
Abstract
Background. Constraint-induced therapy (CIT) is effective in improving upper extremity motor function, but evidence is lacking about effectiveness grasp and trunk control. Objective. This study investigated whether distributed CIT combined with trunk restraint (dCIT + TR) benefited movement kinematics of grasping and the trunk, as well as motor ability of the upper extremity, more than dCIT alone. Methods. A total of 45 stroke participants received 2 hours of dCIT + TR, dCIT, or the dose-matched control intervention for 3 weeks. Movement kinematics, motor ability, and daily function were the outcome measures. Movement kinematics included grasping, joint range, and trunk movement at various phases of reach-to-grasp tasks. Motor ability and daily function of all participants were evaluated using the Fugl-Meyer Assessment and the Motor Activity Log. Results. Four to 5 participants in each group were not included for kinematic analysis because of their inability to grasp a can. The dCIT + TR group showed better preplanned grasping movement and less trunk motion at the early phase of the reach-to-grasp movements than the dCIT or control groups. Compared with the controls, the dCIT + TR participants showed better motor ability in the overall and distal arm scores of the Fugl-Meyer Assessment. The dCIT + TR and dCIT participants demonstrated significantly greater functional use of the affected arm. Conclusions. Administering dCIT + TR produced additional benefits by improving grasping control and reversing the compensatory trunk movement at the early phase of a reach-to-grasp movement. The use of experimental tasks beyond and within arm’s length might improve our understanding of optimal upper extremity rehabilitation.
Keywords
Introduction
Studies on constraint-induced therapy (CIT)1,2 and its less intensive derivatives3-6 found improved motor ability and functional use of the affected upper extremity (UE) in patients with residual motor control of the wrist and finger extensors in hemiparetic subjects after stroke. Participants demonstrated greater gains in the distal compared with the proximal affected UE,4-6 as measured by the Fugl-Meyer Assessment (FMA). However, gains in distal motor ability did not reflect improvement in the control strategy of movements such as grasping. 3 In addition, CIT may not reduce the compensatory strategy of trunk movement during reaching. 1 The absence of changes in these control strategies points out the need to develop CIT further if the goal is to restore more normative control strategies. 1
Patients after stroke often recruit an additional degree of freedom from the trunk to assist reach-to-grasp movements.7-10 Compensatory truncal movements may improve with practice that restricts excessive trunk motion during the UE movement. Trunk restraint may induce better coordination of the arm joints, reduce additional trunk movement, and improve the movement pattern of the affected arm.7,10-12 Woodbury et al 13 combined CIT with trunk restraint and found better reaching control (straighter hand paths), improved coordination of shoulder–elbow joints, and less trunk motion than with CIT alone. No studies on trunk restraint7,10-12 and CIT combined with trunk restraint 13 have explored the possible changes in grasping after the intervention, although most of them used reach-to-grasp movements as training tasks. Changes in the reaching component might affect grasp. 14 In addition, Levin et al 8 showed that the relative amount of the trunk recruited by patients after stroke is greater in the first third of the reach-to-grasp movement.
The present study compares the effects of distributed CIT (dCIT) combined with trunk restraint (dCIT + TR) versus dCIT alone on the control mechanisms of grasping and trunk movements, as well as on motor ability and UE function. We hypothesized that participants who received dCIT + TR would exhibit better grasping control, less trunk compensation at the beginning of the reach-to-grasp movement, and improved motor ability and daily function than those who received dCIT, and that these participants, in turn, would demonstrate better performance than the control group. Kinematic analysis, which is a valid measure of control strategy and movement quality,15,16 was used to investigate the control mechanisms of reach-to-grasp movements.
Methods
Participants
The study recruited 45 participants (35 men) from the rehabilitation departments of 4 hospitals. The individuals, right-hand dominant before their ischemic or hemorrhagic stroke by self-report, had a mean age of 53.8 ± 11.3 years, and a mean time of 15.5 ± 11.9 months (range, 6-59 months) post onset. All the community-dwelling participants signed informed consent forms approved by the institutional review boards.
Inclusion criteria were (a) clinical diagnosis of a first or recurrent unilateral stroke; (b) ability to reach Brunnstrom stage III or above in the proximal and distal part of the UE; (c) considerable nonuse of the affected arm (Motor Activity Log [MAL] amount of use [AOU] average score <2.5); (d) no serious cognitive deficits (Mini-Mental State Examination score ≥24); (e) no excessive UE spasticity (Modified Ashworth Scale score ≤2) in any joint; (f) no balance problems sufficient to compromise safety when wearing the experimental constraint device; (g) no other neurologic, neuromuscular, or orthopedic disease; and (h) no participation in any experimental rehabilitation or drug studies.
