
Abstract
Background. Many stroke patients exhibit excessive compensatory trunk movements during reaching. Compensatory movement behaviors may improve upper extremity function in the short-term but be detrimental to long-term recovery. Objective. To evaluate the evidence that trunk restraint limits compensatory trunk movement and/or promotes better upper extremity recovery in stroke patients. Methods. A search was conducted through electronic databases from January 1980 to June 2013. Only randomized controlled trials (RCTs) comparing upper extremity training with and without trunk restraint were selected for review. Three review authors independently assessed the methodological quality and extracted data from the studies. Meta-analysis was conducted when there was sufficient homogenous data. Results. Six RCTs involving 187 chronic stroke patients were identified. Meta-analysis of key outcome measures showed that trunk restraint has a moderate statistically significant effect on improving Fugl-Meyer Upper Extremity (FMA-UE) score, active shoulder flexion, and reduction in trunk displacement during reaching. There was a small, nonsignificant effect of trunk restraint on upper extremity function. Conclusion. Trunk restraint has a moderate effect on reduction of upper extremity impairment in chronic stroke patients, in terms of FMA-UE score, increased shoulder flexion, and reduction in excessive trunk movement during reaching. There is insufficient evidence to demonstrate that trunk restraint improves upper extremity function and reaching trajectory smoothness and straightness in chronic stroke patients. Future research on stroke patients at different phases of recovery and with different levels of upper extremity impairment is recommended.
Introduction
The upper extremity plays a vital role in the performance of activities of daily living (ADL),1,2 as the ability to reach and grasp is required for over 50% of ADL tasks.3,4 Based on a recent study, 41% of people with moderate to severe stroke and 78% with milder stroke are estimated to regain dexterity 6 months after onset. 5 Hence, improved upper extremity recovery will have a positive effect on ADL.
Numerous studies have demonstrated that stroke patients exhibit excessive trunk movements during pointing and reaching,6-13 a compensatory motor strategy to extend arm reach when shoulder and elbow movement and control is impaired.14,15 Excessive use of compensatory movements can result in secondary complications such as muscle contractures, joint misalignment, pain, limb disuse, and increased energy expenditure.16-18 These complications can impede the longer-term functional recovery of the upper extremity.
Observation of compensatory trunk movement has led to the use of trunk restraint during upper extremity therapy to improve the outcome.19-27 Trunk restraint is usually achieved through a chest harness, based on the assumption that restriction of compensatory trunk movement will encourage the recovery of more normal upper extremity movement patterns. 22 The first study that explored the potential of trunk restraint was conducted on 11 healthy individuals and 11 chronic stroke patients. 22 Kinematic results demonstrated that the amount of trunk displacement during reaching in stroke patients was significantly correlated (r = −0.91) with Fugl-Meyer Upper Extremity (FMA-UE) score, and stroke patients who used the most trunk displacement had the most disrupted coupling between arm joint movements. These findings were substantiated by subsequent studies.19-21,23-27 Restriction of compensatory trunk movements during practice for chronic stroke patients led to reduced trunk displacement, improved shoulder and elbow movements, with straighter reach trajectories, resulting in improvements in reach-to-grasp movements.
From the literature, the trunk restraint technique appears to be a promising adjunct in stroke rehabilitation. However, there is no report of pooled analyses of research data to date. The aim of this systematic review is to evaluate the effects of trunk restraint on upper extremity impairment and function in stroke patients. It will help inform clinical practice and aid therapists in designing comprehensive upper extremity rehabilitation programs for stroke patients.
Methodology
Review Procedure
A comprehensive search of the literature published between January 1980 and June 2013 was conducted using the following electronic databases: CINAHL, EMBASE, MEDLINE, AMED, Web of Science, Cochrane Library, Physiotherapy Evidence Database (PEDro), and OTseeker. The following keywords were used: stroke, cerebrovascular accident, trunk, restraint, upper limb, upper extremity, reaching, reach-to-grasp, grasping. An example of search strategy for MEDLINE is found in Appendix A. This search strategy was modified to suit different databases.
Examining the references from the retrieved articles identified additional relevant studies. Full-text articles were retrieved if they fitted the inclusion criteria. The following criteria were used to identify relevant publications:
The inclusion criteria were the following:
Full publication in a peer-reviewed journal
Published in English language
Randomized controlled trials
Involved adult stroke participants
Intervention involved any form of trunk restraint (physical restraint, auditory feedback)
Outcomes of upper extremity were examined in terms of body functions and body structures, activity, and/or participation, as per the International Classification of Functioning, Disability and Health (ICF)
The exclusion criteria was the following:
The primary purpose was not to promote upper extremity motor impairment or function
The following data were extracted from the identified publications: participants’ characteristics, setting, study design, outcome measures, intervention, and key findings (Tables 1 and 2).
Participants’ Characteristics.
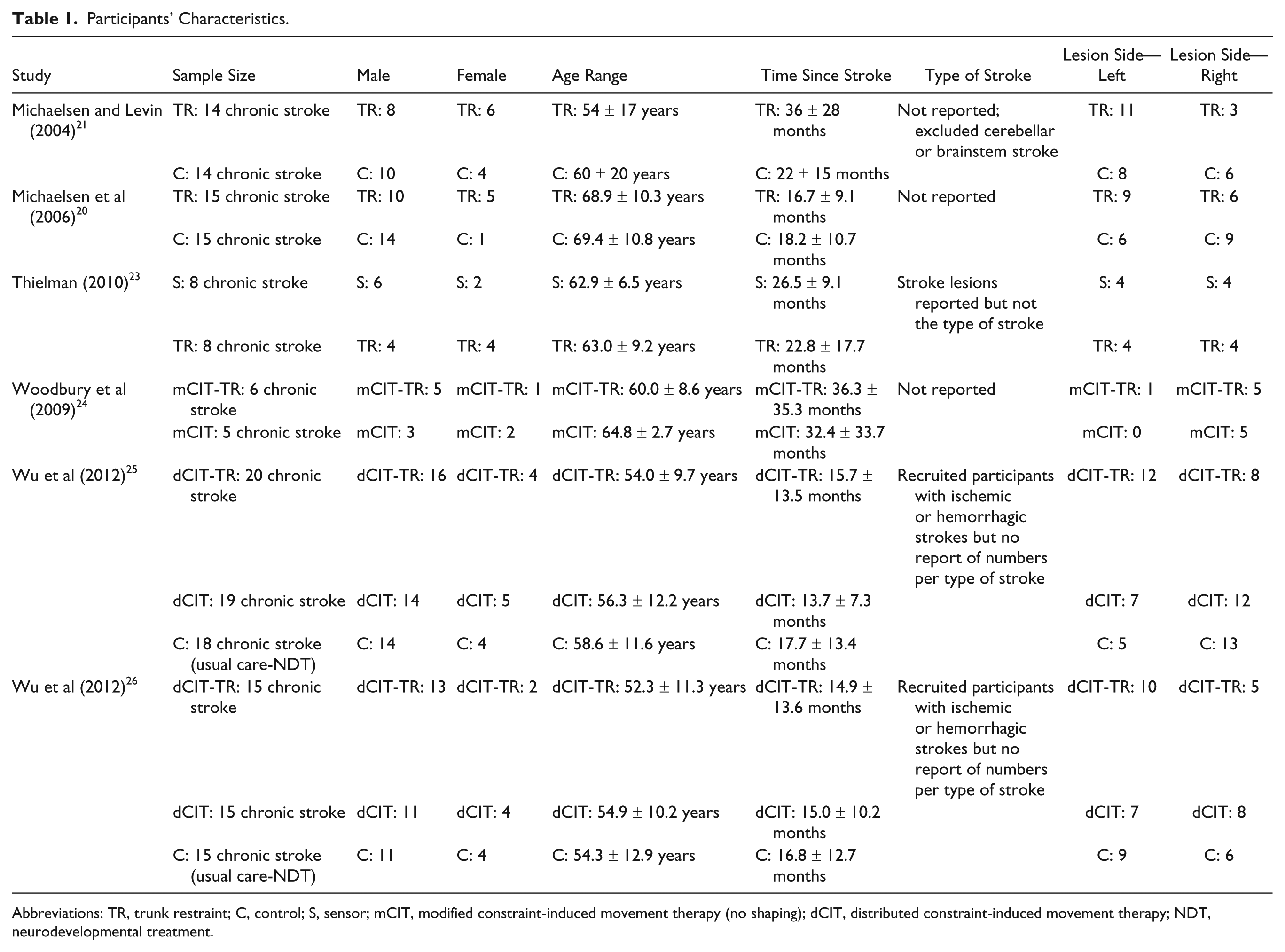
Abbreviations: TR, trunk restraint; C, control; S, sensor; mCIT, modified constraint-induced movement therapy (no shaping); dCIT, distributed constraint-induced movement therapy; NDT, neurodevelopmental treatment.
