
Abstract
Background. Perception of sound in the absence of an external auditory source is called tinnitus, which may negatively affect quality of life. Anodal transcranial direct current stimulation (tDCS) of the left temporoparietal area (LTA) was explored for tinnitus relief. Objective. This pilot study examined tDCS dose (current intensity and duration) and response effects for tinnitus suppression. Methods. Twenty-five participants with chronic tinnitus and a mean age of 54 years took part. Anodal tDCS of LTA was carried out. Current intensity (1 mA and 2 mA) and duration (10 minutes, 15 minutes, and 20 minutes) were varied and their impact on tinnitus measured. Results. tDCS was well tolerated. Fifty-six percent of participants (14) experienced transient suppression of tinnitus, and 44% of participants (11) experienced long-term improvement of symptoms (overnight—less annoyance, more relaxed, and better sleep). There was an interaction between duration and intensity of the stimulus on the change in rated loudness of tinnitus, F(2, 48) = 4.355, P = .018, and clinical global improvement score, F(2, 48) = 3.193, P = .050, after stimulation. Conclusions. Current intensity of 2 mA for 20 minutes was the more effective stimulus parameter for anodal tDCS of LTA. tDCS can be a potential clinical tool for reduction of tinnitus, although longer term trials are needed.
Introduction
Perception of sound in the absence of an external auditory source is called tinnitus. In the United States, approximately 50 million people experience some form of tinnitus and 16 million experience frequent tinnitus. 1 It can lead to anger, frustration, tension, poor communication, and lack of sleep2,3 and can have a devastating impact on overall quality of life.4,5 The underlying mechanisms of tinnitus and its most effective treatment are as yet unresolved. 6
In the past 5 years, attention has been drawn toward the use of noninvasive brain stimulation for tinnitus management.6-8 The history of noninvasive electrical brain stimulation dates back to 43
More recently, the effects of noninvasive transcranial direct current stimulation (tDCS) have been explored in humans, in both healthy and neurological populations. Depending on the polarity of the stimulation, tDCS can increase or decrease the excitability of the underlying cortex. Anodal stimulation increases excitability due to neuronal depolarization, and cathodal stimulation decreases excitability due to neuronal hyperpolarization.12-14 It is postulated that the after effects of tDCS could possibly be due to change in intracortical inhibition or facilitation, which is controlled by synaptic activity. 15
Not all of the current applied at the scalp reaches the cortex, some of it is shunted through the scalp tissue and cerebrospinal fluid; the balance reaches the brain.14,16 Miranda and colleagues 17 modeled the current distribution during tDCS and found that based on the location, size, and number of electrodes used, the percentage of current reaching the brain varied from 39% to 59%. Whereas tDCS might potentially be a powerful strategy for tinnitus intervention,7,18,19 it requires optimization of stimulation parameters. 6 As yet there is no consensus as to the optimal parameters for tinnitus modulation using tDCS (Table 1).
Research Studies Using tDCS for Tinnitus Management
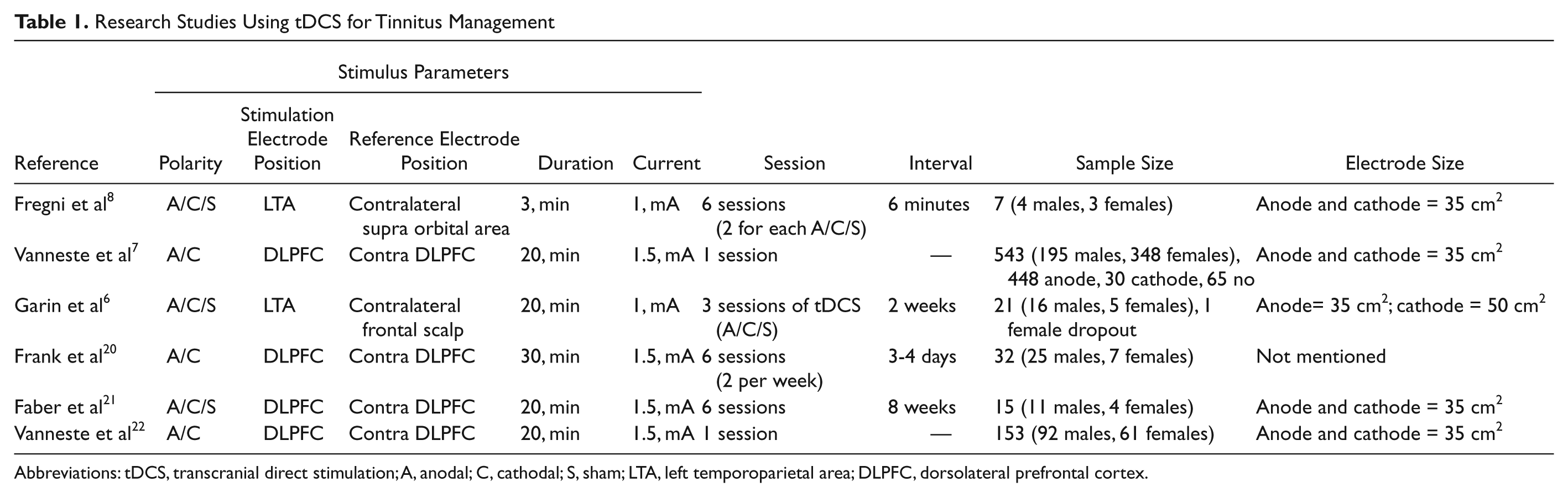
Abbreviations: tDCS, transcranial direct stimulation; A, anodal; C, cathodal; S, sham; LTA, left temporoparietal area; DLPFC, dorsolateral prefrontal cortex.
