
Abstract
Background. In a combined animal and human study, we have previously found that a 5-day treatment that enhances cortical plasticity also facilitates brain-derived neurotrophic factor (BDNF)-tyrosine receptor kinase B (TrkB) signaling and increases activated TrkB and N-methyl-
Keywords
Introduction
We have previously found that a 5-day course of 5 Hz of repetitive transcranial magnetic stimulation (rTMS), a treatment designed to enhance cortical plasticity, upregulates the brain-derived neurotrophic factor (BDNF)-tyrosine receptor kinase B (TrkB) in both the cortex and the peripheral lymphocytes of humans and animals. 1 BDNF-TrkB signaling in lymphocytes is rather stable because samples collected over time are not altered without a targeted intervention. 1 The increments of BDNF-TrkB signaling in lymphocytes were highly correlated with those in the cortex and with changes in cortical excitability, 1 suggesting that BDNF-TrkB signaling in lymphocytes reflects, at least in part, cortical TrkB signaling. Indeed, TrkB, a member of the neurotrophin receptor tyrosine kinase family, is expressed ubiquitously in the nervous system, in different organs and in immune cells. On binding of BDNF, TrkB signaling promotes, in general, cell development, maturation, and survival2,3 and, at the cortical level, also facilitates mechanisms related to neuronal plasticity, including long-term potentiation (LTP) and synapse formation.4-6
Parkinson’s disease (PD) is a progressive neurodegenerative disorder characterized by abnormal motor and nonmotor signs. More recently, electrophysiological studies have also revealed decreased LTP-like plasticity in the cortex of patients with PD.7,8 As a result, PD patients exhibit deficits in short- and long-term retention of newly learned motor skills9-12 that can be restored by enhancing local LTP-like plasticity with rTMS. 12 A more general improvement in plasticity might be obtained by aerobic exercise, as suggested by recent studies in normal animals, 13 in an animal model of PD, 14 in normal humans, 15 and in patients with neurodegenerative diseases. 16 In particular, the multidisciplinary intensive rehabilitation treatment (MIRT), a 4-week protocol that includes aerobic exercise as well as functional and goal-directed training,17-21 produces a long-lasting improvement on the motor and nonmotor functions of patients with PD.22-25 Specifically, in a 2-year study, a comparison between 2 groups of patients in the early stages of PD treated with the same amount of rasagiline revealed that Unified Parkinson’s Disease Rating Scale (UPDRS) II and III scores as well as other clinical parameters progressed more slowly in the MIRT group. 25 More important, at the end of this study, the percentage of patients requiring an increase in levodopa-equivalent dosage remained lower in the MIRT group (25%) compared to that in the other group (80%). Altogether, these results suggest that MIRT might decrease the rate of disease progression, although the precise mechanisms remain largely unknown. Nevertheless, it is very plausible that the enhancement of phenomena related to cortical plasticity might play a role in these neuroprotective and neurorestorative effects. If so, based on our finding that changes of BDNF-TrkB signaling are highly correlated in the cortex and in the lymphocytes, 1 we could expect that a 4-week MIRT in patients with PD will also enhance BDNF-TrkB signaling in lymphocytes.
Materials and Methods
Participants and Clinical Assessment
Participants were 16 patients with PD whose clinical characteristics are reported in Table 1. Inclusion criteria were Mini-Mental State Examination score >24, ability to walk without physical assistance, ability to perceive visual and auditory cues, right-handedness, and no neurological conditions other than PD. Participants were admitted to the Department of Parkinson’s Disease Rehabilitation at “Moriggia Pelascini” Hospital (Gravedona ed Uniti, Italy) and underwent a 4-week MIRT while continuing their pharmacotherapy. We collected blood at 3 time points: at baseline, after 2 weeks of MIRT, and after 4 weeks of MIRT. Clinical scores were assessed at baseline and after 4 weeks of MIRT by the same neurologist and physiotherapist, experts in movement disorders and blinded to the study design. The assessments included the following: UPDRS, 6-Minute Walking Test, Berg Balance Scale, Timed Up and Go Test, Parkinson’s Disease Disability Scale, and the Freezing of Gait Questionnaire. The same neurologist performed all clinical assessments. The study protocol was conducted according to the Declaration of Helsinki and approved by the local scientific committee and institutional review board of “Moriggia Pelascini” Hospital. All participants gave informed consent before participation.
Characteristics of Patients at Baseline.
