
Abstract
Background. In many children with unilateral spastic cerebral palsy (USCP), the corticospinal tract to the affected hand atypically originates in the hemisphere ipsilateral to the affected hand. Such ipsilateral connectivity is on average a predictor of poor hand function. However, there is high variability in hand function in these children, which might be explained by the complexity of motor representations of both hands in the contralesional hemisphere. Objective. To measure the link between hand function and the size and excitability of motor representations of both hands, and their overlap, in the contralesional hemisphere of children with USCP. Methods. We used single-pulse transcranial magnetic stimulation to measure the size and excitability of motor representations of both hands, and their overlap, in the contralesional hemisphere of 50 children with USCP. We correlated these measures with manual dexterity of the affected hand, bimanual performance, and mirror movement strength. Results. The main and novel findings were (1) the large overlap in contralesional motor representations of the 2 hands and (2) the moderate positive associations of the size and excitability of such shared-site representations with hand function. Such functional associations were not present for overall size and excitability of representations of the affected hand. Conclusions. Greater relative overlap of the affected hand representation with the less-affected hand representation within the contralesional hemisphere was associated with better hand function. This association suggests that overlapping representations might be adaptively “yoked,” such that cortical control of the child’s less-affected hand supports that of the affected hand.
Introduction
Unilateral spastic cerebral palsy (USCP) is typically characterized by motor skill impairments on the side of the body contralateral to the lesion. However, the range of severity in impairment is large. Many factors potentially contribute to impaired hand function in children with USCP. The type of corticospinal tract (CST) pattern and the timing, location, and size of brain lesions predict upper-limb function in USCP (see reviews1,2). In many children with USCP, the CST to the affected hand does not originate in the hemisphere contralateral to the affected hand, as it does in typically developing children. Very early in development, the CST of each hemisphere projects bilaterally to the spinal cord. 3 In typical development, ipsilateral (same-sided) CST projections are pruned, whereas contralateral CST projections are strengthened. 4 In USCP, a loss of activity from the lesioned hemisphere has been shown to contribute to a loss of the CST from the lesioned hemisphere and maintained CST projections to each hand from the contralesional hemisphere.5,6 The presence of same-sided (ipsilateral) CST connections to the affected hand is associated with poorer hand function than preserved crossed CST connections to the affected hand.2,7-10 However, even among children with this ipsilateral CST pattern, there is high variability in hand function. 9 The source of this variability remains unknown.
Motor map organization might explain some variability in hand function in children with USCP. Changes in the areal size and total excitability of motor representations of an affected limb following injury and intervention have been landmarked in a range of contexts (eg, animal models,11-14 adult stroke, 15 amputation, 16 and spinal cord injury 17 ) and in healthy adults (eg, Sanes et al 12 ). Although our group found an association between changes in map size and improved hand function after intensive bimanual training in children with USCP, we found no correlation between excitability of motor representations and hand function. 18 Also in USCP, but not in the context of therapeutic intervention, Kesar et al 19 found no link between motor function and the excitability of motor representations. Because sample sizes in both studies were small (n = 10 participants 18 , n = 7 participants 19 ), associations might be identified in a larger study.
Healthy animal models and those of cerebral palsy have suggested that the relative overlap of primary motor cortex (M1) motor representations, or so-called dual-response representations, is more predictive of hand skill than the absolute size and excitability of such representations. A study with healthy squirrel monkeys showed that an increase in dual-response representations of movement combinations were more frequently used following digit skill training. 20 The authors suggested that the temporal correlation of movements drove changes in cortical motor reorganization. Similarly, increases in dual-response representations have been shown following activity-dependent use in cats. 21 In contrast, damage to M1 (by means of muscimol inactivation) has been shown to dramatically decrease dual-response representations. 22 Thus, dual-response representations in the context of damage to a primary motor structure and in the context of motor-skill intervention suggest at least some functional importance in their relative existence, at least with regard to contralateral representations of multiple joints within a given limb. In USCP, representations of both hands are often predominantly found in the contralesional hemisphere. Similar to the convergence of within-limb representations, convergence of between-limb representations in USCP might be related to function. Whether such representations are overlapping, and at all related to function, is currently unknown. It is conceivable that such representations overlap to some extent such that the cortical control of the unaffected hand can assist or be adaptively yoked to the advantage of the affected hand. On the other hand, unlike the convergence of within-limb representations, the convergence of between-limb representations might be negatively related to function, as that which has been shown in focal hand dystonia. 23
We investigated the relationship between hand function and the size and excitability of contralesional motor representations of the affected hand, and the overlap of these representations with that of the less-affected hand, using single-pulse transcranial magnetic stimulation (TMS). We focused on children with contralesional (ie, ipsilateral) CST connections to the affected hand because (1) most children with USCP have such CST patterns (either predominantly, called an ipsilateral CST pattern, or combined with contralateral connections, called a bilateral CST pattern)9,24; (2) the source of variability in hand function in children with contralesional CST patterns is unknown; and (3) overlap in motor representations of the 2 hands can only be studied in children whose maps are both located in 1 hemisphere. We hypothesized that hand function would be positively associated with overall size and excitability of affected hand motor representations and their overlap with less-affected hand representations.
Methods
Participants
A total of 50 children with USCP participated. Table 1 shows demographics and clinical scores for children included in the final analyses. Some functional and motor mapping data have been used: n = 23 and n = 17 of this study’s participants were included in Smorenburg et al 10 and Friel et al, 18 respectively. Preintervention unimanual and bimanual measures for these participants are in Smorenburg et al 10 and Friel et al. 18 The measure of total map size for these participants is used in their comparison with postintervention scores in Friel et al. 18 However, neither publication addressed the hypotheses presented here.10,18
Demographic and Clinical Characteristics of Participants, Stratified by CST Pattern.
