
Abstract
Background. Following biceps transfer to enable elbow extension in individuals with tetraplegia, motor re-education may be facilitated by greater corticomotor excitability. Arm posture modulates corticomotor excitability of the nonimpaired biceps. If arm posture also modulates excitability of the transferred biceps, posture may aid in motor re-education. Objective. Our objective was to determine whether multi-joint arm posture affects corticomotor excitability of the transferred biceps similar to the nonimpaired biceps. We also aimed to determine whether corticomotor excitability of the transferred biceps is related to elbow extension strength and muscle length. Methods. Corticomotor excitability was assessed in 7 arms of individuals with tetraplegia and biceps transfer using transcranial magnetic stimulation and compared to biceps excitability of nonimpaired individuals. Single-pulse transcranial magnetic stimulation was delivered to the motor cortex with the arm in functional postures at rest. Motor-evoked potential amplitude was recorded via surface electromyography. Elbow moment was recorded during maximum isometric extension trials, and muscle length was estimated using a biomechanical model. Results. Arm posture modulated corticomotor excitability of the transferred biceps differently than the nonimpaired biceps. Elbow extension strength was positively related and muscle length was unrelated, respectively, to motor-evoked potential amplitude across the arms with biceps transfer. Conclusions. Corticomotor excitability of the transferred biceps is modulated by arm posture and may contribute to strength outcomes after tendon transfer. Future work should determine whether modulating corticomotor excitability via posture promotes motor re-education during the rehabilitative period following surgery.
Keywords
Introduction
After spinal cord injury (SCI) at the C6 or C7 cervical level, individuals retain active elbow flexion but lack active elbow extension due to triceps paralysis. Voluntary control of elbow extension significantly improves functional abilities and independence for individuals with tetraplegia resulting from SCI. Active elbow extension can be enabled in these individuals via surgical transfer of the distal tendon of the nonparalyzed biceps to the insertion of the paralyzed triceps (referred to as biceps transfer hereafter).1,2 Following biceps transfer, individuals must learn to activate the transferred biceps in its new function to extend the elbow. Motor re-education of the transferred biceps may be facilitated by increased excitability of the corticomotor pathway projecting to the transferred biceps (neural pathway that originates in the motor cortex, descends the corticospinal tract, and innervates biceps muscle fibers). Corticomotor excitability of upper limb muscles in nonimpaired individuals can be increased by positioning of the arm.3,4 When the nonimpaired upper limb is positioned in postures associated with increased corticomotor excitability, there is evidence that the sense of effort during contractions is decreased, 3 and the gain between the muscle electromyography (EMG) and isometric muscle force is altered such that a lower level of EMG is needed to produce a specific force magnitude. 5 Thus, identifying arm postures in which the corticomotor pathway to the transferred biceps is most excitable could aid in motor relearning for individuals with tetraplegia.
Corticomotor excitability of the nonimpaired biceps at rest is modulated in a consistent manner according to the multi-joint position and orientation of the upper limb. 4 Specifically, the amplitude of the motor-evoked potential (MEP) recorded from the nonimpaired biceps in response to transcranial magnetic stimulation (TMS), a measure of corticomotor excitability, is greater when the arm is positioned in the horizontal plane, relative to other functional arm postures. 4 Also, when the forearm is fully supinated for a given static orientation of the shoulder and elbow, MEP amplitude recorded from the nonimpaired biceps is consistently greater relative to MEP amplitude recorded with the forearm oriented in neutral or fully pronated.4,6
Whether corticomotor excitability of the transferred biceps at rest is modulated by multi-joint position and orientation of the upper limb similar to the nonimpaired biceps remains unknown. Differences in the biceps anatomy and function, nervous system organization and function, and behavioral demands between individuals with tetraplegia and nonimpaired individuals may alter posture-dependent excitability of the transferred biceps relative to the nonimpaired biceps. Evidence that muscle anatomy and function play a role in posture-dependent excitability comes from the different effect of identical arm postures on corticomotor excitability of the nonimpaired posterior deltoid relative to the nonimpaired biceps. 4 Behavioral demands may also alter posture-dependent excitability because training and skill acquisition affect corticomotor excitability, although most current evidence for this comes from cortical reorganization poststroke.7,8 Only Beekhuizen and Field-Fote have investigated cortical excitability after functional training in individuals with tetraplegia; they found that functional training increased cortical excitability of thenar muscles. 9 Thus, corticomotor excitability of the transferred biceps may differ relative to the nonimpaired biceps in upper limb postures that are frequently used by wheelchair-bound individuals with tetraplegia.
The purpose of this study was to determine whether multi-joint arm posture affects corticomotor excitability of the biceps after SCI and tendon transfer similarly to the nonimpaired biceps (nonimpaired data previously reported by Mogk et al 4 ). We hypothesized that posture-dependent corticomotor excitability of the transferred biceps would differ relative to the nonimpaired biceps. Corticomotor excitability of arms with biceps transfer was assessed using TMS. We also aimed to determine whether corticomotor excitability of the transferred biceps is related to maximum isometric elbow extension strength and muscle length. The results of this study will inform whether corticomotor excitability may be modulated by arm posture to potentially enhance motor re-education and strength after biceps transfer.
Methods
Subjects
Corticomotor excitability was assessed in 7 arms of individuals with cervical SCI who had undergone biceps transfer. Nine individuals with tendon transfer were screened for participation; 5 males qualified (Table 1). SCI participants underwent biceps transfer performed by 1 of our 2 surgeon coauthors (MB and MK) at least 1 year prior to enrollment in this study and completed the standard postsurgery rehabilitation. Pre- and postsurgery manual muscle testing and range of motion assessments were conducted using techniques described by the Medical Research Council 10 and standard occupational therapy techniques. 11 SCI participants were excluded from the study if they had concurrent severe medical illness or used a baclofen pump. Corticomotor excitability of the biceps was previously assessed in 12 arms of nonimpaired subjects aged 23 to 35 years (3 females and 9 males; mean age 26.5 ± 3.3 years). 4 All subjects were free of contraindications for TMS (including metal implants, history of seizure, etc). The protocol was approved by the Institutional Review Board of the Edward Hines, Jr. VA Hospital. All subjects provided informed written consent that included Health Information Portability and Accountability Act consent. This study is registered on www.clinicaltrials.gov under the study title Comparing Outcomes of Elbow Extension Tendon Transfers and trial registry number NCT01204736.