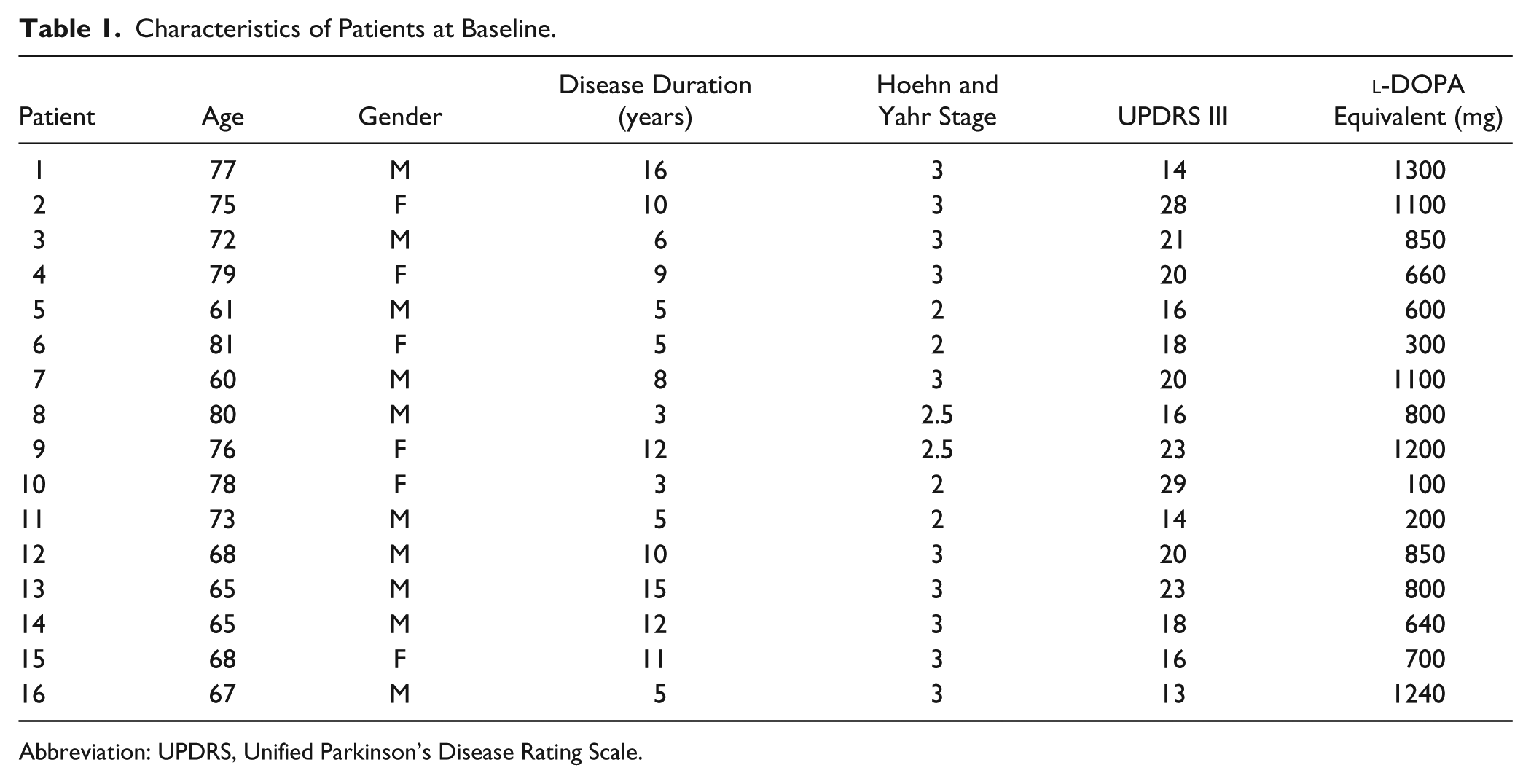
Abbreviation: UPDRS, Unified Parkinson’s Disease Rating Scale.
Multidisciplinary, Intensive Rehabilitation Treatment
MIRT has been fully described in previous publications.17-25 Briefly, MIRT consisted of 4 weeks of physical therapy and exercise, with 3 daily sessions, 5 days a week. The first was a one-to-one session with a physical therapist, involving muscle stretching; exercises to improve the range of motion of the spinal, pelvic, and scapular joints; strengthening of abdominal muscles; postural changes; and balance training on a posturographic platform. The second session included aerobic training on (1) a treadmill equipped with both visual and auditory cues, (2) a stationary bike, (3) an elliptical machine providing visual feedback, and (4) a stabilometric platform. The third was an occupational therapy session to improve autonomy in daily life, use of tools, dressing, transferring from sitting to standing, rolling from supine to sitting, and leg coordination in walking and turning.