Design
This study used a randomized pretest and posttest control group design (Figure 1). Participants, who were blinded to the study hypotheses, were randomized to the dCIT + TR, dCIT, or control group. A prestratification strategy based on participating hospital was applied. A set of numbered envelopes was prepared for each site that contained cards indicating the allocated group. When a new participant was registered, one envelope was randomly extracted, and the relevant occupational therapist was informed of the group allocation. The intervention took place in the occupational therapy clinic, and all other routine stroke rehabilitation, including physical therapy or speech therapy, proceeded as usual. The outcome measures were administered before and after a 3-week intervention by 3 trained occupational therapists blinded to group allocation.
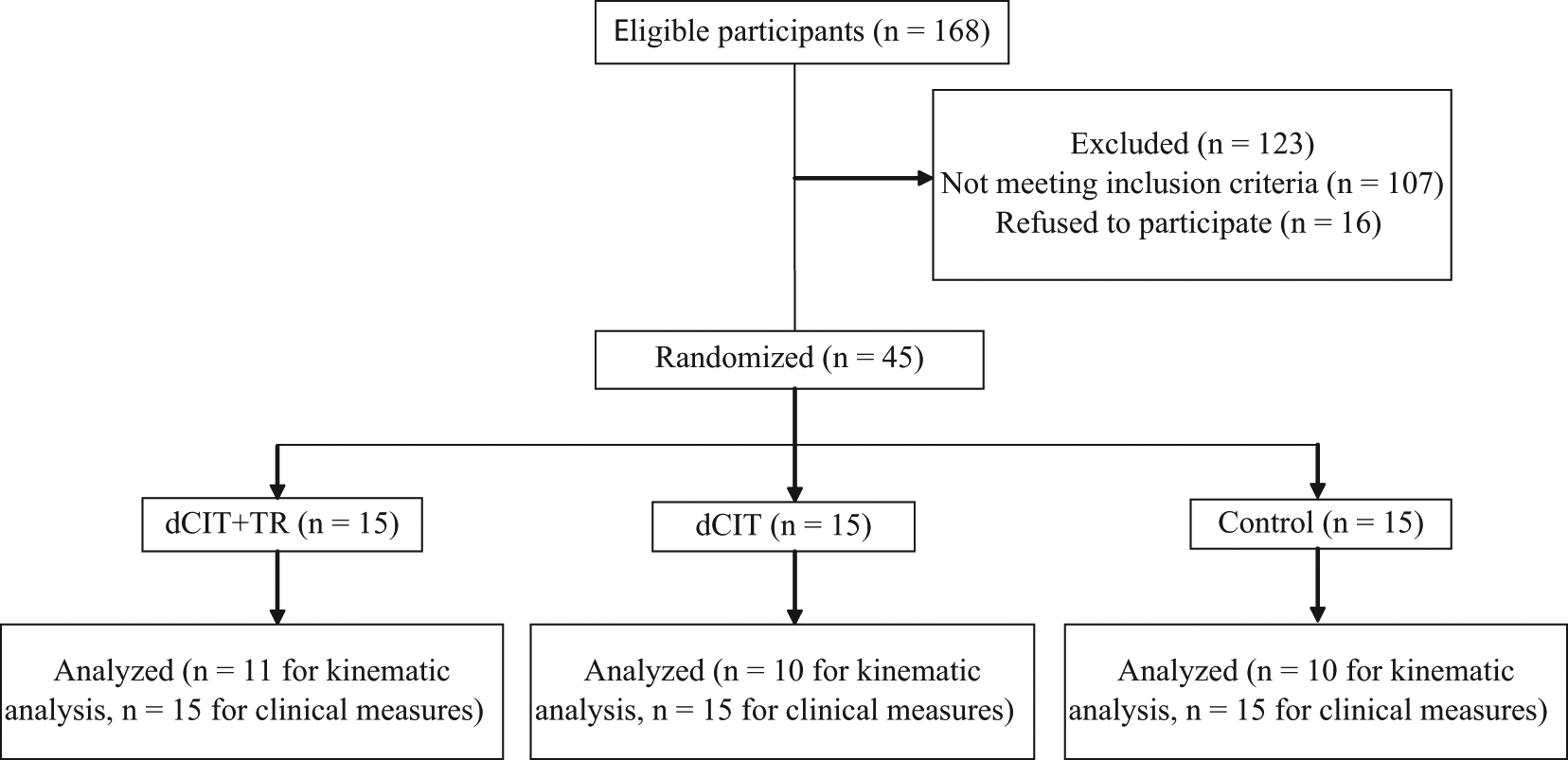
Flow diagram showing the randomization procedure. Abbreviations: dCIT, distributed constraint-induced therapy; TR, trunk restraint.
Intervention
One-to-one treatments were designed, and all groups received treatment of equal intensity (2 h/d, 5 d/wk, for 3 consecutive weeks). The treating therapists were trained in the administration of these 3 protocols by the investigators to provide consistent intervention protocols. The targets used in the training tasks in the 3 groups were placed inside the individual’s reachable workspace.