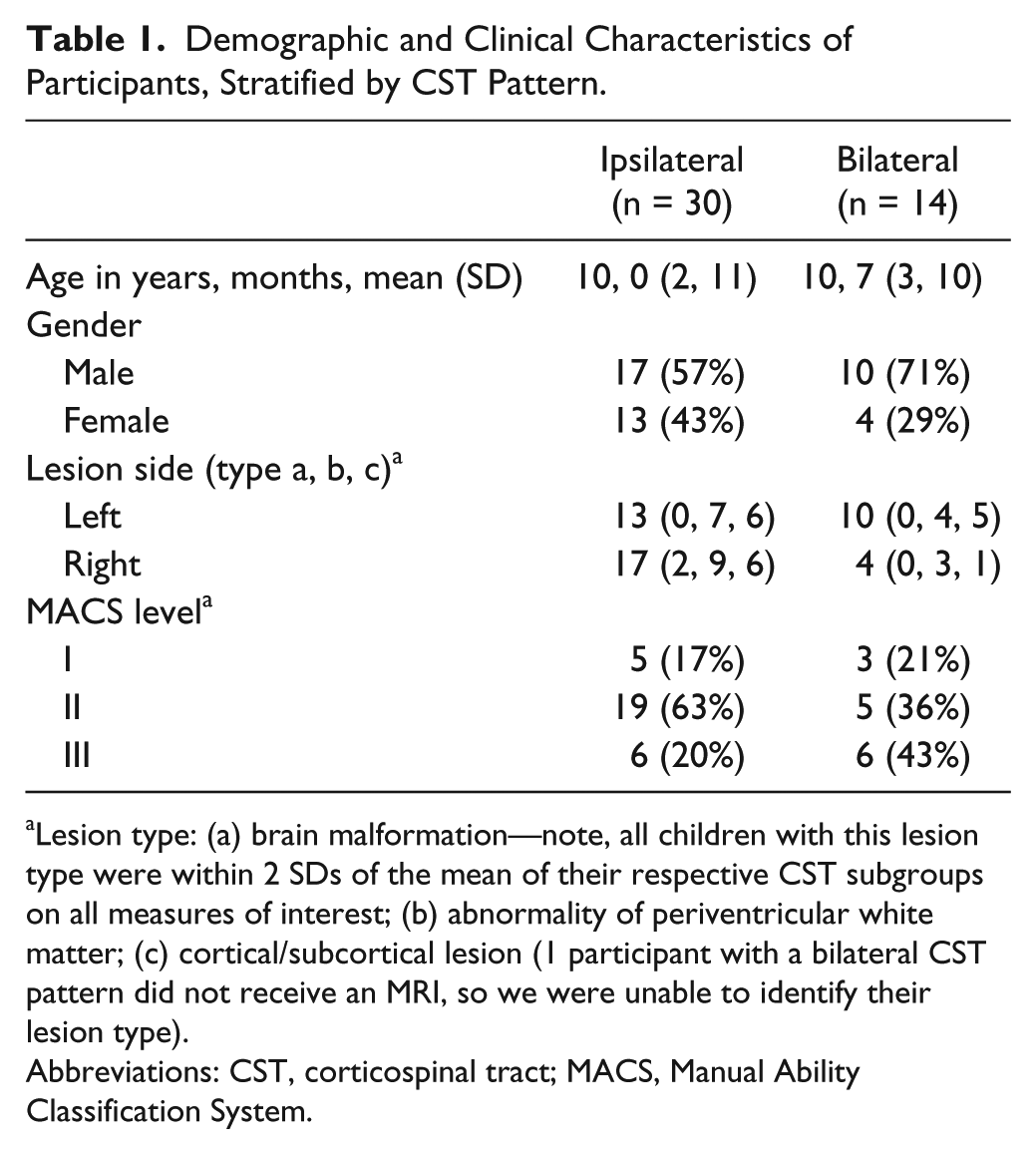
Lesion type: (a) brain malformation—note, all children with this lesion type were within 2 SDs of the mean of their respective CST subgroups on all measures of interest; (b) abnormality of periventricular white matter; (c) cortical/subcortical lesion (1 participant with a bilateral CST pattern did not receive an MRI, so we were unable to identify their lesion type).
Abbreviations: CST, corticospinal tract; MACS, Manual Ability Classification System.
Participants were recruited from clinics, online communities, ClinicalTrials.gov (NCT00305006), and our website (http://www.tc.edu/centers/cit/) as part of a larger intervention study; data presented here were preintervention measures. Inclusion criteria were (1) congenital USCP, (2) ability to lift arms 15 cm above a surface and grasp light objects, (3) mainstreamed in school (n = 2 received special education services), and (4) ability to follow instructions. Exclusion criteria were (1) medical illness that would interfere with participation, (2) seizure history after age 2 years or use of antiseizure medications, (3) uncorrected visual problems, (4) severe spasticity (Ashworth ≥ 3), (5) affected-hand surgery in past year, (6) botulinum toxin in upper extremity in past 6 months, and (7) nonremovable metal in body. All study procedures were approved by Institutional Review Boards where the testing was conducted (Teachers College, Columbia University, Burke Rehabilitation Hospital, Université Catholique de Louvain, and New York State Psychiatric Institute and Weill Cornell Medical College). Participants gave written informed assent, and parents gave written informed consent.
Materials and Procedures
Hand Function
We measured manual dexterity, bimanual performance, and the strength of mirror movements (involuntary movement of the less-affected hand during voluntary movement of the affected hand). Manual dexterity of the affected hand was measured using the Jebsen-Taylor Test of Hand Function 25 (JTTHF). The JTTHF measures the duration (in seconds) of one hand to perform functional movements. The total time of 6 subtests was used (flipping cards, manipulating small objects, simulated eating, checker stacking, and manipulating empty and full cans). The maximum time to perform each subtest was 180 s. A higher score indicates poorer dexterity. Bimanual performance was measured using the Assisting Hand Assessment (AHA),26,27 which quantifies the quality with which the child uses the affected hand as an assisting hand during bimanual play-based activities. The AHA has excellent validity and reliability,26,27 with a higher score (AHA units) indicating better bimanual performance.
Mirror movements were measured using electromyographic (EMG) signals recorded from the first dorsal interosseous (FDI) muscles bilaterally using surface bipolar electrodes (Coviden, Mansfield, MA) in a belly-tendon configuration with a ground electrode on the wrist styloid process. The EMG signal was sampled (4000 Hz), amplified (gain 600 V/V), bandpass filtered (10-400 Hz), and notch filtered (55-60 Hz) to minimize movement artifacts. With both forearms and hands relaxed and supported comfortably on cushions, participants were visually cued to pinch with the thumb and index finger of one hand only. Pinches were held for 5 s, followed by a 5-s rest period. EMG activity was monitored in real time to ensure instructions were followed appropriately. A total of 10 trials were completed using the less-affected hand, then the affected hand. We are currently investigating the relationship between EMG- and clinically derived measures of mirror movements 28 in a larger, separate study. At this time, we only have clinical ratings of mirror movements in a small subset of children included in this study (n = 14 out of 30 in the ipsilateral CST group, and n = 7 out of 14). In this small subset for which we have clinical data, correlations between clinically derived and EMG-derived mirror movements are moderate and positive, but not significant; we suspect the associations to become significant with more data points. We decided to use the EMG-derived measures of mirror movements over the clinical-derived measures because (1) we have double the amount of data for the former compared with the latter and (2) the former is a more objective measure of the two and is not subject to rater reliability.
