
Abstract
Background. Walking speed is assumed to be a key factor in regaining ambulation after spinal cord injury (SCI). However, from the literature it remains unclear which walking speed usually results in independent community ambulation. Objective. The primary aim of this study was to determine at which walking speed SCI patients tend to walk in the community instead of using a wheelchair. The secondary aim was to investigate clinical conditions that favor independent ambulation in the community. Methods. Data from SCI patients were collected retrospectively from the European Multicenter Study about Spinal Cord Injury database. We determined a cutoff walking speed at which the patients tend to walk in the community by plotting a receiver operating characteristics curve, using the Spinal Cord Independence Measure for outdoor mobility. Univariate analyses investigated which factors influence independent community ambulation. Results. A walking speed of 0.59 m/s is the cutoff between patients who do and do not ambulate independently in the community, with a sensitivity of 91.6% and a specificity of 80.3%. Age, injury severity, and lower limb muscle strength have a significant influence on independent community ambulation. Conclusions. Patients with an SCI who regain a walking speed of 0.59 m/s tend to achieve a level of walking effectiveness that allows for independent community walking. Although such patients tend to be younger and less severely injured, this walking speed can be a target for locomotor training in rehabilitation and clinical trials that lead to a meaningful outcome level of community walking.
Introduction
A main goal of patients with a spinal cord injury (SCI) is to regain ambulatory capacity. 1 Specific rehabilitation concepts aim at improving functional abilities such as walking. Most of them are based on improving muscle strength and locomotor training.2,3 For patients with a complete or incomplete but severe SCI, exoskeletons are an option for regaining some ambulatory function. The recovery of walking ability after SCI may improve or maintain cardiovascular health, muscle function, and bone quality. It is also beneficial for psychological well-being, participation in the community, and quality of life.4,5
Previous studies have shown that preserved muscle strength, as assessed using the International Standards for Neurological Classification of Spinal Cord Injuries (ISNCSCI) neurological assessment, is highly correlated with ambulation ability.6,7 Ambulatory capacity is defined as the degree of independence in walking, both at home and outdoors in the community. Kim et al 7 found that hip extensor strength explained up to 64% of the variance in ambulatory capacity between SCI patients. This shows that effective control of the hip muscles is essential for a higher level of ambulation, while the strength of the less affected leg is most predictive of ambulatory capacity. However, limitations in walking speed and endurance, combined with other factors such as the ability to manage curbs and stairs, could lead walking to not be the preferred method of mobility in the community. 7
The 10-meter walking test (10MWT) is a validated short-distance test to measure walking speed in daily life.8,9 This test can easily be performed in a standardized testing environment. 10 The minimum walking speed required for independent community mobility is not precisely known. The literature shows that the mean walking speed needed to cross an intersection controlled by traffic signals is 0.49 m/s. 11 For nonimpaired people, who have a mean walking speed of 1.3 to 1.4 m/s, crossing an intersection is safe and effective. 12 However, people who suffer a cerebral stroke or SCI walk less quickly. Of those who are still able to walk, they have a mean walking speed of 0.8 m/s.13,14 Forrest et al 15 showed that a minimum walking speed of 0.44 m/s is necessary for limited community ambulation after an incomplete SCI. Furthermore, it has been suggested that a walking speed of 1.20 to 1.31 m/s is required for independent ambulation in the community, since it is similar to the preferred walking speed of nonimpaired people. 16
SCI patients with limited lower extremity muscle power who are unable to bear their body weight (eg, AIS [American Spinal Injury Association Impairment Scale] A, B, and C SCI) can still walk using an exoskeleton. An exoskeleton is an orthosis with electromotors at the hip and knee joints, rechargeable batteries, and a computer-based control system. 17 The mean walking speed of a patient with a complete SCI who walks using an exoskeleton is 0.26 m/s, 18 which is much lower than the 0.49 m/s needed to safely cross an intersection. For the future, the question is whether exoskeleton ambulation will be sufficient to be a serious competitor for the wheelchair in daily life mobility. Therefore, it is important to have more knowledge about the distinguishing factors that make patients decide to walk or use a wheelchair.
This study focuses on walking speed in relation to daily life community mobility in SCI patients, between 6 months and 1-year postinjury. The primary aim is to determine the walking speed at which SCI patients tend to walk instead of using a wheelchair in the community. The secondary aim is to investigate differences in patient characteristics, including age, injury severity, gender, and lower extremity motor score (LEMS) between patients who choose or abstain from ambulation in the community.
Methods
Study Design and Patient Population
Patient data were collected from the European Multicenter Study about Spinal Cord Injury (EM-SCI) database. The EM-SCI database prospectively collects data from patients with SCI at 19 specialized European centers, on a fixed time schedule (acute phase, 4, 12, 24, and 48 weeks). The examinations consist of a standard set of neurological, neurophysiological, and functional assessments, including the ISNCSCI neurological assessments, 10MWT, and Spinal Cord Independence Measure (SCIM) evaluations. 19 All patients with ISNCSCI assessments, SCIM evaluations, and a 10MWT at 6 months or 1 year postinjury were included in this study.