The dCIT + TR group
Participants in this group focused on the intensive training of the affected arm in functional activities with behavioral shaping and combination with trunk restraint. The functional tasks included, for example, flipping pages of magazines and picking up coins. The shaping skills involved individualized task selection, graded task difficulty (eg, practicing deficient parts of the selected activity and then performing the entire activity), verbal feedback, prompting, physical assistance with movements, and modeling. To limit trunk movement when sitting, participants wore a harness that was secured to the chair back by Velcro straps and adjusted to allow for arm movement (Figure 2A). Participants were also required to place their unaffected hand and wrist in a mitt for 6 hours a day during the 3-week period and documented mitt compliance in daily logs.

(A) The intervention setup of dCIT + TR group. (B) The setup for kinematic tests. Seated participants were asked to reach and grasp a cylindrical can using their affected arm with self-paced speed. Abbreviations: dCIT, distributed constraint-induced therapy; TR, trunk restraint.
The dCIT group
The dCIT group participants received an intervention protocol that resembled the dCIT + TR intervention, except for the lack of trunk restraint.
The control intervention group
The control group primarily employed neurodevelopmental treatment techniques and focused on improving strength, muscle tone, range of motion, body posture, and functional task performance. Participants used the affected arm, or both arms with the unaffected arm assisting the affected arm, for performing unilateral or bilateral functional activities. The control intervention was considered as the baseline treatment and allowed us to estimate if specific intensive treatments, such as dCIT and dCIT + TR, would confer greater treatment benefits for participants with hemiparesis after stroke than the intervention usually used in the clinics.
Primary Outcome Measures: Kinematic Analysis
The experimental task used in the kinematic analysis was reaching to grasp a can (5.3 cm in diameter and 10.5 cm in height; Figure 2B) along the participants’ midsagittal plane. The reach-to-grasp task was suggested to be a sensitive task item representing motor improvement of the affected arm. 17 We measured the arm’s length as the distance from the acromion to the third fingertip and standardized the task distances to 90% and 125% of this distance to explore the trunk compensation in different task demands. During the tasks, the participant sat without trunk restraint on a height-adjustable chair with the seat height set to 100% of the lower leg length, measured from the lateral knee joint to the floor. Adjacent to the chair was a table with a height adjusted to 5 cm below the elbow while the participant sat on the chair. The participant’s affected hand was initially positioned on the edge of the table with elbow flexion at 90°.
After a practice trial, 3 data-producing trials with self-paced speed were performed. A 7-camera motion analysis system (VICON MX; Oxford Metrics Inc, Oxford, UK) was used with a personal computer to capture the movement of the reference markers. Reference markers were placed on the seventh cervical vertebra (C7), the fourth thoracic vertebra (T4), midsternum, the bilateral clavicles, and the affected side of acromion, middle of humerus, lateral epicondyle, styloid process of the ulna and radius, thumb nail, and index nail. Movements were recorded at 120 Hz and digitally low-pass filtered at 5 Hz using a second-order dual-pass Butterworth filter. Movement onset and offset were defined for each trial using the time at which the tangential wrist velocity rose 5% above and fell 5% below its peak value for 3 consecutive samples based on the rules used in the previous studies.9,18
Data reduction for kinematic variables
Kinematic variables were chosen to indicate the control strategy and movement quality for grasping, joint range of the UE (the shoulder and elbow joints), and trunk movement.
The variables of the grasping component were maximum grip aperture (MGA) and the percentage of time to maximum grip aperture (TMGA), which represent the control strategy of grasping. The MGA was calculated as the maximum distance between the markers on the thumb and index nails, representing the extent of hand opening. A skillful grasping movement normally is made without widely opening the hand. The TMGA, reflecting where the MGA occurs in a percentage of movement time, is an indicator of online grasping correction during enclosure. A high TMGA amplitude refers to a low percentage of time contributing to online correction and indicates a well preplanned grasp. 19
The joint range included the active angular change of shoulder and elbow joints, defined as the difference in degrees from the beginning to the end of the movement. Because the task distance varied across participants, the angular changes of shoulder and elbow joints were normalized to correct for variations in task distance; that is, the angular change was divided by the task distance measured in millimeters.
The slope value represents the ratio of trunk/UE movement of which the displacement in the sagittal plane was obtained. The slope indicates the contribution of trunk motion to the total end point motion. The slope was calculated separately in 3 parts (the start, middle, and the end phase of reach-to-grasp motion) to probe the particular contributed proportion between the UE and trunk. The slope was zero if all of the movement was due to trunk motion and infinite if the trunk did not contribute to the end point movement. 8 The negative value of the slope shows that the trunk moved backward while the UE still reached forward during the reach-to-grasp phase.