Anodal tDCS of the left temporoparietal area (LTA) and dorsolateral prefrontal cortex (DLPFC) are potentially the most favorable polarity and sites of stimulation for tinnitus relief.6-8,20-22 tDCS of LTA results in more widespread diffused impact on cortical areas larger than the target region. However, tDCS of DLPFC results in a more localized impact on the target region itself. 23 Since tinnitus can have widespread underlying causes, 20 LTA was chosen as the site of stimulation for this study.
There have been few if any dose–response studies in tDCS. 24 The aim of the present study was to explore tDCS dose (current intensity and duration) response effects for tinnitus suppression for LTA stimulation. Anodal tDCS of the LTA has led to transient suppression of tinnitus in 42% 8 and 35% 6 of participants. A comparatively long-lasting impact on tinnitus perception, lasting up to a few days, was observed in a recent double-blind, sham-controlled study conducted by Garin et al, 6 where the duration of tDCS was 20 minutes with 1 mA current intensity. Anodal tDCS produced more favorable effects compared with cathodal or sham tDCS. Compared with previous work,7,8 this study had a longer interval between tDCS sessions (2 weeks), and the size of the reference electrode was larger than the stimulating electrode (Table 1). Vanneste and colleagues 7 explored whether tDCS of DLPFC would lead to tinnitus suppression. They used a slightly higher current intensity (1.5 mA) than other authors6,8 and reported a 29.9% positive response rate with bifrontal tDCS (anode on the right DLPFC and cathode on the left DLPFC).
The primary goal of the present study was to optimize parameters for anodal tDCS of LTA. We selected anodal stimulation for investigation, as previous studies have established that anodal tDCS is more effective in tinnitus suppression than cathodal or sham.6,8 We investigated 6 combinations of stimulus intensity and duration, in order to optimize these tDCS parameters for future studies. This is one of the first studies to evaluate the effects of a 2 mA current intensity on tinnitus symptoms.
Methods
Participants
Participants were recruited through the University of Auckland Hearing and Tinnitus Clinic. Volunteers were eligible for inclusion if they were aged at least 18 years and had experienced bothersome tinnitus for at least 18 months. Volunteers were excluded if they had any contraindications to tDCS, such as previous brain surgery, metal or electronic implants, pregnancy, and a history of seizures as determined by a neurologist. Each participant provided written informed consent in accordance with the Declaration of Helsinki, and this study was approved by the University of Auckland human participant’s ethics committee.
Twenty-five participants with a mean age of 54 years (range, 28-78 years) completed the experiment. There were 8 females (32%) and 17 males (68%) with mean Tinnitus Functional Index 25 score of 47.76 (SD, 20.94). All participants had chronic bothersome tinnitus lasting for at least 18 months, with average tinnitus duration of 16.18 years (ranging from 1.5 to 54 years). Twenty-one participants had bilateral tinnitus and 4 had unilateral tinnitus (3 left sided and 1 right sided). Two participants had normal hearing sensitivity and 23 had hearing loss. Tinnitus quality was documented for each participant, and 25.9% rated it as hissing, 22.9% as ringing, 17.1% as buzzing, 11.4% as high pitch whistling, and 22.9% as other qualities (see Table 2).