Lymphocyte Collection, Treatment, Immunoprecipitation, and Western Blotting
Whole blood was collected in EDTA tubes in the morning, between 7 and 8
TrkB signaling complexes, extracellular-signal-regulated kinase 2 (ERK2), and protein kinase B1 (AKT1) in 100 µg lymphocyte lysate were separately immuoprecipitated by a 2-hour incubation (4°C) with 1 µg immobilized anti-TrkB (for assessment of pY-TrkB; phospholipase C [PLC]-γ1, SRC homology-containing protein [Shc] recruitment; and TrkB-N-methyl-
Statistical Analyses
All data are presented as mean ± standard deviation (SD). For each component of the TrkB signaling pathway, we computed the changes between the BDNF-stimulated and unstimulated conditions as a ratio between the two (ie, BDNF-stimulated/ BDNF-unstimulated) at 3 time points (pre-MIRT, 2-weeks after MIRT, and 4 weeks after MIRT). Treatment effects were evaluated by repeated-measures ANOVA, using time as the independent variable with 3 levels: pre-MIRT, 2-week MIRT, and 4-week MIRT. We used Mauchly’s test for the verification of sphericity and reported Greenhouse-Geisser corrected degrees of freedom (df) when sphericity could not be assumed. We used post hoc tests with Bonferroni correction for multiple comparisons.
Furthermore, we computed changes in BDNF-TrkB signaling as follows:

We correlated these changes with the differences between clinical scores collected after 4 weeks of MIRT and those collected pre-MIRT.
Results
Clinical Scores Improve After 4 Weeks of MIRT
