
Abstract
Background. Locomotor training using treadmills or robotic devices is commonly utilized to improve gait in cerebral palsy (CP); however, effects are inconsistent and fail to exceed those of equally intense alternatives. Possible limitations of existing devices include fixed nonvariable rhythm and too much limb or body weight assistance. Objective: To quantify and compare effectiveness of a motor-assisted cycle and a novel alternative, an elliptical, in CP to improve interlimb reciprocal coordination through intensive speed-focused leg training. Methods: A total of 27 children with bilateral CP, 5 to 17 years old, were randomized to 12 weeks of 20 minutes, 5 days per week home-based training (elliptical = 14; cycle = 13) at a minimum of 40 revolutions per minute, with resistance added when speed target was achieved. Primary outcomes were self-selected and fastest voluntary cadence on the devices and gait speed. Secondary outcomes included knee muscle strength, and selective control and functional mobility measures. Results: Cadence on trained but not nontrained devices increased, demonstrating task specificity of training and increased exercise capability. Mean gait speed did not increase in either group, nor did parent-reported functional mobility. Knee extensor strength increased in both. An interaction between group and time was seen in selective control with scores slightly increasing for the elliptical and decreasing for the cycle, possibly related to tighter limb coupling with cycling. Conclusions: Task-specific effects were similarly positive across groups, but no transfer was seen to gait or function. Training dose was low (≤20 hours) compared with intensive upper-limb training recommendations and may be insufficient to produce appreciable clinical change.
Introduction
Cerebral palsy (CP) is a group of disorders comprising the most prevalent childhood onset physical disability. The defining characteristic is a motor impairment that limits daily activities such as self-care and mobility. Intensive task-specific upper-limb training has been shown to be efficacious for improving hand function in children primarily with unilateral CP.1,2 However, intensive task-specific approaches in the lower extremity utilizing motorized treadmills or robotic devices have largely failed to produce similarly consistent positive outcomes or those superior to equally intense nondevice alternatives in CP3,4 or stroke. 5 This has prompted some researchers to recommend reconsideration of these approaches in neurorehabilitation. 6
Despite the lack of scientific consensus, the advent of intensive motor training paradigms has transformed neurorehabilitation practices and stimulated consideration of training characteristics that may predict effectiveness.7,8 Nudo 9 emphasized that both quantity and quality of motor experience can influence brain plasticity and functional recovery after brain injury. With respect to quantity, the amount of repetition or practice is a key ingredient in fostering motor learning; however, he noted that the amount of repetition in clinical trials is often far less than in animal studies, suggesting that rehabilitation may be largely underdosed. Constraint-induced movement therapy (CIMT) is one of the highest-dosed therapies in neurorehabilitation. Dose-response in CIMT has been evaluated in CP, and minimum dosing thresholds for producing clinically important changes in functioning have been proposed.10,11 Insights from trials in CP suggest that 30 hours is insufficient, and although 60 hours can produce clinically significant effects, 90 hours may produce greater and more lasting benefits. 10 Interestingly, results from CIMT are similar to those from other intensive paradigms, such as bilateral training, when doses are equivalent,11,12 supporting the importance of sufficient repetition.
Several qualitative aspects to enhance treatment effectiveness have been proposed, including greater salience or meaningfulness to the learner, 8 more physical and mental engagement during training, 8 and a more flexible and variable underlying rhythm that may reduce spinal habituation, which can occur during rote, repetitive tasks. 13 Therefore, treadmill training at a constant belt speed or using a motorized gait orthosis that can passively move the limbs at a fixed pace may understandably not prove superior to alternatives such as overground walking or activity-based therapies that require more effort. An electroencephalography study during treadmill walking in adults demonstrated greater activity in brain regions involved in motor planning and performance when participants actively controlled treadmill speed rather than responding passively to speed changes. 14 Recent implementation of more adaptive and engaging control strategies or feedback in robotic gait training are demonstrating positive outcomes,15,16 yet comparisons of these with equivalent dose alternatives or previous control systems have not yet been reported.
In addition to robotic or treadmill-based gait training, functional electrical stimulation–assisted or standard stationary cycles have been utilized to improve lower-extremity strength, endurance and/or function in CP. Three studies17-19 have reported mostly positive mean results after approximately 15 hours of cycling in each study, yet results failed to be significantly greater than those from a randomized nonintervention group in 1 study. 17 Although not as directly task specific to walking as treadmill training, 20 cycling shares the same neural circuitry as walking.21-23 Therefore, it is reasonable to propose that repetitive practice on a cycle could improve reciprocal interlimb coordination 24 and thereby enhance stepping performance. Elliptical training is even more closely task related to walking, 20 but no studies have yet been published utilizing this device for locomotor training in CP. Additionally, unlike treadmill protocols, pedal resistance can be added to both devices to increase the strengthening load and/or the aerobic level. 18 In contrast, harnessed or other weight-support systems, such as robotic exoskeletons, may reduce limb loading and the degree of lower-limb strengthening. Harnessed walking also restricts trunk movements. In those with CP who can already perform stepping movements, step training alone may not be very beneficial, but the combination of this with postural training, versus support, and leg strengthening could potentially be more effective. Adequate postural control is a rate-limiting factor in the development of independent walking 25 and is directly related to functional mobility in CP. 26 Use of a stationary cycle, particularly when performed in a supported or recumbent sitting position, also does not require postural control and coordination with leg movements, whereas an elliptical challenges balance control and requires coordination of the trunk and limbs with no weight support provided. The device most similar to an elliptical investigated in CP was an electromechanical Gait Trainer that also supports and moves with the feet; however, in contrast, the speed is motor driven. A randomized trial comparing ten 30-minute sessions on the device focused primarily on increasing movement speed plus 10 minutes of joint mobilization and stretching to 10 sessions of 40 minutes of conventional therapy found improvement in the 10-m and 6-minute Walk Tests for the experimental group after only 5 total hours on the device. 27
The main objective here was to evaluate and compare 2 alternatives to treadmill or robotic-assisted gait training, a motor-assisted stationary cycle designed specifically for rehabilitation and a pediatric elliptical device, for improving gait function in children with bilateral CP. The primary outcome of interest was improved lower-limb reciprocal coordination, with the ultimate aim of improving stepping cadence and thereby increasing gait speed. Training focused primarily on having the children move their legs as quickly as possible in the devices and progressively increase speed first, then resistance.