Characteristics of Studies.
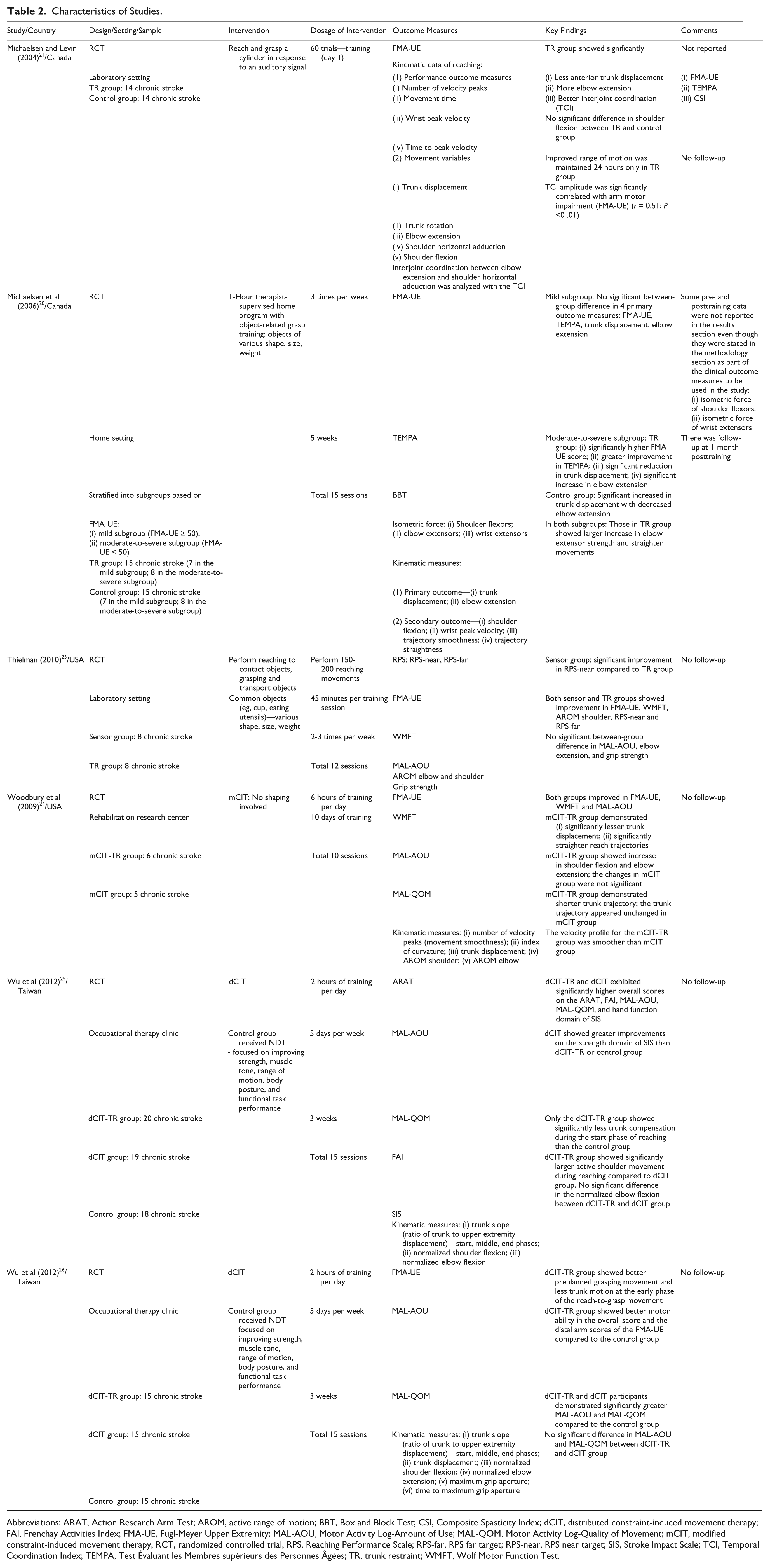
Abbreviations: ARAT, Action Research Arm Test; AROM, active range of motion; BBT, Box and Block Test; CSI, Composite Spasticity Index; dCIT, distributed constraint-induced movement therapy; FAI, Frenchay Activities Index; FMA-UE, Fugl-Meyer Upper Extremity; MAL-AOU, Motor Activity Log-Amount of Use; MAL-QOM, Motor Activity Log-Quality of Movement; mCIT, modified constraint-induced movement therapy; RCT, randomized controlled trial; RPS, Reaching Performance Scale; RPS-far, RPS far target; RPS-near, RPS near target; SIS, Stroke Impact Scale; TCI, Temporal Coordination Index; TEMPA, Test Évaluant les Membres supérieurs des Personnes Âgées; TR, trunk restraint; WMFT, Wolf Motor Function Test.