Participant Characteristics.
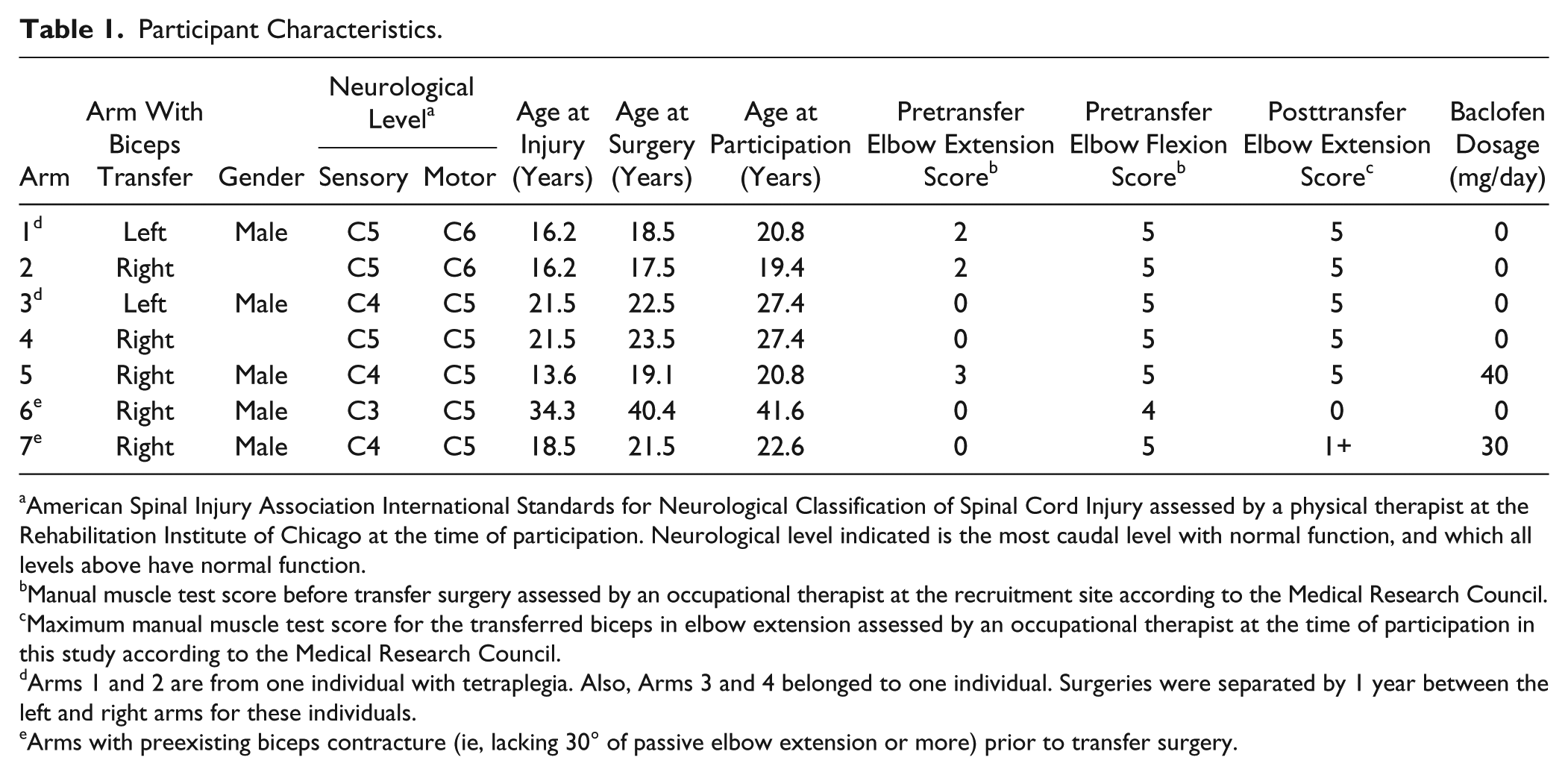
American Spinal Injury Association International Standards for Neurological Classification of Spinal Cord Injury assessed by a physical therapist at the Rehabilitation Institute of Chicago at the time of participation. Neurological level indicated is the most caudal level with normal function, and which all levels above have normal function.
Manual muscle test score before transfer surgery assessed by an occupational therapist at the recruitment site according to the Medical Research Council.
Maximum manual muscle test score for the transferred biceps in elbow extension assessed by an occupational therapist at the time of participation in this study according to the Medical Research Council.
Arms 1 and 2 are from one individual with tetraplegia. Also, Arms 3 and 4 belonged to one individual. Surgeries were separated by 1 year between the left and right arms for these individuals.
Arms with preexisting biceps contracture (ie, lacking 30° of passive elbow extension or more) prior to transfer surgery.
Transcranial Magnetic Stimulation
Single-pulse TMS was delivered to the motor cortex contralateral to the target arm using a Magstim 200 stimulator (Magstim, Dyfed, Wales, UK) via a custom batwing 90-mm figure-of-eight coil. The custom coil was used to maximize the probability of inducing MEPs in individuals with SCI as they are often small or absent.12,13 A linen cap was tied snugly on the subject’s head, with the vertex marked at the intersection of the inion-nasion and inter-aural lines. The coil was held tangentially on the scalp, at a distance about 5 cm from the vertex with the coil center rotated to induce a posterior-to-anterior cortical current across the central sulcus. The location was identified evoking the largest peak-to-peak amplitude MEP in the biceps using the lowest stimulation intensity. All subsequent stimulation was applied at this location. Resting threshold was determined in the horizontal plane with the forearm in neutral, defined as the lowest stimulus intensity that induced an MEP amplitude ≥50 µV in at least 5 of 10 consecutive stimuli. 14 The stimulus intensity for experimental trials was set at 120% of the resting threshold, except for arm 7 belonging to an individual with a high motor threshold to stimulation (Table 2) who was tested at 100% of the maximum stimulator output. During experimental trials, the stimulator was triggered to deliver 10 to 20 stimuli at a rate of 0.2 Hz.