Outcome Assessment
The ISNCSCI neurological assessments were performed according to the international standards. 20 They include motor score testing (graded on a 6-point scale) and sensory testing (graded 0 = absent, 1 = impaired, and 2 = normal). The assessed muscle groups of the lower extremity are the hip flexors, knee extensors, ankle dorsiflexors, toe extensors, and ankle plantarflexors. Since it has been shown that the strength of the less affected leg is more important for functional ambulation than that of the more affected leg, 7 only the best score from either the left or right leg was used in analysis of the individual muscle groups. The neurological assessments also included the LEMS (the total motor score of the muscle groups in both legs) and upper extremity motor score (UEMS; the total motor score of the muscle groups in both arms).
Walking speed was assessed during outpatient rehabilitation using the 10MWT, which measures the seconds a patient needs to walk 10 meters on a flat and smooth surface, at the subject’s preferred speed. A “flying” start is performed; the subjects walk 14 meters, but the time is only measured for walking the intermediate 10 meters. The seconds are then converted into walking speed in meters per second (m/s).
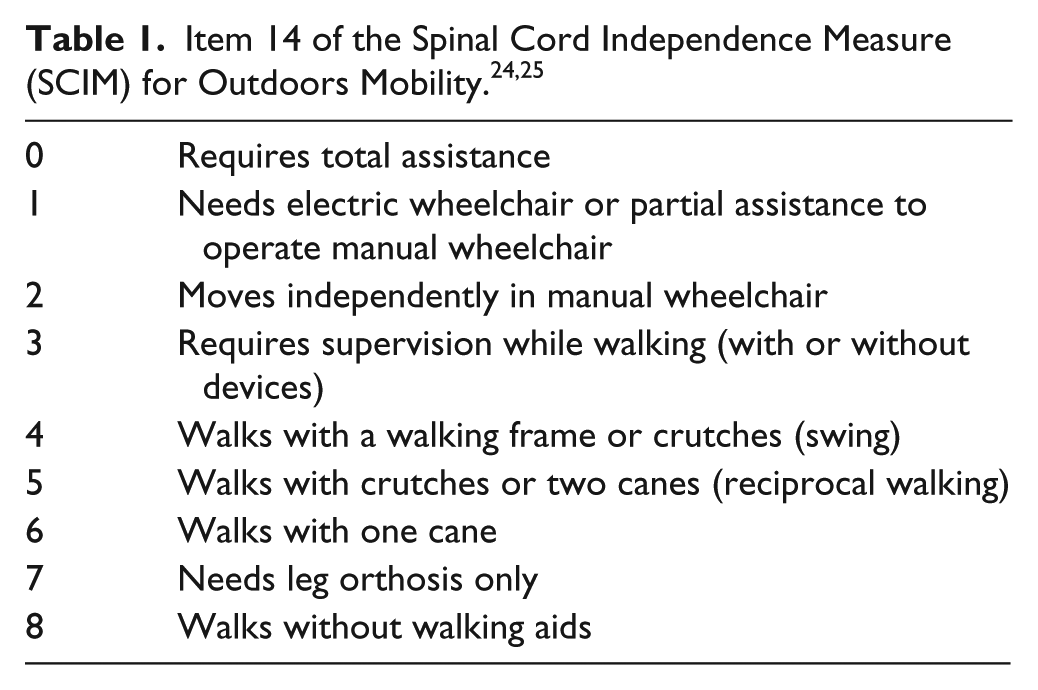
The level of mobility in the community was assessed using the SCIM item 14 for outdoor mobility, which describes how a person covers a distance of more than 100 meters (Table 1). SCIM item 14 scores 4, 5, 6, 7, and 8 were defined as independent community ambulation. This is the ability to walk more than 100 meters without supervision, but potentially with the use of walking aids. SCIM item 14 scores 0, 1, 2, and 3 were defined as being unable to walk independently in the community. This SCIM item 14 cutoff was applied as in previous studies,21-25 and allowed us to divide patients into 2 groups: those who walk independently outdoors and those who do not. The differences in characteristics between both groups were analyzed.
Statistical Analysis
We analyzed the data using SPSS version 21 and set the statistical significance at P < .05. We performed a descriptive analysis of the patient characteristics, calculating absolute and relative frequencies for categorical variables, and mean, standard deviation (SD), median, and range for continuous variables. If appropriate, 95% confidence intervals are shown. We used independent t tests and chi-square tests to determine which factors influence the outcome of independent outdoors mobility, measured at 6 months or 1 year postinjury. A receiver operating characteristics (ROC) curve was plotted using the dichotomized SCIM scores. This can be used to determine a cutoff walking speed with the best sensitivity and specificity, to be able to distinguish between patients who do and do not use a wheelchair in the community.