A total of 16 patients completed the 4 weeks of MIRT. As shown in Table 2 and in agreement with our previous results,17-25 all scores reveal significant improvement after MIRT compared with baseline.
Clinical Scores at Baseline and After 4-Week MIRT (UPDRS II: Activities of Daily Living; UPDRS III: Motor Examination; UPDRS IV: Complications of Therapy).
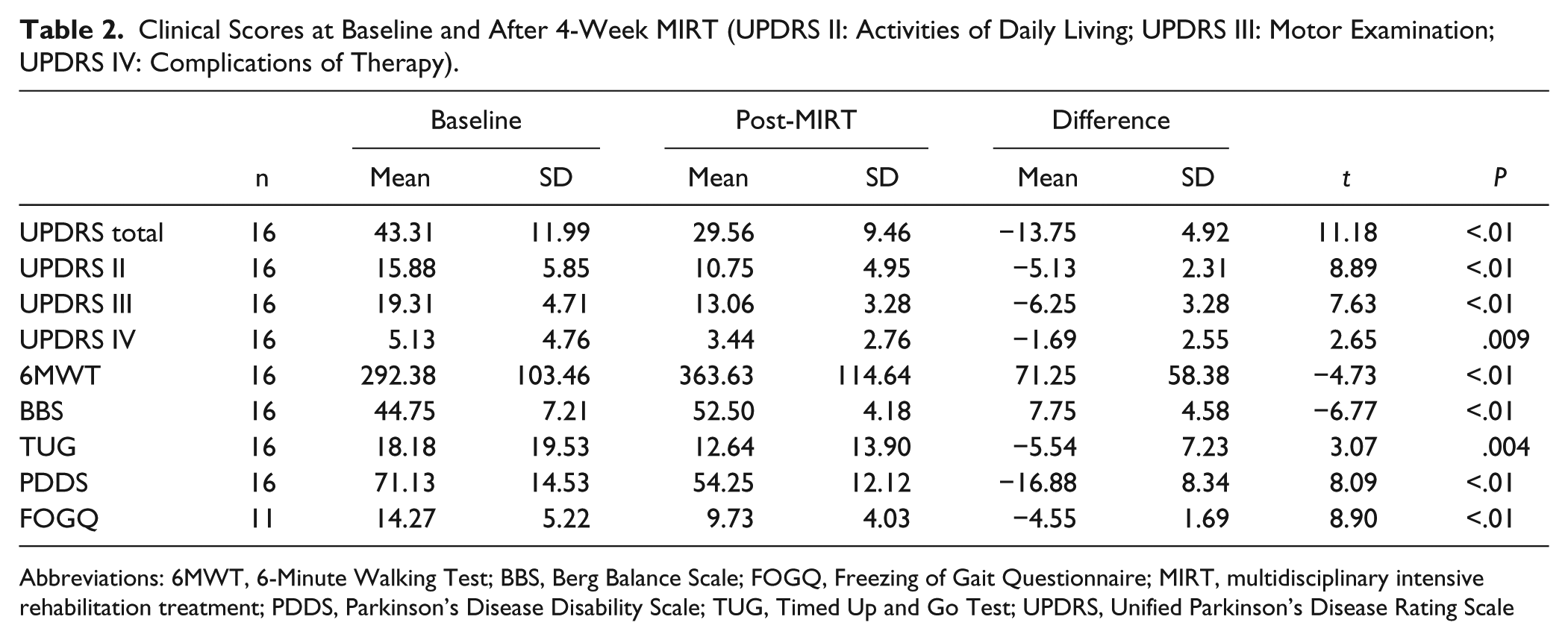
Abbreviations: 6MWT, 6-Minute Walking Test; BBS, Berg Balance Scale; FOGQ, Freezing of Gait Questionnaire; MIRT, multidisciplinary intensive rehabilitation treatment; PDDS, Parkinson’s Disease Disability Scale; TUG, Timed Up and Go Test; UPDRS, Unified Parkinson’s Disease Rating Scale
TrkB Signaling in Lymphocytes Is Enhanced Following MIRT
We first evaluated the changes in BDNF-TrkB signaling in lymphocytes following MIRT. The expressions of TrkB 145-kDa and 95-kDa, ERK2, or Akt1 remain stable across the 3 time points—pre-MIRT as well as after 2 and 4 weeks of MIRT—both under unstimulated and BDNF-stimulated conditions (Figure 1A and 1C). Similarly, the expression of Shc, PLC-γ1, and NR1 was not affected by either BDNF stimulation or MIRT (data not shown).
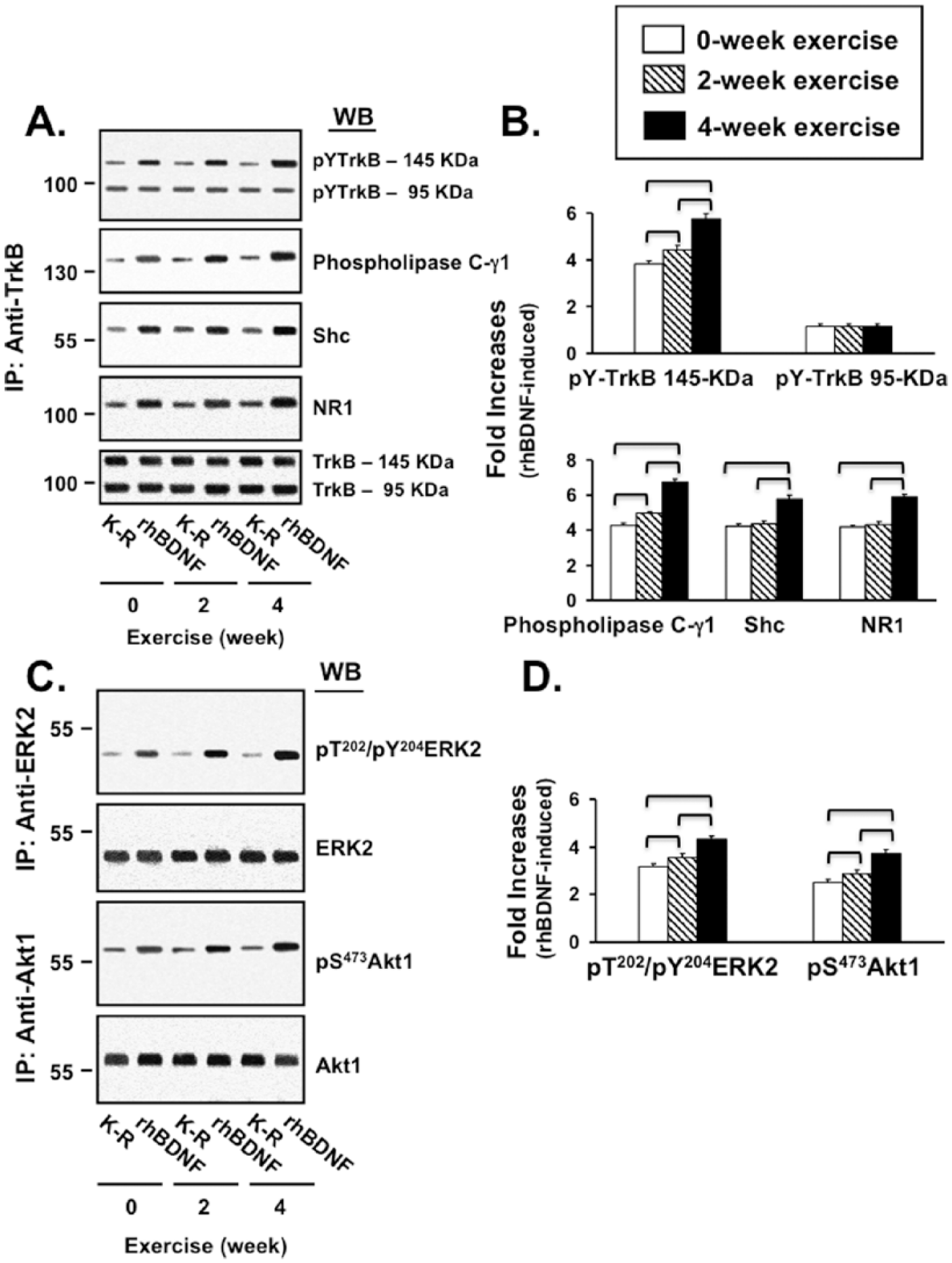
A, B: Levels of pY-TrkB 145-KDa, pY-TrkB 95-KDa, recruited PLCγ1, Shc, and NR1 normalized for total amount of either TrkB-145 KDa or TrkB-95 KDa. C, D: Levels of pT/pY-ERK2 and pS-Akt1 normalized for total amount of ERK2 or Akt1, respectively.