Resting Motor Threshold and Mean Motor-Evoked Potential (MEP) Amplitudes in Transferred Biceps of Individuals with Tetraplegia and Biceps of Nonimpaired Participants, and Maximum Isometric Elbow Extensor Moment in Transferred Biceps a .
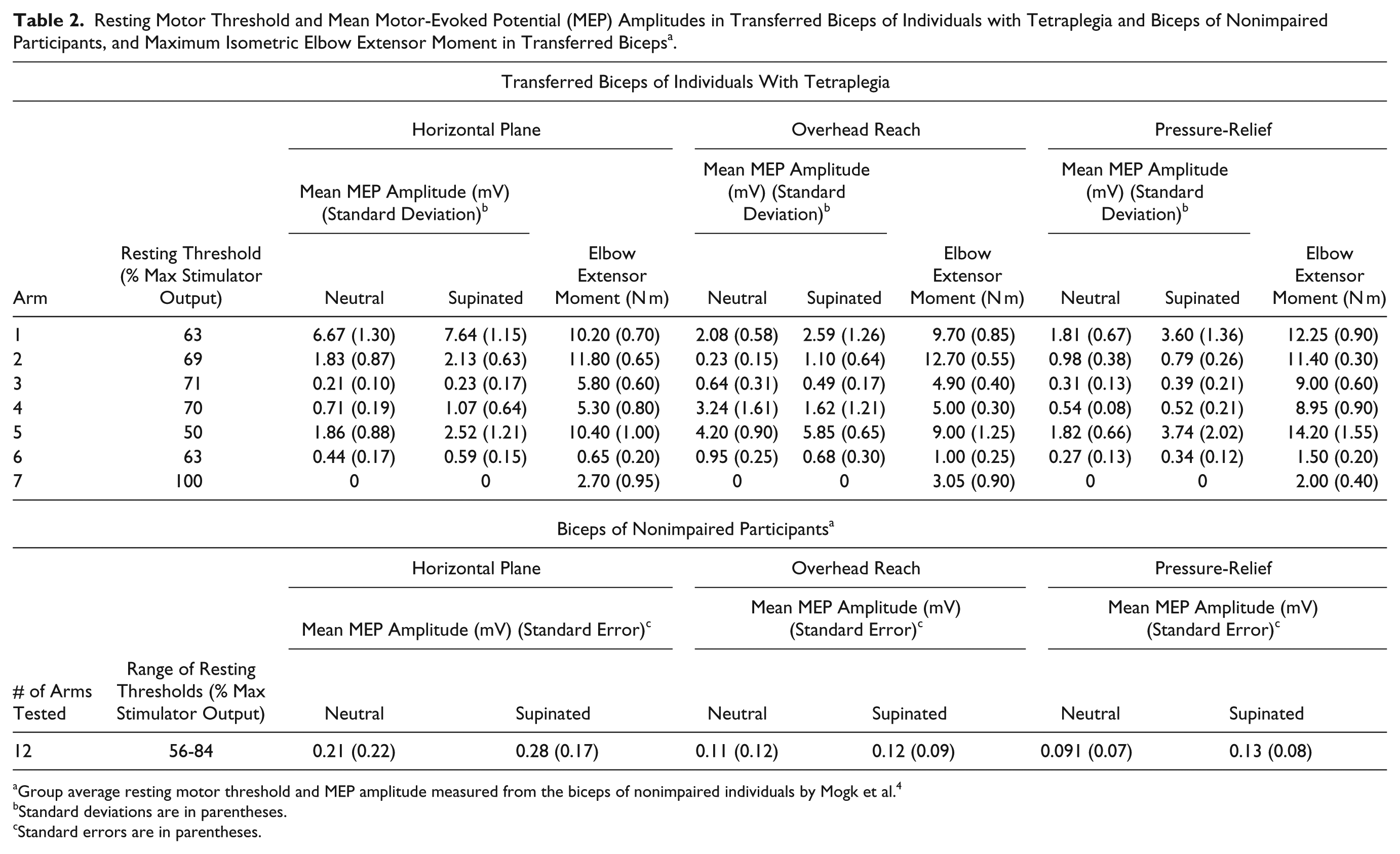
Group average resting motor threshold and MEP amplitude measured from the biceps of nonimpaired individuals by Mogk et al. 4
Standard deviations are in parentheses.
Standard errors are in parentheses.
Electromyography
Surface EMG was used to monitor muscle activity prior to each stimulus event and to record the TMS-induced responses in the biceps. The skin was lightly abraded and cleaned with alcohol. Disposable dual Ag-AgCl electrodes (Noraxon U.S.A. Inc, Scottsdale, AZ) were positioned over the belly of the biceps. The reference electrode was placed over the acromion process. EMG signals were amplified (1000×) and bandpass-filtered (10-500 Hz) using an AMT-8 amplifier (Bortec Biomedical, Calgary, Alberta, Canada), prior to analog to digital conversion (CED Micro 1401 MkII, Cambridge Electronic Design, Cambridge, UK). EMG data were sampled at 2 kHz using Spike2 software (Cambridge Electronic Design, Cambridge, UK).
Transcranial Magnetic Stimulation Protocol
Subjects were seated in their own wheelchair. The arm was supported in each of 3 static functional postures (Figure 1): overhead reach (120° arm abduction, 70° shoulder flexion, 130° elbow flexion), pressure-relief (45° abduction, 50° shoulder extension, 90° elbow flexion), and horizontal plane (90° abduction, 45° shoulder flexion, 90° elbow flexion). Joint angles followed the recommendations of the International Society of Biomechanics. 15 These postures incorporated changes in both shoulder and elbow posture, replicated postures to initiate tasks that are important for functional independence in individuals with tetraplegia, and replicated the postures in which the nonimpaired individuals were tested. 4 In each of the 3 functional postures, the forearm was rotated into 2 different static orientations (neutral and full supination) resulting in a total of 6 postures. In all postures, the forearm and hand were supported by a padded cast that could be translated and rotated relative to the elbow support to accommodate forearms of different length (Figure 1). In the horizontal plane and pressure-relief postures, the arm rested on a custom-built padded support, which was secured to a platform of adjustable height to support the weight of the arm. In overhead reach, the upper arm was supported at the level of the elbow via a contoured pad mounted on a lockable pivoting frame to adjust pad orientation, and attached to a metal stem to adjust pad height. Shoulder and elbow postures were confirmed using a manual goniometer. For each subject, TMS trials were captured in a blocked-random order by functional posture. All measures were made with the arm at rest, as confirmed using surface EMG.