We hypothesized that both device groups would demonstrate improved reciprocal coordination, as measured by increased voluntary cadence on each device as well as increased gait speed at both a self-selected and an “as fast as possible” pace. Within-subject changes during training would also be greater than during a 3-month no-exercise period. We further hypothesized that all would show improvements in secondary outcomes at the International Classification of Functioning, Disability and Health levels of Body Structures and Functions—that is, knee extensor strength and Selective Control Assessment of the Lower Extremity (SCALE) 28 —and Activity and Participation—that is, the computer-adapted version of the Pediatric Evaluation of Disability Inventory (PEDI-CAT) 29 and the Pediatric Outcomes Data Collection Instrument (PODCI). 30 Finally, we hypothesized that outcomes for the elliptical would be significantly greater than that for cycling because of its greater task-specificity to walking and active use of all 4 limbs and the trunk.
Methods
Participants
A total of 27 children with bilateral spastic CP, and a mean age of 10.3 years, ranging from 5.0 to 17.6 years old, 8 male, 19 female, Gross Motor Function Classification System (GMFCS) levels I to III, participated in this study from 2010 to 2015, with no dropouts or withdrawals. A power analysis based on pilot (unpublished) motor-assisted cycling data in children with CP, GMFCS III and IV, indicated that 24 participants, 12 per group, were needed to detect a 20 revolutions per minute (rpm) gain with 80% power. Table 1 presents participant characteristics separated by device group. Although mean weight, height, and age were higher in the elliptical group (P = .09, .09, and .13, respectively), the differences were not significant. Children were recruited through our laboratory database and through Institutional Review Board approved flyers sent to local physicians and therapists who care for children with CP.
Participant Characteristics and Baseline Values for All Outcome Measures, by Device Group, With Associated P Values and Significance Indicated in Bold (P < .05). a
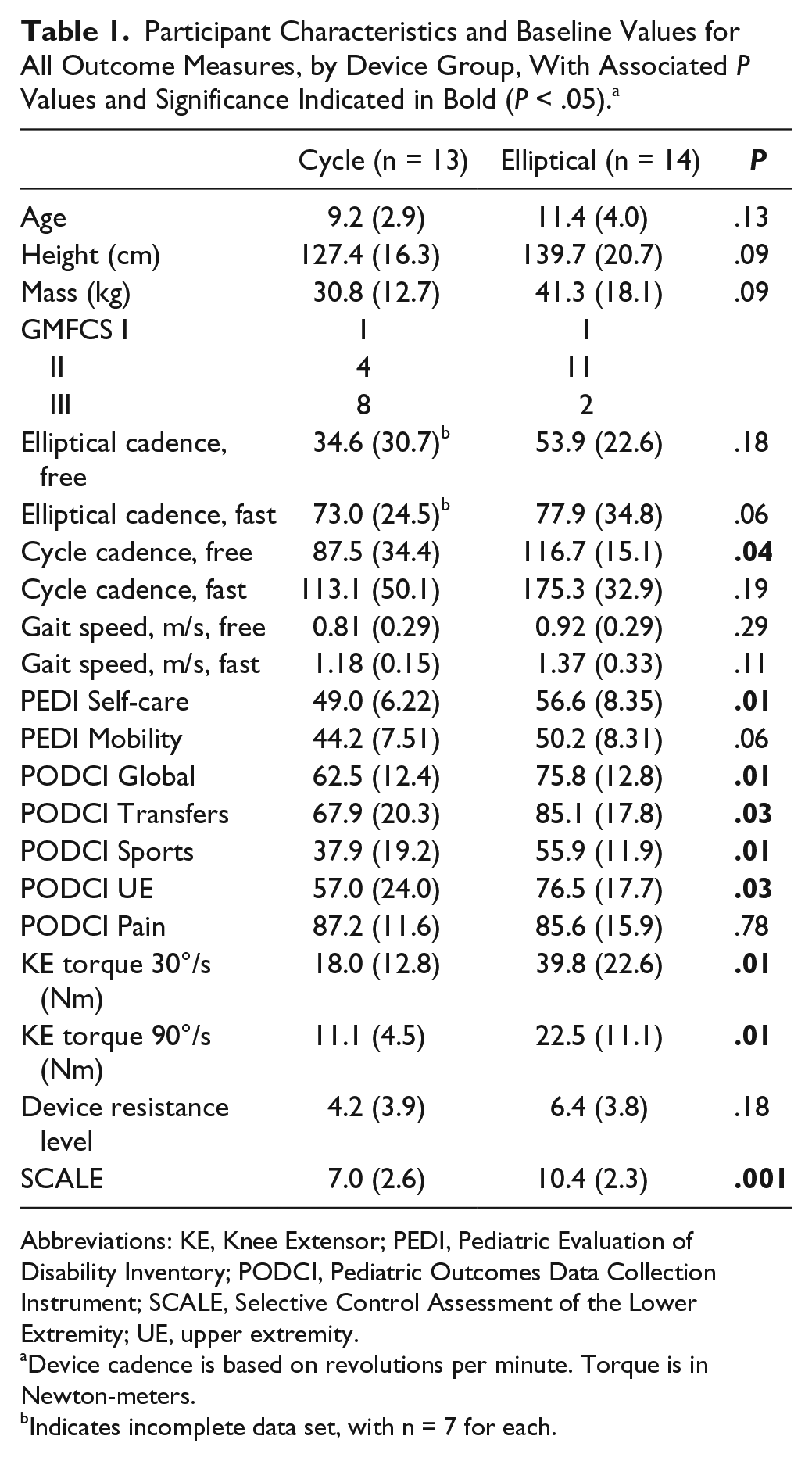
Abbreviations: KE, Knee Extensor; PEDI, Pediatric Evaluation of Disability Inventory; PODCI, Pediatric Outcomes Data Collection Instrument; SCALE, Selective Control Assessment of the Lower Extremity; UE, upper extremity.
