
Abstract
Background. Most people with long-term spinal cord injury (SCI) have a very inactive lifestyle. Higher activity levels have been associated with health benefits and enhanced quality of life. Consequently, encouraging an active lifestyle is important and behavioral interventions are needed to establish durable lifestyle changes. Objective. The Healthy Active Behavioral Intervention in SCI (HABITS) study was aimed to evaluate the effectiveness of a structured self-management intervention to promote an active lifestyle in inactive persons with long-term SCI. Methods. This assessor-blinded randomized controlled trial was conducted at 4 specialized SCI units in the Netherlands. Sixty-four individuals with long-term SCI (>10 years), wheelchair-user and physically inactive, were included. Participants were randomized to either a 16-week self-management intervention consisting of group meetings and individual counseling and a book, or to a control group that only received information about active lifestyle by one group meeting and a book. Measurements were performed at baseline, 16 weeks, and 42 weeks. Primary outcome measures were self-reported physical activity and minutes per day spent in wheelchair driving. Secondary outcomes included perceived behavioral control (exercise self-efficacy, proactive coping), stages of change concerning exercise, and attitude toward exercise. Results. Mixed models analyses adjusted for age, sex, level of SCI, time since injury, baseline body mass index, and location did not show significant differences between the intervention and control groups on the primary and secondary outcomes (P ≥ .05). Conclusions. A structured 16-week self-management intervention was not effective to change behavior toward a more active lifestyle and to improve perceived behavioral control, stages of change, and attitude.
Introduction
An inactive lifestyle is a well-known and serious problem in the general population, and even more in people with spinal cord injury (SCI). Compared with able-bodied individuals and individuals with other chronic disorders, individuals with SCI show the lowest levels of physical activity.1,2 An inactive lifestyle has been associated with deconditioning and secondary health conditions (SHCs) in persons with long-term SCI,3-5 whereas higher activity levels have been associated with the reduction and prevention of SHCs and other physiological and psychological benefits.4-6 Just like the prevention of pressure sores, maintaining a physically active lifestyle should therefore be considered part of the day-to-day self-management in individuals with a long-term SCI. Self-management refers to the individual’s ability to manage the symptoms, treatment, physical and psychosocial consequences, and lifestyle changes inherent in living with a chronic condition. Effective self-management has been shown to be associated with more physical activity in individuals with chronic conditions other than SCI.7,8
Several interventions to increase or maintain levels of physical activity in persons with SCI have been evaluated. For example, Hicks et al reviewed exercise training interventions in SCI, which showed to improve physical capacity but were not aimed to increase into a more active lifestyle. 9 Other studies focused on providing information or education about the importance of an active lifestyle in SCI; they resulted in knowledge transfer but did not facilitate a behavioral change toward an active lifestyle.10,11
Behavioral interventions toward a more active lifestyle might therefore be needed to achieve a sustainable increase of physical activity. Several behavioral interventions aimed at enhancing physical activity have been evaluated in individuals with SCI, including telephone counseling, multistrategy behavioral interventions, and guided and counseled home exercise programs.12-18 These studies provided some support for these interventions to increase physical activity levels, but these studies did not include a control group,13,14,16 or focused on specific intervention characteristics, such as the added value of coping planning 15 or level of support. 12 Nooijen et al 18 showed positive results in a randomized controlled trial (RCT) of a behavioral intervention on physical activity levels in SCI. However, their study included people with subacute SCI, and the other studies were neither specifically aimed at individuals with a long-term SCI.18-21
Behavioral interventions are probably more effective if they incorporate different types of behavioral and active learning strategies. 21 Such multifaceted behavioral interventions have shown to be effective in preventing health problems and in modifying behavior, in both people with recent SCI and persons with other chronic disorders, but they have not been evaluated in persons with long-term SCI.18-21
Therefore, the aim of the Healthy Active Behavioral Intervention in SCI (HABITS) study was to evaluate the effectiveness of a structured self-management intervention on an active and healthy lifestyle measured by physical activity, perceived behavior control, stages of exercise change, and attitude in persons with long-term SCI. It is hypothesized that this intervention will show beneficial effects on an active and healthy lifestyle. Additionally, the effects on perceived behavioral control (exercise self-efficacy, proactive coping), stages of change concerning exercise, and attitude toward exercise were assessed, as well as the effects on the more remote outcomes such as secondary health complications, social support, and participation.
Methods
Design and Overview
This study was a multicenter RCT. Details of the methods and design have been reported elsewhere. 22 Four rehabilitation centers with a specialized SCI unit across the Netherlands participated this study. The intervention group received the 16-week self-management intervention. The control group received information about the importance and maintenance of an active lifestyle only.
Setting and Participants
Adults with SCI were eligible for this study if they met the following criteria: age at injury was 18 years or above; time since injury at least 10 years; current age between 28 and 65 years; able to use a hand-rim wheelchair; and physically inactive as defined by a Physical Activity Scale for Individuals With Physical Disabilities (PASIPD) score lower than the 75th percentile of a Dutch SCI population. 23 Potential participants were excluded from the study if they had no intention to change their exercise behavior in the next 6 months; a progressive disease or severe comorbidities; psychiatric problems that could interfere with the study; and insufficient knowledge of the Dutch language to understand the purpose of the study and the testing methods.
Recruitment
Physicians from the participating rehabilitation centers preselected former inpatients using information from medical charts. Potential participants were sent a patient information letter, and 2 weeks thereafter, they were contacted by the research assistant to check the inclusion and exclusion criteria and to provide further information. All participants signed the consent form after expressing their willingness to participate.
Multicenter approval was granted by the Erasmus MC Medical Ethics Committee, Rotterdam, The Netherlands. Local approval was further granted by all participating centers.
Randomization and Interventions
Randomization
In each rehabilitation center, participants were randomly allocated to the intervention group or the control group after the baseline measurements. Blocked randomization with a block size of 6 was used to ensure an even distribution of participants. The research assistants who performed the measurements for this study were not involved in the self-management intervention and were blinded for group allocation. The researchers were also blinded for group allocation until the initial data analyses of the primary and secondary outcomes were performed.
Intervention
The theoretical framework that was used to design the intervention and to select outcome measures is described in detail elsewhere. 22 In this theoretical framework, we combined 2 well-known models of behavior change: the theory of planned behavior (TPB) 24 and the transtheoretical model of behavioral change (TTM). 25 TPB assumes that intentions to perform (new) behavior are influenced by attitudes (eg, the perceived benefits or importance of the new behavior), subjective norms (eg, social support, attitudes expressed by other people), and perceived behavioral control (eg, confidence in one’s ability to perform the new behavior). 24 The TTM assesses an individual’s readiness to act on a new healthier behavior, 25 such as a more active lifestyle. 26 In other words, readiness is measured as one’s willingness to adopt certain new behavior within a certain time frame.