Motor Mapping
We used single-pulse TMS to map the motor representation of the relaxed FDI muscle in each hand, using the same EMG protocol described above.
Single pulses were delivered by a Magstim 2002 (Magstim Co, Whitland, Dyfed, UK) through a figure-of-eight coil with a 7-cm diameter. The coil handle was oriented at 45° to the midsagittal line to induce a current in a posterior to anterior direction, approximately perpendicular to the central sulcus. Before TMS testing, we acquired a T1-weighted image using a 3T MRI scanner (except for 4 participants who, with their caregivers, did not consent to receiving an MRI). Using Brainsight frameless stereotaxy (Rogue Research, Montréal, Canada), the TMS coil location was recorded and superimposed onto the child’s T1-weighted image. For those without an MRI, the TMS coil location was recorded and superimposed onto a single-subject “model” MRI. Our measures were concerned with the size, excitability, and overlap of motor representations, none of which are affected by the absolute relation to an anatomical image.
We first searched for the region at which TMS produced the largest motor evoked potential (MEP) in the affected FDI (the motor “hotspot”). Single pulses were delivered to the lesioned hemisphere (interstimulus interval: 8-10 s). If no MEP responses for the affected FDI were found in the lesioned hemisphere, single pulses were delivered to the contralesional hemisphere.
After the hotspot was found, the resting motor threshold (rMT) of the affected FDI was measured by delivering pulses over the hotspot and adjusting the stimulator output in 2% increments until an MEP with an amplitude of >50 µV and response latency <40 ms was elicited by 6 of 10 pulses at a given stimulator output. Note that the hotspot of the affected and less-affected FDIs were in most cases in different locations (in 34 of 44 participants). Responses were excluded if baseline EMG activity was >50 µV. The mean rMT of the affected FDI was 63% (SD = 13) of maximum stimulator output, and the mean rMT of the less-affected FDI was 61% (SD = 11), with no significant difference [t(32) = 2.03; P > .05] between these in the 33 children for whom we have both values (missing data are a result of time and cooperativity issues, and not collecting both measures in the first few children we tested).
We next derived a complete motor map of the affected FDI. In Brainsight (Rogue Research, Montréal, Canada), a circular grid of 81 sites, spaced 1 cm apart in 5 concentric rings, centered around the hotspot, was superimposed onto the child’s cortical model. The mapping procedure was ceased once a responsive site was surrounded with 1-cm border of sites that did not elicit MEPs. Single pulses were delivered at 110% rMT of the affected FDI at each grid site, starting over the hotspot and moving concentrically along each ring. Three to 6 pulses were delivered at sites that elicited an MEP (to capture 3 clear trials without noise contamination—ie, EMG activity before TMS onset). One to 2 pulses were delivered at sites that did not elicit an MEP: if the nonresponsive site neighbored a responsive site, 2 pulses were delivered.
Data Analyses
Mirror Movement Quantification (n = 41)
The EMG data for the cued hand were epoched (4-5 s), with movement onset and offset identified manually. Mirror movement epochs were obtained from corresponding epochs of the other hand. Trials were excluded if EMG remained <1 mV for at least 4 s after cue onset (mean number of included trials per child n = 7.8 ± 2.1). The epoched data were rectified, and the root mean square (RMS) was estimated. The relative mirror movement strength was calculated as the mean ratio of mirror to voluntary RMS.
Classification of CST Pattern
Participants were classified as having an ipsilateral CST pattern when 100% of MEPs recorded in the affected FDI resulted from stimulation of the contralesional hemisphere. Participants were classified as having a bilateral CST pattern when MEPs in the affected FDI resulted from stimulation of both hemispheres. Participants were classified as having a contralateral CST pattern when 100% of MEPs in the affected FDI resulted from stimulation of the lesioned hemisphere.
Motor Representation Quantification
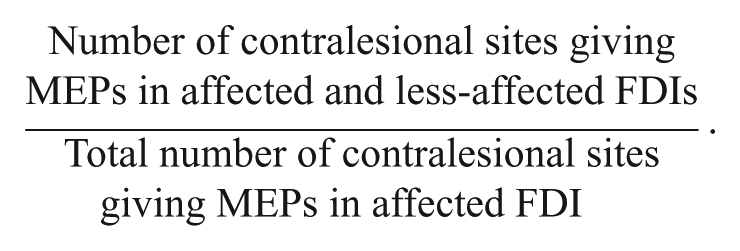
We characterized the areal size and excitability of the contralesional motor representation of the affected FDI. Size (reflective of the spread of the FDI representation) was quantified as per previous motor mapping work in USCP 18 as the number of grid sites at which stimulation evoked an MEP. To quantify excitability (reflective of the strength of the FDI representation), we first calculated the mean peak-to-peak amplitude of MEPs of the affected FDI at each site. We normalized the mean MEP amplitude at each site by dividing it by the largest mean MEP amplitude recorded in the map. The excitability of the affected FDI motor representation was quantified as the total sum of normalized MEP amplitudes; we quantified map excitability in this way to match the quantification of map excitability used in the Kesar et al study. 19 Finally, we rationalized our measures of overlap as the number of sites (and their excitability) that gave dual responses in both hands (as that which has been done in previous animal work). We calculated the proportion of stimulated sites that elicited an MEP in the affected FDI, which also elicited an MEP in the less-affected FDI:
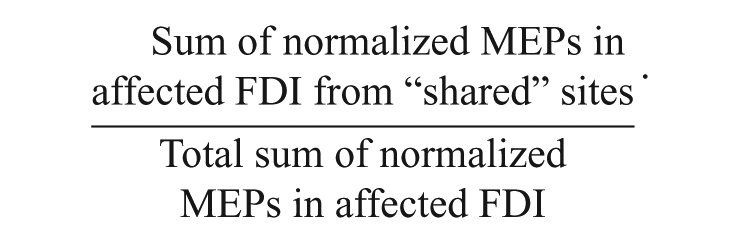
We quantified the relative excitability of these shared sites as the sum of normalized MEPs of these shared sites recorded in the affected FDI relative to the total sum of normalized MEPs recorded in the affected FDI:
Results
Statistical Analyses
More than half of the data were not normally distributed (4 of our 7 measures did not meet the normality assumption, as tested by the Shapiro-Wilk test). Thus, we report results from nonparametric tests (however, the results remain the same with parametric tests). We used Mann-Whitney U tests to compare ipsilateral versus bilateral CST subgroups on manual dexterity (JTTHF affected hand score), bimanual performance (AHA units), mirror movement strength (mirror to voluntary RMS ratio), size and excitability of contralesional motor representations of the affected FDI, and its overlap with motor representations of the less-affected FDI. We report Spearman’s rank correlations (rs) and 95% CIs (in square brackets) as measures of the association between TMS and functional measures. The α level was .05.