Participant Characteristics
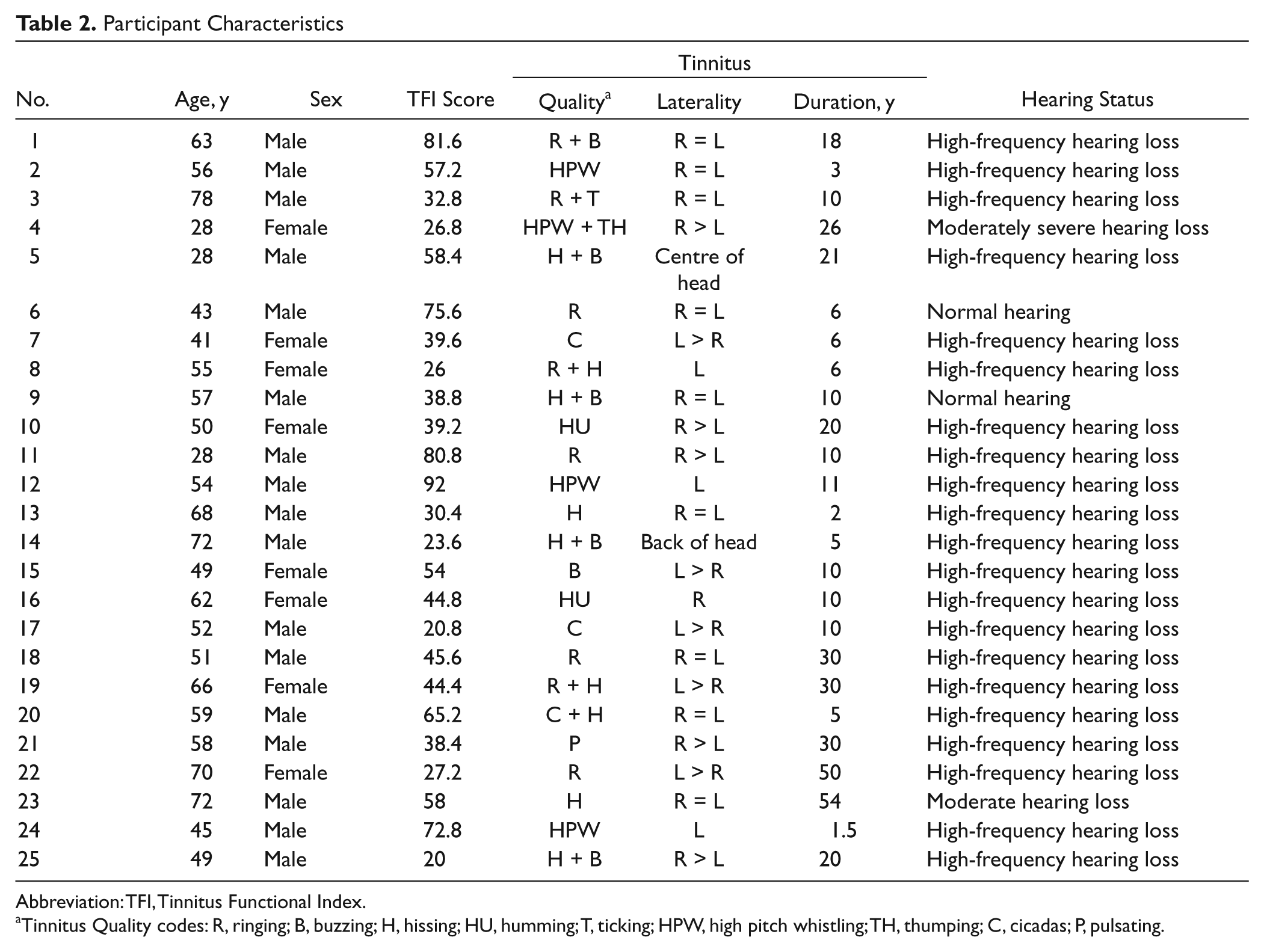
Abbreviation: TFI, Tinnitus Functional Index.
Tinnitus Quality codes: R, ringing; B, buzzing; H, hissing; HU, humming; T, ticking; HPW, high pitch whistling; TH, thumping; C, cicadas; P, pulsating.
Procedure
Experiments were conducted in a sound-treated room (ISO 8253-1:2010). Six combinations of stimulus intensity and duration were used in the following incremental order: 1 mA for 10 minutes, 15 minutes, and 20 minutes followed by 2 mA for 10 minutes, 15 minutes, and 20 minutes. In total, each participant received 6 tDCS stimulations. Participants were blinded to the intensity and duration of the stimulation and were told that the 6 settings would be presented randomly and these could suppress, elevate, or have no effect on their tinnitus. Each participant rated their tinnitus twice before stimulation and twice after each tDCS stimulation. The first rating was immediately after stimulation and the second rating 10 minutes after the first rating. The rationale for doing the rating twice before stimulation was to document the effect of change in environment (day-to-day environment to sound treated room) on the tinnitus. The second rating, after arriving in the sound-treated room, was used as the baseline measure to compare with poststimulation ratings. Tinnitus suppression was defined as a minimum 1 point decrease in a 10-point Loudness-Visual Analogue Scale. If, following stimulation, no tinnitus suppression was observed, participants received the next stimulation following a 10-minute break (up to a maximum of all 6 stimulations in 1 session). If total tinnitus suppression was obtained (defined as not able to hear tinnitus at all), participants returned for the next stimulation a minimum of 24 hours following the previous stimulation (to allow for an extinction of effect; see Figure 1).