Three of the review authors independently assessed the methodological quality of the included studies using the Cochrane Risk of Bias Assessment form (Table 3). 28 Where there was disagreement between the reviewers, consensus was sought through discussion that included the fourth review author. Corresponding authors were contacted for more information that had not been, or was unclearly, reported.
Risk of Bias Assessment.
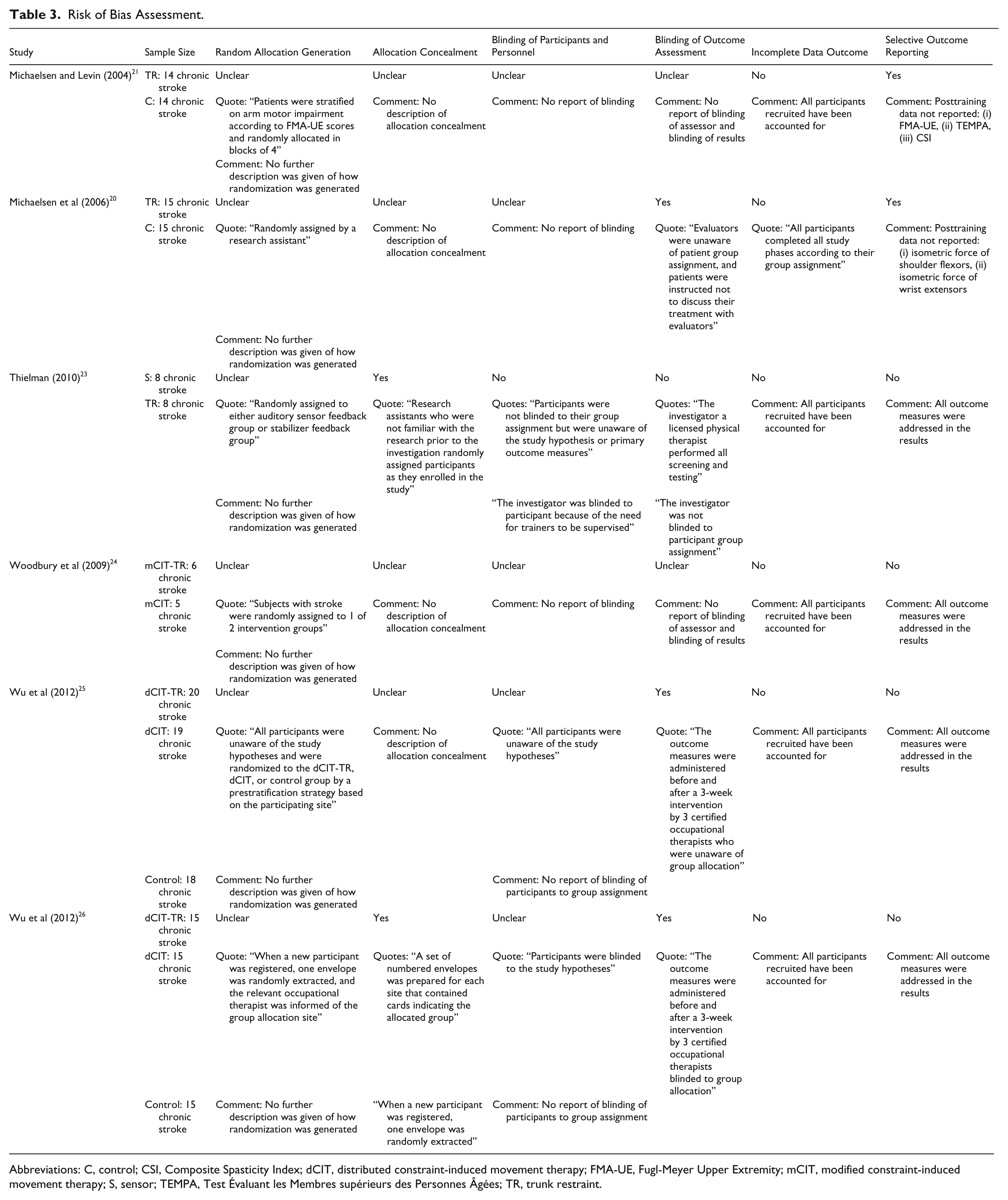
Abbreviations: C, control; CSI, Composite Spasticity Index; dCIT, distributed constraint-induced movement therapy; FMA-UE, Fugl-Meyer Upper Extremity; mCIT, modified constraint-induced movement therapy; S, sensor; TEMPA, Test Évaluant les Membres supérieurs des Personnes Âgées; TR, trunk restraint.
Quality of randomized controlled trials (RCTs) was assessed independently by the reviewers using the PEDro scale (Table 4; available online as supplementary material at http://nnr.sagepub.com/content/by/supplemental-data), 29 which uses a cutoff score of 6 points to distinguish high from low quality studies.
Data Synthesis
Each outcome measure was assessed for suitability for meta-analysis. Identical outcome measures used across the studies were pooled for analysis, and the standardized mean differences (SMD) and 95% confidence intervals (CI) were calculated. The I2 statistic was used to determine heterogeneity of the studies. If I2 was ≤50%, the fixed-effect model would be used for meta-analysis. If I2 was >50% (considered as substantial heterogeneity), the random-effect model would be used.28,30 The fixed-effect model and random-effect model with 95% CI were analyzed using the Cochrane Review Manager software RevMan 5.2 (http://ims.cochrane.org/revman/download).
Where meta-analysis was not possible due to different outcome measures being used, the effect size of individual outcome measure was calculated by using Hedges’s g, which included adjustments for small sample size.31,32 By convention, an effect size of 0.2, 0.5, 0.8, and 1.3 is considered small, medium, large, and very large, respectively. 33
Results
The study selection flow diagram is detailed in Figure 1. Eighty-eight citations were identified from all the database searches and another 39 from citation reference lists. After removal of duplicates, 30 titles and abstracts were reviewed and filtered for relevance for this systematic review. Following the filtering process, 12 full-text articles were identified and retrieved for detailed evaluation. Six articles19,22,27,34,35,36 were excluded because they did not meet the inclusion criteria (Appendix B). Six RCTs20,21,23-26 were included in the final review. All the studies scored ≥6 points on the PEDro scale, indicating high-quality studies (Table 4; available online as supplementary material at http://nnr.sagepub.com/content/by/supplemental-data).