Secondary Outcome Measures: Clinical Measures
The clinical measures included the FMA and the MAL. The UE part of the FMA 20 assesses several dimensions of motor impairment, including movements of the proximal (shoulder, elbow, and forearm) and distal (wrist and hand) structures.21-23 The MAL is a semistructured interview that obtains information about how participants use their affected limbs during 30 important daily activities and assesses the AOU and the quality of movement (QOM) of the affected arm.24-27
Data Analysis
The χ2 test and the analysis of variance test were used to determine comparability at baseline characteristics of participants. Analysis of covariance was used to compare the relative effects of the treatment on participants for each variable. The pretest score was the covariate, the group was the independent variable, and the posttest score was the dependent variable. Post hoc analysis was performed based on significant group effects by the least significant difference test. To index the magnitude of group differences in performance, η2 = SSb/SStotal was calculated for each outcome variable. 28 A large effect is represented by a η2 of at least .138, a moderate effect by a η2 of .059, and a small effect by a η2 of .01. 29
Results
Characteristics of Participants
All demographic and clinical characteristics at baseline were comparable among the participants in the 3 groups (Table 1). There were no preexisting significant differences between the 3 groups on any of the outcome measures (P = .529 to .938).
Demographic and Clinical Characteristics of Study Participants
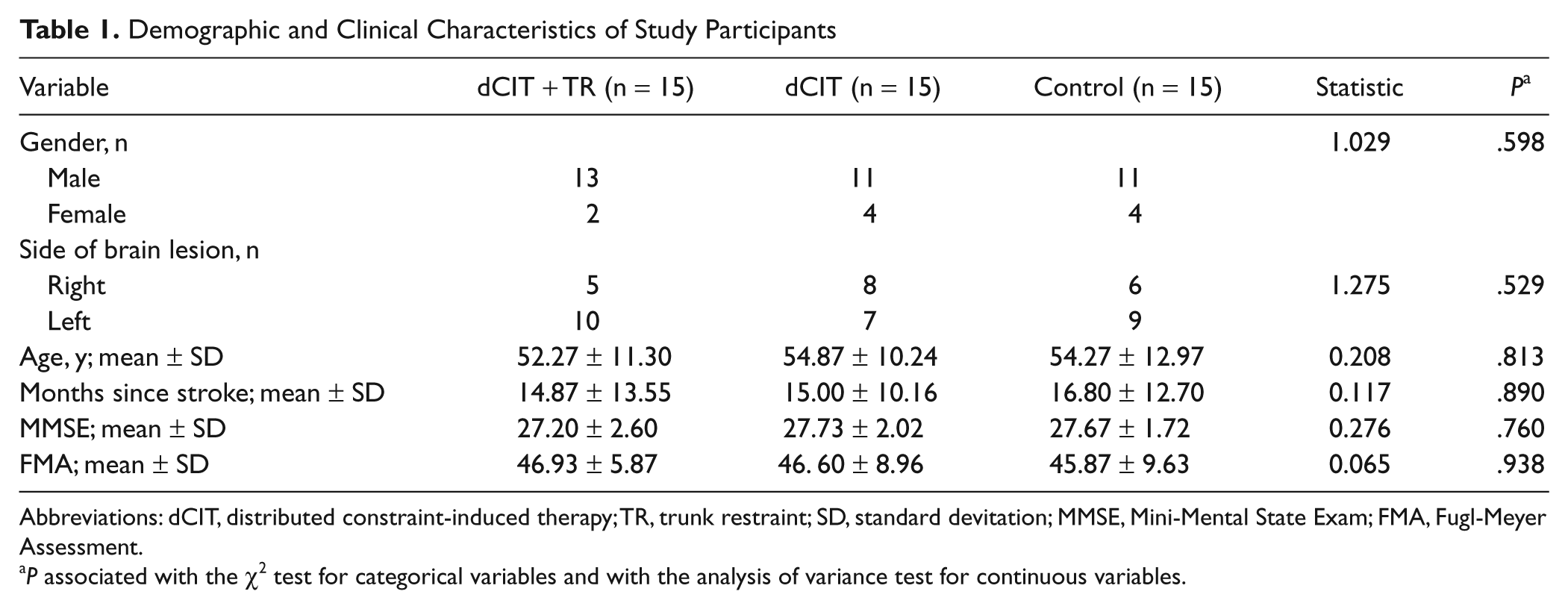
Abbreviations: dCIT, distributed constraint-induced therapy; TR, trunk restraint; SD, standard devitation; MMSE, Mini-Mental State Exam; FMA, Fugl-Meyer Assessment.
P associated with the χ2 test for categorical variables and with the analysis of variance test for continuous variables.