The results of statistical analysis of MIRT effects (repeated-measure ANOVA and post hoc tests) on each component of TrkB signaling are summarized in Table 3. In lymphocytes collected pre-MIRT, BDNF-stimulation increased pY-TrKB 145 kDa level by 286% ± 31%, with minimal changes in pY-TrkB 95 kDa (19% ± 7%). Following 2 and 4 weeks of MIRT, the BDNF-induced pY-TrkB 145 kDa levels were further increased by 15.6% ± 7.1% and 52.6% ± 10.8%, respectively, without significant increases of pY-TrkB 95 kDa levels. Post hoc tests confirmed that the pY-TrKB 145-kDa level pre-MIRT (3.86 ± 0.31) was significantly lower compared with both 2 (4.47 ± 0.55) and 4 weeks of MIRT (5.89 ± 0.60). The difference between 2 and 4 weeks was significant as well (Figures 1A and 1B).
Results of ANOVA and Post Hoc Tests: Effect of MIRT on BDNF-TrkB Signaling and TrkB-NMDAR Recruitment. a
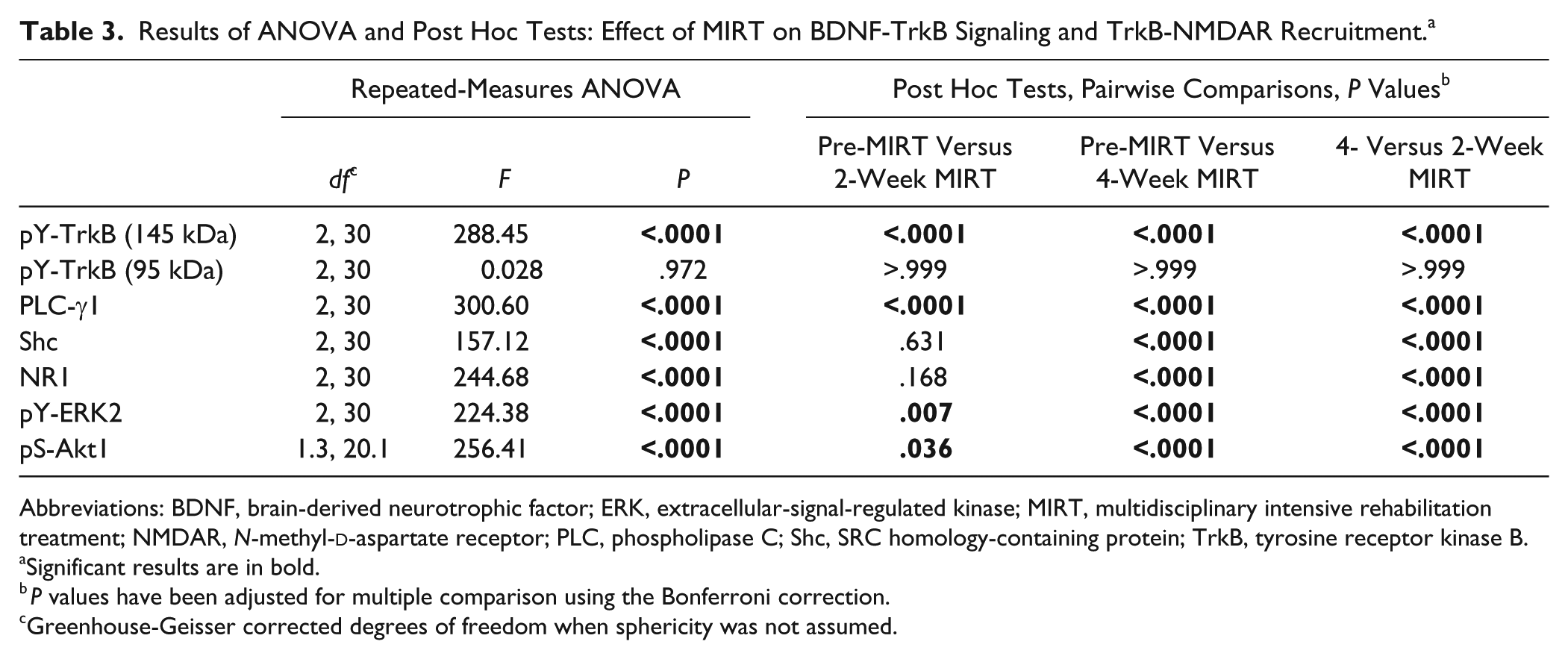
Abbreviations: BDNF, brain-derived neurotrophic factor; ERK, extracellular-signal-regulated kinase; MIRT, multidisciplinary intensive rehabilitation treatment; NMDAR, N-methyl-
Significant results are in bold.
P values have been adjusted for multiple comparison using the Bonferroni correction.
Greenhouse-Geisser corrected degrees of freedom when sphericity was not assumed.
Similar results were obtained for PLC-γ1 and Shc (Figures 1A and 1B). Pre-MIRT, BDNF stimulation enhanced pY-TrkB recruitment of PLC-γ1 and Shc by 328% ± 41% and 321% ± 47%, respectively. It is important to note that MIRT significantly