The HABITS intervention specifically targeted on 2 conditions for behavior change: optimizing intentions toward a healthier lifestyle and improving perceived behavioral control. Perceived behavioral control included (1) self-efficacy, defined as a person’s confidence in one’s ability to perform certain behavior, namely, a more active lifestyle 27 ; and (2) proactive coping, which assumes that individuals do not only react on threatening situations but that they can also anticipate on situations that may be a threat or influence their goals, a more active lifestyle, in the future.28,29
The HABITS intervention consisted of 1 home visit, 5 individual and 5 group sessions during a total of 16 weeks. The HABITS intervention contained various elements that should facilitate an active lifestyle and the development of self-management skills: guidance of the HABITS counselor, peer support and mastery experiences (experiencing task accomplishment strengthens self-efficacy),21,27 discussions on various themes related to an healthy active lifestyle, action and proactive coping planning, problem solving, activity monitoring, a self-help workbook, and a booklet, “How to Stay Fit With SCI.” 30
The intervention was provided by counselors who were already working in one of the participating rehabilitation centers, were experienced in the treatment of persons with SCI, for example, physical therapist, and were trained in motivational interviewing (MI). MI is a directive client-centered counseling style to elicit behavior change by helping clients explore and resolve their ambivalence toward behavior change. 31
Control Group
The control group received information about active lifestyle in SCI including one information group meeting in the first week of the study In addition, they received the same self-health booklet as the intervention group, “How to Stay Fit With SCI.” 30 This book was published at the same time as the start of the study and resonated with the information needed for the control group.
Outcomes and Follow-up
Data were collected for both groups at baseline (T0) and at 16 weeks (T1) and 42 weeks (T2) after baseline. Measurements at the different time points included wearing an activity monitor, self-report questionnaires, and physical tests performed at the rehabilitation center.
The hierarchy in the outcome measures was determined according to the research questions and the theory we used: the primary outcomes provide the direct answer on the research questions. The secondary outcomes are those that may reveal the mechanisms between behavior changes. The tertiary outcomes concern the more remote outcomes of our RCT.
Primary Outcomes
Amount of self-propelled wheelchair driving
Physical activity was objectively measured as the amount of time of self-propelled wheelchair driving in seconds, using 2 accelerometer-based devices (ActiGraph GT3X+). 32 One accelerometer was attached at the wrist and the other to the spokes of one wheelchair wheel with special Velcro bands. Based on the data of the 2 accelerometers, a custom-made algorithm in MatLab (r20011b) differentiated between self-propelled wheelchair driving and other activities. This method allowed the identification of self-propelled wheelchair driving with a sensitivity of 88% and a specificity of 83%. 33 Participants were asked to wear the activity monitor directly after each test occasion continuously for 5 consecutive days, except while swimming, bathing, or sleeping. They were instructed to continue their ordinary daily activities during these 5 days. Data were included in the analysis if patients wore the activity monitor for at least 3 days and for at least 10 hours a day. Participants received a simple diary—as reference to the data—in which they could indicate whether they have worn the activity monitor and if there were any peculiarities that could have influenced the measurement.
Self-reported physical activity
Self-reported levels of physical activity (PA) was assessed with the PASIPD. 34 The Dutch adaptation of the PASIPD consists of 11 items concerning sports, hobbies, and household- and work-related activities. The questionnaire includes items on the number of days a week and the hours a day a certain activity was performed during the past 7 days. The total score of the PASIPD was computed by multiplying the average hours per day for each item by a metabolic equivalent value (METs) associated with the intensity of the activity, MET * hour/week. PASIPD scores range between 0 and 182.
Both measures provide other but sufficient information about physical activity. The objective method we have used in our study provides information on the duration of wheelchair use, expressed in, for example, minutes of active wheelchair driving. The PASIPD aims to assess energy expenditure, based on duration of activity categories of different intensities.
Secondary Outcomes
Perceived behavioral control
Perceived behavioral control (consisting of self-efficacy and proactive coping) was measured with 2 scales:
The SCI exercise self-efficacy scale 35 measures self-reported self-efficacy for various types of physical exercise in individuals with SCI. This scale includes 10 items with a 4-point scale (1 = not at all true; up to 4 = exactly true). The maximum range of the total score is 10 to 40. Internal consistency was 0.93. 35 This questionnaire was translated into Dutch and validated in a sample of individuals with SCI. 36
Proactive coping was measured with the Utrecht Proactive Coping Competence scale,29,37 which assesses self-reported competency with regard to proactive coping, meaning anticipating on and dealing with possible future situations. This self-report scale includes 21 items with 4-point response scales (1 = not capable; up to 4 = very capable). The total score is the mean of the item scores, and therefore the range is also 1 to 4. Internal consistency has shown to be between 0.83 and 0.95, and test-retest reliability between 0.45 and 0.82.29,37
Stage of exercise change
The University of Rhode Island continuous measure (URICA-E2) 38 assesses readiness to change with regard to regular exercise and was based on the TTM 25 and a previous questionnaire, the URICA. 39 The URICA-E2 consists of 24 statements reflecting intentions toward exercise change. The responses are given on a Likert-type 1 to 5 point scale, from “strongly disagree” to “strongly agree.” Internal consistency of this questionnaire was 0.80 to 0.93. 40
Attitude to change behavior
Attitude was measured using the Exercise Decisional Balance. 41 This questionnaire reflects the individual’s relative weighing of the pros and cons of changing exercise behavior. The questionnaire consists of 10 statements (5 cons, 5 pros). The importance of each pro and con is rated on a 5-point scale ranging from 1 (not at all) to 5 (extremely). Mean internal consistency of this measure was 0.8 for the pro subscale and 0.7 for the cons subscale. Test-retest reliability of the pros and cons scales was 0.84 and 0.74, respectively. 41
Tertiary Outcomes
The tertiary outcomes concern the more remote outcomes of our RCT. Secondary health conditions (Spinal Cord Injury Secondary Conditions Scale 42 ), Social Support (Social Support for Exercise Behavior Scale 43 ), Aerobic Capacity (VO2peak [L/min]/POpeak [W]) measured during a wheelchair treadmill test,44,45 Functional Independence (Spinal Cord Independence Measure III46,47), Mood (Mental Health Inventory-548,49), Fatigue (Fatigue Severity Scale50-52), Participation (The Utrecht Scale for Evaluation of Rehabilitation-Participation and Quality of Life 53 ), Quality of Life (5 items from the World Health Organization Quality of Life Assessment 54 ), and body mass index (BMI).