Results
Between 2001 and 2015, 3568 patients were included in the EM-SCI database, 920 of whom fulfilled the inclusion criteria for this study and were selected for data evaluation. Of those 920 patients, 319 (34.7%) had performed the 10MWT at 6 months postinjury, and 601 patients (65.3%) had performed this test at 1 year postinjury. Injury severity, LEMS, walking speed at 10MWT, and the SCIM item 14 scores all date from the same time, which depends on when the patient performed the 10MWT. For instance, if the 10MWT was performed at 6 months postinjury, the other variables date from 6 months postinjury as well. Most patients had a traumatic SCI (92%), the remaining 74 patients suffered an ischemic SCI. The mean age of all patients was 47 years, their mean walking speed was 0.97 m/s, and 86.5% had an AIS D SCI (see Table 2).
Patient Characteristics of the Entire Sample (n = 920).
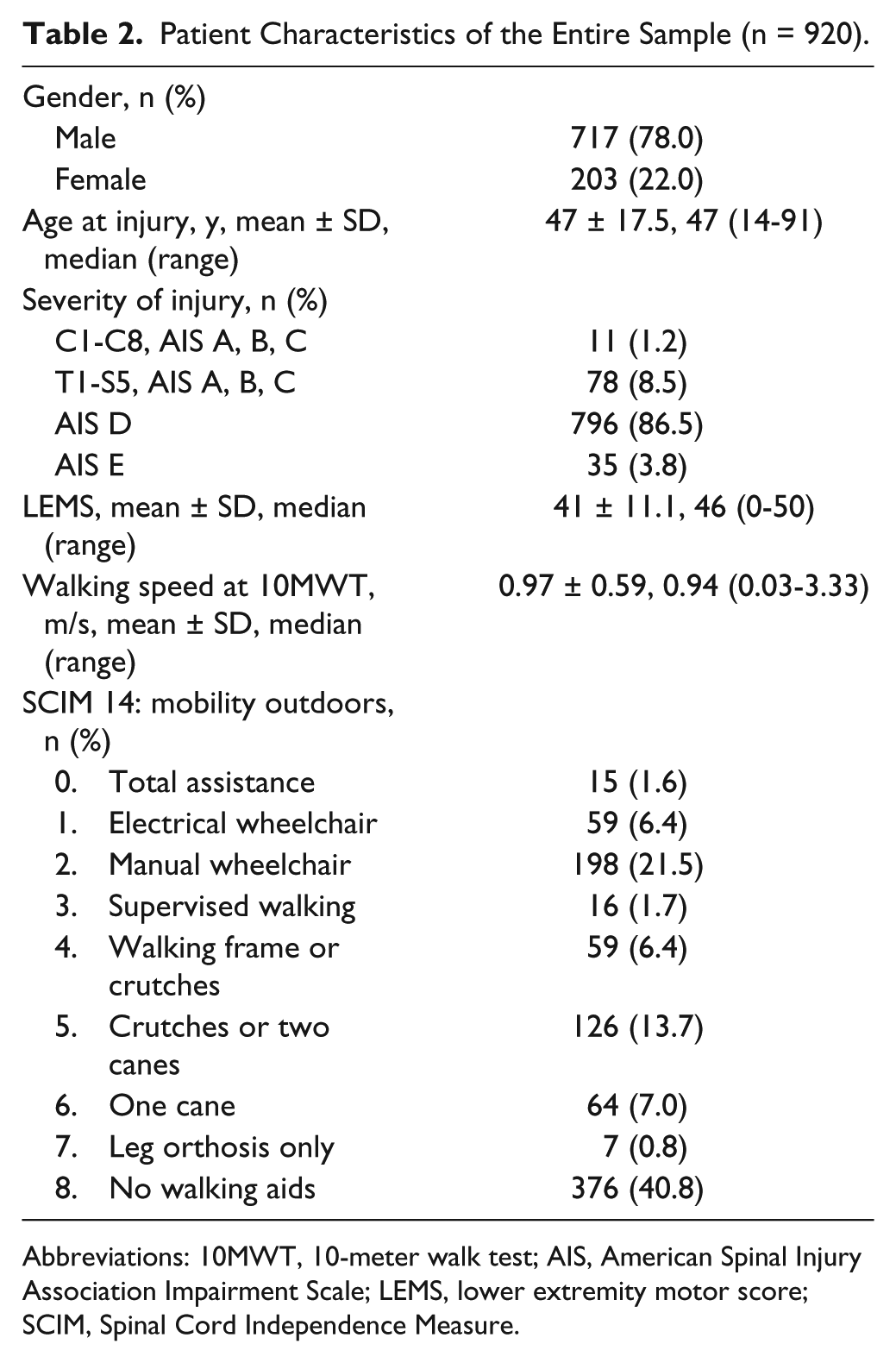
Abbreviations: 10MWT, 10-meter walk test; AIS, American Spinal Injury Association Impairment Scale; LEMS, lower extremity motor score; SCIM, Spinal Cord Independence Measure.