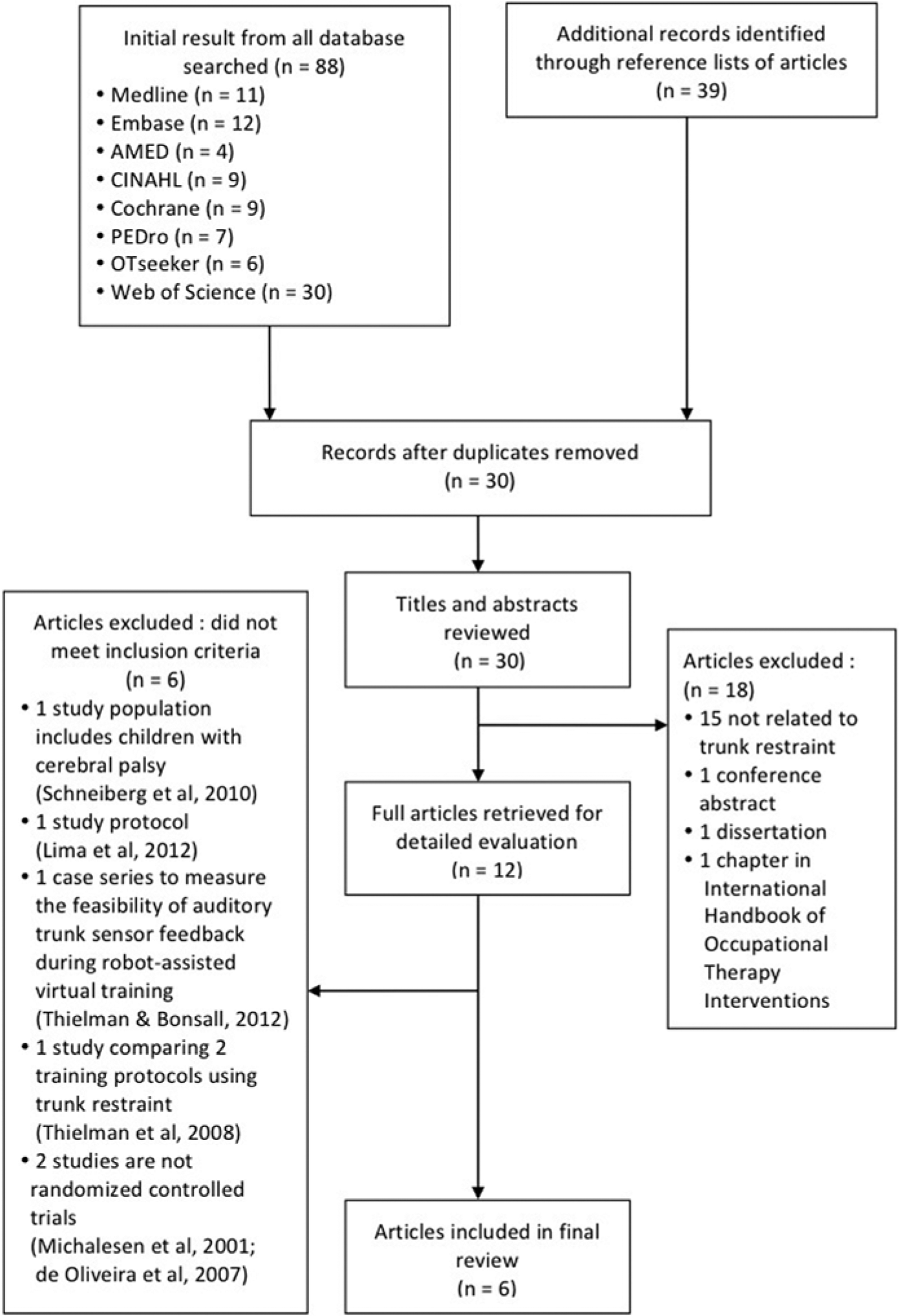
Study selection flow diagram.
The 6 studies included a total of 187 participants in the chronic phase (>6 months) of stroke (Table 1). Mean age of the participants ranged from 52.3 years to 69.4 years, with nearly equal proportion of right (49.7%) and left hemiparesis (50.3%). FMA-UE 37 score ranged from 24 to 56, that is, mild (score 51-66) to moderately severe (score 21-50). 38 There were no reports of dropouts in any of the 6 studies. Methodologies and key findings of the studies are summarized in Table 2.
Most studies used a chest harness to strap the participant to the back of chair.20,21,23,25,26 Exception were the following: Thielman 23 examined auditory feedback when the participants moved away from pressure sensor at the back of the chair, and Woodbury et al 24 who used a padded shield located anterior to the participants’ sternum to discourage anterior trunk displacement.
The training session in 1 study 21 consisted of reaching and grasping a cylinder (60 repetitions) in response to an auditory signal. In 2 studies,20,23 the training consisted of reaching and grasping objects of various sizes, shapes, and weight. The other 3 studies24-26 incorporated constraint-induced movement therapy (CIMT) in the training with trunk restraint.
Number of therapy sessions in the 6 studies ranged from 121 to 1520,25,26 and frequency either 2 or 3 times per week. Number of hours of upper extremity training ranged from 1 hour 21 to 15 hours 20 in the non-CIMT trials. In the 3 studies that incorporated CIMT, training time ranged from 30 hours25,26 to 60 hours. 24
Sixteen different impairment and function outcome measures in a variety of combinations were used in the 6 studies (Table 2). Five studies20,21,24-26 recorded trunk and upper extremity kinematics by using motion capture systems and reported 14 kinematic variables.
Five studies20,21,23,24,26 used FMA-UE to measure upper extremity impairment. Poststroke upper extremity motor function was measured with the Action Research Arm Test (ARAT), 39 Wolf Motor Function Test (WMFT), 40 Test Évaluant les Membres supérieurs des Personnes Âgées (TEMPA), 41 or Box and Block Test (BBT). 42 Motor Activity Log (MAL), which provides a functional measurement of a participant’s perception of real-world use of the affected upper extremity, was also used.24,26
Other outcome measures were the Reaching Performance Scale (RPS) 43 ; Frenchay Activity Index (FAI) 44 ; Stroke Impact Scale (SIS) 45 ; Composite Spasticity Index (CSI) 46 ; grip strength via dynamometry 47 ; isometric force of shoulder flexors, elbow extensors, wrist extensors; and active range of motion of elbow and shoulder via goniometry. 48 CSI and the strength items were not analyzed due to incomplete data reporting. There was no follow-up assessment of participants in 5 studies.21,23-26
Risk of Bias in the Included Studies
The assessment of risk of bias and methodological quality across the 6 studies are presented in Table 3.
Meta-Analysis
Out of the 16 clinical outcome measures and 14 kinematic measures, only the following measures were common to at least 2 studies and therefore appropriate for meta-analysis: FMA-UE, trunk displacement, shoulder flexion, elbow extension, reaching trajectory smoothness, reaching trajectory straightness, and MAL. In the 2 studies on CIMT,25,26 meta-analysis was made between the CIMT group with trunk restraint and the CIMT group without trunk restraint.
As for the other outcome measures, their effect sizes were calculated using Hedges’s g. Results are summarized in Tables 5 and 6 (available online as supplementary material at http://nnr.sagepub.com/content/by/supplemental-data).
The meta-analysis of FMA-UE pooled data from 3 studies,20,24,26 with a total of 36 participants in the trunk restraint group and 35 in the control group. Results showed that trunk restraint had a moderate significant effect on FMA-UE in favor of the trunk restraint group (SMD 0.54; 95% CI = 0.06 to 1.01; P = 0.03; I2 = 0%, fixed-effect model; Figure 2). This implied that these chronic stroke participants had demonstrated improvement in their upper extremity impairment after training with trunk restraint.