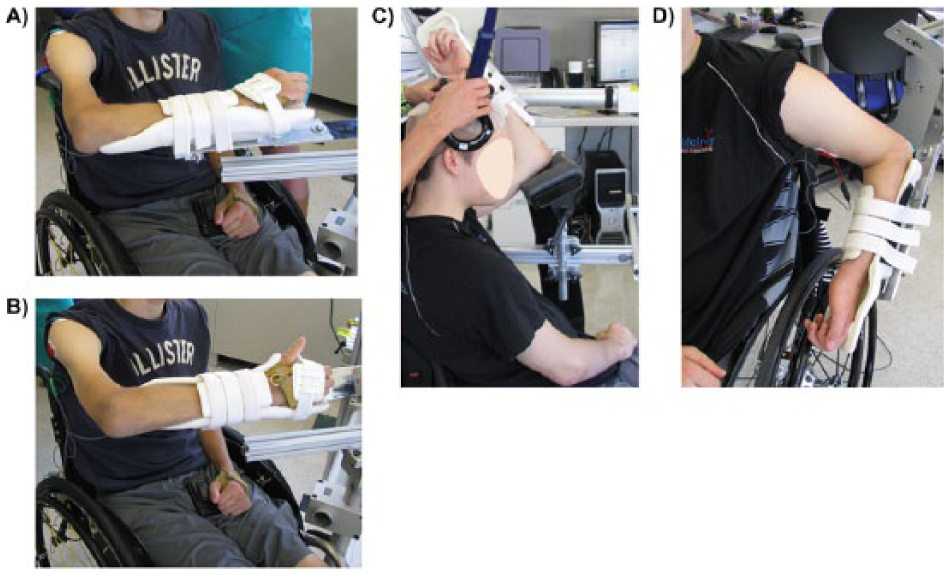
Arm postures. The arm was supported against gravity during the transcranial magnetic stimulation protocol. (A) Arm positioned in the horizontal plane with the forearm in neutral. (B) Arm positioned in the horizontal plane with the forearm supinated. (C) Overhead reach posture. (D) Pressure-relief posture.
Peripheral Nerve Stimulation
We conducted a control experiment in 3 arms with biceps transfer, who also participated in the TMS protocol, to determine how the EMG in the arm postures we tested were influenced by changes in muscle electrophysiology with muscle length. In the control experiment, we stimulated the musculocutaneous nerve and recorded the resulting compound motor action potential, or M-wave, thereby excluding the influence of the motor cortex and spinal cord. The musculocutaneous nerve was stimulated in the axillary fold with the arm at rest while EMG was recorded from the transferred biceps. Single-pulse stimulation, 200 µs in duration, was delivered using a bipolar stimulating electrode (0.47 cm2; 2.5 cm inter-electrode distance) connected to a constant current stimulator (DS7AH, Digitimer Ltd, Welwyn Garden City, UK). The minimum stimulus intensity that evoked a maximal M-wave was determined in each arm posture and 1.5 times this intensity was used for the subsequent experimental trials during which 5 M-waves were evoked every 3 to 5 seconds. Subjects were seated in their own wheelchair and the arm was fully supported in each arm posture, which were identical to those in the TMS protocol.
Maximum Isometric Voluntary Elbow Extension
Voluntary isometric moments during maximum elbow extension were measured in the arms with biceps transfer using an elbow moment transducer. 16 Three measures of the maximum isometric moment were recorded in each functional posture with the forearm oriented in neutral. Maximum effort was held for 5 seconds with 2 minutes rest between trials. Elbow moments were computed from the transducer’s output using a linear calibration equation (accuracy is 0.028 N m for moments ≤1 N m and 0.045% of moment for moments >1 N m using calibration methods described by Memberg et al 16 ). For each trial, the maximum extensor moment was computed as the greatest average moment maintained over 0.5 seconds.
Muscle Fiber Length Estimation
The muscle fiber length of the transferred biceps in each functional posture was estimated by adapting a biomechanical model of the upper extremity. 17 The biceps transfer was modeled by altering the musculotendon path of the biceps based on illustrations and descriptions of the surgical procedure.1,2 The long and short heads of the biceps were routed medially around the humerus and merged with the insertion path of the triceps. We assumed that (1) the moment arm of the transferred biceps equaled that of the triceps and (2) the moment arm of the transferred biceps in elbow extension does not change with forearm orientation. Each posture was replicated using the model to estimate muscle fiber length.
Data and Statistical Analysis
We calculated the root mean square (RMS) amplitude of the evoked response, the RMS amplitude of the prestimulus background EMG (over a duration matched to the duration of the corresponding evoked response), and the peak-to-peak amplitude of the evoked response (MEP or M-wave) using purpose-written Matlab code (The MathWorks, Inc, Natick, MA). Stimulus events where the prestimulus RMS amplitude was larger than the evoked response, or where voluntary activity was detected, were discarded to ensure similar levels of background activity across postures. MEP and M-wave amplitudes recorded in each of the 6 test postures were normalized by responses in the horizontal plane with the forearm in neutral.
We compared the mean of normalized MEP amplitudes measured from the biceps in arms with biceps transfer and nonimpaired arms to test our hypothesis that posture-dependent corticomotor excitability of the transferred biceps would differ relative to the nonimpaired biceps. To account for the repeated measure nature of our experiment, a random intercept only, linear mixed-effect model was used to compare mean normalized MEP amplitudes due to population (biceps transfer and nonimpaired), functional posture, and forearm orientation. The analysis included individual MEP amplitudes in each posture, as opposed to an average response in each posture for each arm. Population, main posture, and forearm orientation were treated as fixed factors and arm was treated as a random factor. The inverse of population variances was weighted in the model to account for unequal variances between the biceps transfer and nonimpaired groups. Post hoc comparisons were performed when the main effects were significant (P < .05). A separate 2-way analysis of variance was performed to confirm that the mean RMS amplitude of prestimulus EMG did not differ between population and postures. There was considerable variability in MEP amplitude between arms within the same individual with tetraplegia. Thus, we treated these arms independently. For example, in Arm 1 MEP amplitude ranged from 1.81 to 7.64 mV across postures. In Arm 2, belonging to the same individual as Arm 1, MEP amplitude ranged from 0.23 to 2.13 mV. Other previous studies have also treated arms with tendon transfer in individuals with tetraplegia as independent data points due to as much or more variability between limbs within a single patient as between patients.18,19 Furthermore, spinal cord injuries usually do not affect both limbs symmetrically.