Table 3 describes characteristics of the patient groups who either walk independently in the community or not. Chi-square analysis was used for calculating differences between the 2 groups regarding gender and severity of injury. Independent t tests were used for calculating differences within age, UEMS, LEMS, and walking speed. There are significant differences in age, severity of injury, UEMS, LEMS, and walking speed between the 2 groups of patients. On average, patients who ambulate independently are younger, were less severely injured (ie, SCI graded AIS D or E), have a higher UEMS and LEMS, and have a higher walking speed than the group that does not ambulate independently in the community.
Characteristics of Patients Who Do and Do Not Ambulate Independently in the Community.
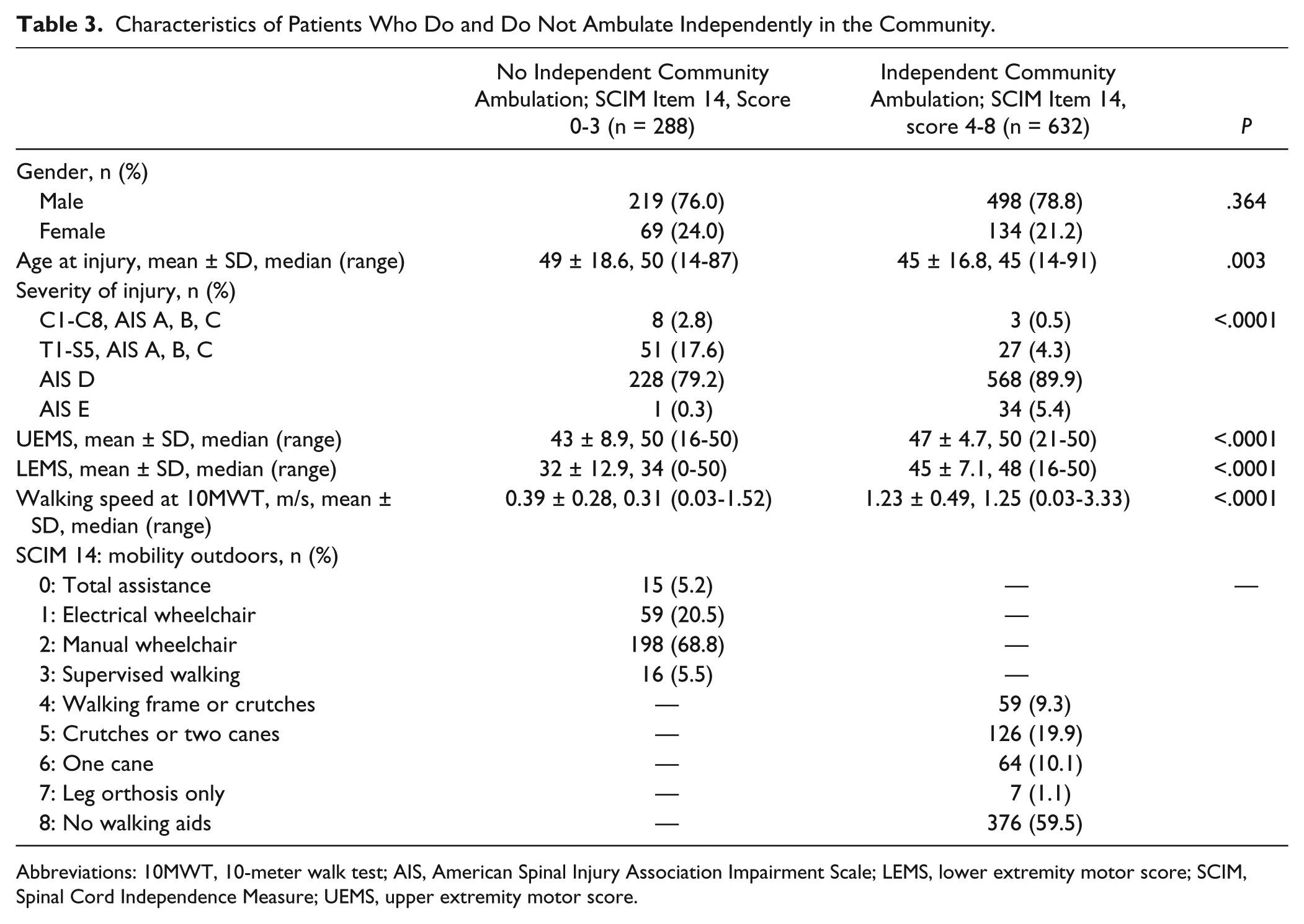
Abbreviations: 10MWT, 10-meter walk test; AIS, American Spinal Injury Association Impairment Scale; LEMS, lower extremity motor score; SCIM, Spinal Cord Independence Measure; UEMS, upper extremity motor score.
In the group of patients who do not walk outdoors, 52 had a relatively high or normal LEMS (ranging from 45 to 50 points). These patients, with a mean age of 59 years (SD 15.7 years) and a mean UEMS of 42 points (SD 8.5), had a mean walking speed of 0.60 m/s (SD 0.28 m/s; ranging from 0.14 to 1.21 m/s). Of these patients, 42% used a manual wheelchair, 27% used an electrical wheelchair, and 19% needed supervision while walking, 12% were not able to ambulate at all.