Device cadence is based on revolutions per minute. Torque is in Newton-meters.
Indicates incomplete data set, with n = 7 for each.
Inclusion criteria were the following: (1) ages 5 to 17 years inclusive; (2) diagnosis of bilateral CP; (3) GMFCS levels I to III; (4) preterm birth (34 weeks of gestation or less); (5) periventricular leukomalacia verified by magnetic resonance imaging; (6) no surgery within a year and no lower-limb muscle injections within 4 months; (7) ability to follow simple directions, and perform and complete the exercise program as judged by a parent and/or referring therapist or physician; (8) not currently participating in locomotor device training. The inclusion criteria of preterm birth and periventricular leukomalacia were to increase the homogeneity of the study population with all likely to have white matter injury. The protocol (No. 10-CC-0073) was approved by the institutional review board at the National Institutes of Health; written informed consent was obtained from a parent, and verbal assent was obtained from each child.
Rationale for Choice of Training Devices
The primary training goal was to encourage active self-paced reciprocal leg movement at increasingly faster velocities with minimal external assistance. The cycling device selected here (MOTOMed gracile, RECK, Germany) has a unique servomotor that can initiate the motion and maintain it at a low cadence for those who cannot start or maintain a continuous cycling rhythm; however, to encourage children to control their own pace as much as possible, the target for all children was to exceed the cadence on the machine to take over control of the cadence themselves. Once in control, the rhythm becomes more flexible and variable and requires greater voluntary effort, as opposed to a rote, invariable speed that encourages greater passivity or automaticity. We anticipated that all children with bilateral CP GMFCS levels I, II, and III would be capable of using the cycle with minimal practice. Because no study had yet been performed in CP using elliptical devices, we were uncertain whether all would be able to use this well enough to participate in training. Elliptical cadence is totally driven by the user and, therefore, more challenging. However, the elliptical has the attractive advantage that upper limbs can assist lower-limb movement as needed until children can more fully use their lower limbs. The ability to increase pedal resistance in both devices may not only improve leg strength in addition to coordination, 18 but also increase the amount of muscle (electrical) activation or sensory input ascending from spinal pathways to the cortex, thus enhancing the neuroplastic effects of training. 31 The elliptical further requires reciprocation of all 4 limbs, which could further enhance sensorimotor stimulation. The elliptical device selected for this study (Cardiokids, Kidsfit, Huger, SC) was designed specifically for children and had resistance settings from 1 to 10.
Procedures
The study design consisted of randomization of participants after enrollment using a randomly generated, by a statistician, order of assignment to 1 of 2 device groups: elliptical or cycle. This list was maintained by the PI and not revealed to the members of the study team who enrolled all participants until after enrollment. However, at the initial assessment, 6 participants were found to be either too short to comfortably reach the elliptical handles, even though it was designed for those 5 years of age and older, or were unable to move the elliptical pedals in a continuous manner for 30 s with no resistance. Three of those had been assigned to the elliptical group (1 was too small, and 2 could not pedal continuously; all were GMFCS level III). Randomization had to be broken in these cases, and the statistician recommended that they be assigned instead to the next cycle condition on the list. That condition regardless of location on the list was then replaced with the unfilled elliptical condition for future assignments. The other 3 had been assigned to the cycle group but were all also GMFCS level III, with one who was 5 years old having difficulty reaching and holding onto the handles. However, 2 other 5-year-old children, both GMFCS level II, one of whom was the smallest child in the study, were able to train with the elliptical. No child was too small for or unable to use the cycle.
Each participant was tested 3 times at 3-month intervals, and training occurred either in the first or second 3-month interval depending on device availability at enrollment. The number of devices for this study was limited because of their expense ($3000 each). If a device was available at enrollment, the child started training immediately and was followed for another 3 months after the training ended. If a device was not yet available, the child was followed for a 3-month baseline period, then received a second assessment prior to training, with their last visit being the posttraining assessment.
Exercise Intervention
In this study, the cycle servo motor was set to only assist cadences below 20 rpm. Families were given written instructions on how to use the computerized cycle, which were reviewed prior to having the device delivered to their home. The elliptical device was simpler to operate, and this was also reviewed with the family prior to delivery. The resistance settings were 1 to 20 on the cycle; however, to be more consistent with the elliptical, we used only even numbers as increments for progression. Each family was contacted every 2 weeks throughout training by the therapist to evaluate exercise safety and compliance and to ascertain training parameters such as current speed and duration as well as level of resistance if any. If a child had met the target cadence and had maintained it for a week, the resistance was increased by 1 increment unless the child went below the target speed and the level of exertion was so high that the child could not talk easily while training. If either occurred, the child was to continue working on increasing speed and to try to add resistance the following week.
For all participants, the assigned device was delivered to their home, and they were instructed to exercise above 40 rpm for 20 minutes, 5 days a week for 12 weeks. Children were instructed to wear shoes when exercising to protect their feet, but not ankle foot orthoses. The goal was to complete at least 90% or 54 of 60 total sessions, allowing them to miss some sessions as a result of illness or vacation. Through parent report (24/27 participants with completed log sheets, with 2 in the cycle group and 1 in the elliptical group failing to complete them), the mean number of completed sessions was 57.3, with only 2 participants (both in the elliptical group) reporting fewer than 54 sessions completed.