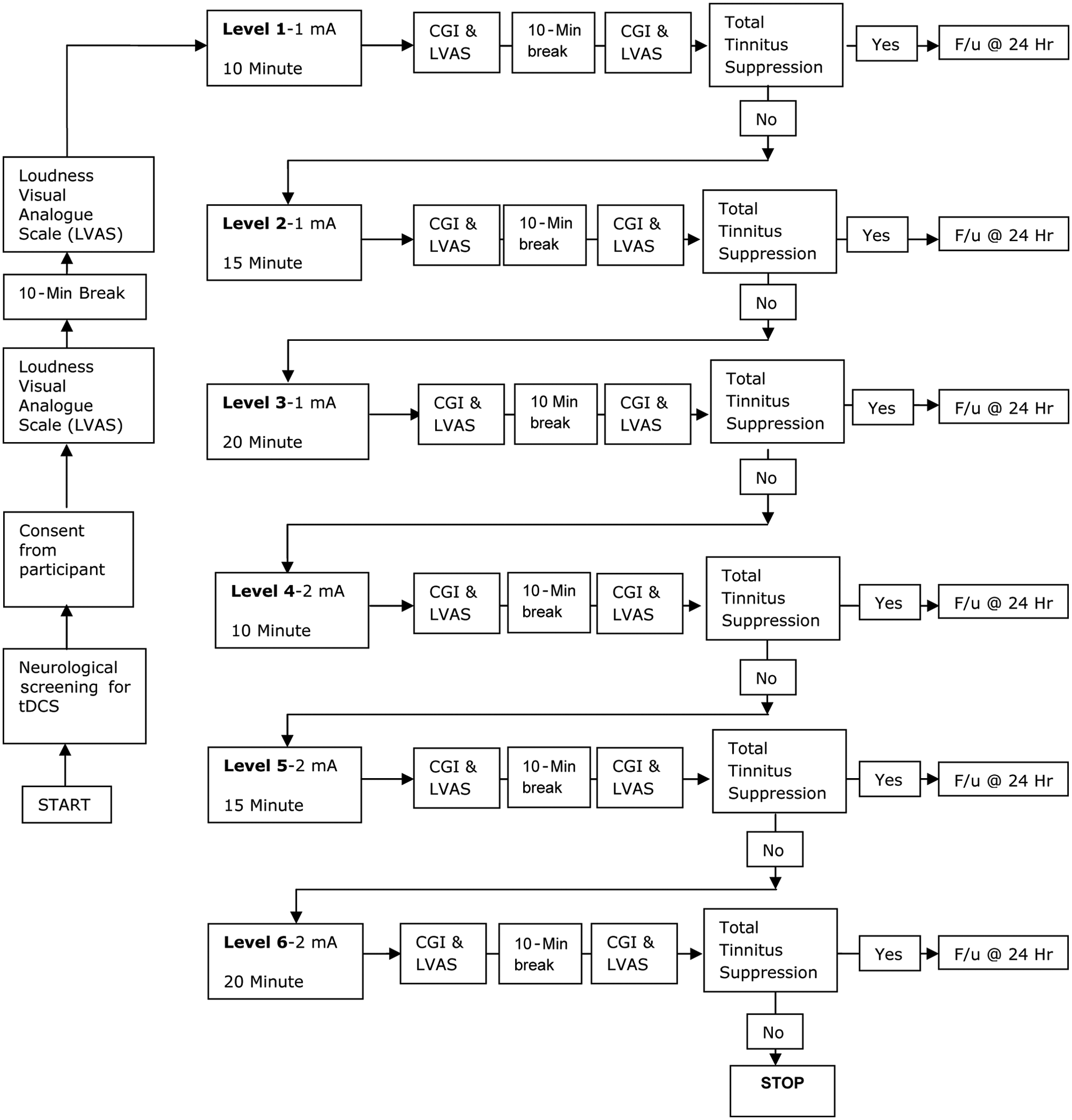
Protocol used for tDCS. Abbreviations: tDCS, transcranial direct current stimulation; CGI, Clinical Global Impression; LVAS, Loudness Visual Analogue Scale.
Clinical Evaluation
A Clinical Global Improvement (CGI) measure 26 was used to assess the total change in tinnitus complaint compared with before stimulation. The CGI is a 7-point rating scale where 4 is No change, 3 is Minimally better, 2 is Much better, 1 is Very much better, 5 is Minimally worse, 6 is Much worse, and 7 is Very much worse. A loudness measurement of tinnitus was made with a 10-point Loudness Visual Analogue Rating Scale, 27 where 1 to 10 represented a spectrum of tinnitus from very quiet (1) to very loud (10). Patient-reported ratings and any incidental observations were recorded after every stimulation.