Figure 1 shows a ROC curve; the area under the ROC curve was 0.939 (95% CI = 0.924-0.955). A cutoff walking speed of 0.59 m/s was determined, which distinguishes between patients who do or do not walk outdoors in the community with a sensitivity of 91.6% and a specificity of 80.3%.
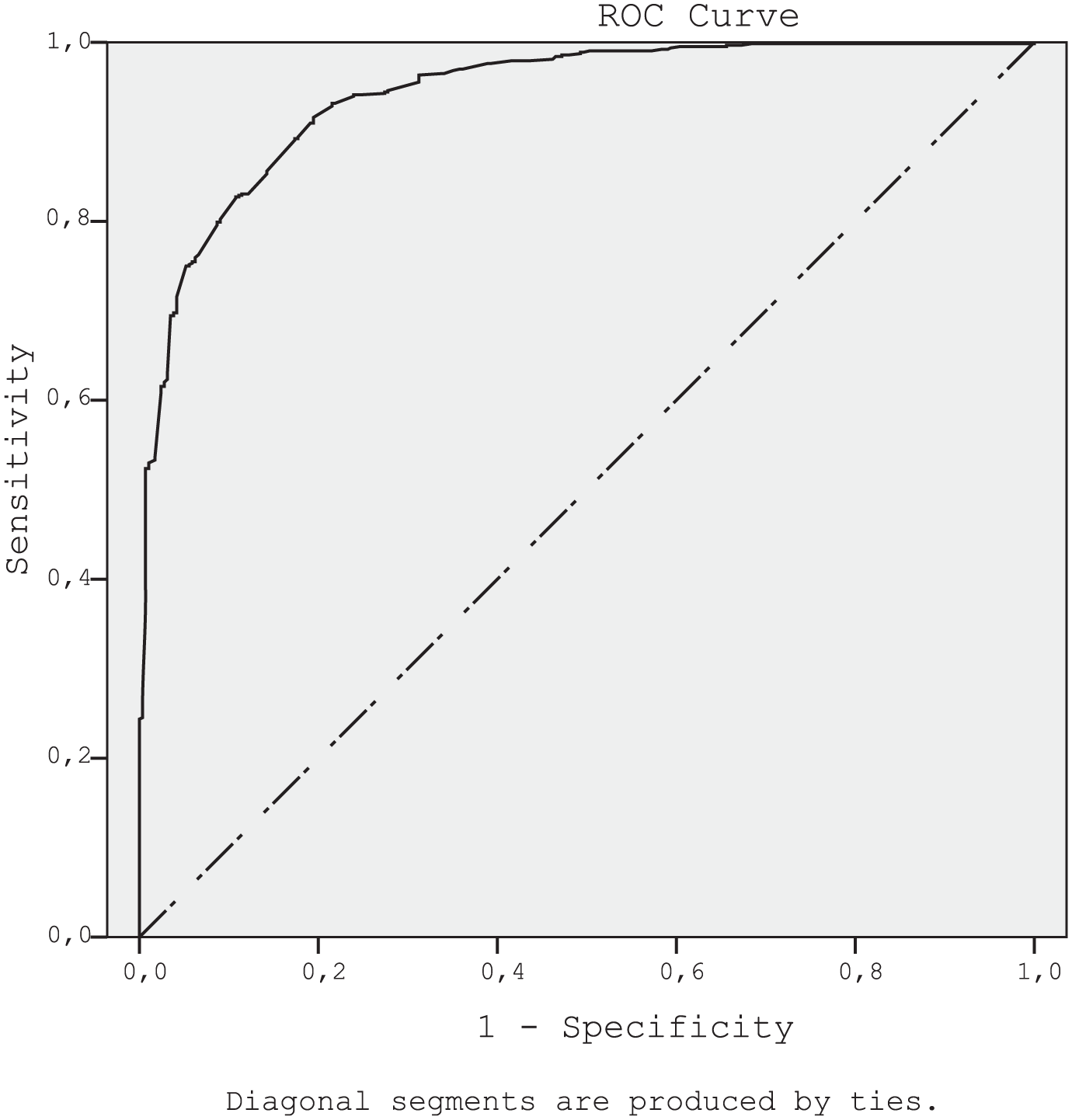
ROC curve distinguishing between patients who walk and who roll in the community.