Data Collection
All children participated in 3 assessments approximately 3 months apart at a national research hospital in Bethesda, MD. Assessments were to be performed within 1 week prior to the start and 2 weeks after completion of the intervention. The primary outcomes, voluntary device cadence and gait speed, were based on 3D gait analysis, and the same standardized data collection procedures were followed for all 3 assessments. A 10-camera motion capture system (Vicon Motion Systems, Denver, CO) was used to quantify self-selected and fast paces for barefoot walking and voluntary cycling and elliptical cadences. All children were tested on both devices, unless they were too small for or unstable on the elliptical. Those who could stand on the elliptical safely but had difficulty pedaling were still assessed each time. Five cycles of each condition were collected and only the temporal-spatial data are reported here. However, revolutions during device trials were determined by tracking foot motion over time, averaged within each trial. The secondary strength or selective control measures were not blinded, and the same therapist who performed these, with assistance as needed from other members of the research team, also trained children on each device and followed up with the family. To reduce bias, results of prior assessments were not available during subsequent assessments. One therapist-administered assessment was the SCALE, which compares voluntary ability to move 5 lower-extremity joints per limb independently of others within passive limits. 28 Scores per joint range from 0 to 2, with 10 points the maximum (best) score per limb and 20 for the total score.
Knee flexor and extensor muscle group isokinetic peak torques (Nm) at 30°/s and 90°/s were recorded at each assessment. All participants were positioned on the Biodex System 3 (Shirley, NY) isokinetic dynamometer in a supported semireclined sitting position with the knee joint aligned with the dynamometer axis. A resistance test on the trained device was also performed at each assessment to evaluate the ability to withstand and maintain pedal resistance at a relatively fast pace initially and after training. They were asked to maintain pedal speed at 20 rpm as resistance was added by 1 level every 30 s until the rate dropped below 20 rpm for more than 5 s. The highest resistance level achieved prior to that was recorded.
Two computer-based functional parent (proxy) reported outcome measures, the PODCI (version 1.36) and PEDI-CAT (version 2.5), both in English, were used to determine the child’s functional capabilities. The same parent completed these at all assessments. Both measure functional mobility as well as self-care or upper-extremity function. The PEDI-CAT yields a single score scaled from 0 to 100 for both Mobility and Self-care, with higher scores indicating greater function. The PODCI has a Global Function Score that includes 4 subscales, which also can be evaluated separately: Transfers and Basic Mobility, Sports and Physical Function, Upper Extremity, and Comfort/Pain. Scores ranged from 0 to 100 on each, with higher scores indicating less disability.
Statistics
A general linear mixed-model design was used to assess the effects of time (pretraining vs posttraining) and group (elliptical or cycle) on the primary and secondary outcomes. Change scores for the primary outcomes were also compared during the nonexercise (3-month baseline or follow-up) and exercise periods across device groups using a general linear mixed model with P <.05 (SPSS Version 22; IBM Corporation, Armonk, NY). Change scores for device cadences over the training period were compared across groups and were also correlated with changes in knee extensor torque and the increase in the amount of pedal resistance during training using Pearson’s r (P < .05) to assess the extent to which strength changes or greater training effort were related to outcomes.
Results
Primary Outcome Measures
Voluntary coordination on the trained device, assessed by device cadence at self-selected and fast speeds for all participants, improved markedly and significantly as a result of training (see Table 2). With the exception of the self-selected cycle condition, results differed across device groups, and all device comparisons showed a significant interaction indicating that the groups behaved differently over time. Specifically, this indicated that the elliptical group had greater gains on the elliptical and the cycle group on the cycle, which reflected the task specificity of the training. No significant transfer to increased cadence on the nontrained devices was seen; however, a trend toward increased elliptical cadence was found in the cycle group (P = .063 free and .054 fast).
Mean Values of Primary Outcomes Before and After Training in Each Device Group, With P Values for Main Effects for Group and Time, and Interaction of Group and Time (G × T). a
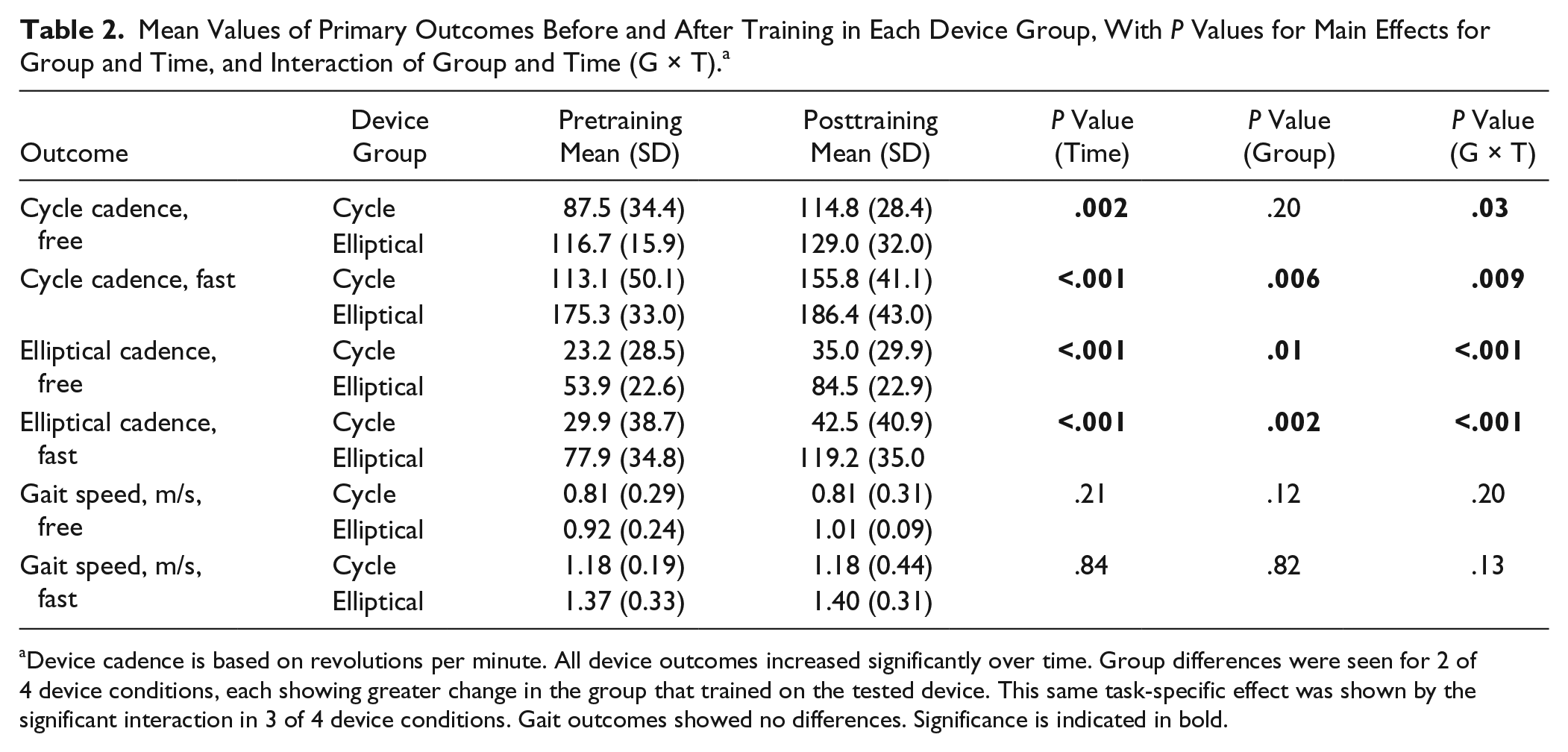
Device cadence is based on revolutions per minute. All device outcomes increased significantly over time. Group differences were seen for 2 of 4 device conditions, each showing greater change in the group that trained on the tested device. This same task-specific effect was shown by the significant interaction in 3 of 4 device conditions. Gait outcomes showed no differences. Significance is indicated in bold.