Primary Outcome Measures: Kinematic Analysis
No kinematic data were obtained from 4 to 5 participants in each group because they were unable to successfully grasp a can. Consequently, kinematic data of 11, 10, and 10 participants were analyzed in the dCIT + TR, dCIT, and control groups, respectively. Table 2 shows descriptive statistics of the joint angle and trunk contribution for the kinematic tasks in each group at pretest and posttest.
Descriptive Statistics of Joint Range and Trunk Contribution for the Kinematic Tasks a
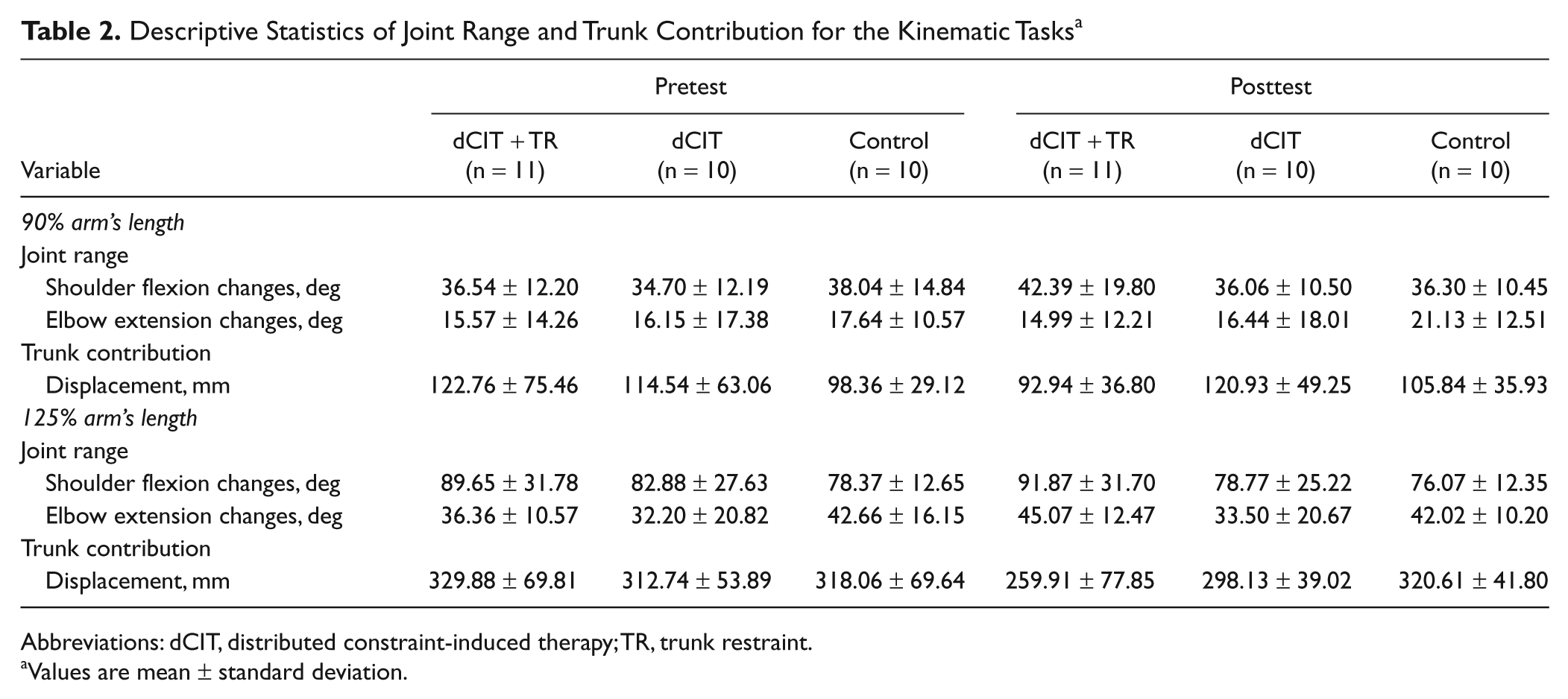
Abbreviations: dCIT, distributed constraint-induced therapy; TR, trunk restraint.
Values are mean ± standard deviation.
Grasping components
A significant and large effect was found in the MGA variable at both task distances; however, the result on TMGA showed a significant difference only at the task performed at 125% arm’s length (Table 3). Post hoc analyses showed significant differences between the dCIT + TR and control groups. Compared with the control group, the dCIT + TR group, but not the dCIT group, showed a significantly smaller MGA at both tasks (90%, P = .013; 125%, P = .011) and a larger TMGA at the task at 125% arm’s length (P = .016).