Confounders
We included age, sex, time since injury, level of SCI, rehabilitation center, and baseline BMI as confounders. Differences between the intervention and control groups with respect to these variables may distort the outcomes of the study since we supposed female gender, older age, a longer time since onset of SCI, a higher level of SCI, and a higher BMI to be associated with lower levels of physical activity. 55
Statistical Analysis
The desired size of the study sample (N = 80) was based on a power analysis with a power of 80%, α = .05, and an expected increase of 30 minutes per day in the duration of self-propelled wheelchair driving as assessed with the accelerometer-based activity monitor in the intervention group compared with the control group. This estimation was based on levels of daily physical activity found in persons with SCI in previous studies of our department.1,56
We performed nonresponse analyses with data available from medical charts including the following variables: age, sex, level of SCI, completeness of SCI, and time since injury. In addition, 50 individuals who declined participation in the RCT volunteered to complete the baseline questionnaire. Group differences were tested with t tests or χ2 tests.
To determine the effectiveness of the self-management intervention, linear mixed models analyses with a 3-level structure (repeated measures, participants, and rehabilitation center) were performed. In the linear mixed model analyses, we adjusted for the correlated observations within the participant and for the correlated observations within the rehabilitation center by adding a random intercept on both levels to the model. Only participants who completed the baseline and at least one follow-up test occasion were included in these analyses. First, separate overall models were made for each outcome variable, including group allocation and the baseline value of the particular outcome variable, to estimate the overall intervention effect over time Second, we added time and an interaction between group allocation and time to these overall models to assess the between-group differences at the 2 follow-up moments (T1 and T2).
The regression coefficient (B), the P value, and confidence intervals were computed for the unadjusted models as well as for the models that were adjusted for age, sex, time since injury, level of SCI, and baseline BMI.
For the stages of exercise change, Poisson mixed model analyses were performed, including the same steps as the linear mixed models analyses.
Because analyses could not be performed if baseline values were missing and because of the relatively large amount of missing data in the objectively measured physical activity, we replaced missing baseline values by the overall (intervention and control) group baseline value. This step was only performed if the 2 follow-up measurements were available.
IBM SPSS Statistics version 21 was used for all statistical analyses except for the Poisson mixed model analyses, where STATA version 13 was used.
Results
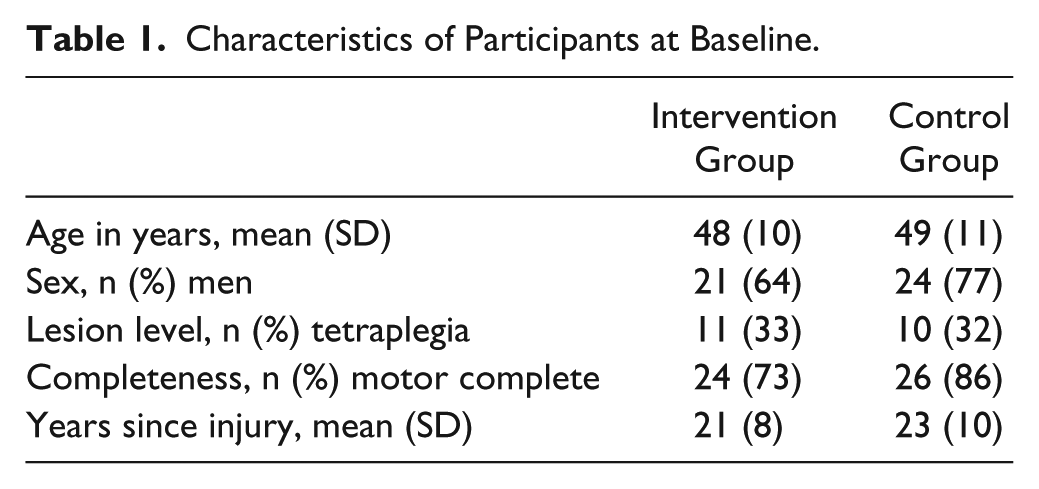
Between January 2012 and October 2014, 64 persons with long-term SCI were included in this study. Figure 1 shows the flow diagram of the inclusion. Baseline, personal, and lesion characteristics of the 64 participants are presented in Table 1. Dropouts in the intervention group (n = 7) and in the control group (n = 8) did not significantly differ from the included participants in terms of personal or lesion characteristics and physical activity at baseline.