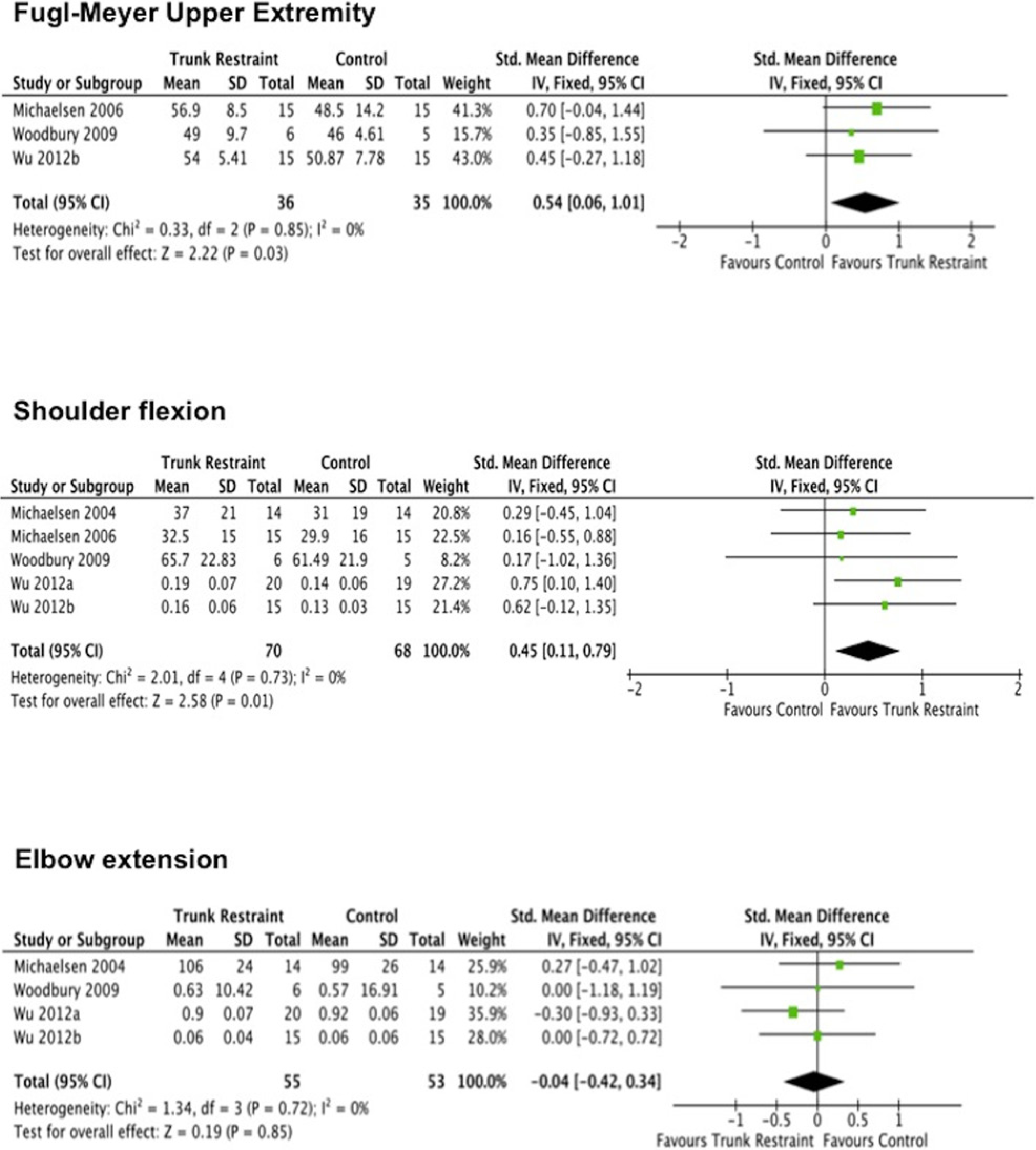
Forest plot for the effect of trunk restraint on Fugl-Meyer Upper Extremity score, shoulder flexion, and elbow extension.
Five studies20,21,24-26 were included in the pooled analysis for shoulder flexion outcome, with a total of 70 participants in the trunk restraint group and 68 in the control group. Results from the meta-analysis showed that trunk restraint had a moderate significant effect on improving active shoulder flexion, in favor of the trunk restraint group (SMD = 0.45; 95% CI = 0.11 to 0.79; P = 0.01; I2 = 0%, fixed-effect model; Figure 2).
Four studies21,24-26 were included in the meta-analysis for elbow extension outcome, with a total of 55 participants in the trunk restraint group and 53 in the control group. Results showed that trunk restraint did not have a significant effect on improving active elbow extension in the chronic stroke participants (SMD = −0.04; 95% CI = −0.42 to 0.34; P = 0.85; I2 = 0%, fixed-effect model; Figure 2).
Summary results of the effect size for ARAT, WMFT, TEMPA, BBT, FAI, and SIS are presented in Table 6 (available online as supplementary material at http://nnr.sagepub.com/content/by/supplemental-data). There was a small effect size ranging from −0.39 to 0.35, in favor of trunk restraint.
The meta-analysis results for the MAL-Amount of Use (MAL-AOU) and the MAL-Quality of Movement (MAL-QOM) are reported in Figure 3. Pooled analyses of both demonstrated that the trunk restraint did not have a significant effect on improving MAL-AOU (SMD = −0.12; P = 0.58) and MAL-QOM (SMD = −0.15; P = 0.50) in the chronic stroke participants.