We tested for a correlation (Pearson’s) between mean MEP amplitude and isometric moments across individual arms and postures to determine whether corticomotor excitability of the transferred biceps is related to maximum isometric elbow extension strength. We also tested for a correlation (Pearson’s) between normalized MEP amplitude and normalized elbow moment (normalized to the mean value in the horizontal plane, neutral forearm posture). Furthermore, we tested for Pearson correlations between normalized and unnormalized MEP amplitude with relative muscle fiber length (length normalized to the horizontal plane posture).
Results
Demographic and clinical characteristics of participants with biceps transfer are summarized in Table 1. The mean (±SD) age of the nonimpaired control participants (3 females, 9 males) was 26.5 ± 3.3 years. 4 MEP amplitude, resting threshold, and maximum isometric moment in elbow extension varied across subjects with biceps transfer, and also between arms within subjects with biceps transfer. MEP amplitude ranged from 0 to 7.64 mV and resting threshold ranged from 50% to 100% of maximum stimulator output across arms with biceps transfer (Table 2). Maximum isometric moment in elbow extension ranged from 0.65 to 14.20 N m (Table 2).
Effect of Population and Arm Posture on Normalized MEP Amplitude
Mean MEP amplitude differed due to population (biceps transfer vs nonimpaired biceps), functional posture, and forearm orientation. The main effects of population (F1,16 = 5.2, P = .04) functional posture (F2,1065 = 375.8, P < .001), and forearm orientation (F2,1065 = 208.0, P < .001) were significant in the linear mixed-effect model of corticomotor excitability. The interaction effects of functional posture and population (F2,1065 = 45.6, P < .001) and functional posture and forearm orientation (F2,1065 = 67.5, P < .001) were significant. Post hoc comparisons demonstrated that normalized MEP amplitude was greater in arms with biceps transfer relative to nonimpaired biceps in overhead reach with the forearm in neutral (t1078 = −6.0, P < .001) and supinated (t1078 = −4.2, P < .001; Figure 2). Within the biceps transfer group, normalized MEP amplitude was greater with the forearm supinated relative to in neutral in the horizontal plane posture (t1078 = −2.3, P = .02; Figure 2). Within the nonimpaired group, normalized MEP amplitude was greater with the forearm supinated relative to neutral in the horizontal plane (t1078 = −17.7, P < .001), overhead reach (t1078 = −3.2, P = .002), and pressure-relief postures (t1078 = −4.1, P < .001; Figure 2).
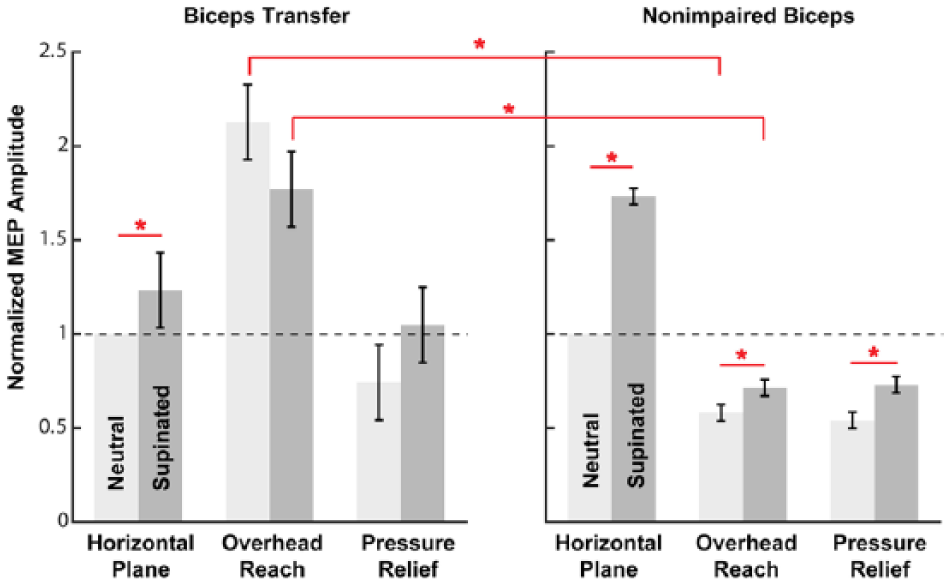
Posture-dependent differences in mean normalized motor-evoked potential (MEP) amplitude in transferred and nonimpaired biceps. Mean normalized MEP amplitude (normalized to MEPs in horizontal plane, neutral posture) was greater in the arms with biceps transfer relative to the nonimpaired biceps in the overhead reach posture in both forearm orientations. In the biceps transfer group, normalized MEP amplitude was greater with the forearm supinated relative to neutral in the horizontal plane posture. In the group of nonimpaired biceps, normalized MEP amplitude was greater with the forearm supinated relative to neutral in each posture. Error bars are ±1 standard error of the means. Significant differences (P < .05) are indicated by *.
Relationships Between MEP Amplitude and Elbow Extension Strength and Muscle Length
Individual mean MEP amplitude was positively correlated with maximum voluntary moment generated during isometric elbow extension across transferred arms and functional postures (r = .48, P = .029; Figure3A). When MEP amplitude and elbow moment were normalized to the horizontal plane, neutral posture within individual arms, normalized MEP amplitude and normalized elbow moment were not related (P = .62; Figure 3B). Neither individual mean MEP amplitude (P = .32; Figure 4A) nor normalized mean MEP amplitude (P = .12; Figure 4B) were correlated with relative muscle fiber lengths.