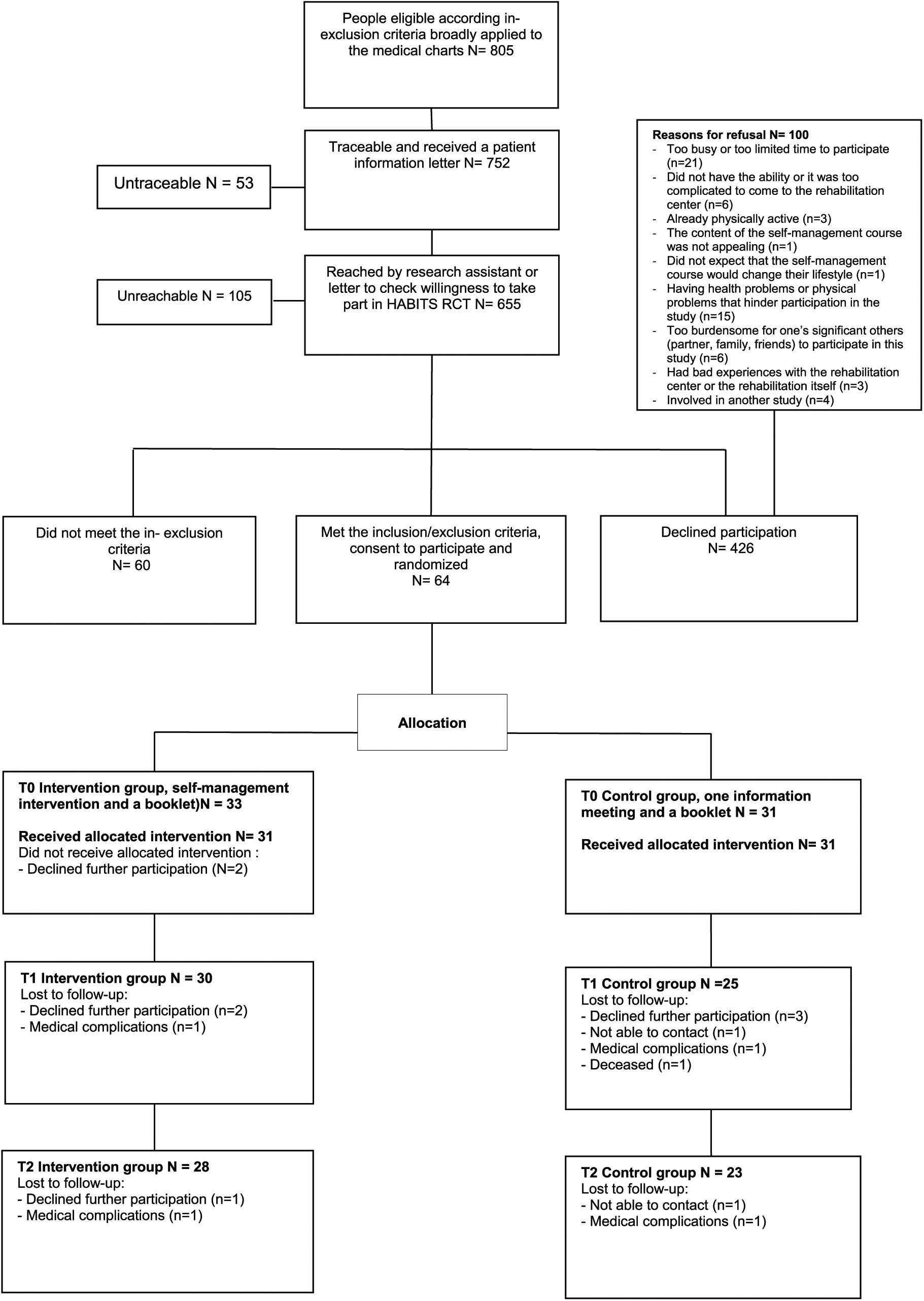
Flow chart.
Characteristics of Participants at Baseline.
No significant differences were found between the included participants of this study (n = 64) and data on the nonparticipants available from the medical charts (N = 394-617; P > .05; N varies, since not all data on every characteristic were available for all nonresponders). In addition, no significant differences (P > .05) were found between the self-reported main and secondary outcomes between the participants of this study and the nonparticipants who volunteered to complete the baseline questionnaire. Adherence percentages to the different parts of the intervention were 100 for the home visits, and 86 and 96 for the group sessions and telephone counseling sessions, respectively.
Of the 192 potential activity monitor data points, 98 were available (38 at T0, 29 at T1, and 24 at T2). Five measurements at T0, 3 at T1, and 5 at T2 were missing due to technical problems. Seventy-four measurements (21 at T0, 33 at T1, 38 at T2) were not available because the participant did not wear the activity monitor for at least 3 days.
Intervention Effects
The observed data of the primary and secondary outcomes are presented in Figure 2 and in Tables 2 and 3. The modeled data are presented in Tables 4 and 5. In the models adjusted for confounders, no overall intervention effects were found on the primary outcomes amount of self-propelled wheelchair driving (B = 4.68; P = .19; 95% CI = −2.46 to 11.81) and self-reported physical activity (B = 9.97 minutes; P = .83; 95% CI = −93.21 to113.22). The same applies to the between-group differences at T1 and T2. On the secondary outcomes we did not find an overall intervention effect or between-group differences for perceived behavioral control. For the stages of exercise change, a positive trend (P = .08) was found for the overall intervention effect in favor of the intervention group. For exercise attitude, a higher score was found for the intervention group at T1, whereas at T2 the control group had a higher score than the interventions group.
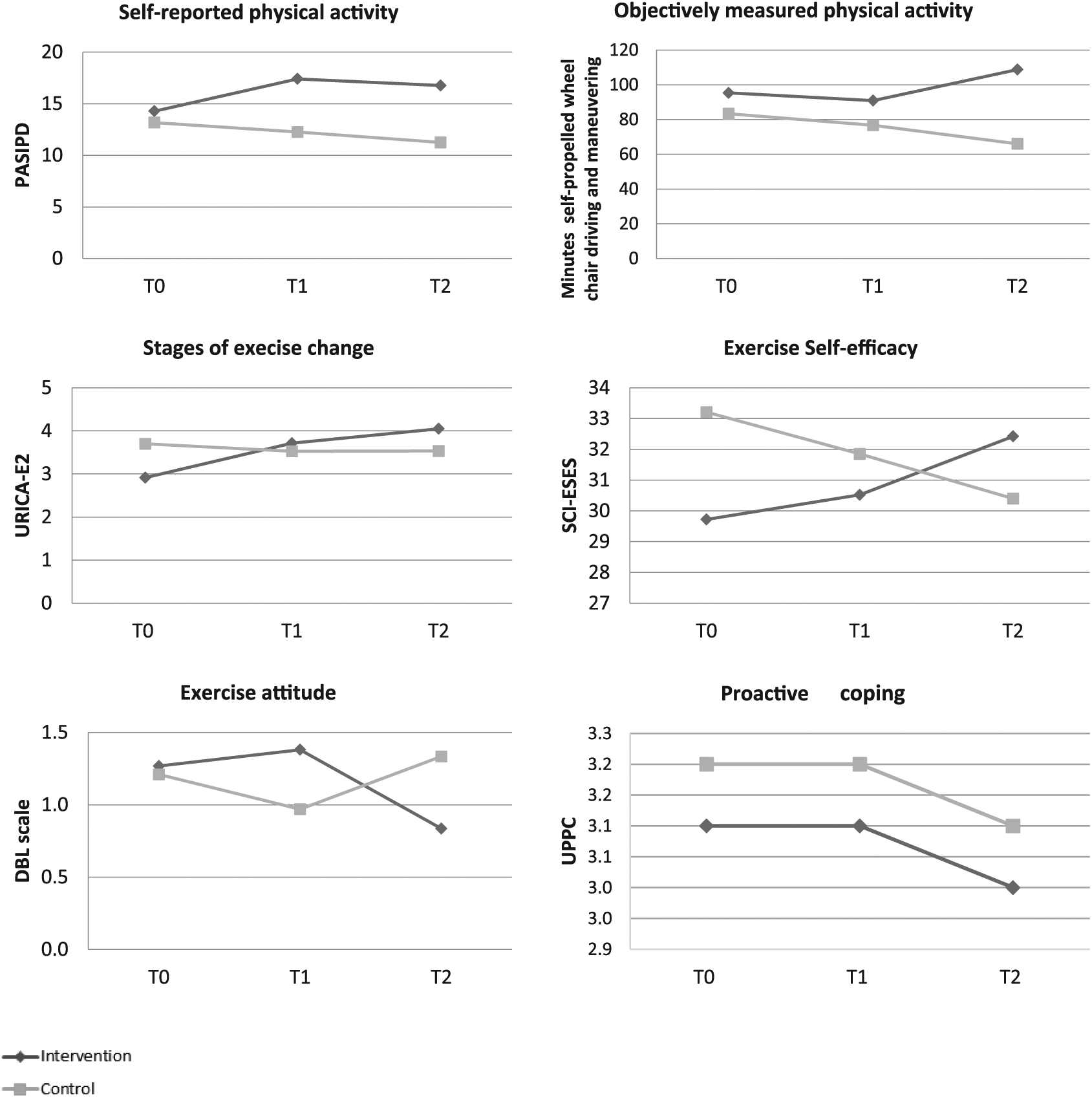
Observed data primary and secondary outcomes. (The measures of error are presented in Table 2.)