Because some children had their 3-month no-exercise period before and some after the training, changes in outcomes for each period were first compared using paired t-tests and not found to be statistically different. We then combined the change scores for these periods and compared these to the changes as a result of training. Again with the exception of the self-selected cycle condition (mean difference = +17.5 steps/min during training; P = .25), gains during training were significantly higher than during the no-training period (Figure 1). Notably, only 2 participants had a decrease in device cadence after training, and in both, the trained device was the cycle and the decrease was only in the self-selected pace, whereas a large increase was seen for each in the fast pace. No significant changes were seen in gait speed for time or group, with the means for the 2 periods virtually identical in the cycle group; however, a strong trend toward increased self-selected gait speed (data missing for 1 participant who only had fast speed data) was seen for the elliptical group (P = .054; Table 2). Figure 2 shows individual results for that condition by group.
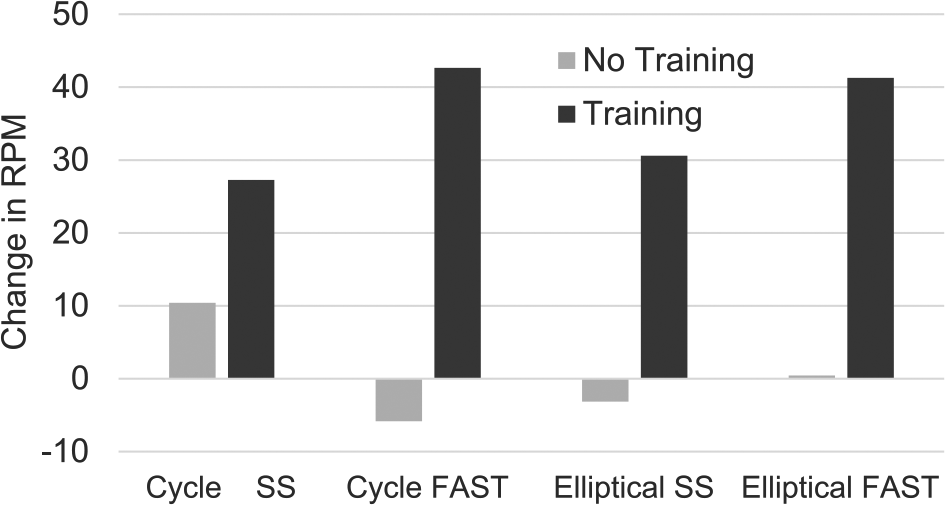
This shows the mean change in revolutions per minute (rpm) within device groups for both self-selected (SS) and fast speeds, with the darker bars representing the change after the 3-month training and the lighter bars showing the amount of change in the 3-month no-training period.
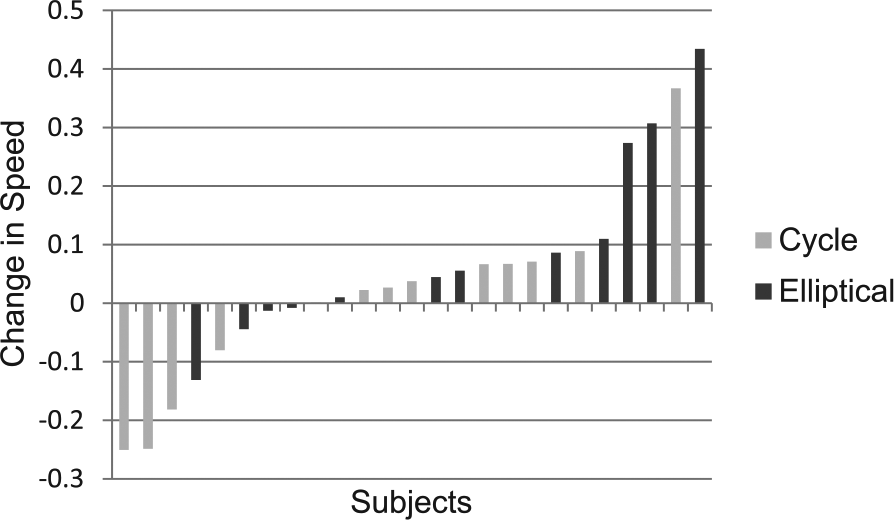
This shows the individual results for change in freely selected gait speed for participants by device group, with those in the cycle group represented by the lighter bars and those in the elliptical group by the darker bars.