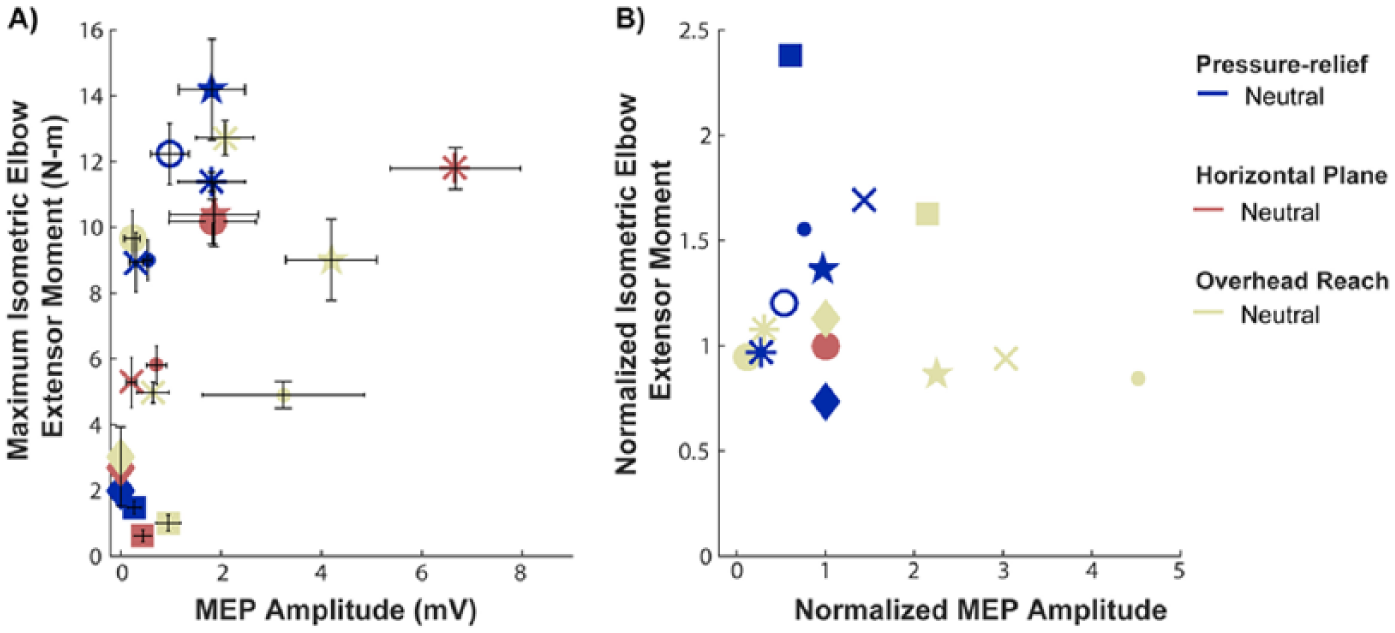
Motor evoked potential (MEP) amplitudes and elbow extensor moments in arms with biceps transfer. A) Unnormalized motor evoked potential (MEP) amplitudes were positively correlated with maximum voluntary moments in isometric elbow extension across arms with biceps transfer and postures (r = .48, p = .029). Each symbol corresponds to one arm. Error bars are ± one standard deviation. B) Within individual arms with biceps transfer, there was no relationship between the normalized MEP amplitudes and the normalized elbow extensor moments (p = 0.62). MEPs and elbow moments were normalized to the horizontal plane, neutral posture for each arm.
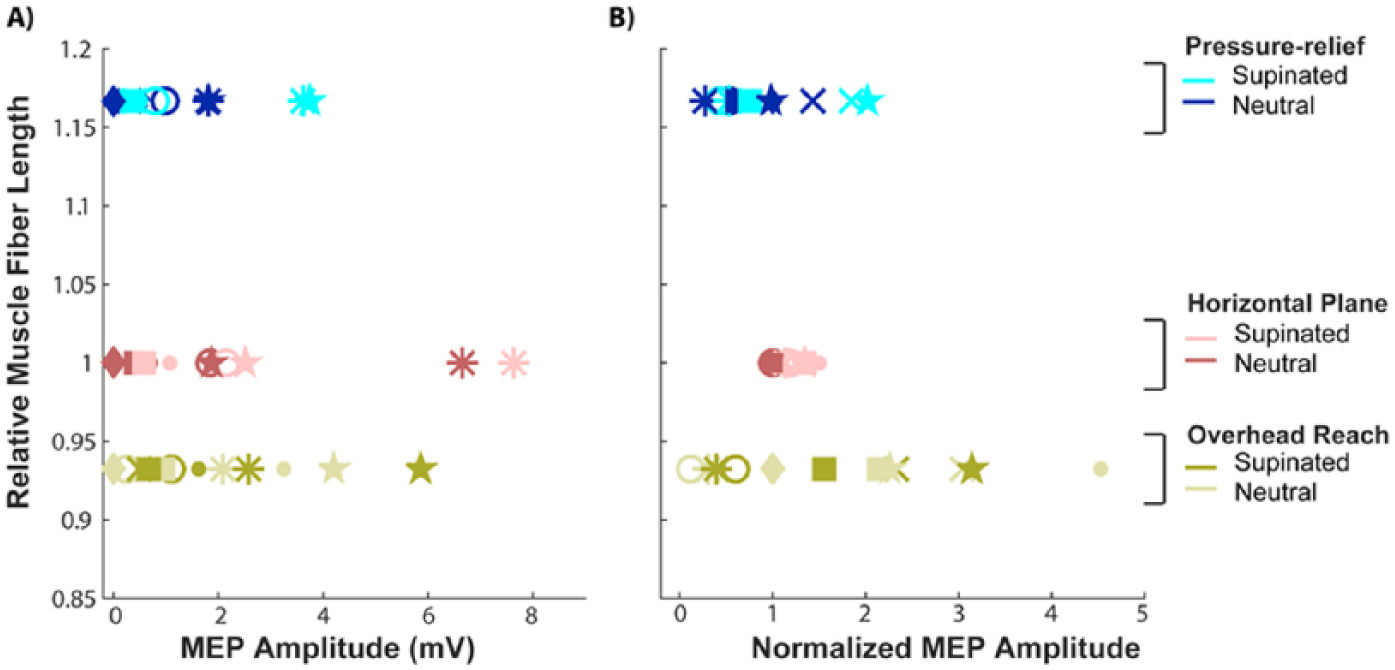
Motor evoked potential (MEP) amplitudes and relative muscle fiber lengths in arms with biceps transfer. A) Unnormalized motor evoked potential (MEP) amplitudes were not correlated with relative muscle fiber length across arms with biceps transfer and postures. Error bars are ± one standard deviation. B) Within individual arms with biceps transfer, there was also no relationship between the normalized MEP amplitudes and relative muscle fiber lengths. MEPs and fiber lengths were normalized to the horizontal plane, neutral posture.