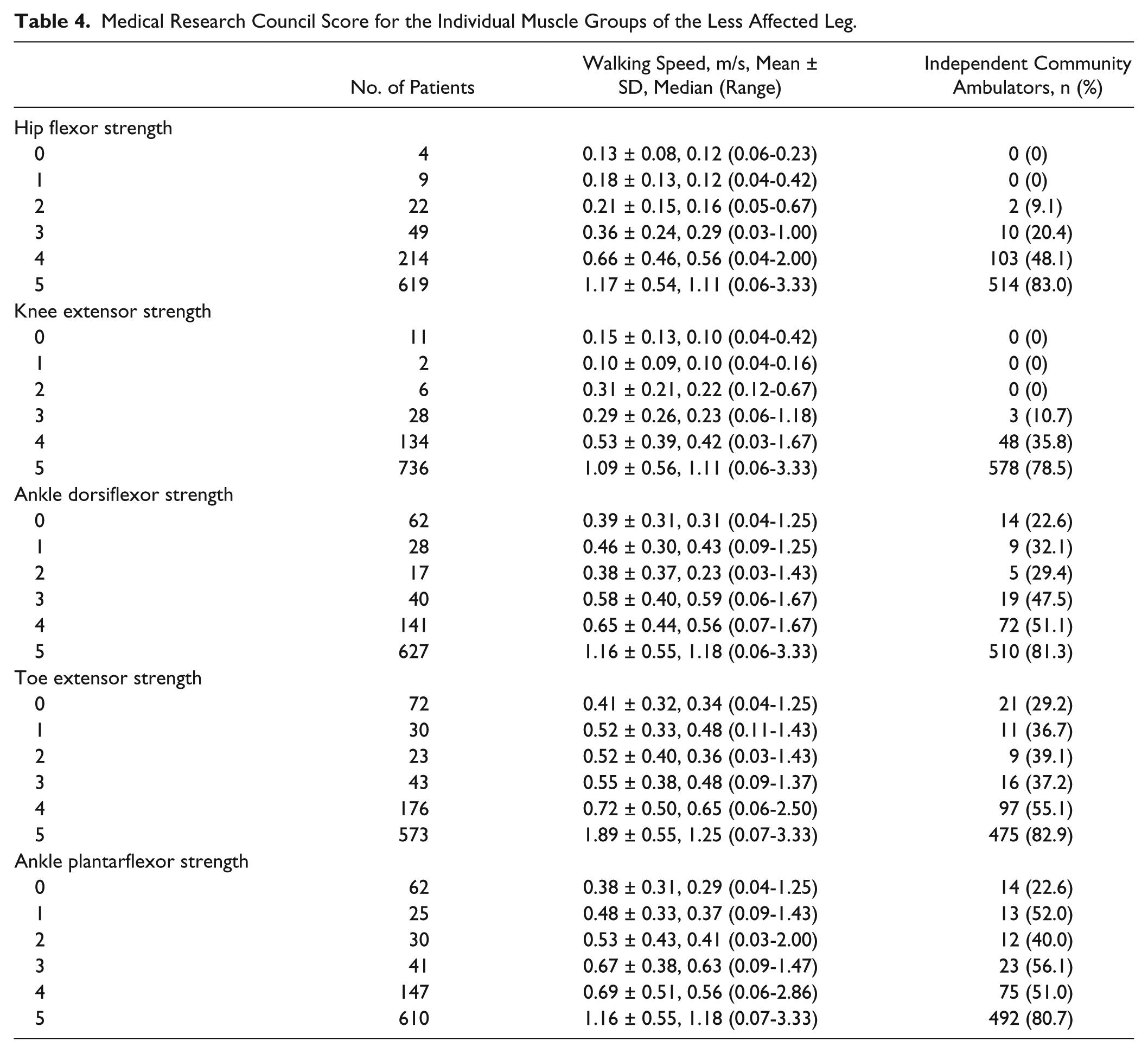
Our analysis of the individual muscle groups from the lower extremity found that a higher Medical Research Council (MRC) score results in a higher walking speed (see Table 4). An exception is a 1-point knee extensor strength MRC score, but this is based on only 2 patients. Table 4 also shows that patients with an MRC score between 0 and 2 points for the hip flexors or the knee extensors do not walk independently in the community, with the exception of 2 patients with a score of 2 points for hip flexor strength.
Medical Research Council Score for the Individual Muscle Groups of the Less Affected Leg.
Finally, we investigated the individual scores on SCIM item 14 for outdoors mobility (see Table 5). In general, mean walking speed increases with increasing SCIM scores. However, people with an SCIM 14 score of 0 have a higher mean walking speed than the following score, which may be due to the smaller number of patients in the first group. The mean scores on LEMS and UEMS show no evident increase for every increase in the SCIM score.
Walking Speed per Score on SCIM Item 14.