Transcranial Direct Current Stimulation
tDCS was applied in accordance with the recommendations of international guidelines.28-30 A NeuroConn DC stimulator (Germany) was used for all procedures. The rubber electrodes had a surface area of 35 cm2 (anode) and 50 cm2 (cathode) as a smaller stimulating electrode can lead to a more focused stimulation area and a larger reference electrode has minimal physiological effects. 31 Electrode sponges were soaked in NaCl solution (0.85%) based on Dundas et al. 32 The anode was placed at LTA and the cathode was placed at the contralateral frontal scalp. These locations were identified using the international 10-20 system. LTA was defined as being the halfway point between C3 and T5.8,33 The contralateral frontal scalp site was defined as being halfway between F8 and T4. 6 All stimulation protocols included a fade in/out time of 8 seconds. Impedance and voltage were monitored and maintained <6 kΩ and <6 V, respectively, across all the stimulation settings used.
Data Analysis
The CGI ratings and the change in tinnitus loudness rating were analyzed using SPSS software. Tinnitus Loudness Visual Analogue Scale rating and CGI scores were analyzed using 2 separate 3-way repeated-measures analyses of variance (ANOVAs) with current intensity (1 mA, 2 mA), stimulation duration (10 minutes, 15 minutes, and 20 minutes), and time (immediately and 10 minutes after stimulation) as the factors. A criterion for statistical significance of .05 was chosen. Where significant interaction effects were detected, post hoc comparisons were made using 2-tailed paired t tests. No attempt was made to control the type 1 error rate for repeated comparisons. Mauchly test for sphericity was performed to validate interactions between current intensity, stimulation duration, CGI score, and rated loudness of tinnitus.
Results
tDCS was very well tolerated by all participants. Mild headache was reported by 2 participants after first stimulation (1 mA current intensity and 10 minutes duration). We assumed this was because of tension in the Velcro straps, as the headache resolved within 15 minutes of readjusting the Velcro straps and participants did not experience it further with the rest of the stimulations.
Fourteen (56%) out of 25 participants experienced a transient suppression in tinnitus loudness (Figure 2). This suppression was compared with a reference loudness rating obtained in the sound-treated room by participants 10 minutes after arrival. For this study suppression in tinnitus loudness was defined as a minimum 1-point decrease in the Visual Analogue Scale loudness rating of tinnitus.7,8
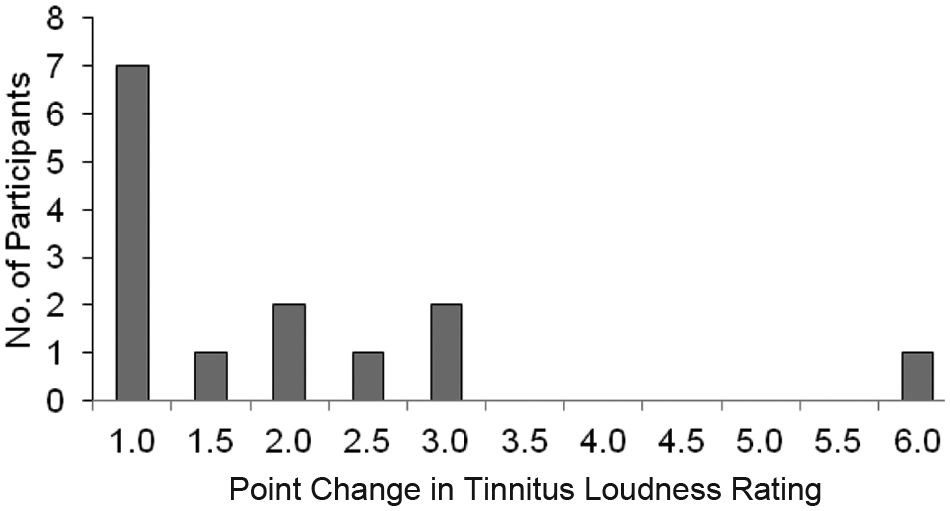
Point change in the loudness rating of participants (14 participants out of 25, remaining 11 participants did not experience any change). Point changes were collapsed across both intensities and all durations.
The majority of participants (13) reported a 3-point or less suppression in tinnitus, 1 participant reported a 6-point suppression on the Loudness Visual Analogue Scale. The mean loudness rating before treatment was 5.9 (SD = 2.2), and after 1 mA, 10 minutes stimulation the rating was 6.1 (SD = 2.3); 1 mA, 15 minutes stimulation 5.8 (SD = 2.3); 1 mA, 20 minutes stimulation 5.7 (SD = 2.3); 2 mA, 10 minutes stimulation 5.5 (SD = 2.2); 2 mA, 15 minutes stimulation 5.2 (SD = 2.1); and 2 mA, 20 minutes stimulation 5 (SD = 2.2).