Observed Values for Primary and Secondary Outcomes.
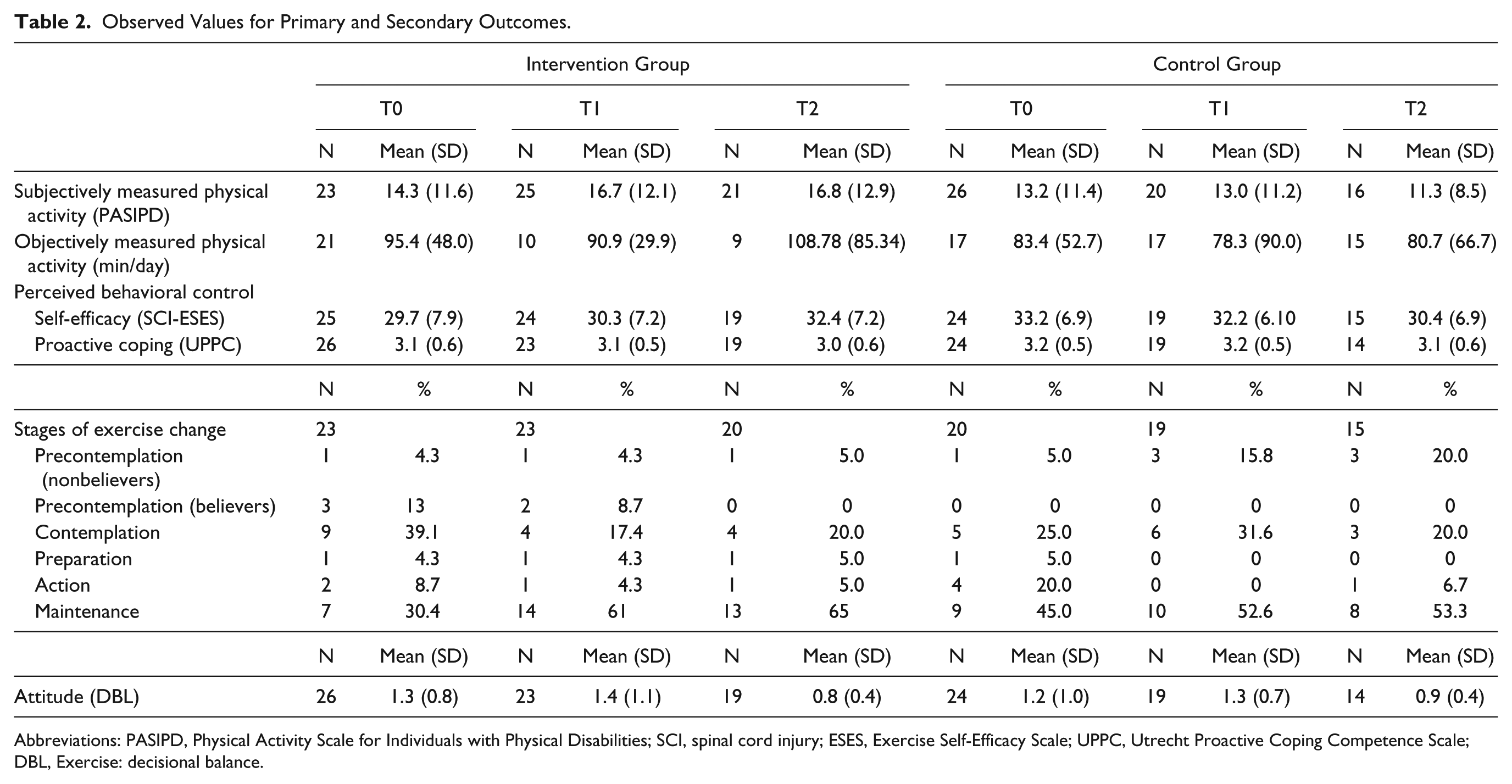
Abbreviations: PASIPD, Physical Activity Scale for Individuals with Physical Disabilities; SCI, spinal cord injury; ESES, Exercise Self-Efficacy Scale; UPPC, Utrecht Proactive Coping Competence Scale; DBL, Exercise: decisional balance.
Observed Values for Tertiary Outcomes.