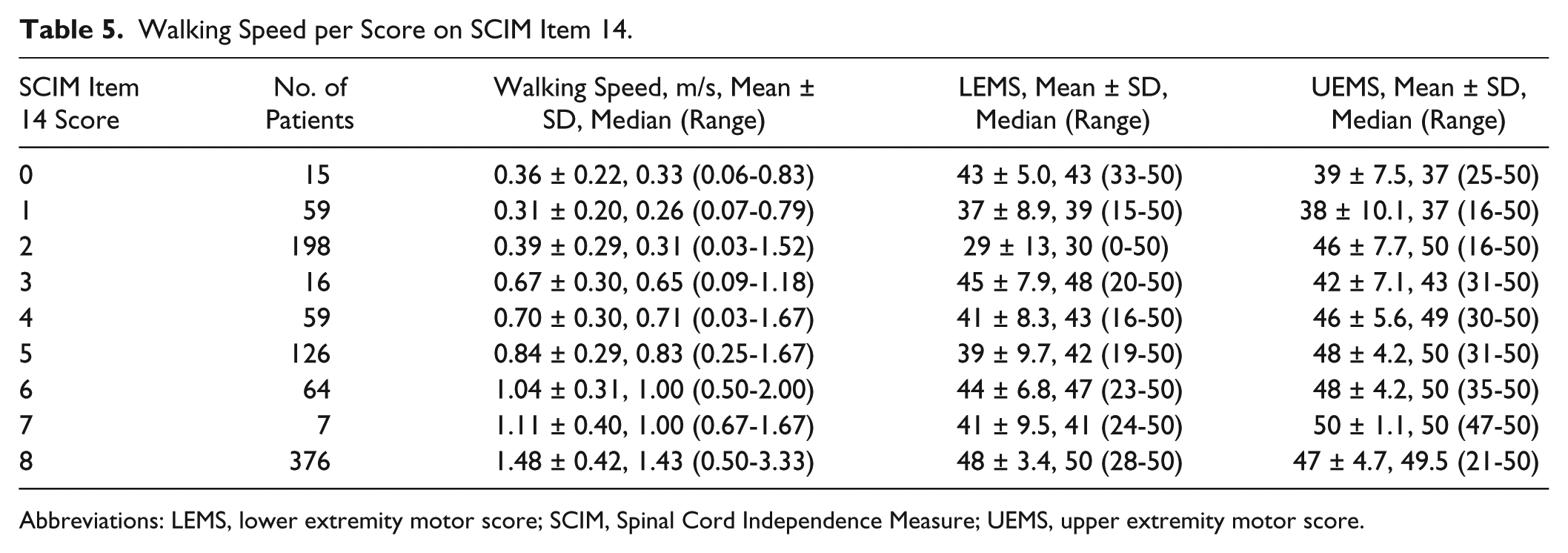
Abbreviations: LEMS, lower extremity motor score; SCIM, Spinal Cord Independence Measure; UEMS, upper extremity motor score.
Discussion
In this study, we determined a cutoff walking speed of 0.59 m/s, measured on the 10MWT. At this cutoff point, patients tend to walk in the community, with or without walking aids, instead of using a wheelchair. The finding that 0.59 m/s is apparently sufficient for independent community ambulation corresponds with earlier observations that a minimum walking speed of 0.49 m/s is required for crossing a road with traffic lights. 11 However, it is lower than previously found in patients with cerebral stroke or with AIS D SCI, who ambulate with a mean walking speed of 0.8 m/s at the 10MWT.13,14 This could be explained by the different diagnosis and patient selection, as well as the much smaller study populations than in this study: 48 cerebral stroke patients and 32 AIS D SCI patients. The preferred walking speed of the healthy population is 1.20 to 1.31 m/s, 16 which is about twice as fast as the cutoff walking speed determined in this study. The patients in this study who walk without any walking aids had a mean walking speed of 1.48 m/s, which is similar to the preferred walking speed of the healthy population. 16
SCI patients who walk independently in the community are on average years younger than patients who do not. This age effect was also found by Oleson et al, 26 who investigated the influence of age in patients with an AIS B graded SCI on the likelihood of being able to walk 1 year postinjury. Compared with younger patients, patients aged 50 years or older are less likely to regain walking function; 80% to 90% of the patients younger than 50 years could walk at 1 year postinjury versus only 30% to 40% of the patients 50 years and older. In normal aging, functional capacity gradually declines after about the age of 30 years, and SCI may potentially accelerate this process of decline. 27 Another hypothesis is that a higher age correlates with a worse recovery of muscle power and functional capacities. In addition, older patients might be less motivated to regain ambulatory capacity or might more easily accept the wheelchair for their outdoor mobility. Also, older patients might be more afraid of falling when walking, while sitting in a wheelchair feels secure. 28
Patients who ambulate independently in the community more often have AIS D or E SCI and higher walking speeds on the 10MWT than patients who do not. The motor scores for individual lower extremity muscles, including the UEMS and LEMS, were found to be significantly higher in patients who ambulate independently in the community than in patients who do not. This is in line with the current literature, which indicates that the muscle strength of the legs is strongly associated with functional walking performance.6,7,29 Kay et al 30 already showed that patients with an AIS C or D graded SCI are more likely to walk than patients with an AIS A or B injury; and patients with an AIS D injury are all likely to walk at discharge, regardless of their injury level. Hasegawa et al 31 found that in patients with an incomplete cervical SCI, LEMS and UEMS are the most important factors for community ambulation.
This study shows that patients need to be able to flex their hip and extend their knee against gravity to be able to independently ambulate in the community. The other leg muscle groups appear to be less important to regaining outdoors mobility. These results are similar to the findings of Kim et al, 7 who showed that hip flexor strength explains more than 50% of the variance in gait speed in patients with chronic incomplete SCI.