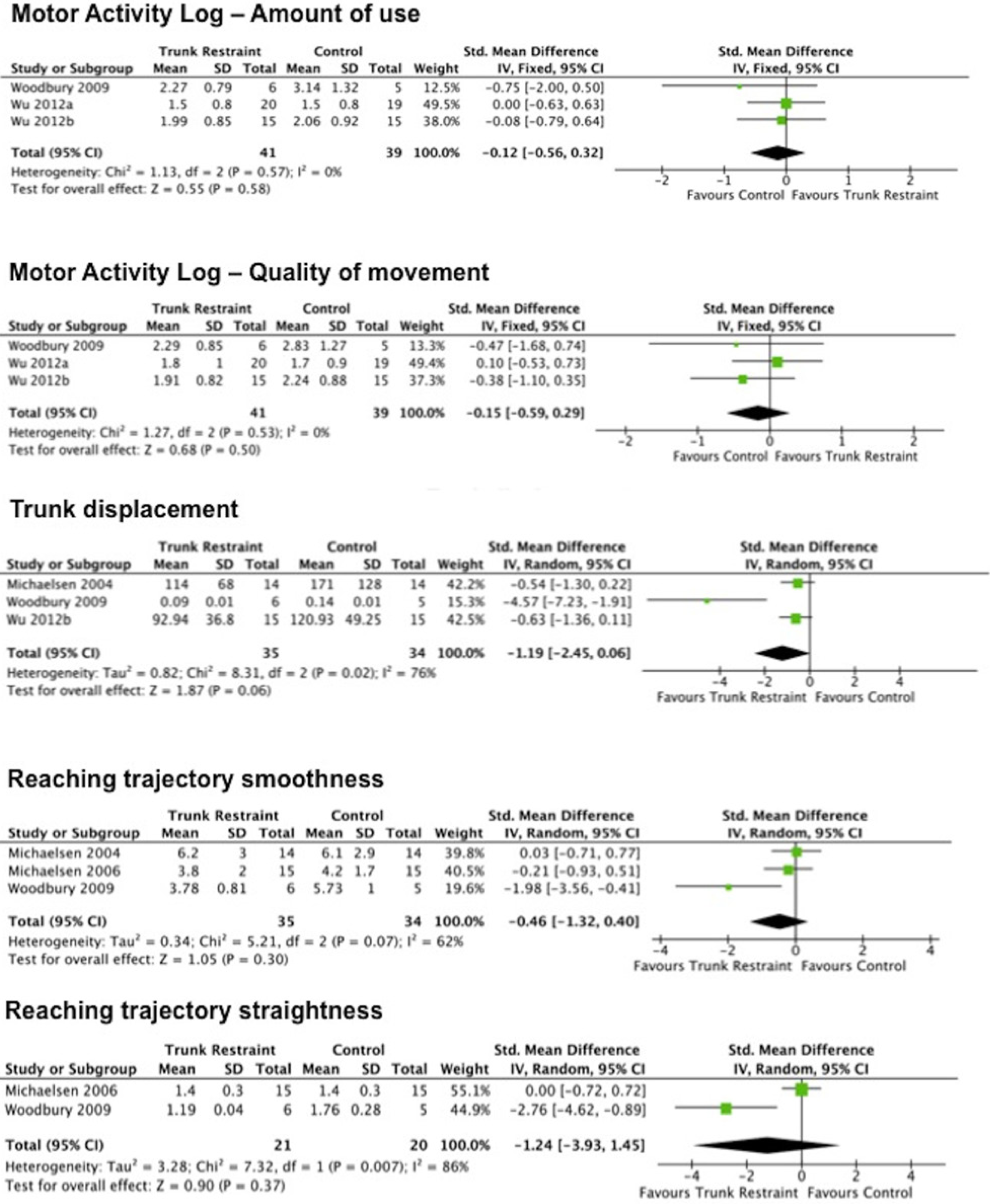
Forest plot for the effect of trunk restraint on Motor Activity Log-Amount of use, Motor Activity Log-Quality of movement, trunk displacement, reaching trajectory smoothness, and reaching trajectory straightness.
The meta-analysis of trunk displacement pooled data from 3 studies,21,24,26 with a total of 35 participants in the trunk restraint group and 34 in the control group. Results showed that trunk restraint had a large effect on the amount of trunk displacement in favor of the trunk restraint group (SMD = −1.19; 95% CI = −2.45 to 0.06; P = 0.06; I2 = 76%, random-effect model; Figure 3). There was a trend toward a significant effect for improvement in the amount of trunk displacement (P = 0.06), favoring the trunk restraint group. However, there was substantial heterogeneity among the studies (I2 = 76%).
The meta-analysis demonstrated that the trunk restraint had a moderate nonsignificant effect on trajectory smoothness (SMD = −0.46; 95% CI = −1.32 to 0.40; P = 0.30) and a large nonsignificant effect on trajectory straightness (SMD = −1.24; 95% CI = −3.93 to 1.45; P = 0.37), both in favor of the trunk restraint group (Figure 3).
Training Effects Based on the Severity of Upper Extremity Motor Impairment Level
One study 20 divided the participants into a subgroup (n = 7 in trunk restraint group; n = 7 in control group) with mild upper extremity impairment (FMA-UE ≥ 50) and another subgroup (n = 8 in trunk restraint group; n = 8 in control group) with moderate-to-severe impairment (FMA-UE < 50). Analysis of the mild impairment subgroup showed no significant difference between the trunk restraint and control groups in 4 primary outcome measures, namely, FMA-UE, TEMPA, trunk displacement, and elbow extension.
In the moderate-to-severe impairment subgroup, the gains in FMA-UE were significantly larger (effect size = 0.68; P < 0.001) in the trunk restraint group compared with the control group. Those participants in the trunk restraint group had higher TEMPA scores than control group but this result did not reach significance (effect size = 0.26; P < 0.07). Reduction in trunk displacement was significantly larger (effect size = −0.93; P < 0.003) in the trunk restraint group. There was also significantly more (effect size = 1.22; P < 0.04) elbow extension in the trunk restraint group compared with the control group.
The control group (which received task-specific training without trunk restraint) within the moderate-to-severe impairment subgroup exhibited significantly increased trunk displacement (P < 0.05) and decreased elbow extension posttraining.
Discussion
Upper Extremity Impairments
Meta-analysis revealed that trunk restraint had a moderate significant effect on FMA-UE and shoulder flexion, in favor of the trunk restraint group. The SMDs of 0.54 and 0.45, respectively, implied medium effect size. 33 Trunk restraint did not however have a statistically significant effect on elbow extension, although Michaelsen et al 20 reported improvements in elbow extension with trunk restraint and a large effect size (0.98 at posttraining; 1.40 at 1-month follow-up). Their results should be interpreted with caution due to small sample size in the trunk restraint group and control group (n = 15 per group). Consistent with our meta-analysis, Malcolm et al 49 demonstrated that shoulder flexion was more amenable to change than elbow extension. The difference between effect on shoulder and elbow movement can be explained by factors unrelated to trunk control or proximal weakness and consequently not improved by trunk restraint. For example, reaching may be impaired by abnormal elbow flexor synergy patterns comprising excessive coactivation between elbow flexors and elbow extensors with activation of shoulder abductors and the resultant joint torque coupling of shoulder abduction with elbow flexion, 50 or spasticity of the biceps. 22 Ellis et al 50 showed that abnormal torque coupling dramatically reduced reaching range of motion when stroke patients were required to lift their upper extremity against gravity and reach outward which further supports this thesis.
Trunk restraint constrains shoulder girdle and trunk movements and minimizes the components of the scapular protraction and elevation synergy. This reduces the opportunity for the individual to perform reaching tasks using abnormal movement synergies. Thus, trunk restraint may encourage more normal upper extremity synergies, that is, shoulder flexion and elbow extension, during reaching. In contrast, CIMT has been shown in recent studies51,52 to promote the use of compensatory strategies rather than the recovery of more normal movement patterns, demonstrating improved functional outcome scores (ARAT 51 and WMFT 52 ), despite increased compensatory shoulder abduction 52 (kinematic measures) and no meaningful improvements in upper extremity impairment (FMA-UE). 51 However, other studies24-26 showed improvement in impairment-level outcome measures, such as reduced compensatory trunk displacement, more direct reach trajectories, as well as improved functional arm ability when trunk restraint was incorporated into CIMT training compared with CIMT only training. These findings suggest that the use of trunk restraint during therapy may help “unmask” latent potential recovery of upper extremity movement.