M-Wave Amplitude Across Arm Postures
Changes in M-wave amplitude with arm posture were small relative to the changes in MEP amplitude in the 3 arms with biceps transfer that we assessed (Arms 2, 3, and 4 in Table 1; see Figure 5). The normalized difference in mean MEP amplitude between the most and least excitable posture (overhead, neutral and pressure relief, neutral, respectively) was 2.30 for the 3 arms in which M-waves were measured (Figure 5A). The mean difference in normalized M-wave amplitude between these same postures was 0.10 (Figure 5B). The largest difference in normalized M-wave amplitude across postures was 0.26, which was between the horizontal plane, supinated and pressure-relief, neutral postures (Figure 5B).
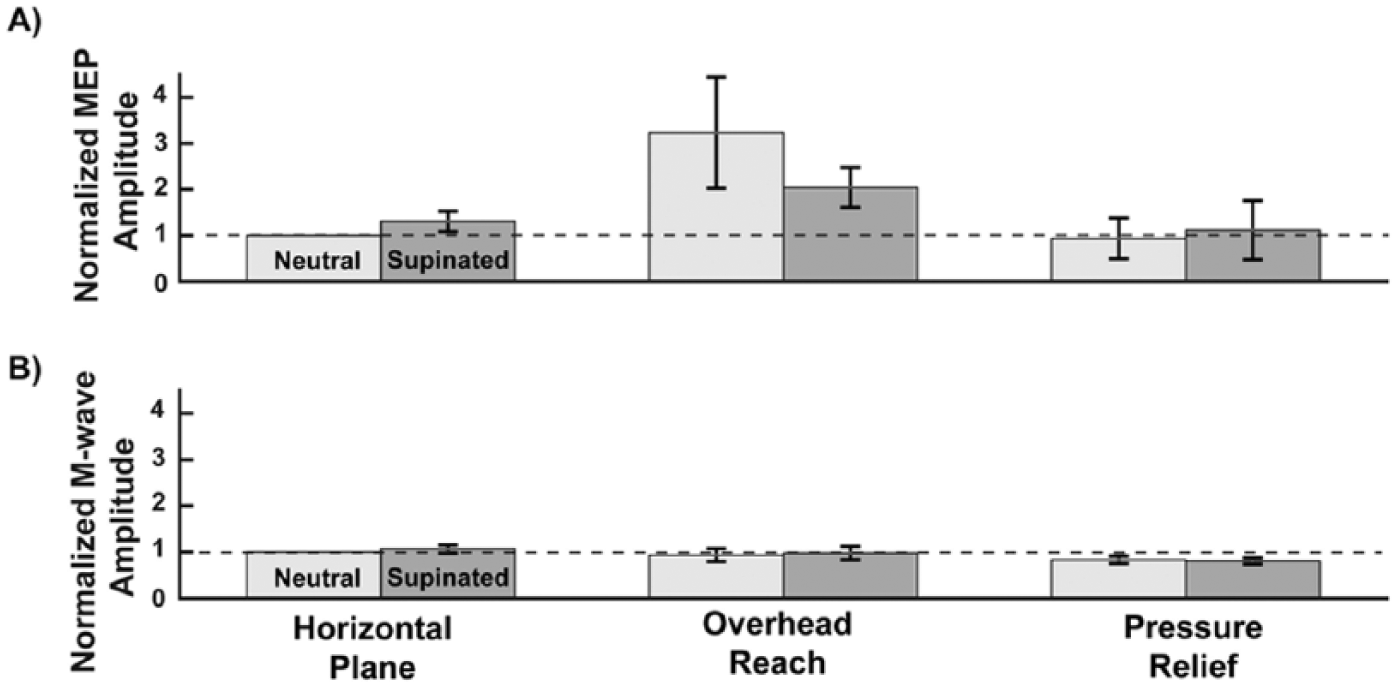
Normalized motor-evoked potential (MEP) amplitude and M-wave amplitude. Differences in normalized MEP amplitude across postures (A) were larger relative to differences in mean M-wave amplitude (B) across postures in the 3 arms with biceps transfer in which M-waves were recorded. Error bars are ±1 standard error of the means. As in Figure 2, lighter gray bars indicate a neutral forearm, darker gray bars indicate a supinated forearm.
Discussion
We investigated the effects of multi-joint upper limb posture on the excitability of surgically transferred biceps at rest in individuals with tetraplegia. Posture-dependent changes in TMS-evoked responses were taken as evidence of posture-related modulation of overall corticomotor excitability. We hypothesized that posture-dependent corticomotor excitability of the transferred biceps would differ relative to the nonimpaired biceps. 4 Our hypothesis was supported; MEP amplitude was greater in the transferred biceps relative to the nonimpaired biceps in overhead reach regardless of forearm orientation. Thus, motor re-education of the transferred biceps may be facilitated in an overhead reach posture should a facilitated pathway make the transferred muscle easier to activate. Our expectation that a facilitated pathway may make a muscle easier to activate is based on facilitated pathways affecting the EMG-force gain 5 and decreasing sense of effort during contractions of nonimpaired muscle. 3 Although on average the overhead reach posture was most excitable in the arms with biceps transfer we tested, not all of the transferred arms were most excitable in the overhead reach posture (Table 2). Therefore, motor re-education of the transferred biceps may be most beneficial when tailored to the most excitable posture for each individual. We also investigated the relationship between corticomotor excitability and maximum strength of the transferred biceps muscle. Arms with greater overall corticomotor excitability could generate greater maximum moments during isometric elbow extension. Thus, rehabilitative strategies to increase corticomotor excitability (eg, repetitive TMS, 20 EMG biofeedback, 21 anodal transcranial direct stimulation 22 ) may be beneficial for elbow extension strength.