increased the recruitment of PLC-γ1 and Shc; post hoc tests confirmed that the levels of recruited PLC-γ1 after 2 weeks of MIRT (4.95 ± 0.37) were already significantly higher than pre-MIRT (4.28 ± 0.42). Further significant increase was observed after 4 weeks of MIRT (6.75 ± 0.53). On the other hand, Shc recruitment at pre-MIRT (4.22 ± 0.48) and after 2 weeks of MIRT (4.33 ± 0.55) were comparable but significantly higher after 4 weeks of MIRT (5.78 ± 0.69).
To gain insight into MIRT-induced recruitment of the NMDA receptor, we measured the level of obligatory NMDAR NR1 subunit associated with TrkB (Figures 1A and 1B). Pre-MIRT, BDNF stimulation increased TrkB-NR1 association by 315% ± 22%. TrkB-NMDAR interaction increased with MIRT; post hoc tests showed that 4 weeks of MIRT (5.87 ± 0.47) significantly increased TrkB-NMDAR interaction compared with pre-MIRT (4.15 ± 0.22) and 2 weeks of MIRT (4.32 ± 0.44).
BDNF-activated pT/pY-ERK2 and pS473-Akt1 levels also increased with MIRT, as shown in Figures 1C and 1D. In lymphocytes collected pre-MIRT, BDNF stimulation increased pT/pY-ERK2 by 224% ± 13% and pS473-Akt1 by 158% ± 19%. MIRT significantly elevated pT/pY-ERK2 and pS473-Akt1. Post hoc tests showed significant differences between pre-MIRT and 2 weeks of MIRT for both pT/pY-ERK2 (3.24 ± 0.13 vs 3.46 ± 0.28) and pS473-Akt1 (2.58 ± 0.19 vs 2.76 ± 0.32). Further increases were also observed after 4 weeks of MIRT for both pT/pY-ERK2 (4.32 ± 0.25) and pS473-Akt1 (3.74 ± 0.26).