We investigated the efficiency of walking using walking speed, LEMS and UEMS for each score on the SCIM item 14 for community ambulation. van Hedel et al 32 defined categories of functional ambulation while using combinations of the SCIM items 12 and 14 for both indoors and outdoors mobility. The 5 categories are (1) patients who are dependent on a wheelchair, (2) patients who require supervision while walking indoors and use a wheelchair for longer distances outdoors, (3) patients who walk indoors without assistance but use a wheelchair outdoors, (4) patients who require a walking aid outdoors, and (5) patients who can walk without walking aids.
van Hedel et al 32 found the mean walking speed for each category to be (1) 0.01 m/s, (2) 0.34 m/s, (3) 0.57 m/s, (4) 0.88 m/s, and (5) 1.46 m/s. In our study, these categories corresponded with similar mean walking speeds except for the first category: (1) 0.31 m/s, (2) 0.32 m/s, (3) 0.47 m/s, (4) 0.86 m/s, and (5) 1.49 m/s. The walking speed for the first category in our study was significantly higher than that of van Hedel et al. 32 One explanation could be that patients without ambulatory capacity, who are therefore unable to perform a 10MWT, were excluded from our study due to the inclusion criteria.
Clinical Relevance
The 10MWT cutoff walking speed might be useful in clinical practice to assess whether SCI patients are likely to take part in the community as pedestrians. In addition to walking speed, the patient’s age and the strength of hip flexor and knee extensor muscles were found to be important distinguishing factors, which may be used to identify patients who have the potential to ambulate independently in the community. Rehabilitation training programs for patients with SCI that aim to restore outdoor walking capacity should focus on strength training of the hip flexors and knee extensors. The extent to which the second decimal of the walking speed cutoff of 0.59 m/s is relevant for clinical practice can be questioned. However, the 0.6 m/s threshold was confirmed when we analyzed the data in categories of 0.1 m/s walking speed; we found that at a walking speed of 0.6 m/s, more patients walk in the community than use their wheelchairs (see the Supplementary Information). Therefore, this cutoff walking speed could be used as a target for the innovation of orthotic devices like exoskeletons. Improving the speed those devices can ambulate with will make it more likely that, in the future, even nonambulating complete SCI patients may use them to ambulate independently in the community.
Study Limitations
In spinal cord research, a follow-up of 1 year post-injury is considered to be representative for the long-term outcome. 33 Van Middendorp et al 21 previously validated the use of a 6-month follow-up when there is no 1-year follow-up available. They observed a highly significant correlation in patients with both 1-year and 6-month follow-ups, therefore replacing the missing 1-year follow-up measurement with a 6-month measurement could be regarded as a valid approach. Moreover, this approach has been followed in previous studies.22,25
One might argue that the flat and regular surface on which a 10MWT is performed does not resemble the conditions in the community, which include irregular surfaces, steps, and curbs. However, literature shows that the 10MWT is a validated test to assess walking speed in daily life.8,9 The current study showed that walking speed on the 10MWT corresponds well with the outdoor mobility SCIM 14 scores, resulting in high specificity and sensitivity when discriminating between patients who walk in the community and those who do not.
The definition of independent community ambulation we used in this study was based on the SCIM outdoor mobility scores, as has been done in multiple previous studies.21-25 The cutoff for the SCIM scores may not be validated, but it is likely that patients with 4 to 8 points on SCIM item 14 would not use a wheelchair for distances of more than 100 meters and could be regarded as independent community ambulators. van Hedel et al 32 even considered supervised walkers (3 points on the SCIM item 14) to be community ambulators. Since our study focused on independent outdoor mobility, we did not consider supervised walkers to be independent community walkers; this is in line with other studies.22,25 However, supervised walkers have an average walking speed of 0.67 m/s and a mean LEMS of 45 points (Table 5), which is more similar to independent walkers than to non-walkers. Therefore, it is questionable whether supervised walkers should be considered independent community walkers.
In addition to walking speed, age, injury severity, and muscle strength, there are other factors that influence community ambulation and were not investigated in this study. A recent study showed that in stroke patients, factors like the intention to walk outdoors, social influence, self-efficacy and attitude toward physical activity influence whether patients walk in the community. Furthermore, outdoor ambulatory capacity in stroke patients is influenced by loss of balance, reduced walking distance and impairments of motor control, cognition and aerobic capacity, as well as fatigue. 34 These factors have not been investigated in the current study; however, they might explain why a small group of SCI patients with a relatively high or normal LEMS did not walk outdoors.
Conclusion
SCI patients who walk independently in the community are generally younger, have less severe injuries, have higher UEMS and LEMS, and should be able to flex their hips and extend their knees against gravity. SCI patients with a walking speed of 0.59 m/s and higher, as measured with the 10MWT, are predominantly independent community walkers. Proximal leg muscle strength training is an important goal for rehabilitation programs, and the walking speed cutoff of 0.59 m/s could be used in clinical practice to estimate whether patients are likely to walk or roll in the community.
Footnotes
Acknowledgements
All spinal cord injury centers participating in the EM-SCI network contributed to the study.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.