The difference in posture-dependent excitability between the transferred biceps in individuals with tetraplegia and the biceps of nonimpaired individuals may arise from differences in behavioral demands between the groups. Wheelchair-bound individuals perform many activities of daily living with overhead motions because of the necessity for a seated position. Thus, individuals with biceps transfer who participated in this study may be relatively more skilled in activities that involve extending their elbow in an overhead posture compared to nonimpaired individuals. In support of this possible effect of behavioral demands, other studies that have investigated populations with unique upper limb training have found increased MEP amplitude (eg, hand muscles of racket players 23 ), increased cortical map area of motor representation (eg, hand muscles of pianists 24 and blind braille readers, 25 and shoulder muscles of volleyball players 26 ), or decreased MEP threshold (eg, pianists 24 ).
The effect of forearm orientation on corticomotor excitability in the arms with biceps transfer adds to the existing evidence that the mechanical function of a muscle does not determine posture-dependent excitability. Corticomotor excitability of transferred biceps, nonimpaired triceps, 6 and nonimpaired posterior deltoid 4 are more excitable with the forearm supinated in particular elbow and shoulder orientations, although none of these muscles mechanically influence forearm orientation. Differences in spatial orientation of the transferred biceps relative to the EMG electrodes cannot account for the effect of forearm orientation on excitability because we measured a consistent M-wave amplitude with the forearm in neutral and fully supinated. Thus, our data support previous work demonstrating that corticomotor excitability of a muscle can be influenced by the orientation of a joint that the muscle does not span.4,6,27
Corticomotor excitability of the transferred biceps was not related to estimated muscle fiber length based on a musculoskeletal model, which agrees with previous work demonstrating strong central modulation of corticomotor excitability with changes in posture, as opposed to peripheral modulation.4,28 There is evidence for central modulation of posture-dependent corticomotor excitability involving afferent contributions at cortical, 28 spinal, 29 and motor neuron levels. 30 In the current study, we assessed the overall excitability of the corticomotor pathway, which reflects a balance between excitatory and inhibitory processes at all levels. Further studies are needed to determine relative contributions of cortical and subcortical level excitatory and inhibitory processes to posture-dependent corticomotor excitability.
The positive relationship between corticomotor excitability and maximum isometric elbow extensor moment suggests that corticomotor excitability may contribute to strength outcomes after tendon transfer. We observed large differences in MEP amplitude between the weakest (Arms 6 and 7; Table 2) and strongest arms (Arms 1, 2, 4, and 5; Table 2) with biceps transfer. For the 2 transferred arms in which maximum elbow extensor moments were weakest, biceps excitability may have been low prior to transfer. Clinical assessments before transfer surgery indicate elbow function was more impaired in these 2 arms in which biceps transfer MEP amplitude was small or absent (Arms 6 and 7; Tables 1 and 2) relative to the other arms with biceps transfer that we tested. The 2 transferred arms with the smallest MEP amplitudes had limited passive range of motion in elbow extension (ie, elbow flexion contracture) and no active elbow extension prior to transfer surgery (triceps manual muscle test grade = 0; see Table 1). Inadequate motor re-education to activate the transferred biceps after surgery resulting in detrimental neuroplasticity may have also contributed to the small or absent MEP amplitudes recorded in Arms 6 and 7. Evidence that the transfer surgery itself did not decrease corticomotor excitability of the transferred biceps comes from increased corticomotor excitability (increased MEP amplitude and decreased resting motor threshold) after free functioning muscle transfer of the gracilis muscle (a thigh adductor) to replace a damaged upper limb muscle. 31 Although the gracilis transplantation procedure differs from the biceps transfer, Chen et al demonstrated functional plasticity of the motor system projecting to a transferred muscle. Future work should assess corticomotor excitability of the biceps prior to transfer surgery and throughout the rehabilitative period, to better understand relationships between corticomotor excitability and elbow extension strength.
Four out of 5 of the strongest arms with biceps transfer were hyperexcitable, suggesting reorganization of the motor system to facilitate activation of the transferred biceps. Mean MEP amplitude across postures in each of these 4 arms (Arms 1, 2, 4, and 5; Table 2) exceeded the mean MEP amplitude measured in the nonimpaired arms (Table 2). MEP amplitude was assessed at stimulus intensities 120% of resting motor threshold in the individuals with tetraplegia and the nonimpaired individuals. 4 The hyperexcitability of the transferred biceps is consistent with previous work demonstrating reorganization to favor activation of muscles with residual function after SCI.32-35 Most directly, Edwards et al found that the nontransferred biceps was hyperexcitable in an individual with SCI with preserved biceps function. 35 Further research is needed to determine the location and nature of reorganization of the motor system projecting to the biceps after SCI, and after transfer surgery.
The lack of relationship between normalized MEP amplitude and normalized elbow moment within individual arms across postures suggests that maximum strength is primarily determined by other posture-dependent biomechanical factors (ie, moment arms, muscle force-length relationship), or that posture-dependent excitability changes during voluntary activation relative to rest. We assessed corticomotor excitability with the muscle relaxed as a baseline measure of posture-dependent excitability after biceps transfer. Future studies to investigate relationships between corticomotor excitability and posture during voluntary activation are needed.
Conclusions
Corticomotor excitability of the transferred biceps at rest depends on arm posture in individuals with tetraplegia. Posture-dependent excitability of the transferred biceps differed relative to the biceps of nonimpaired individuals. Corticomotor excitability was positively related to elbow extension strength across the individuals with tetraplegia and biceps transfer. Modulating arm posture to increase corticomotor excitability may contribute to improve strength outcomes after tendon transfer and may be beneficial for promoting motor re-education during the rehabilitative period.
Footnotes
Acknowledgements
We thank Vikram Darbhe and Heidi Roth at the Rehabilitation Institute of Chicago for their assistance with the data collection.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Merit Review Award #I01 RX000377 (formerly B7515R) from the United States (U.S.) Department of Veterans Affairs Rehabilitation Research and Development Service. The contents do not represent the views of the U.S. Department of Veterans Affairs or the United States Government.