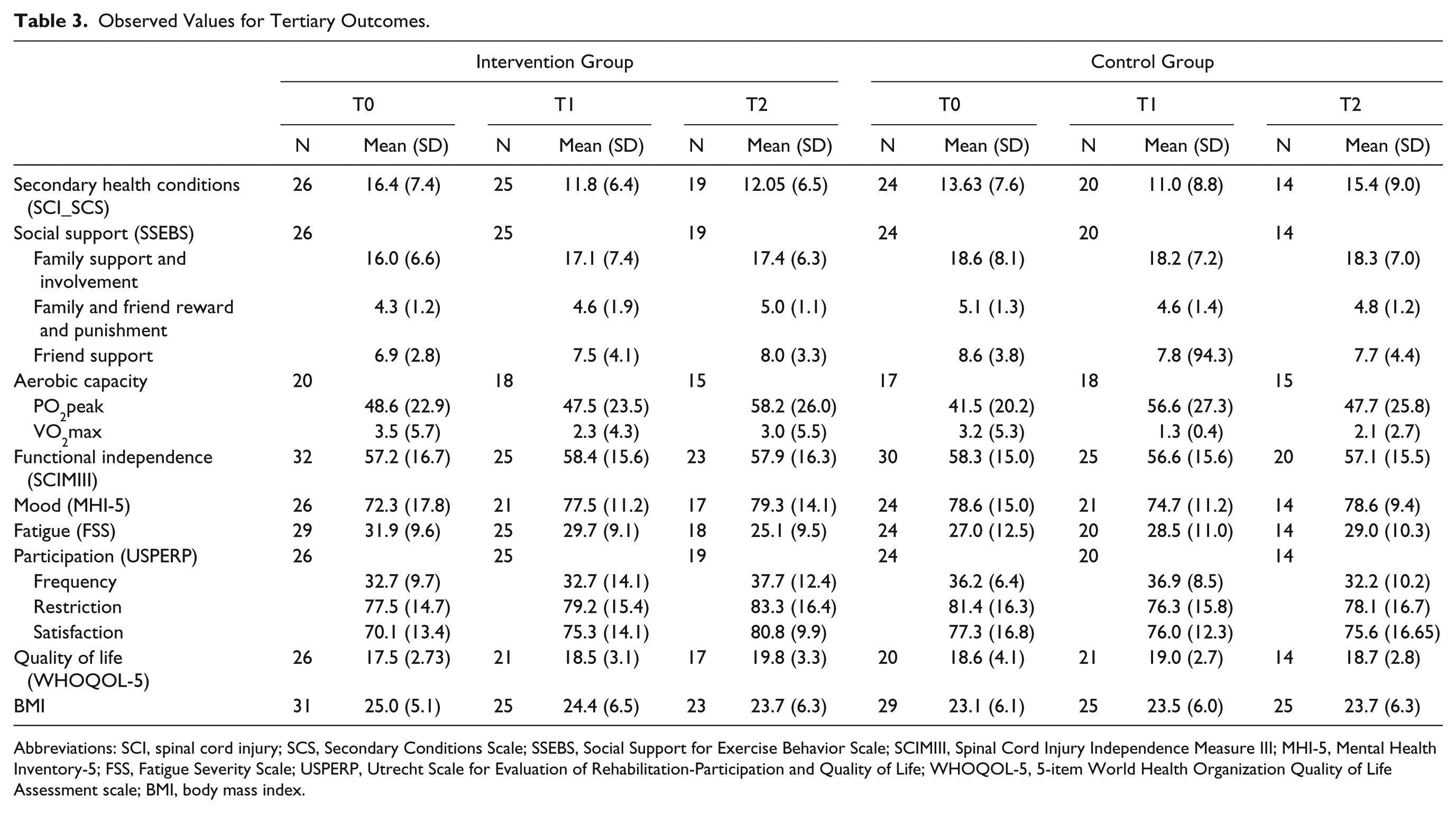
Abbreviations: SCI, spinal cord injury; SCS, Secondary Conditions Scale; SSEBS, Social Support for Exercise Behavior Scale; SCIMIII, Spinal Cord Injury Independence Measure III; MHI-5, Mental Health Inventory-5; FSS, Fatigue Severity Scale; USPERP, Utrecht Scale for Evaluation of Rehabilitation-Participation and Quality of Life; WHOQOL-5, 5-item World Health Organization Quality of Life Assessment scale; BMI, body mass index.
Mixed models for primary and secondary outcomes.
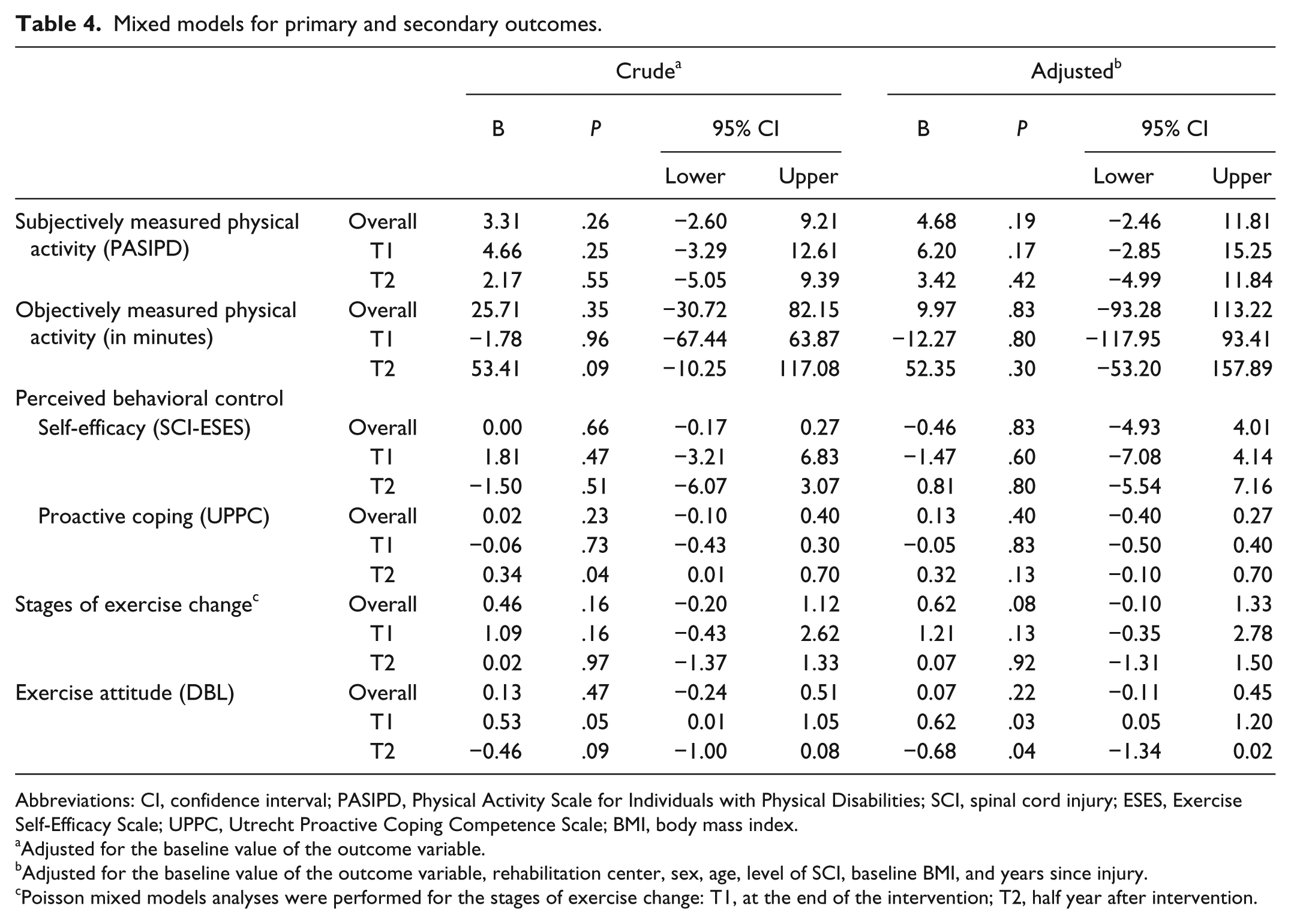
Abbreviations: CI, confidence interval; PASIPD, Physical Activity Scale for Individuals with Physical Disabilities; SCI, spinal cord injury; ESES, Exercise Self-Efficacy Scale; UPPC, Utrecht Proactive Coping Competence Scale; BMI, body mass index.