The effects of MIRT on BDNF-TrkB signaling and TrkB-NMDAR interaction are summarized in Figure 2.
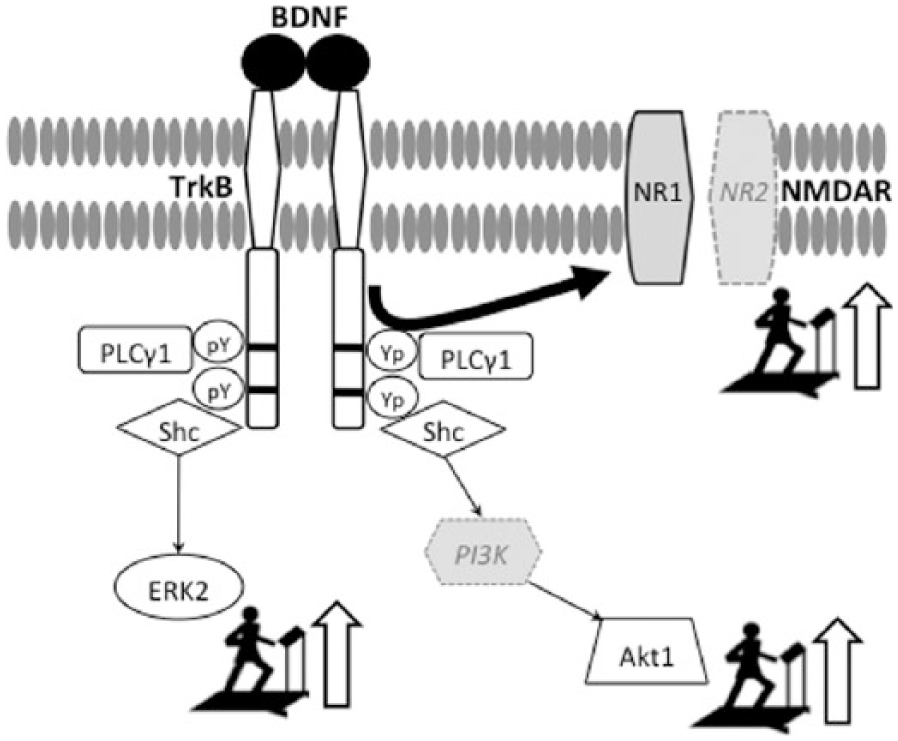
MIRT improves lymphocyte BDNF-TrkB signaling and TrkB-NMDAR interaction. BDNF dimer upon binding its receptor, TrkB recruits PLCγ1 and adaptor protein Shc, enabling activation of the downstream signaling components: ERK2 and Akt1. In addition, the activated TrkB associates with NR1 subunit of NMDAR. Exercise increases all components of these pathways. PI3K and NR2 (in light gray) were not measured.
TrkB Signaling Enhancement in Lymphocytes Correlates With Improvements in UPDRS Scores
We found that the decrements in UPDRS total scores were significantly correlated with the increases in TrkB signaling at the receptor (TrkB 145 kDa), intracellular mediator (PLC-γ1, Shc), and NMDAR interaction levels (NR1). No correlations were found with TrkB 95 kDa and downstream effectors (ERK2 and AKT1), which, however, are not exclusive components of BDNF-TrkB signaling because they participate in other pathways as well and have not been immunoprecipitated with the TrkB complex. Similar results were found for UPDRS II scores (activities of daily living). Illustrations as well as r and P values of such correlations are reported in the supplemental material (Supplemental Figures 1A and 1B). We did not find significant correlations between changes in TrkB signaling components and all the other indices of clinical improvement.
Discussion
The primary and novel result of these studies is that in patients with PD, 4 weeks of MIRT upregulates BDNF-TrkB signaling in the peripheral lymphocytes at the levels of receptors, intracellular mediators, and downstream effectors. It is important to note that these effects were not mediated by increases in the abundance of TrkB and its signaling mediators because there were no detectable changes in the expression levels of any components in the BDNF-TrkB signaling cascade. This indicates that 4 weeks of MIRT fosters a more efficient BDNF-TrkB signaling in lymphocytes, possibly by enhancing BDNF affinity for TrkB. 1 Second, the enhancement of BDNF-TrkB signaling was already present after 2 weeks of MIRT and further increased at the completion of the treatment. Finally, as in the previous MIRT studies,17-25 motor and nonmotor functions improved after the 4-week treatment, despite unchanged pharmacological therapy. The new finding is that TrkB signaling enhancement significantly correlated with improvements in the total UPDRS scores and in activities of daily living, suggesting that the changes in BDNF-TrkB signaling produced a generalized improvement rather than a focal effect on one or a few motor or nonmotor signs. This type of general effect seems in accord with the benefit of aerobic exercise on multiple functions. 15 Although this study did not include a no-exercise group of patients with PD, it is unlikely that the changes we found are related to the mere passage of time, as suggested by the results of previous studies. 1 In addition, in the present study, the changes through the 3 time points were progressive and in the same direction of increased TrkB signaling. Based on these considerations, it is plausible that the changes in lymphocyte BDNF-TrKB signaling are the effects deriving from MIRT and not by the passage of time. Indeed, future studies are warranted to address precisely this point.