Descriptive and Inferential Statistics for the Kinematic Tasks a
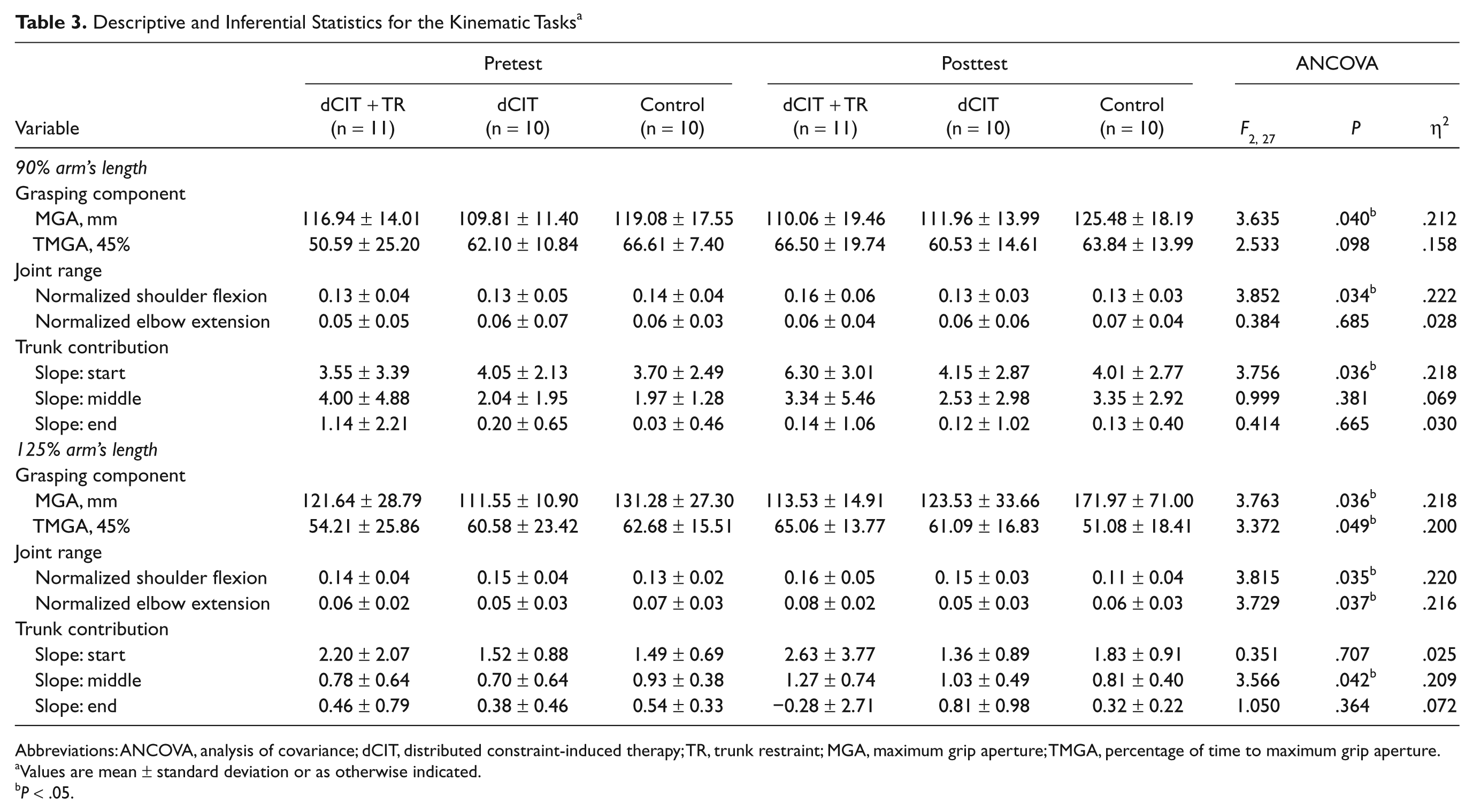
Abbreviations: ANCOVA, analysis of covariance; dCIT, distributed constraint-induced therapy; TR, trunk restraint; MGA, maximum grip aperture; TMGA, percentage of time to maximum grip aperture.
Values are mean ± standard deviation or as otherwise indicated.
P < .05.
Joint range
The angular changes of normalized shoulder flexion represented significant and large effects at both task distances among the 3 groups (Table 3). Post hoc analyses revealed that the dCIT + TR participants showed larger active shoulder movement than the dCIT participants (P = .044) at the task at 90% arm’s length and the control participants at both tasks (90%, P = .015; 125%, P = .010). However, the dCIT group exhibited no significant difference compared with the control group in shoulder joint angle at both tasks.
Nonsignificant and small effects were observed in normalized elbow extension at the task at 90% arm’s length, but significant and large effects were observed at the task at 125% arm’s length (Table 3). Post hoc analyses showed the dCIT + TR participants recruited larger elbow movement than those in the dCIT group (P = .013) at the task at 125% arm’s length. No other pairwise comparisons showed significant differences.