Adjusted for the baseline value of the outcome variable.
Adjusted for the baseline value of the outcome variable, rehabilitation center, sex, age, level of SCI, baseline BMI, and years since injury.
Poisson mixed models analyses were performed for the stages of exercise change: T1, at the end of the intervention; T2, half year after intervention.
Mixed Models for Tertiary Outcomes.
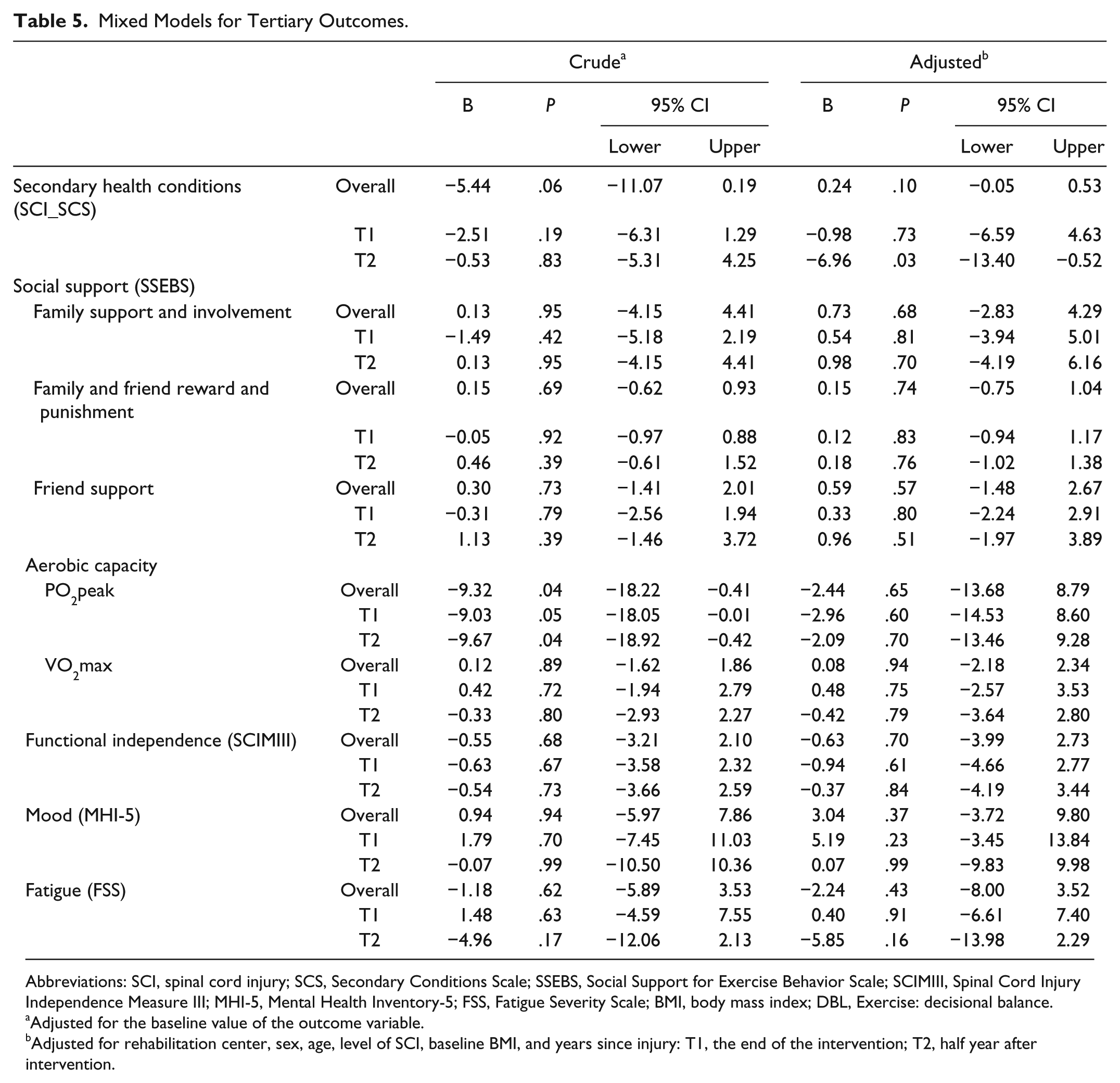
Abbreviations: SCI, spinal cord injury; SCS, Secondary Conditions Scale; SSEBS, Social Support for Exercise Behavior Scale; SCIMIII, Spinal Cord Injury Independence Measure III; MHI-5, Mental Health Inventory-5; FSS, Fatigue Severity Scale; BMI, body mass index; DBL, Exercise: decisional balance.
Adjusted for the baseline value of the outcome variable.
Adjusted for rehabilitation center, sex, age, level of SCI, baseline BMI, and years since injury: T1, the end of the intervention; T2, half year after intervention.
Of the tertiary outcomes, only secondary health complications showed significant difference: at T2 the intervention group experienced significantly less impact of SHCs compared with the control group.
Discussion
To our knowledge, this is the first RCT to examine the effectiveness of a self-management intervention on physical activity levels in individuals with long-term SCI. Overall, we did not find significant differences between the intervention and control groups on the outcome measures, and thus our study does not support the effectiveness of the self-management intervention.