CST Pattern Characterization
In 30 children, only stimulation of the nonlesioned hemisphere evoked MEPs in the affected FDI (ie, ipsilateral affected CST pattern). In 14 participants, stimulation of both hemispheres evoked MEPs of the affected FDI (ie, bilateral affected CST pattern). In 6 children, only stimulation of the lesioned hemisphere evoked MEPs in the contralateral, affected FDI (ie, contralateral affected CST pattern); as stated above, these children were excluded from analyses.
No Association Between Hand Function and CST Pattern
We found no significant difference between ipsilateral and bilateral CST subgroups on measures of unimanual dexterity (U = 177.00; P > .05), bimanual performance (U = 192.00; P > .05), and mirror movement strength (U = 86.00; P > .05); see Figure 1. We explored whether size and excitability of contralesional motor representations of the affected hand, and their overlap with the less-affected hand, might be related to these functional measures in CST subgroups. Because the subgroups did not differ on any measures, we combined them for correlational analyses.
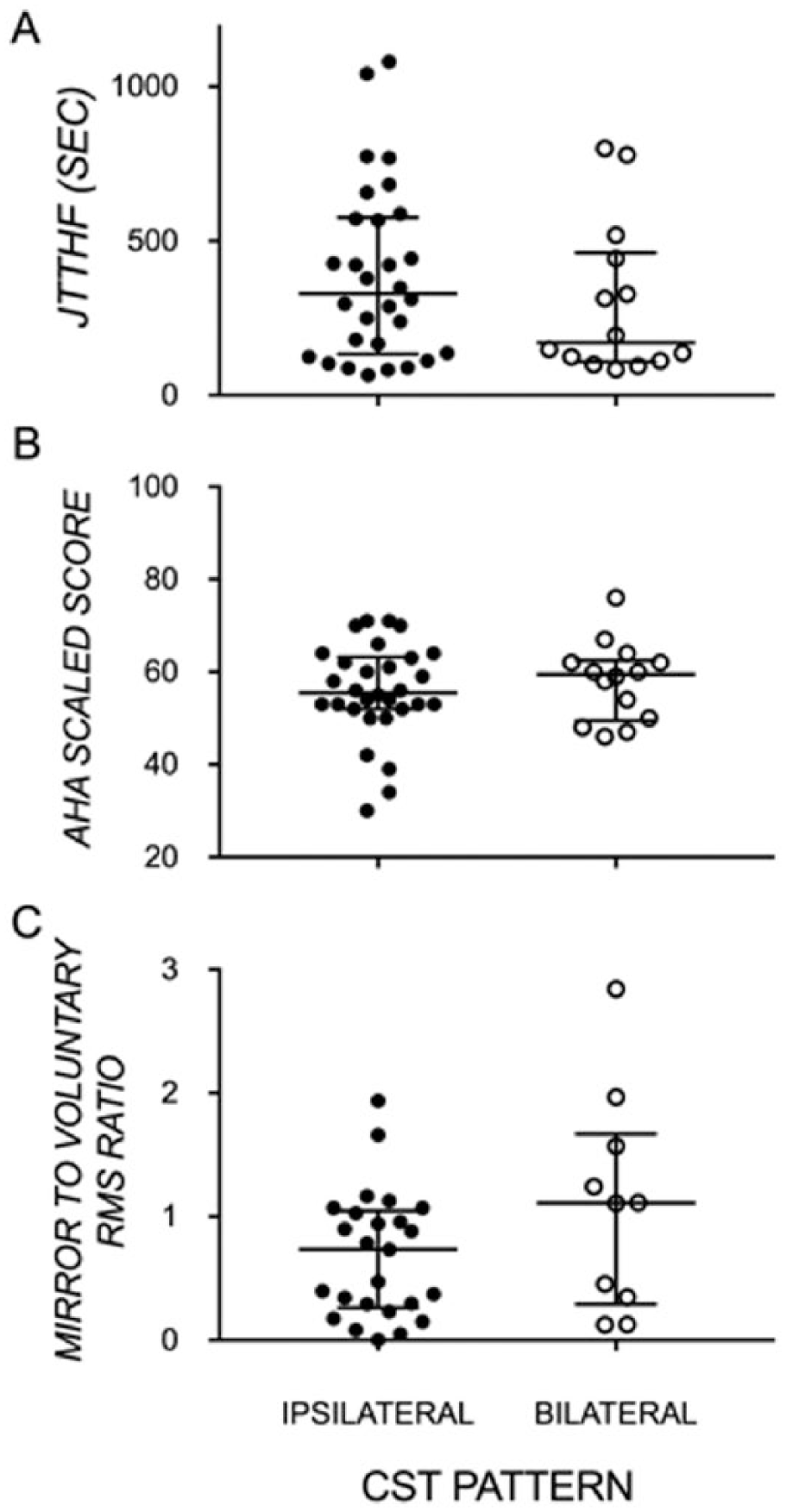
Median and interquartile range of (A) manual dexterity of the affected hand, (B) bimanual performance, and (C) strength of mirror movements by ipsilateral and bilateral CST pattern.
No Association Between Size and Excitability of Contralesional Motor Representations and Hand Function
Representative maps of stimulated sites, and their excitability, in a child with an ipsilateral CST and a child with a bilateral CST are shown in Figure 2. The number of stimulated sites (size) and their overall excitability evoking MEP responses in the affected FDI were similar in both children. As shown in Figure 3 across all participants, there were no significant differences in size (U = 190.50; P > .05) or excitability (U = 167.00; P > .05) of MEP responses between CST subgroups. Nevertheless, these measures of size and excitability of MEP responses in the affected FDI were not associated with manual dexterity (size: rs = 0.03 [−0.28, 0.33], P > .05; excitability: rs = 0.10 [−0.21, 0.40], P > .05), bimanual performance (size: rs = −0.17 [−0.45, 0.14], P > .05; excitability: rs = −0.17 [−0.45, 0.15], P > .05), or mirror movements (size: rs = 0.15 [−0.21, 0.47], P > .05; excitability: rs = 0.13 [−0.22, 0.45], P > .05). Together, this suggests that the magnitude of unimanual and bimanual impairments and mirror movement strength in these children is not explained by the absolute size or excitability of the contralesional motor representation of the affected hand.