Trunk contribution
In the reach-to-grasp task at 90% arm’s length, there was a significant and large effect only on the start third of the reach-to-grasp phase among the groups (Table 3). The dCIT + TR group showed significantly less trunk contribution during the start third phase than the dCIT group (P = .024) and the control group (P = .028), but the dCIT group was not significantly different from the control group.
The results of trunk contribution in the task at 125% arm’s length showed that only the middle phase achieved statistical significance and a large effect (Table 3). In this phase, the dCIT + TR group exhibited less trunk compensation than the control group (P = .013), but no significant differences were noted between the dCIT + TR and dCIT groups or between the dCIT and control groups.
Secondary Outcome Measures: Clinical Measures
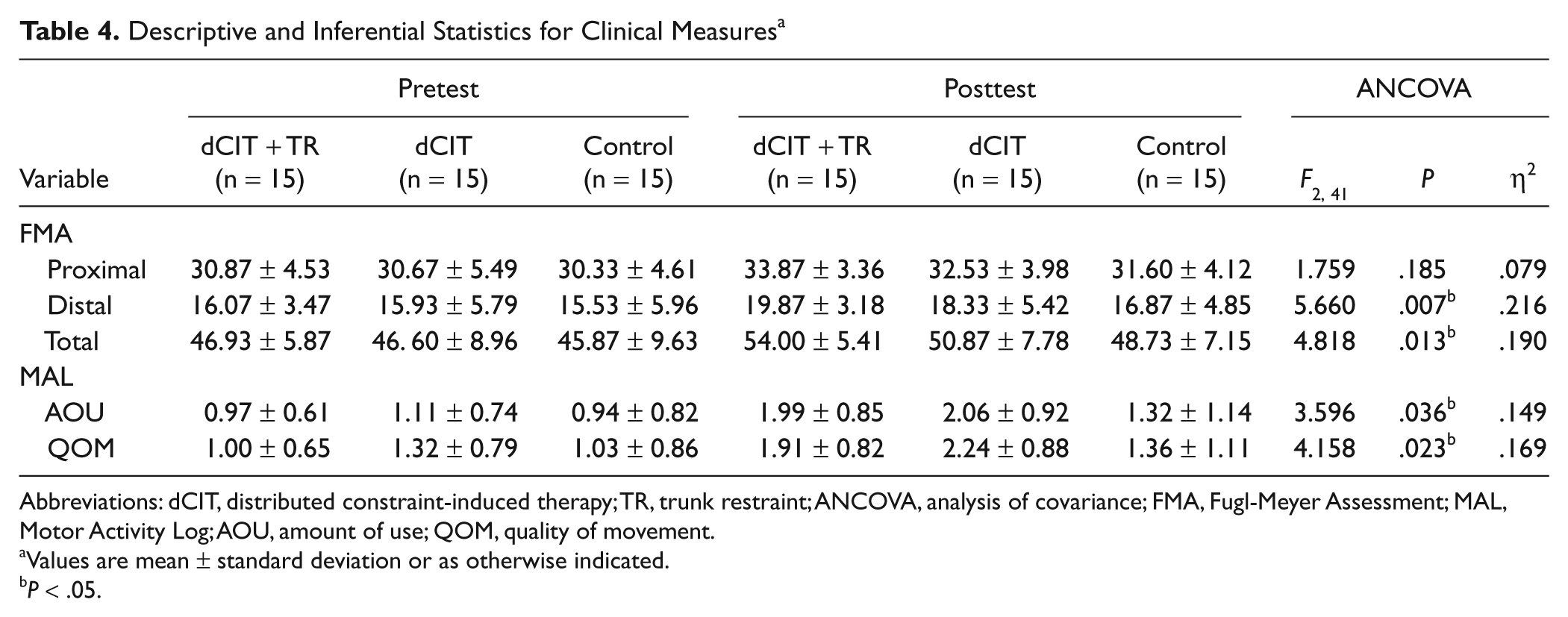
The participants in all of the groups exhibited improved clinical scores after the interventions. Results of the analysis of covariance showed significant differences in the distal part and total scores of the FMA, but no significant difference in the proximal part (Table 4). Post hoc analyses revealed that the dCIT + TR group had more improvements in the distal (P = .002) and total scores (P = .004) than the control group.
Descriptive and Inferential Statistics for Clinical Measures a
Abbreviations: dCIT, distributed constraint-induced therapy; TR, trunk restraint; ANCOVA, analysis of covariance; FMA, Fugl-Meyer Assessment; MAL, Motor Activity Log; AOU, amount of use; QOM, quality of movement.
Values are mean ± standard deviation or as otherwise indicated.
P < .05.
Compared with the control group after the 3-week intervention (Table 4), the dCIT + TR and dCIT participants used their affected hand with higher frequency (dCIT + TR vs control, P = .021; dCIT vs control, P = .031) and higher quality (dCIT + TR vs control, P = .021; dCIT vs control, P = .014). The differences in AOU and QOM between the dCIT + TR and dCIT groups were not significant.