This result on the lack of effectiveness is not what we hypothesized. Other studies in SCI populations provided some indication for positive effects of behavioral interventions on physical activity levels in individuals with SCI and in people with other chronic conditions (eg, diabetes, arthritis and asthma).19-21 The RCT of Nooijen et al 18 most strongly corresponds with our study, and in that study positive results of a behavioral intervention on level of physical activity were found. However, in that study people with a subacute SCI participated, instead of the chronic SCI group in our study. It might be that people in the subacute stage are more open to behavioral interventions. Because almost everything has changed and everything needs to be done differently than in the past, people might also be more open to adapt behaviors that are taught or advised, such as an active lifestyle. Our study participants have lived with the condition for many years, learned to cope with their SCI, and will have developed stable behavior pattern. As a result, they do not experience a strong need to change their behavior, with a resulting increased difficulty to change their behavior.
Another explanation for the intervention not being effective—with respect to levels of physical activity and other outcomes—might be that we did not include the chronic SCI participants for whom the intervention could have been most effective. For example, we included individuals with a PASIPD score lower than the 75th percentile of a Dutch SCI population 5 years post-onset. 23 Our study sample showed to have an average level of physical activity of about the 70th percentile, quite close to the allowed maximum of 75. Consequently, our sample did have relatively less potential for improvement, although the mean PASIPD score in our study was still substantially lower compared with a Dutch cohort study (13.8 vs 19.0).
Other outcomes also showed relatively high baseline scores. For example, the average baseline exercise self-efficacy score of 31.4 (SD 7.6) seems high compared with the maximum value of 40, and it is similar to the results (mean 31.4, SD 7.8) of a large sample of individuals with long-standing SCI (N = 268) who were not selected on activity level (H. P. Kooijmans et al, unpublished data, 2017). Similarly, the mean baseline proactive coping score in our study was 3.1 (SD 0.5), which seems to be relatively high compared to the range of 1 to 4, and comparable to the mean score of a population with a recent SCI and who were not selected on activity level (mean score = 3.2, SD 0.4). 18 In addition and maybe most important, a large part of the participants already were in the action or maintenance phase of the stages of exercise change at baseline, which means according to themselves they were already active. This makes it difficult to further improve on this outcome, which is remarkable because the aim of the study—to improve active lifestyle—was also clarified to the participants. This cannot be logically linked to being categorized in the action and maintenance phase.
We did not see evidence for effectiveness of the intervention on the secondary outcome measures either. An intervention effect on these outcomes was expected, since previous studies in other populations showed that exercise self-efficacy57,58 and perceived behavioral control 59 could be improved by a behavioral intervention. However, behavioral studies with negative results on outcomes such as self-efficacy can also be found.60,61 Although these studies have a common target, they also differ in many aspects, making it difficult to speculate about the background of the between-study differences in effects. A specific factor that might have contributed to the absence of significant effects on the secondary outcomes might be that the participants in the intervention group may have developed a more critical look on their behavioral control and attitude after their intervention, since they are much more aware of their (in)capabilities after the intervention. This explanation is also suggested by Maher et al in their study with adolescents with cerebral palsy. 60
With respect to exercise attitude, we found no overall intervention effect, but the intervention group showed a significantly more positive exercise attitude directly after the intervention compared with the control group. However, at follow-up the control group was significantly more positive compared with the intervention group. This shift in effect on attitude is difficult to explain. The observed data show that all participants of the intervention group remained a positive exercise attitude; however, it became less positive as compared with the control group.
It can be questioned whether the design and the execution of the intervention affected the effectiveness of the intervention. It takes time to change behaviors to an active lifestyle in individuals with physical disabilities, 62 and it is assumed that at least 6 months are needed. 25 An important requirement for a behavioral change is that people are aware of their own abilities (similar to perceived behavioral control) and intentions to perform physical activities. 62 For some of the participants the length of our intervention might have been too short to change behavior, despite the fact that they have received tools to put their self-management skills into practice and tools to proceed on their goals after the determination of the intervention. Furthermore, as a result of the multicenter character of our study, a uniform execution of the intervention cannot be guaranteed. It might also be possible that the intervention was not completely executed according to the protocol. However, we made every arrangement to ensure that the intervention was executed as intended. The counselors received 3 training sessions in advance of the intervention, and there was a contact meeting during the intervention in which the process and the protocol of the intervention were discussed.
We already discussed the possible role of patient characteristics in the effectiveness of the intervention. One point should be added to this discussion. In our study, we did not succeed in including the required number of 80 participants as indicated by our power calculation. After having invited 805 individuals with a long-term SCI to participate in this study, only 64 participants agreed to participate and were included. This may have caused selection bias, and the lack of power may have had an impact on our results. However, when we compared the demographic characteristics of the participants of study and all nonparticipants, we did not find any significant differences. Furthermore, 50 nonparticipants completed a questionnaire with the main outcomes of this study, and again, no significant differences were found between participants and nonparticipants.
Strengths and Limitations
A strength of our study was that the study was blinded, for both the assessor and the researcher, also in the phase of data analysis. Furthermore, by performing mixed models analyses, we have used the best possible statistical analyses that handles longitudinal, repeated measures in small numbers and relatively high dropouts in the best possible way. 63
Another strength is the application of objective assessment of levels of physical activity. The primary aim of the intervention was to increase levels of physical activity. Because it is known that in the area of physical activity outcomes from self-reported instruments differ from objectively measured outcomes, we included both types of instruments in our study.
The main limitations in our study were the small sample size, selection bias, missing values, and dropouts. Individuals with a long-term SCI are a vulnerable group; 2 participants died (not related to the study) during the study and several participants dropped out of the study because of illness or secondary complications.
Future Research
Firstly, future research should focus on people who have a greater potential to improve. For this, insight is needed in the determinants of the outcomes of behavioral interventions.
Second, the measurement of objective physical activity should become less burdensome to the patients to minimize missing data. The devices we used were much smaller than activity monitors used before, 56 but 5 days proved to be very long.
Third, it seems important to further decrease the burden of participation in the intervention, for example, by making use of e-health to reduce transportation time and problems or to organize more intensive support in the home environment, for instance, by home visits or collaborations with local gyms. However, the effectiveness of such an e-health program in this kind of population needs to be studied.
Conclusion
A structured 16-week self-management intervention was not effective to change behavior toward a more active lifestyle and to improve perceived behavioral control, stages of change, and attitude in individuals with a long-term SCI.
Footnotes
The trial was registered in the ISRCTN registry (Number 11233847).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by ZonMW and Fonds Nutsohra (Grant No. 89000006).