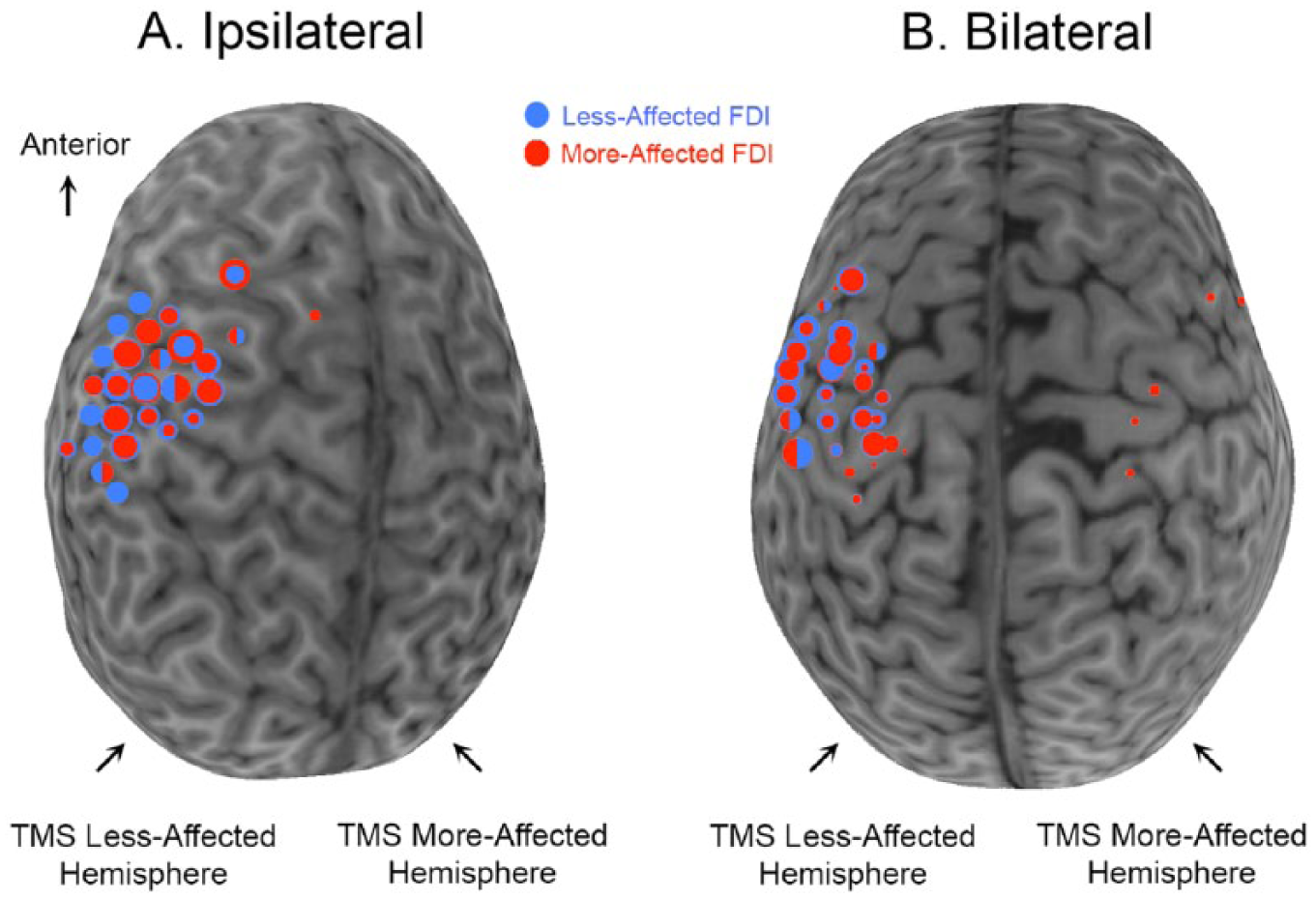
Individual representative maps of children with ipsilateral (A) or bilateral (B) control of the affected FDI. Circles are superimposed onto each child’s MRI. Red circles denote sites at which a TMS pulse evoked an MEP in the affected FDI. Blue circles denote sites at which a TMS pulse evoked an MEP in the less-affected FDI. The size of the circle represents the excitability of the MEP response at that site. At many sites, MEPs were evoked in both FDIs. When one MEP was stronger than the other, different-sized concentric circles represent the sizes of the 2 MEPs. If MEP size was similar for both FDIs at one spot (less than 0.20 difference in normalized MEP), the circle is half red, half blue.

Medians and interquartile ranges showing no group differences in ipsilateral and bilateral CST types but large within-group variation in (A) the number of stimulated sites that evoked an MEP in the affected FDI; (B) the sum of normalized MEPs in the affected FDI; (C) proportion of stimulated sites that elicited an MEP in the affected FDI, which also elicited an MEP in the less-affected FDI; and (D) the proportion of the sum of normalized MEPs of “shared” sites (sites evoking bilateral MEPs) recorded in the affected FDI relative to the total sum of normalized MEPs recorded in the affected FDI.
Association Between Overlap in Motor Representations and Hand Function
In most children, the maps of the affected and less-affected FDIs were highly overlapping (ipsilateral: 77.50% ± 24.56%; bilateral: 79.77% ± 21.71%) and contributed substantially to the summed excitability from all sites eliciting MEPs in the affected FDI (ipsilateral: 80.64% ± 26.30%; bilateral: 83.78% ± 20.96%). On average, 4 sites elicited MEPs in only the more affected FDI, 8 sites elicited MEPs in only the less-affected FDI, and 17 sites (ie, ~80% of responses in affected FDI) elicited MEPs in both FDIs. There were no significant differences in the amount of overlap (U = 196.00; P > .05) and the excitability of overlapping sites (U = 188.00; P > .05) between CST subgroups.