Longer term (24 hours) improvement of tinnitus symptoms was reported by 11 participants, 10 reported no change, and 4 reported worsening of their tinnitus symptoms (report by emails from participants). The beneficial effects were described as “less annoyance of tinnitus,” “more relaxation,” and “good sleep during the night.” Four participants reported negative effects; they felt the tinnitus was more annoying, obvious, and loud. An important point to note is that both the positive and negative effects lasted only for 24 hours.
Two separate 3-way repeated-measures ANOVAs were used to investigate tinnitus Loudness Visual Analogue Scale ratings and CGI scores. Mauchly test for sphericity indicated that the sphericity assumption of the repeated-measures ANOVA was met. There was an interaction between duration and intensity of the stimulus on the change in the rated loudness of tinnitus after stimulation, F(2, 48) = 4.355, P = .018 (Figure 3A), and CGI score, F(2, 48) = 3.193, P = .050 (Figure 3B). The maximum amount of loudness change was observed following 2 mA stimuli for 20 minutes. There was no 3-way interaction between duration, intensity, and time, F(2, 48) = 0.673, P = .472.
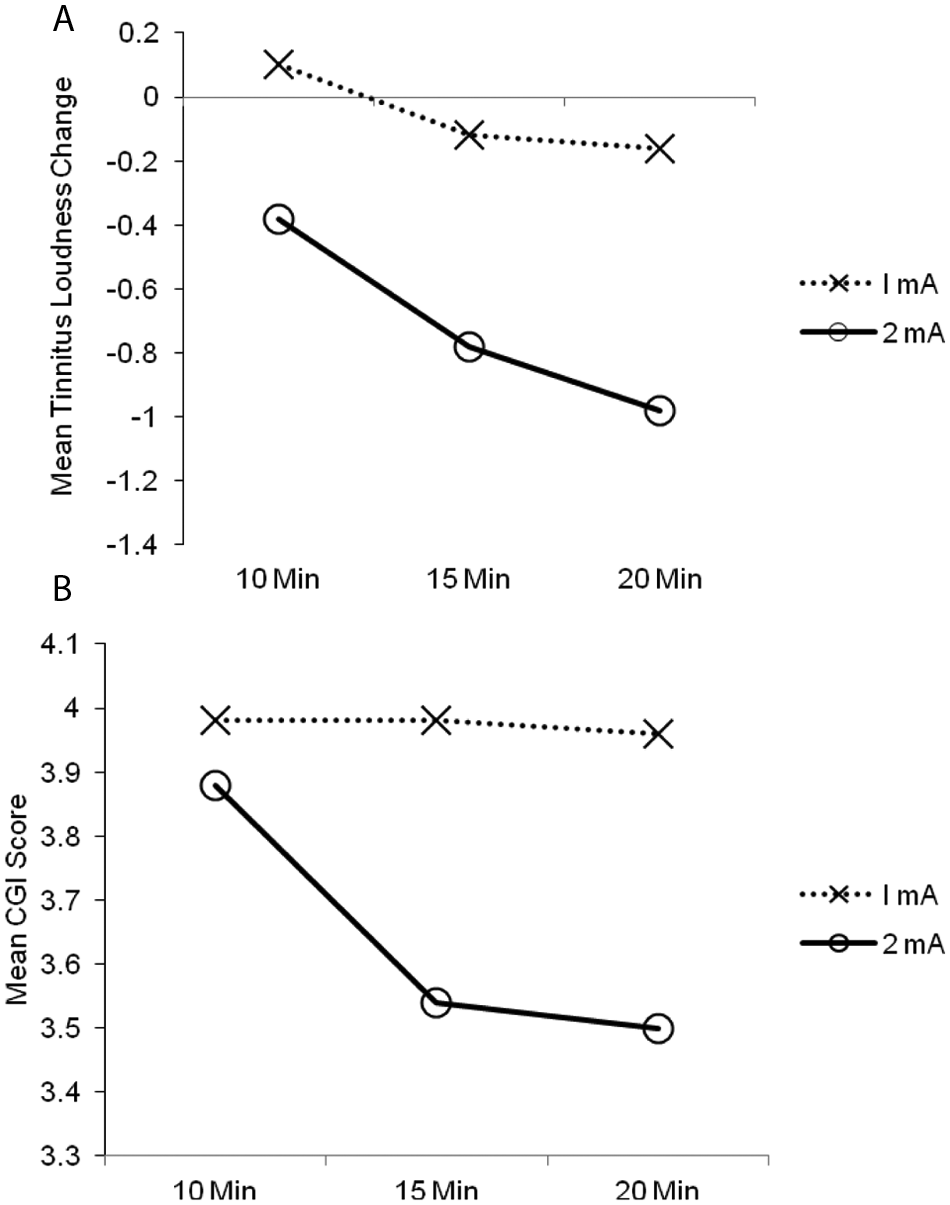
(A) Interaction between duration and intensity for Tinnitus Loudness score change. (B) Interaction between duration and intensity for CGI score change. Abbreviation: CGI, Clinical Global Impression.