Trial and error is a key component of motor learning and involves using sensory feedback to correct “errors” that compromise goal achievement. 53 Trunk restraint not only removes the “error” of abnormal trunk movement, “forcing” utilization of available upper extremity joint range, but also provides an afferent cue when the individual leans forward. Initially, this may be a cognitive decision but with practice may become an automatic response and with high intensity, repetition and task-specificity may facilitate cortical reorganization54,55 and hence neuroplasticity.56,57 Therefore, learning how to control and stabilize the trunk during training may explain reduction in compensatory trunk movement. Pooled analysis in this review showed that trunk restraint had a large effect on trunk displacement.
Upper Extremity Function
Overall, there was small effect of trunk restraint on upper extremity function. The difference in magnitude of effect size between the upper extremity function outcome measures may be related to differences in responsiveness, consistency, and precision between tests. 58
The overall finding of small effect size of trunk restraint on upper extremity function is not surprising. The trunk restraint is an external device that minimizes compensatory trunk movements, with the aim of improving amount and quality of upper extremity movement during training. The outcome of upper extremity function is mainly dependent on the type of therapeutic intervention rather than on the trunk restraint. Hand dexterity is a fundamental skill in performing ADL and occupational tasks, 59 and dexterity has been demonstrated to correlate with upper extremity function. 60 Therefore, the upper extremity functional outcome is also dependent on the amount of hand dexterity training provided to patients.
In this review, 3 studies20,21,23 involved reaching practice while the other 3 studies24-26 incorporated CIMT. The nature and intensity of therapy therefore differs across the studies. Intensity of therapy has been shown to impact on functional outcome; evidence suggests that higher intensity therapy results in better functional outcome.61,-63 This may account for the difference in outcome of upper extremity function in the 6 studies.
Studies have highlighted that it is the improvement of upper extremity function that matters to stroke patients.64,65 Perception of the recovery of upper extremity function was linked to the self-reported outcome measures. With the small effect size of trunk restraint on upper extremity function, it was not an unexpected result that trunk restraint had no significant effect on MAL-AOU, MAL-QOM, FAI, and SIS.
Reaching Kinematics
There was a moderate to large nonsignificant effect of trunk restraint on the reaching trajectory smoothness and trajectory straightness, and substantial heterogeneity among the studies analyzed (I2 = 62% and 86%, respectively). The computations of reaching trajectory smoothness and straightness were similar in all 3 studies.20,21,24 Trajectory smoothness was determined by the number of peaks in the velocity profile during reaching. Trajectory straightness was determined by the index of curvature, which is the ratio of actual end point path to a straight line. However, the experimental protocols to determine these variables were different. Two studies20,21 required that participants reached and grasped a cylinder placed in midline at xiphoid level, while participants in another study 24 performed reaching with the tip of the index finger to touch a 15-mm target at shoulder height and in-line with the knee on the hemiparetic side. In addition, the mean age of participants and time since stroke onset were different in all the 3 studies20,21,24 (Table 1). Dutta et al 66 found that diminished joint coordination in the elderly individuals led to more variable hand paths compared with young adults. These factors may account for the heterogeneity among the studies.
Effect of Trunk Restraint Based on the Severity of Upper Extremity Motor Impairment Level
Unsurprisingly, trunk restraint was not beneficial for mildly impaired stroke patients 20 ; they may not exhibit excessive trunk movement in reaching. For the moderate-to-severe impairment group, the trunk restraint was beneficial in improving the upper extremity movement at both the impairment level and at the functional level. Restriction of compensatory trunk movements may encourage the recovery of more “normal” reaching patterns. 22 Interestingly, the control group exhibited increased compensatory trunk movement and decreased elbow extension with unrestricted practice. This supports the idea that compensations may be maladaptive because they lead to nonoptimal movement patterns, which hinders further improvement and potential recovery of the upper extremity. 20
Limitations of the Included Studies
The limitations of these 6 trunk restraint studies include small sample size (n = 5-20), homogenous population (only chronic stroke patients with mild to moderately severe level of upper extremity impairment), and lack of longer-term follow-up. These limitations affect the generalizability of the results. The effect of trunk restraint on stroke individuals with severely impaired upper extremity remains unknown.
Quality of the Evidence
All the studies in this review were classified as high-quality studies (PEDro ≥ 6 points). However, it is also equally important to weigh the methodological quality of the studies based on the assessment of risk of bias (Figures 2 and 3 and Table 3).
Randomization was carried out in all 6 studies. Selection bias may occur due to a lack of random sequence generation67,68 in all the studies and a high proportion of unclear risk of bias in allocation concealment (66.7%).
Performance and detection bias may occur due to poor blinding. Blinding of participants and personnel were not explicitly reported in 83.3% of the studies. Blinding of outcome assessors occurred in only 50% of the studies. One third of the studies20,21 exhibited reporting bias due to no reports of key outcome measures related to impairment and functional levels.
In summary, there is a moderate degree of confidence in the results of this review due to moderate quality of the studies.
Limitations of This Review
A comprehensive search strategy was conducted to identify relevant published studies for this review. However, as only publications in English were considered, additional studies in other languages were excluded, potentially introducing bias.
The studies used a wide range of outcome measures. A meta-analysis for all the outcome measures could not be conducted due to insufficient data reported and the poor response rate from some corresponding authors when requests for information were made by the review authors. We acknowledged that all the 6 RCTs have small sample size (n = 5-20), and inclusion of small trials that are underpowered may affect the validity of the results in meta-analysis. Turner et al 69 cautioned that small studies included in a meta-analysis tend to show more extreme treatment effects than larger studies.
Implications for Clinical Practice
Following stroke, the continual utilization of excessive compensatory trunk movements during reaching may lead to abnormal upper extremity movement, which may inhibit recovery in the longer term. The trunk compensatory strategy may reflect a habitual response of the central nervous system when there was insufficient motor control and/or strength to perform the task more efficiently, especially in the acute phase of stroke recovery. 70 Undesirable habits formed in the early phase poststroke will be more difficult to modify and unlearn. 17 In addition, excessive use of compensatory movements can result in secondary complications such as muscle contractures, joint misalignment, pain, limb disuse, and increased energy expenditure.16-18 These complications can affect the execution of more efficient movement patterns of the upper extremity and impede its longer-term functional recovery.