We found significant moderate correlations between manual dexterity of the affected hand (rs = −0.51 [−0.70, −0.24]; P < .001) and bimanual performance (rs = 0.44 [0.15, 0.65]; P < .01) with the amount of overlap of the maps of the 2 FDIs (Figure 4). Furthermore, the relative excitability of these shared sites also correlated with manual dexterity (rs = −0.48 [−0.68, −0.20]; P < .01) and bimanual performance (rs = 0.39 [0.10, 0.62]; P < .01). These findings suggest that the size and excitability of overlapping shared representations of the 2 hands, rather than the overall size or excitability of representations of the affected hand, is related to manual dexterity and bimanual hand use in children with contralesional CST patterns.
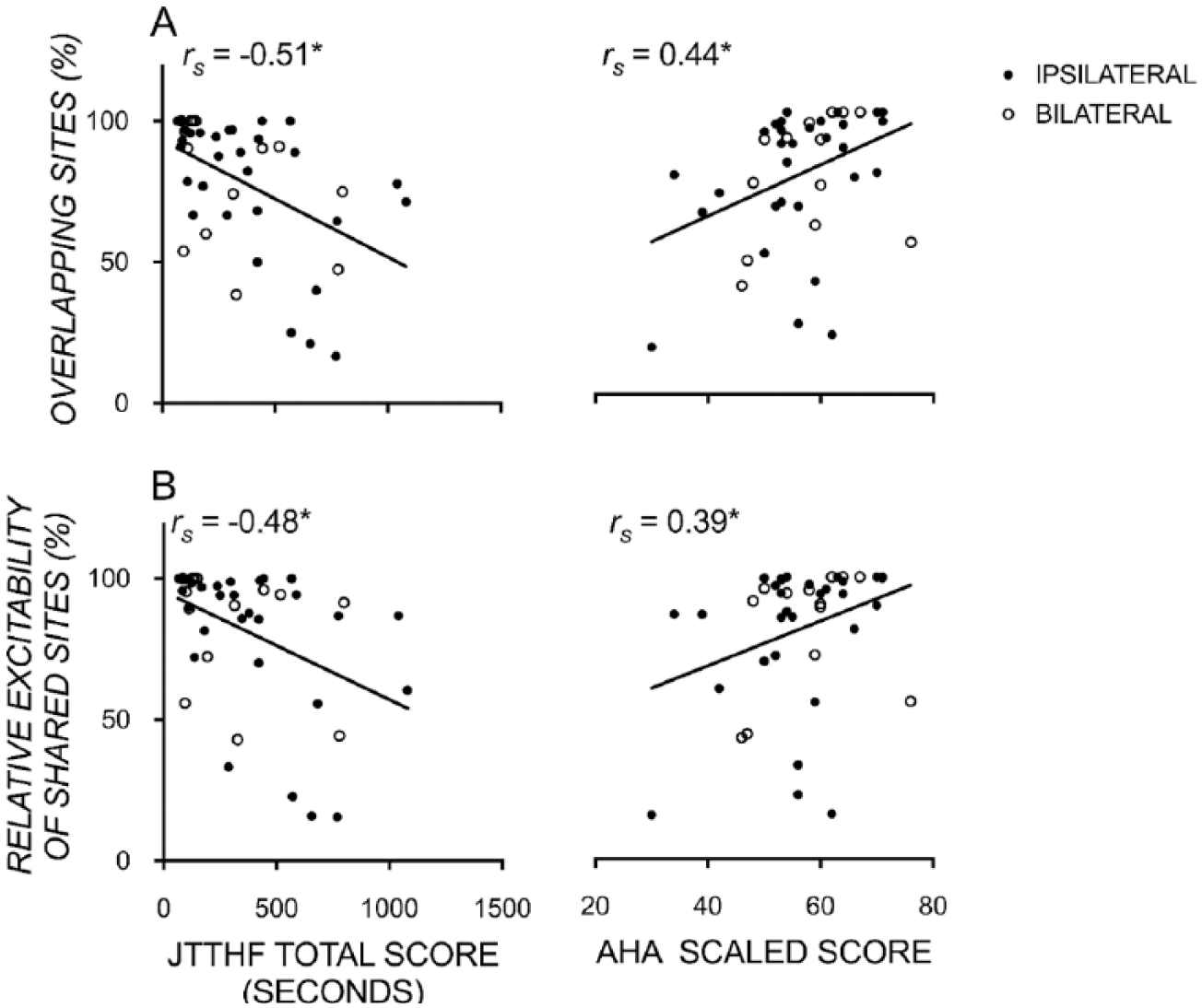
Scatterplots showing significant moderate correlations between unimanual function (JTTHF), bimanual function (AHA logit score), and the proportion of (A) sites and (B) their strength/excitability that were ipsilateral to the more affected hand and evoked bilateral motor-evoked potentials recorded in both the more- and less-affected FDI muscles. *P < .05.
Finally, we found moderate correlations between mirror movement strength and the size (rs = 0.54 [0.24, 0.74]; P < .001) and excitability (rs = 0.58 [0.30, 0.77]; P < .001) of overlapping maps of the 2 FDIs (Figure 5). Of note, there was no significant association between mirror movement strength and unimanual dexterity (rs = −0.07 [−0.40, 0.28]; P > .05) or bimanual performance (rs = −0.009 [−0.33, 0.35]; P > .05). This indicates that a greater map overlap has the functional consequence of coactivating both hands during voluntary movement of the less-affected hand, the latter of which does not help or hinder unimanual or bimanual performance.