Secondary Outcome Measures
Complete data sets were available for all secondary outcomes, with results summarized in Table 3. Isometric and isokinetic knee extensor and flexor strength at 30°/s did not increase significantly, but there was a significant increase at 90°/s in the knee extensors only over time. No group interaction was found, suggesting that the groups behaved similarly; however, the device groups did differ in absolute strength, with the elliptical group having consistently higher values. No significant correlations between changes in device cadence with knee extensor torques at 30°/s or 90°/s were found (P = .62 and .63 for free cadence; P = .87 and .97 for fast cadence).
Results for Secondary Outcomes Showing That Strength and Device Resistance Increased Over Time in the Entire Sample. a
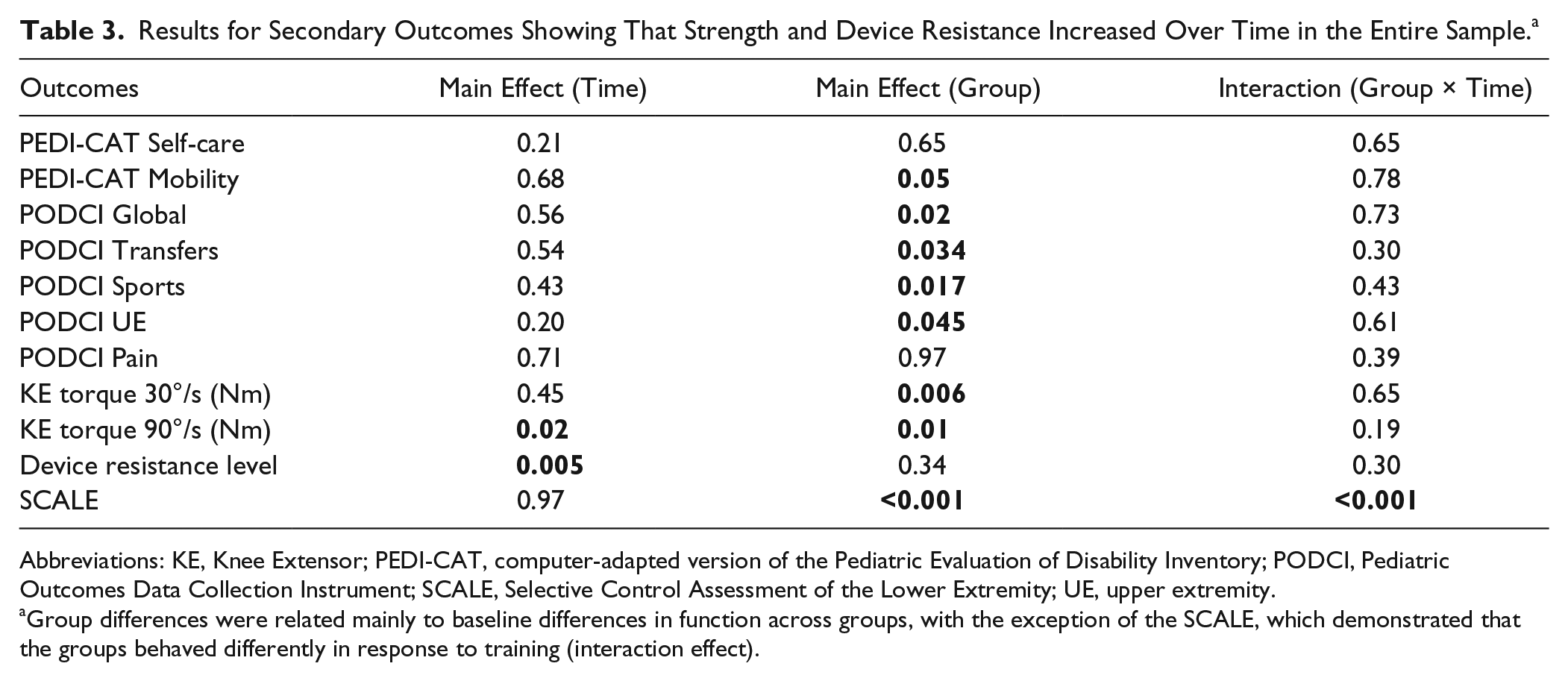
Abbreviations: KE, Knee Extensor; PEDI-CAT, computer-adapted version of the Pediatric Evaluation of Disability Inventory; PODCI, Pediatric Outcomes Data Collection Instrument; SCALE, Selective Control Assessment of the Lower Extremity; UE, upper extremity.
Group differences were related mainly to baseline differences in function across groups, with the exception of the SCALE, which demonstrated that the groups behaved differently in response to training (interaction effect).
The resistance test results were similar to the faster speed isokinetic test in that the resistance increased over time, with no differences between groups and no interaction. A greater increase in resistance over the training period measured in the laboratory was moderately correlated with greater gains in fast device cadence (r = 0.60; P < .05). We also tracked progression in resistance during training and found that increased device cadence was related to progressive increases in training effort as measured by increased levels of resistance with r = 0.53 (P < .01) for free and r = 0.54 (P < .01) for fast cadences. There were no differences across groups in the amount of progression in training resistance (P = .30).
SCALE results showed no main effect for time (P = .97); however, a significant difference for group (P < .001) and a Group × Time interaction (P < .001) were seen, with the elliptical group showing a small increase and the cycle group a small decrease in scores after training.
No significant main effects for training compared with no training periods were seen in the PEDI-CAT Self-care and Mobility domains or in the PODCI Global Function Score or subscales. A significant main effect for device group was seen for all scales and subscales except for PEDI-CAT Self-care and PODCI Comfort/Pain, which likely reflected the higher baseline function of the elliptical group. Only the cycle group showed negative mean differences after training in some outcomes, none of which was significantly worse (Table 4).