It is well established that, in neural cells, the activation of the BDNF-TrkB signaling facilitates LTP by triggering phosphorylation and expression of proteins that are markers of synaptic plasticity. 6 However, the roles of TrkB signaling and TrkB-NMDAR interaction in immune cells are far from being completely understood. BDNF-TrkB signaling seems to be critical in the early T-cell development, in that it promotes both survival of the precursors and further differentiation of the thymocytes throughout the T-cell differentiation pathway.2,26 TrkB signaling is also necessary for normal B-cell development in the bone marrow. 3 It is then plausible that BDNF-TrkB signaling in immune cells might be used to promote cell proliferation and differentiation. TrkB-NMDAR interaction, on the other hand, appears to regulate lymphocyte cytokines production (eg, interleukins, interferon-γ), which in turn, modulates astrocyte and microglia activation and promotes glutamate clearance after neural damage.27,28 It has also been shown that NMDAR is expressed in the lymphocytes that infiltrate the brain lesion sites. 27 In our study, significant changes for BDNF-TrkB signaling but not for TrkB-NMDAR interaction were present already after 2 weeks of treatment, as indicated by the association of NR1 with TrkB. This finding suggests that the enhancement of TrkB signaling precedes the increases in TrkB-NMDAR interaction. Thus, a possible interpretation of the present findings is that the MIRT-induced upregulation of TrkB signaling, and TrkB-NMDAR association in lymphocytes may reflect anti-inflammatory or other processes that in turn promote neurorestoration and recovery of function. Indeed, the results of some studies indicate that inflammation and microglia activation occur in PD. 29 Increased levels of proinflammatory cytokines are present in the serum, spinal fluid, and nigrostriatal regions of patients with PD together with activated microglia surrounding dopaminergic neurons and infiltrated peripheral leukocytes. 29 In support of this interpretation, recent studies showed that motor recovery after 6-hydroxydopamine-induced lesions was delayed in rats with genetically induced lymphocyte deficiency compared with wild-type rats. 30 Nevertheless, further studies are needed to verify whether this is a possible scenario and to define the cascade of effects triggered by the activation of BDNF-TrkB signaling and TrkB-NMDAR association in the lymphocytes. The likelihood of interactions between the cortex and lymphocytes in this context has found further support with the recent discovery of a central nervous lymphatic system. 31
Regardless of their precise functions in the lymphocyte, BDNF-TrkB signaling in lymphocytes and in neural cells are highly correlated because we recently found that they both respond to multiple sessions of rTMS, a treatment that increases LTP-like plasticity. 1 Because of this correlation, we concluded that the enhancement of BDNF-TrkB signaling in the lymphocyte reflects, at least in part, an increase in LTP-related phenomena at the cortical level. 1 Therefore, based on these conclusions, one might interpret the present data and speculate that MIRT-induced upregulation of the BDNF-TrkB pathway may also occur at the cortical level, with an effect on the mechanisms promoting cortical plasticity. Indeed, preliminary results of ongoing electrophysiological studies in our labs show an increase of LTP-like plasticity at the cortical level in a small number of patients who underwent MIRT (G. Frazzitta, M. F. Ghilardi, A. Quartarone, unpublished data). Nevertheless, these data should be interpreted with caution because further studies are needed to prove any scenario correct.
In summary, the main result of the present study is that MIRT enhances BDNF-TrkB signaling in lymphocytes of patients with PD, an increase that parallels their improvement in clinical scores. Further studies are needed to define the relationship between these 2 findings and to determine the mechanisms that link immunity, plasticity, and recovery of function in PD.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the National Institute of Health (NS-054864 to MFG) and the Michael J. Fox Foundation (to HR). The funding sources had no role in data collection, analysis, and interpretation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.