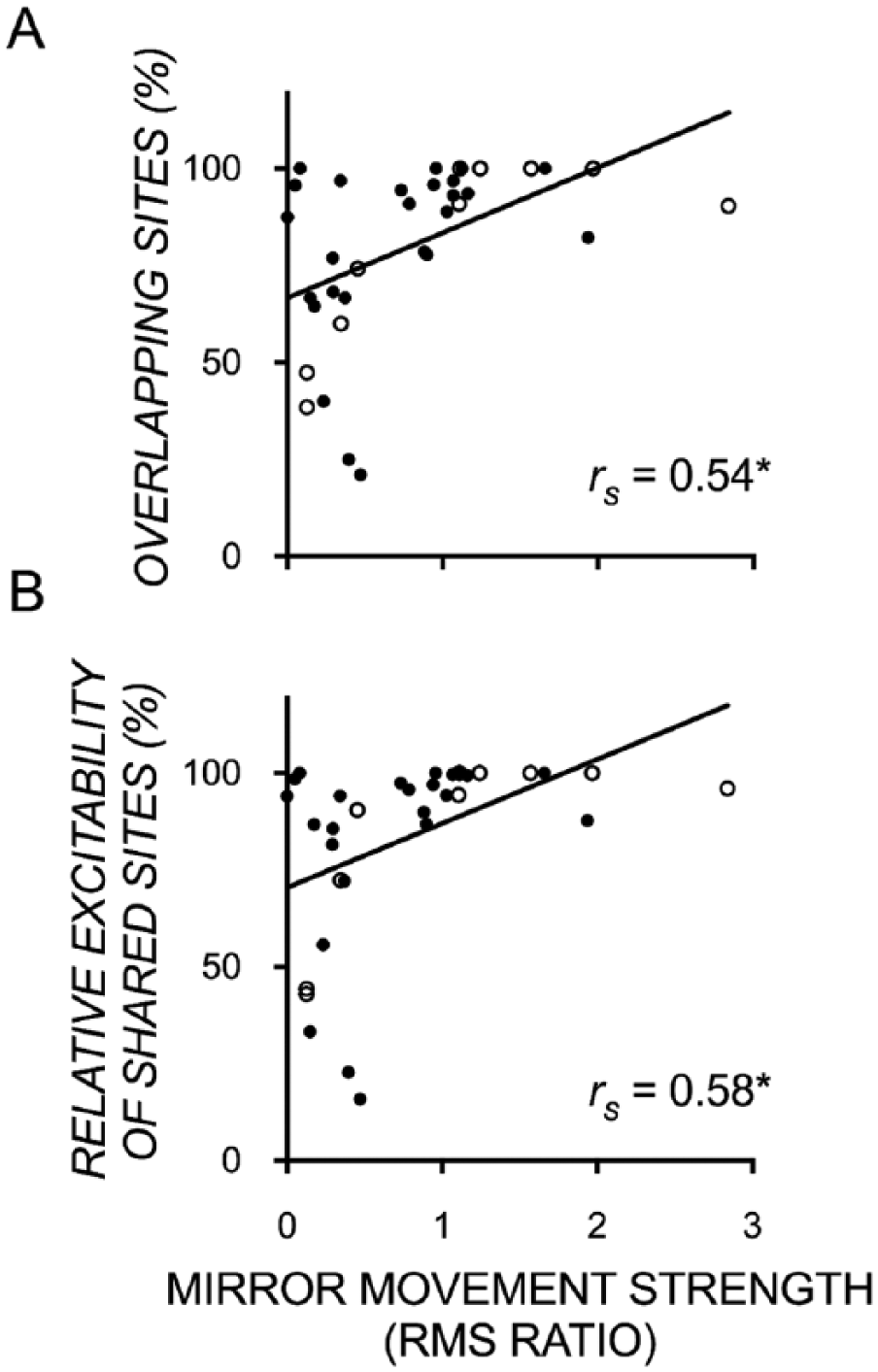
Scatterplots showing significant moderate correlations between mirror movement strength (ratio of mirror to voluntary RMS) and the proportion of (A) sites and (B) their excitability that were ipsilateral to the more-affected hand and evoked bilateral motor-evoked potentials recorded in both the more- and less-affected FDI muscles. *P < .001.
Discussion
Here, we investigated the link between hand function and the size and total excitability of motor representations of the affected hand, and their overlap with motor representations of the less-affected hand, in the contralesional hemisphere of children with USCP. The first main and novel finding is the large amount of overlap in contralesional motor representations of the affected hand with that of the less-affected hand. Second, and as we hypothesized, we found that the size and excitability of such shared-site representations were moderately and positively associated with manual dexterity of the affected hand and the effectiveness to which this hand is incorporated in bimanual play. We also found that the size and excitability of such shared-site representations were moderately and positively associated with the strength of mirror movements. Contrary to our hypothesis, such associations were not present when we correlated these behavioral measures with overall size and excitability of motor representations of the affected hand (ie, including representations from sites that were not shared). To our knowledge, this is the first study to have examined the overlap between affected and less-affected motor representations in the contralesional hemisphere in children with USCP.
Substantial Overlapping Motor Representations
We found that the affected hand’s contralesional motor representation was largely overlapping with the less-affected hand’s contralateral motor representation. This has not yet been demonstrated in children with USCP with ipsilateral CST patterns, though overlap of multijoint representations has been demonstrated in healthy adults 12 and animal models.11,20-22 Also, the center of gravity of less-affected and affected motor maps have been shown to overlap in a small subset of children (n = 6) with congenital hemiplegia. 29
Association Between Hand Function and Overlapping Motor Representations
Consistent with a previous report, 9 we found large variation in affected hand function in children with ipsilateral or bilateral CST patterns. We examined whether features of contralesional motor representations might explain the source of this variation. Although hand function was unrelated to the size and excitability of motor representations of the affected FDI, we found that the size and excitability of overlapping motor representations was related to hand function. Greater and stronger overlap was associated with better unimanual and bimanual performance as well as stronger mirror movements.
The links between manual dexterity and bimanual performance and overlapping motor representations has not been documented in USCP. However, in animal models, motor learning or postinjury motor recovery is associated with increased multijoint representations.21,22 In humans, motor representations of fingers that are often used together (eg, ring and middle fingers) 30 and muscles within 1 limb12,31,32 often overlap. There are important differences between that shown in previous work in healthy adults, in animal work, and in children with USCP. The healthy adult and animal studies show relationships between function and overlap of motor representations of multiple muscles/movements of 1 limb in 1 hemisphere. Here, we show relationships between function and overlap in motor representations of muscles from 2 limbs in 1 hemisphere. In both cases, their relationships to functional measures (eg, hand motor skill in animal work, unimanual and bimanual motor performance, and mirror movement in USCP) raises the possibility that such convergence of representations (of muscles within the hand and between hands) is to some extent functionally useful. In the animal work, it has been suggested that multijoint sites might encode simple motor synergies and, at least in the cat and monkey, increase in frequency in skill training that encourages such synergies.20,33 The role of overlapping representations of the 2 hands within the contralesional hemisphere might be different from that of overlapping representations of multiple joints of 1 limb in the contralesional hemisphere. Particularly, overlapping motor representations within the contralesional hemisphere might be adaptively “yoked,” such that cortical control of the less-affected hand assists or supports that of the affected hand. Although speculative, children with contralesional CST patterns might benefit more from bilateral hand therapeutic interventions, if such interventions increase overlapping motor representations.