Pretraining to Posttraining Results by Device Group, Including Mean Difference, 95% CI, and Effect Size. a
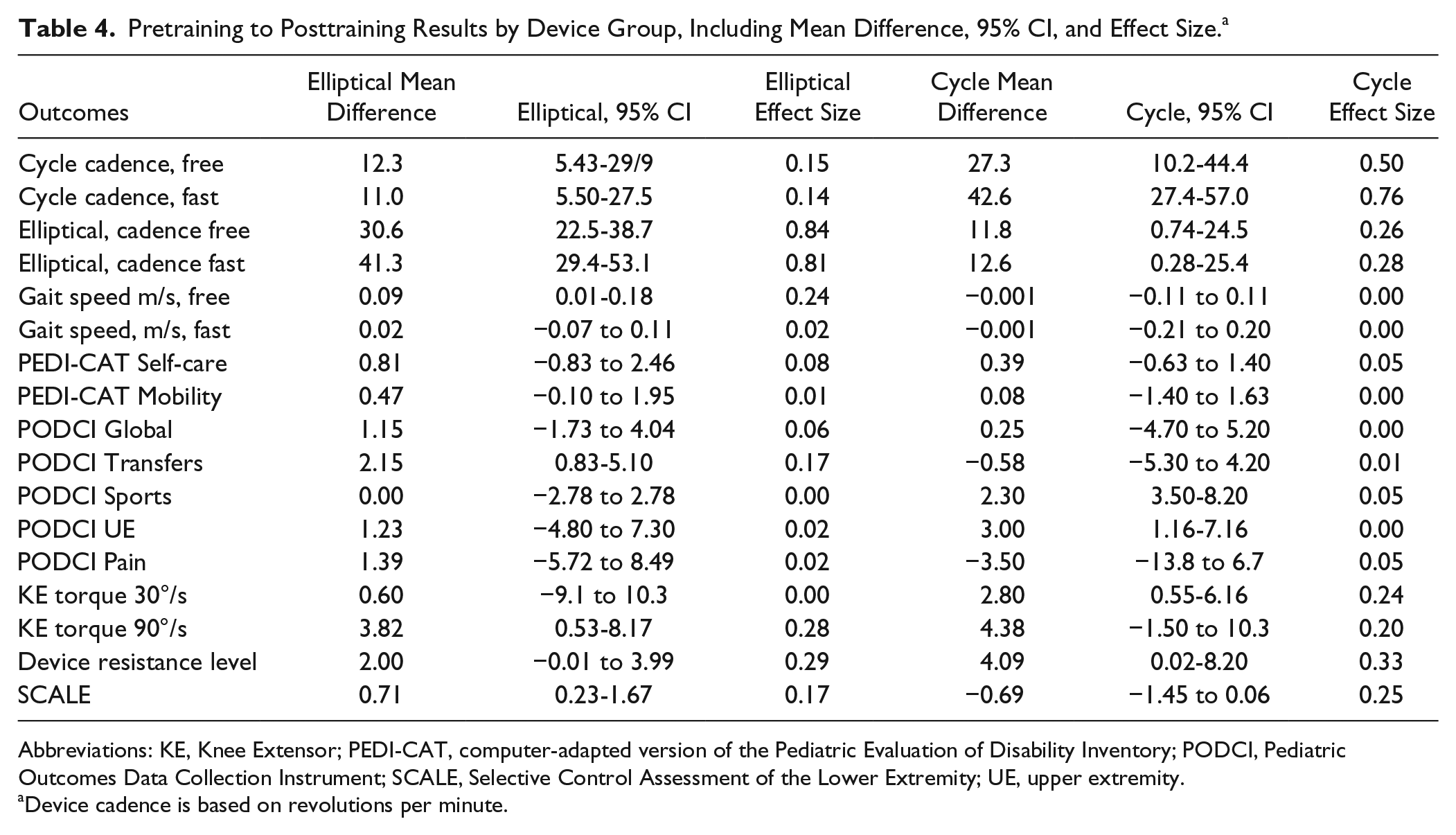
Abbreviations: KE, Knee Extensor; PEDI-CAT, computer-adapted version of the Pediatric Evaluation of Disability Inventory; PODCI, Pediatric Outcomes Data Collection Instrument; SCALE, Selective Control Assessment of the Lower Extremity; UE, upper extremity.
Device cadence is based on revolutions per minute.
Discussion
The first hypothesis stated that device cadence would increase as a task-specific effect of training. This was supported in that for both device groups, the major change after training was a marked increase in device cadence, with the high maximum cadences achieved particularly remarkable. A potential advantage of each of these devices over treadmills that may have facilitated this outcome is the apparently greater ease in producing a faster cadence that is closer to normal walking cadence as well as a more variable one because the pace was self-initiated rather than externally imposed.
The underlying neural premise here was that children with bilateral CP often seem to experience difficulty when required to perform asynchronous leg tasks that may be partly a result of an underlying deficit in reciprocal coordination. Abnormal development of spinal interneurons after early brain injury have been identified and have been found to affect motor prognosis and the later development of the corticospinal tract and the motor map. 32 Speed-focused training may help children more rapidly turn their muscles on and off as needed to perform alternating leg tasks. The ability to increase speed or cadence with training was clearly and dramatically shown here but was specific to the device, at least at the dose delivered here, and was related to progressively greater effort (resistance) during training. Interestingly, peak torque production at the fastest isokinetic speed also increased significantly, although it was not related to speed outcomes. This increase is notable because a deficit in the rate of producing force is more pronounced and functionally relevant than weakness in CP 33 and has been shown to respond differentially to high velocity training. 34 However, increased training resistance accounted for only a small portion of the variance (R2 = 0.36) in increased device cadence, suggesting that additional factors such as improved reciprocal coordination may have been responsible for the change. It is also possible that the increased resistance produced greater electrical input from muscles to the brain, which may have helped improve motor coordination as well; however, these hypotheses will require further investigation. The maintenance of device cadence 3 months after training in those with a postintervention follow-up further suggests that the change was more likely a result of improved motor coordination rather than strength changes, which would have been more transient.