A stimulus intensity of 2 mA delivered for 15 minutes and 20 minutes led to a greater decrease in CGI scores than a 1 mA stimulus intensity of any duration (10, 15, 20 minutes) and a 2 mA stimulus intensity for 10 minutes. There was a significant difference between CGI scores with 2 mA for 10 minutes and 2 mA for 15 and 20 minutes (P < .05). There was no 3-way interaction between duration, intensity, and time, F(2, 48) = 0.842, P = .437.
There was marginal, but nonsignificant, evidence of an interaction between long-term improvement of tinnitus symptoms (overnight) and duration of stimuli, F(2, 46) = 2.943, P = .063; (Figure 4A). Overnight improvement in tinnitus appeared to be associated with the longer duration settings of tDCS. The participants who experienced a greater effect of the tDCS in the short term (0-10 minutes) were also those whose tinnitus improved in the longer term (Figure 4B).
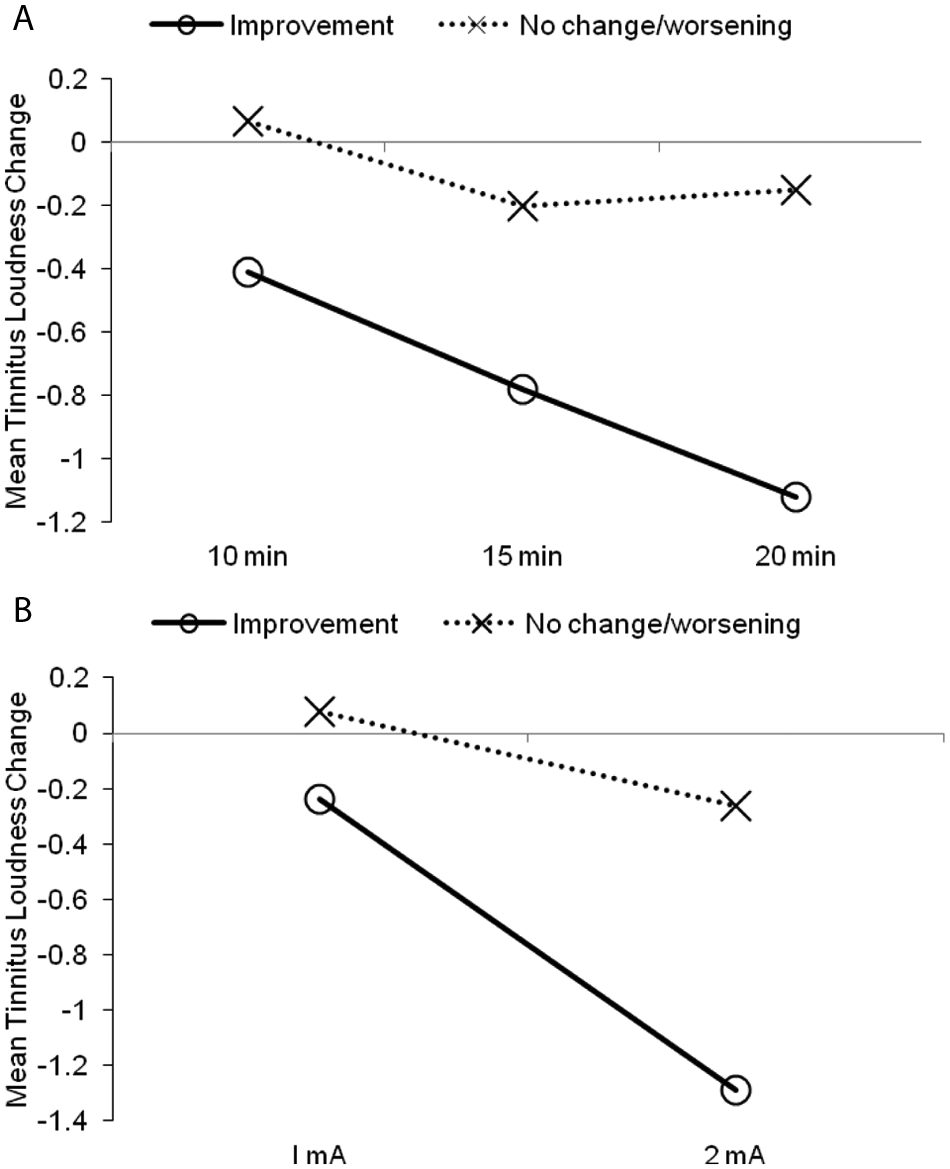
(A) Interaction between tDCS duration and long-term improvement of tinnitus symptoms (overnight) collapsed across intensity. (B) Interaction between tDCS intensity and long-term improvement of tinnitus symptoms (overnight). Abbreviation: tDCS, transcranial direct current stimulation. The 11 participants who experienced overnight positive impact were in the “improvement” group, and the “no change/worsening” group comprised 4 participants who experienced worsening of tinnitus symptoms and 10 participants who did not experience any change overnight.