The links between the strength of mirror movements and overlapping representations has also not been reported in USCP. However, in a mouse model, conditional forebrain ablation of the Ephrin A4 gene, which is involved in preventing spinal axons from crossing the midline, resulted in sustained bilateral CST connections. 34 Intracortical microstimulation of M1 unilaterally evoked movement of both forelimbs, suggesting overlapping motor representations to be a possible neural mechanism underlying mirror movements. Greater map overlap, and its excitability, has the functional consequence of coactivating both hands during voluntary movement of one hand. Interestingly, coactivating both hands during voluntary movement of one hand does not appear to help or hinder unimanual or bimanual performance.
We found that mirror movements were not associated with unimanual or bimanual performance. This suggests that the presence of mirror movements does not help or hinder hand function, at least as measured in our sample. The association between mirror movements and upper-limb function is unclear: whereas some studies find no associations,9,35 others show weak to moderate associations.36,37 Varying findings are likely a result of varying measures of mirror movements and hand function. For example, it could be argued that our assessments did not measure the ability to precisely individuate digits or the ability to perform different actions with each hand, skills that might be impaired by mirror movements. Therefore, mirror movement or other functional assessments that specifically measure digit individuation might show an opposite relationship to overlapping motor representations, which would suggest negative consequences of such overlapping representations. We did not specifically measure how overlapping motor representations in the contralesional hemisphere might affect digit individuation, within or between hands. It is possible that overlapping motor representations might show a different functional association depending on how function is measured.
It is notable that overlapping motor representations have also been associated with maladaptive processes, suggesting that overlap of motor representations can also have negative functional consequences. The best-characterized symptom arising from overlapping cortical representations is focal hand dystonia (see review 38 ). In focal dystonia, repetitive hand use and coactivation of sensory receptors can result in the convergence of sensory and motor representations of different muscles. This maladaptive plasticity results in painful, repetitive, uncontrolled movements. The neurophysiological underpinnings of focal dystonia include not only the overlap of different representations, but also altered inhibitory control (eg, intracortical inhibition, surround inhibition) and sensorimotor integration.23,38 Children with USCP with ipsilateral CST patterns showed reduced short-interval intracortical inhibition compared with those with contralateral CST patterns. 39 The interactions between motor representation overlap, inhibitory control, and hand function need further exploration in children with USCP.
No Association Between Hand Function and Size and Excitability of Contralesional Motor Representations of the Affected Hand
Unlike the demonstrated functional importance of overlapping hand representations in the contralesional hemisphere, there were no significant associations between hand function and the size and excitability of affected hand motor representations. This result was unsurprising because many have shown that intervention-based changes in map size18,20,22 or overlap of maps,11,22 rather than absolute size or excitability of maps, are most meaningfully related to function. These findings are consistent with those of Kesar et al, 19 who showed no link between total map excitability and motor function in USCP.
Limitations and Future Directions
Some limitations constrain the applicability and interpretation of our findings. First, the less-affected FDI’s motor representation might have been under- or overestimated because the rMT of the affected FDI was used to calculate the mapping intensity (110% rMT). Thus, it is likely that we have not reliably captured the less-affected FDI motor representation. Ideally, contralesional motor maps would be mapped twice, at 2 stimulus intensities, based on the rMT of each FDI. The rMT of the less-affected FDI was typically lower or equal to the rMT of the affected FDI, meaning that the less-affected FDI representation was often derived using a stimulation intensity greater than 110% rMT. Thus, we could not compare the size and excitability of the less-affected FDI representation with that of the affected FDI.
Second, our results were derived from children with mild to moderate impairment severity. Therefore, our findings cannot be generalized to children with more severe impairments. Children with more severe impairments are more likely to have ipsilateral CST patterns.7,8 Thus, including children with more severe impairments might show hand function differences between different CST subgroups. Furthermore, larger sample sizes (particularly of the bilateral CST group) might also show between-group differences in functional and TMS measures.
Third, a study by Vandermeeren et al 40 has identified in a subsample of children with congenital hemiplegia the presence of distinct clusters of long-latency MEPs (>40 ms) in addition to the presence of the more commonly studied short-latency MEP (<40 ms). In the current study, we excluded any MEPs with latencies longer than 40 ms because we found it difficult to objectively discriminate such responses from muscular and/or auditory startle responses. As Vandermeeren et al noted, these longer-latency MEPs might have mechanisms that are distinct from short-latency ones as well as unique functional associations. Thus, it is conceivable for motor maps derived from longer-latency MEPs to have a different functional association than that derived from short-latency MEPs as was used here.
Fourth, we note the possibility of TMS-evoked responses to arrive via extrapyramidal tracts and not necessarily CST. 41 That extrapyramidal tracts are polysynaptic rather than monosynaptic in nature might result in TMS-evoked responses with longer latencies that are present after the 40-ms cutoff that we imposed on useable MEPs. Carr et al 24 have also shown in children with USCP that ipsilateral MEPs are similar in latency to contralateral MEPs (unlike that seen in healthy adults; eg, Ziemann et al 42 ), thereby adding to the likelihood that these MEPs are mediated via CST and not via other polysynaptic tracts. Finally, Williams and Martin 43 recently showed that these extrapyramidal tracts compete with the corticospinal system after developmental corticospinal injury. They found that M1 inactivation in the cat reduced rubrospinal tracts and increased CSTs (thus, CSTs outcompeted rubrospinal tracts on the ipsilateral side), demonstrating that CSTs steer development and ultimately function of another. Thus, it is more likely for ipsilateral responses to be mediated by CSTs than rubrospinal tracts, following developmental CST injury.
Finally, although we found moderate correlations between hand function and contralesional map overlap, we suspect the contribution to a child’s impairment to be multifactorial, which likely include the timing and location of a child’s lesion 1 and the amount of therapy received.
Conclusion
This is the first study in children with USCP to document the large amount of overlap in contralesional motor representations of the 2 hands, which our results suggest is a behaviorally favorable byproduct of neuroplasticity.
Footnotes
Acknowledgements
We thank Muc Du, Doug Fallon, PhD, and Jonathan Dyke, PhD, for MRI acquisition and Geoff Hammond, PhD, for his assistance with data interpretation. We also thank all study volunteers for their assistance with data collection and analyses and the participants and their families for participating in the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funded by R01 HD076436-A01, NS062116 (KMF), Columbia Professional Schools Diversity Award (KMF), NIH CTSA Award (KMF; KL2 RR024157, UL1 RR024156, TL1 RR024158), Fonds de recherche du Québec–Santé (Postdoctoral training award, VHF), Horace W. Goldsmith Foundation Grant (DG), and Endeavour Australia (Research Fellowship, MM). Research reported in this publication was supported by the National Center for Advancing Translational Science of the National Institute of Health Under Award Number UL1TR000457.