Reciprocal or interlimb coordination for walking primarily involves the proximal hip musculature to either advance the limb forward or be stretched passively as the opposite limb advances. Intralimb coordination is fundamentally different, that is, whether one joint can move independently of others in the same limb. We utilized the SCALE here to assess selective control before and after training; however, this test primarily evaluates intralimb control, which may help explain why both device groups could have had similar increases in cadence as a result of improvements in interlimb coordination, whereas their results on the SCALE, although not statistically or clinically significant 35 in the group comparison, were in opposite directions, which led to a significant interaction. Ankle movements on the elliptical are not tightly coupled to the hip or knee because they are on the cycle, which may have caused the small divergence in changes in intralimb control for the elliptical and cycle. Similarly, individual results for gait velocity were more positively skewed for those in the elliptical group and more negatively skewed for those in the cycle groups, with 4 of 5 participants showing a clinically significant 0.1-m/s improvement being in the elliptical group and 3 of 4 showing a 0.1-m/s decrease being in the cycle group. Although these individual trends were not supported by significant group differences or a Group × Time interaction, potential differences in training regimens warrant further evaluation. However, it is important to note that more than two-thirds of all participants in each group improved in gait speed after training.
One major limitation of this study was that the comparison of outcomes across device groups was undermined by the inability to randomize some children to the elliptical group because of smaller physical size and/or greater motor impairments. The 2 groups, although not significantly different in age, weight, or height in this relatively small sample, did show a disproportionate distribution in GMFCS levels II and III, with many more in the cycle group classified at lower functional levels, a difference that was reinforced by significantly lower PODCI scores, PEDI Self-care scores, and nonnormalized strength values in that group as well as lower cycle cadence at free speed. The elliptical required greater baseline coordination, and interestingly, 1 child in the cycle group who could not continuously pedal the elliptical at baseline was able to do this quite proficiently after the cycle training, suggesting that children who are less functional could be progressed to this more challenging device. The elliptical cadence for those in the cycle group was the only outcome with incomplete data having no pre-post data in 6 participants, with 1 of the 6 who could not do it at baseline able to do this after training. Other study limitations included nonblinding of therapists who conducted the isokinetic torque and SCALE assessments and the fact that the 3-month nontraining period differed across individuals, with some having a double baseline before training and others a follow-up after training. This was done to expedite enrollment as devices became available.
This randomized trial, by demonstrating that children with bilateral CP could significantly increase both speed and resistance on the trained device, suggests that these devices could provide new options for achieving fitness goals in CP. Cycling places far less compressive stress on the joints than treadmill walking, a factor that will be increasingly important as the length of time these devices are utilized increases. Elliptical trainers involve a motion that is similar to cycling, but involves stepping plus limb loading in upright that more closely simulates over ground or treadmill walking. These also have smaller joint impact forces compared with treadmill walking. 36 Many individuals with CP experience earlier and greater joint deterioration because of their abnormal loading patterns and the high impact forces they may experience during walking, which may lead to a cessation of walking in adulthood. 37 Therefore, it is critically important that any long-term exercise or therapy does not significantly exacerbate joint stress and deterioration.
The second half of the first hypothesis that training would lead to improvements in gait speed as a result of training was not supported here. A recent systematic review of interventions for children with CP aimed to improve gait speed demonstrated that gait training was the most effective in increasing gait speed, with resistance training not shown to be effective, with the exception of high-velocity (power) training. 38 Given the task specificity of gait training, this finding is not entirely surprising. The frequency of interventions, but not total doses, were reported in the review. We believe that our lack of significant changes in gait speed here for each group as a whole may have been a result of the fact that the maximum total training dose for any participant was only 20 hours. This is far less than the minimal dose hours associated with positive outcomes from upper-limb training, so it is possible that with extended training, the elliptical device in particular could ultimately have positive effects on gait and other aspects of gross motor function, assuming that the trends were sustained over time. Many, if not most, studies on locomotor training and cycling in CP have used even lower total doses; therefore, dosing studies on locomotor training paradigms should be performed in CP before concluding that these are not effective. Similar to strength training in the lower extremities, it may take far more training before functional benefits become evident. 39
The parent (proxy) report measures of their child’s physical function also did not change after training. The sensitivity of the selected secondary functional measures for measuring changes after physical therapy is also a consideration, with the PODCI showing greater responsiveness to change for surgical interventions 40 and with the PEDI-CAT not as well studied in older children and those with chronic conditions.41,42 It is possible that a condition-specific evaluative measure such as the GMFM-66 or computer-adapted test such as the recently published CP LE CAT 43 may have been more responsive.
Although devices have featured prominently in locomotor training, Bleyenheuft et al 44 challenged this practice by presenting significant positive results on the 6-minute walk test and the ABILICO functional mobility measure from intensive bilateral upper- and lower-limb training of approximately 80 hours compared with the same dose of conventional therapy, based on the Bobath method, which has been shown not to be effective. 2 The much higher training dose in that study is notable and warrants comparison to other activity-based or device-augmented therapies of equal doses.
The strengths of this study were the implementation of 2 novel devices in CP; the high compliance rate; a fairly homogeneous study group, in that all were born preterm and had diffuse white matter injury with resultant spastic CP; and absence of significant adverse events. Limitations were failed randomization in some participants that compromised the functional equivalence of study groups. This could be addressed in the future by adding size criteria and giving participants more opportunity for practice on the elliptical prior to training.
Concluding Remarks
Intense leg training with a motor-assisted cycle and elliptical device produced large task-specific changes that could enable children with CP to exercise at higher speeds and aerobic levels than before training. The primary aim to improve gait and gross motor function was not achieved, although positive individual and mean trends were seen mainly in the elliptical group that may become more evident with longer training. Highly effective therapies for improving gait and gross motor function still remain elusive in CP, with inadequate dosing likely being a factor.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Intramural Research Program of the National Institutes of Health Clinical Center (Protocol # 10-CC-0073).