Discussion
This study is one of the first attempts to optimize tDCS parameters (intensity and duration) for tinnitus suppression and the first to evaluate the effects of a 2 mA current intensity on tinnitus symptoms. The positive response rates in previous studies investigating LTA as stimulation site were 42% 8 and 35%. 6 A slightly higher positive response rate (56%) was obtained in the present study, possibly because a higher current intensity (2 mA) was used. The present results indicate that higher intensity and longer duration anodal tDCS of LTA (2 mA and 20 minutes) more effectively suppressed tinnitus symptoms than lower intensity stimulation of any duration (1 mA for 10 minutes, 15 minutes, and 20 minutes). Longer term (overnight) effects were also observed following stimulation: 11 participants reported less annoyance, more relaxation, and good sleep; 4 participants felt that they were more aware of their tinnitus and found it to be louder than usual. Interestingly, all participants experiencing positive or negative effects reported a return to baseline after 24 hours. This is in contrast to a previous study reporting transient tinnitus suppression for several days in some participants, 6 a result that could be attributed to the altered plasticity induced by tDCS; however, the exact mechanism remains to be determined.
The present study supports LTA as an effective site of stimulation for tinnitus. Underneath the LTA lies a neural network that plays a significant role in tinnitus perception such as Brodmann areas (BA) 41, 42 (primary auditory cortex), BA areas 21, 22 (auditory association areas), and part of the limbic system (amygdala and hippocampus).34-36 A possible explanation for transient suppression of tinnitus by tDCS could be that depolarization of neurons at the various cortical and subcortical structures facilitate a reduction in abnormal hyperactivity in the cortex via inhibitory networks and competition, 8 and once the impact of stimulation fades away the tinnitus comes back to its usual state. It is likely that the current flow through LTA toward the contralateral frontal site has a widespread impact on various cortical and subcortical structures (eg, the para limbic system and subcallosal areas, which play a role in long-term habituation to tinnitus 37 ).
Another interesting point for consideration is that if higher intensity stimulation leads to better results, could current intensities higher than 2 mA be used? A review of studies since 1998 using tDCS in humans across various clinical conditions found that none used a current intensity of greater than 2 mA. 24 Hence, the current intensity chosen in this study did not exceed 2 mA. Use of current higher than 2 mA would require a preparatory investigation of safety issues, which was beyond the scope of this study.
Potential Limitations
The washout period between the stimulation sessions was 10 minutes, which may not have completely eliminated the impact of previous stimulation. It is therefore not possible to rule out a cumulative impact of brain stimulation on tinnitus perception. A relatively large electrode (50 cm2, cathode) was used on the contralateral frontal scalp; it is possible that this electrode site provided stimulation at a high (2 mA) dose. Although a physiological effect cannot be completely ruled out, it is hypothesized to be minimal compared with the intended stimulation site.
Another potential limitation is that no sham control was used. Patients were told before the stimulation that it could suppress, elevate, or have no effect on their tinnitus. They were told that 6 different tDCS settings will be randomly used to study the impact of those settings. If suppression were a placebo effect, it would be reasonable to expect that participants would have reported changes with the first stimulation settings as well as last; however, we did not observe any perceptual change with the initial settings of tDCS, and there was no evidence that participants could distinguish low-dose tDCS from high-dose tDCS. The majority of the positive effects were observed with higher intensity and longer durations of stimulation. Further sham-controlled trials of tDCS use in tinnitus are desirable.
Conclusion
The current study reveals that anodal tDCS of LTA using a 2 mA current intensity delivered for 20 minutes was the most effective combination of tDCS parameters for transient suppression of tinnitus. tDCS can be a potential clinical tool for patients with tinnitus although more research is needed in this area.
Footnotes
Acknowledgements
We would like to thank Professor Alan Barber for neurological screening of participants and Dr David Welch for statistical support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to thank the Neurological Foundation of New Zealand for a small project grant.