Discussion
This study demonstrated that the dCIT + TR had additional benefits on grasping control strategies and trunk motion in the early phase of the reach-to-grasp movements, extending the study by Woodbury et al 13 to different types of CIT protocols. Generally speaking, the dCIT + TR group showed less MGA than the control group, obtained greater gains in voluntary range of motion at the shoulder and/or elbow than the dCIT or control group, and decreased trunk compensation more than dCIT and/or the control therapy at the different phases of the reach-to-grasp tasks, depending on the target distance.
The dCIT + TR group, but not the dCIT group, showed less hand opening at tasks within and beyond arm’s length and greater relative TMGA only at the task beyond arm’s length than the control group. The nonsignificant differences in hand opening and TMGA between the dCIT and control groups are similar to the findings of Lin et al. 3 These results indicated that the dCIT + TR group used more preplanned and skillful strategies rather than heavily depended on online error correction after the intervention than the other groups. Whereas the pattern decreased after dCIT + TR therapy, the MGA tended to increase and TMGA decreased in both task distances after the dCIT and control interventions, suggesting that the dCIT and control groups depended more on online error correction and used less skillful, compensatory strategies to complete the tasks. 30
In healthy individuals, the acquisition of new motor skills involves a decrease in the number of degrees of freedom used 31 and incorporation of these degrees of freedom into a controllable system, represented by “optimal synergies” 32 or “coordinative structure.”18,33 In a similar way, dCIT + TR participants were forced to block the additional degree of freedom in trunk (ie, abnormal synergies) and reorganize the required degrees of freedom from the UE into a more normal coordinative structure. The control of grasping consequently improved.
The shoulder joint range was significantly increased in the dCIT + TR group compared with the dCIT group in the task within arm’s length and the control group in both tasks, in agreement with previous studies,7,13 which may preserve the ability to adapt movements to various external conditions. Furthermore, voluntary shoulder flexion is more amenable to change than elbow extension. 30 Limiting trunk compensation may force participants to focus on important elements of the movement pattern and encourage the recovery of shoulder joint flexibility.
In normal reach-to-grasp tasks, adults maintain some elbow flexion at the end of reaching to facilitate final adjustments to hand location and orientation. 34 We speculated that the dCIT + TR participants might use a similar strategy and primarily use shoulder flexion for accomplishing the reach-to-grasp task. The elbow joint was significantly more recruited in the dCIT + TR group than in the dCIT group only at the task at 125% arm’s length, which is partially consistent with previous research.1,7,10-13 The differential results—the present study showed improvements in the elbow but the previous studies did not7,11,13—might have occurred because of the difference in the experimental tasks or in the control strategies that participants individually learned and adopted during training.
Less relative trunk contribution in the early phase of reach-to-grasp movements was found in the dCIT + TR group. Truncal support and restraint may trigger an implicit learning strategy that enabled more normal trunk adaptation.7,13,31 A possible reason for decreased trunk segment motion in the middle third of reaching for the task at 125% arm’s length might be that the long reach-to-grasp distance required the generation of high force at the initial stage of the movements.34,35 Trunk assistance at the start of reaching might facilitate higher force generation, and therefore, decreased compensatory trunk motion was shifted to the middle third of reaching.
The positive effects on the distal FMA score were paralleled by gains in grasping kinematics after dCIT + TR, but not after dCIT, indicating that adding trunk restraint to dCIT helps augment the treatment effects on UE motor function, especially distally. As with the kinematic improvements, FMA gains in distal UE motor function may rely on developing more normal movement strategies rather than just adapting to compensatory or undesired movement patterns. The dCIT + TR and dCIT interventions showed similar beneficial effects in the AOU and QOM scores of the MAL, but this test includes few activities requiring UE–trunk motion. 13 Moreover, the dCIT participants might successfully achieve the tasks required in the MAL by compensatory movements.
A few study limitations are of note. First, our sample size was too small to reach a definite conclusion, and the findings may not be generalized beyond the scope of the particular participants in the study. Second, we did not address retention of the intervention effects. In addition, our therapies excluded practice at distances farther than 125% arm’s length and sideways reaching. 36
Conclusion
This study demonstrated the additional benefits of trunk restraint when integrated into dCIT to improve the control of grasp and decrease truncal compensatory motion. Both, the dCIT + TR and dCIT, led to more improvement on functional use of the affected arm than the control therapy. The findings suggest the need for further research in a broader population and for outcome measures that best reflect gains in UE-truncal activities.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the National Health Research Institutes (NHRI-EX99-9920PI and NHRI-EX100-10010PI) and the National Science Council (NSC-97-2314-B-002-008-MY3, NSC-97-2314-B-182-004-MY3, and NSC-99-2314-B-182-014-MY3) in Taiwan.