not change either. One of the implications of this finding that emerges is that average loudness, measured with a VAS, does not represent the mental impact of tinnitus, as measured with TFI.
The recently developed HD tDCS of right DLPFC resulted in a significant improvement in TFI total score, with a clinically significant improvement in 31% of the patients, confirming the promising results with HD tDCS.14,23 Henin et al 24 found no significant reduction in the tinnitus percept using a sham-controlled HD tDCS study, but they were not able to resolve the effects of HD tDCS with the limited sample size. Moreover, the electrode position differed slightly from previous studies, and 2 different treatments were included in each session. 24 It is interesting to note that no significant improvement in TQ score was found in the current study. A possible explanation for this might be that TQ is less sensitive to changes in tinnitus compared with TFI, possibly because of the answer possibilities. Answers to TQ should be given on a 3-point scale, ranging from true to partly true and not true, whereas TFI uses a Likert scale from 0 to 10. Another possible explanation for the lack of TQ score improvement is that TQ measures slightly different aspects of tinnitus, such as somatic complaints. Neither HADS nor HQ or VAS changed significantly after HD tDCS, similar to the previously discussed results of tDCS.
The current study compared HD tDCS with tDCS because HD tDCS appeared to be a promising therapy for tinnitus treatment. This comparison revealed no significant differences between the 2 tDCS treatments (ie, DLPFC and RSO-LTA tDCS) and HD tDCS of DLPFC. However, the application of HD tDCS has some practical advantages. First, because the electrodes are positioned in a cap according to the 10/20 international system for EEG electrode placement (Figure 3 B1), the clinician can easily administer the stimulation to the targeted area. Second, patients complain less about undesired sensations caused by HD tDCS compared with tDCS. Nevertheless, a comparison of these 2 techniques in the same group of tinnitus patients would be beneficial.
The limitations of the current study need to be acknowledged, most notably the absence of a sham arm. Therefore, the results must be interpreted with caution. The decreased tinnitus can be attributed to a placebo effect. Yet Shekhawat and Vanneste 23 showed a significant effect of HD tDCS of DLPFC in a double-blind, sham-controlled, randomized trial. The systematic review by Song et al, 10 which also showed a significant effect of tDCS, was limited to sham-controlled studies. In addition to the previously discussed studies, other sham-controlled studies have not indicated an effect of sham tDCS compared with actual tDCS.3,38,39 Moreover, a delayed-start group of cervical physical therapy for tinnitus did not improve on TFI total score during a 6-week wait-and-see period in a study of Michiels et al, 40 indicating no spontaneous improvement of tinnitus perception. Further research should include a control group to rule out the placebo effect and reveal the real effect of tDCS and particularly HD tDCS. Moreover, previous studies consistently indicated changes in tinnitus loudness after electrical neuromodulation, whereas the current study did not reach significance for that aspect of tinnitus. This rather contradictory result may be a result of the fact that questionnaires were filled out at fixed time points by use of a computer, meaning that there was no interference by the researcher. In many other studies, VAS was taken as an outcome measure often directly questioned by the researcher straight after intervention, possibly leading toward bias. Although there was a lack of improvement in VAS, the disturbance caused by the tinnitus, which did improve in the current study, is also an important reason why patients request help. Finally, the comparison of tDCS and HD tDCS may be limited by the combination of 2 studies and, thus, the current study not being a randomized study. However, this was partly overcome by matching the participants of the 2 studies.
For future research, we recommend investigation of the long-term effects of tDCS and HD tDCS on tinnitus perception. Furthermore, it would be interesting to conduct neuromodulation trials with multiple locations and different transcranial electrical stimulation techniques, such as the little-studied technique, transcranial random noise stimulation.41-43 Moreover, a sham-controlled, double-blind and randomized study of HD tDCS would be of great value in the research of tinnitus treatment. Finally, case-controlled trials for tinnitus treatment would be beneficial for the field because of the heterogeneity in tinnitus. Subtyping of different forms of tinnitus will, thus, be an important issue in future research.
Conclusions
Conventional tDCS and HD tDCS are investigated and compared in the current study. Both therapies are safe and well-tolerated stimulation techniques. HD tDCS of right DLPFC, RSO-LTA tDCS, and DLPFC tDCS result in significant improvements in TFI total score, being clinically significant in 31%, 27%, 38% of the therapy groups, respectively. There is no significant difference between the 3 stimulations with regard to changes in tinnitus perception. However, HD tDCS has practical advantages for the administration. Because of the absence of a sham arm, the results need to be intepreted with caution. Further research is required to control for a possible placebo effect.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.