This review suggests that trunk restraint is a promising adjunct to incorporate into the upper extremity rehabilitation program as it demonstrates moderate effect in improving upper extremity movement and aids the reduction of compensatory trunk movements during reaching. With the use of trunk restraint as a cue, the knowledge of results (KR) and knowledge of performance (KP), with regard to excessive trunk movement, are made available to the individual. KR and KP are essential and critical elements for motor learning.71,72 The combined KR and KP feedback provides the individual with the opportunity to engage in an implicit learning process of discovering an alternative motor strategy that enables successful completion of the task. 24
The evidence from this review suggests that the most appropriate trunk restraint technique (chest harness or auditory feedback device 23 ) may depend on the level of trunk control poststroke. For those individuals with poor trunk control, a chest harness may be more suitable during rehabilitation. As the trunk control improves, progression to an auditory feedback device may be considered. This is supported by findings that a training protocol of progressive fading of visual and verbal feedback was more effective in promoting motor learning than one that provides constant feedback.18,73 In addition, training with an auditory feedback device requires the stroke patient to participate more actively to minimize compensatory trunk movements compared with the reliance on a trunk restraint. Thielman 23 had demonstrated that stroke patients in the auditory feedback group improved significantly more on reaching ability than the trunk restraint group. This is consistent with findings of other studies that active motor training is more effective than passive motor training in eliciting performance improvements74,75 and cortical reorganization. 75 These results highlight the pivotal role of voluntary drive in motor learning.
Future Research
Age is a variable that can affect motor learning and adaptation. 76 The mean age of the participants in the included studies ranged from 52.3 years to 69.4 years. It is unknown whether trunk restraint will have a different effect on younger stroke individuals (below 50 years old) versus those who are older (above 70 years old). Thus, research on the effect of trunk restraint on stroke individuals from different age group, at different phase of stroke recovery, and with different levels of upper extremity impairment is recommended.
Finally, there are no published studies on the effect of trunk restraint on the trunk and upper extremity of individuals with trunk ataxia due to neurological disorders such as cerebellar stroke or brainstem stroke. Gaining an understanding of the underlying mechanisms of how trunk restraint works, in terms of improving trunk stabilization for this group of individuals, may provide insights into a new therapeutic approach for the management of trunk ataxia and upper extremity in neurorehabilitation.
Conclusion
Trunk restraint has a moderate effect on reduction of upper extremity impairment in chronic stroke patients, in terms of FMA-UE score, increased shoulder flexion, and reduction in excessive trunk movement during reaching. There is insufficient evidence to support that trunk restraint improves upper extremity function and reaching trajectory smoothness and straightness in chronic stroke patients. Future research on a larger sample of stroke individuals at different phases of recovery and with different levels of upper extremity impairment is recommended. There is also a need for longer-term follow-up to examine the retention of treatment effects.
Footnotes
Appendix A
Appendix B
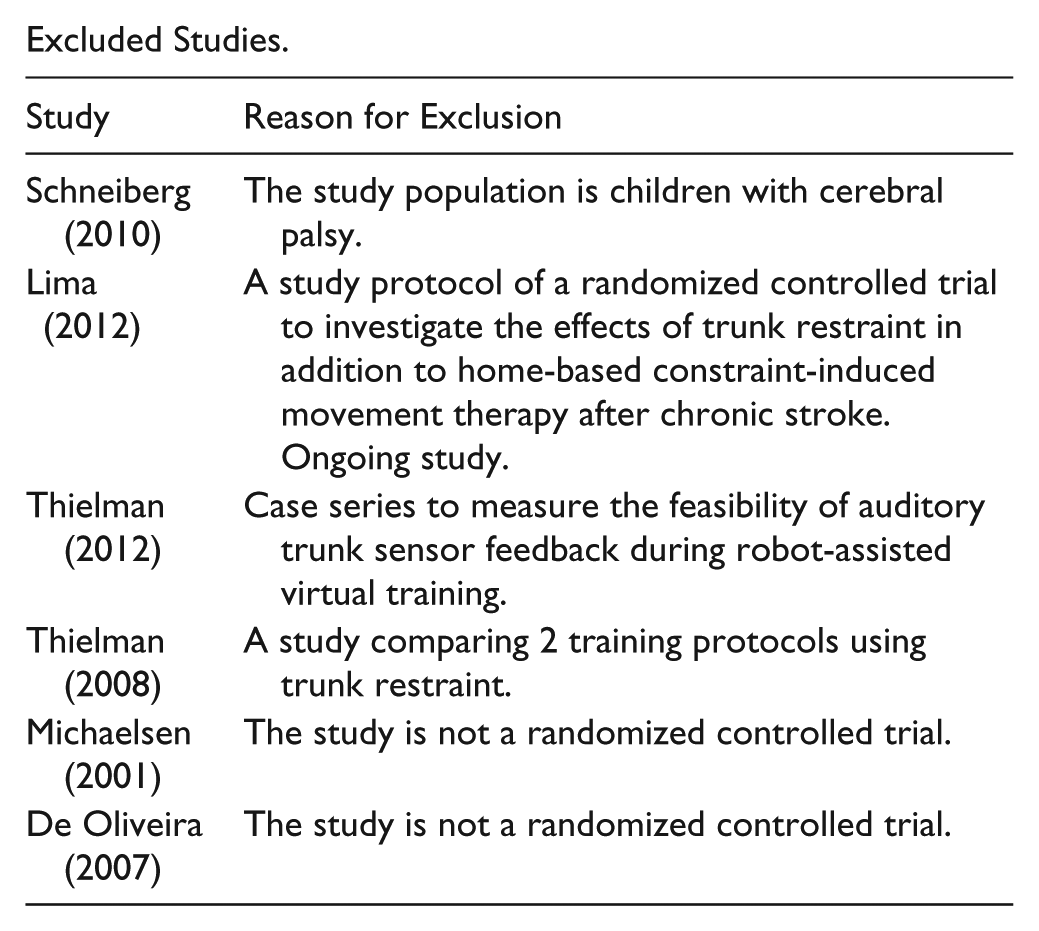
Excluded Studies.
| Study | Reason for Exclusion |
|---|---|
| Schneiberg (2010) | The study population is children with cerebral palsy. |
| Lima (2012) | A study protocol of a randomized controlled trial to investigate the effects of trunk restraint in addition to home-based constraint-induced movement therapy after chronic stroke. Ongoing study. |
| Thielman (2012) | Case series to measure the feasibility of auditory trunk sensor feedback during robot-assisted virtual training. |
| Thielman (2008) | A study comparing 2 training protocols using trunk restraint. |
| Michaelsen (2001) | The study is not a randomized controlled trial. |
| De Oliveira (2007) | The study is not a randomized controlled trial. |
Acknowledgements
We wish to thank Dr Sean Ewings, statistician of the Southampton Statistical Sciences Research Institute, University of Southampton, United Kingdom, for his kind assistance and constructive advice on statistical analysis for this systematic review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Seng Kwee Wee would like to acknowledge Tan Tock Seng Hospital, Singapore, for funding his PhD study at the University of Southampton, United Kingdom.