
Abstract
Background. Cardiorespiratory fitness is low after stroke. Improving fitness has the potential to improve function and reduce secondary cardiovascular events. Objective. This review with meta-analysis aims to identify characteristics and determine the effectiveness of interventions to improve cardiorespiratory fitness after stroke. Methods. A systematic search and review with meta-analysis was undertaken. Key inclusion criteria were the following: peer-reviewed articles published in English, adult stroke survivors, an intervention with the potential to improve cardiorespiratory fitness, and peak oxygen consumption (VO2peak) assessed preintervention and postintervention via a progressive aerobic exercise test. Results. From 3209 citations identified, 28 studies were included, reporting results for 920 participants. Studies typically included chronic, ambulant participants with mild to moderate deficits; used an aerobic or mixed (with an aerobic component) intervention; and prescribed 3 sessions per week for 30 to 60 minutes per session at a given intensity. Baseline VO2peak values were low (8-23 mL/kg/min). Meta-analysis of the 12 randomized controlled trials demonstrated overall improvements in VO2peak of 2.27 (95% confidence interval = 1.58, 2.95) mL/kg/min postintervention. A similar 10% to 15% improvement occurred with both aerobic and mixed interventions and in shorter (≤3 months) and longer (>3 months) length programs. Only 1 study calculated total dose received and only 1 included long-term follow-up. Conclusions. The results demonstrate that interventions with an aerobic component can improve cardiorespiratory fitness poststroke. Further investigation is required to determine effectiveness in those with greater impairment and comorbidities, optimal timing and dose of intervention, whether improvements can be maintained in the longer term, and whether improved fitness results in better function and reduced risk of subsequent cardiovascular events.
Introduction
In primary prevention, level of physical activity is an independent predictor of stroke risk.1,2 Lack of physical activity accounts for 28.5% (99% confidence interval [CI] = 14.4%-48.5%) of stroke population–attributable risk, second only to hypertension (34.6%, 99% CI = 30.4%-39.1%). 2 Adults who are highly or moderately active have an approximately 25% lower stroke risk. 1 Following stroke, evidence is scant for the benefit of physical activity to reduce death, dependence, or disability; prevent subsequent stroke; or improve longitudinal cardiovascular health outcomes.3-5 However, given the benefits of exercise in primary prevention, there is a very high probability that it is also beneficial in secondary prevention. It is therefore concerning that an estimated 77% of stroke survivors are sedentary or have low levels of physical activity. 6 Cardiorespiratory fitness after stroke is very low, with peak oxygen consumption (VO2peak) values ranging from 8 to 22 mL/kg/min, which equates to 26% to 87% of gender- and aged-matched healthy individuals. 7 Levels below 15 and 18 mL/kg/min for women and men, respectively, can lead to loss of independence because activities of daily living become too fatiguing. 8 Stroke guidelines recommend cardiorespiratory fitness training after stroke9-12; however, this is rarely implemented because regaining physical function is a primary focus. Many clinicians have limited experience with cardiorespiratory fitness testing or exercise prescription after stroke. 13
The aim of this systematic review with meta-analysis was to determine the effectiveness of exercise interventions to improve cardiorespiratory fitness after stroke. The primary outcome was change in cardiorespiratory fitness, as measured by the gold standard of VO2peak achieved during progressive aerobic exercise testing using open-circuit spirometry. Subgroup analyses were planned to investigate factors hypothesized to influence effectiveness of the interventions. By synthesizing the data available regarding characteristics of studies, participants (gender, age, and time poststroke), and interventions (type, dose, training setting, group/individual program, risks, satisfaction, and effect maintenance), our aim was also to inform clinicians on strategies to improve cardiorespiratory fitness of people poststroke.
Methods
The conduct and reporting of this review was guided by the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) 14 and the Consolidated Standards of Reporting Trials (CONSORT) 15 statements.
Eligibility Criteria
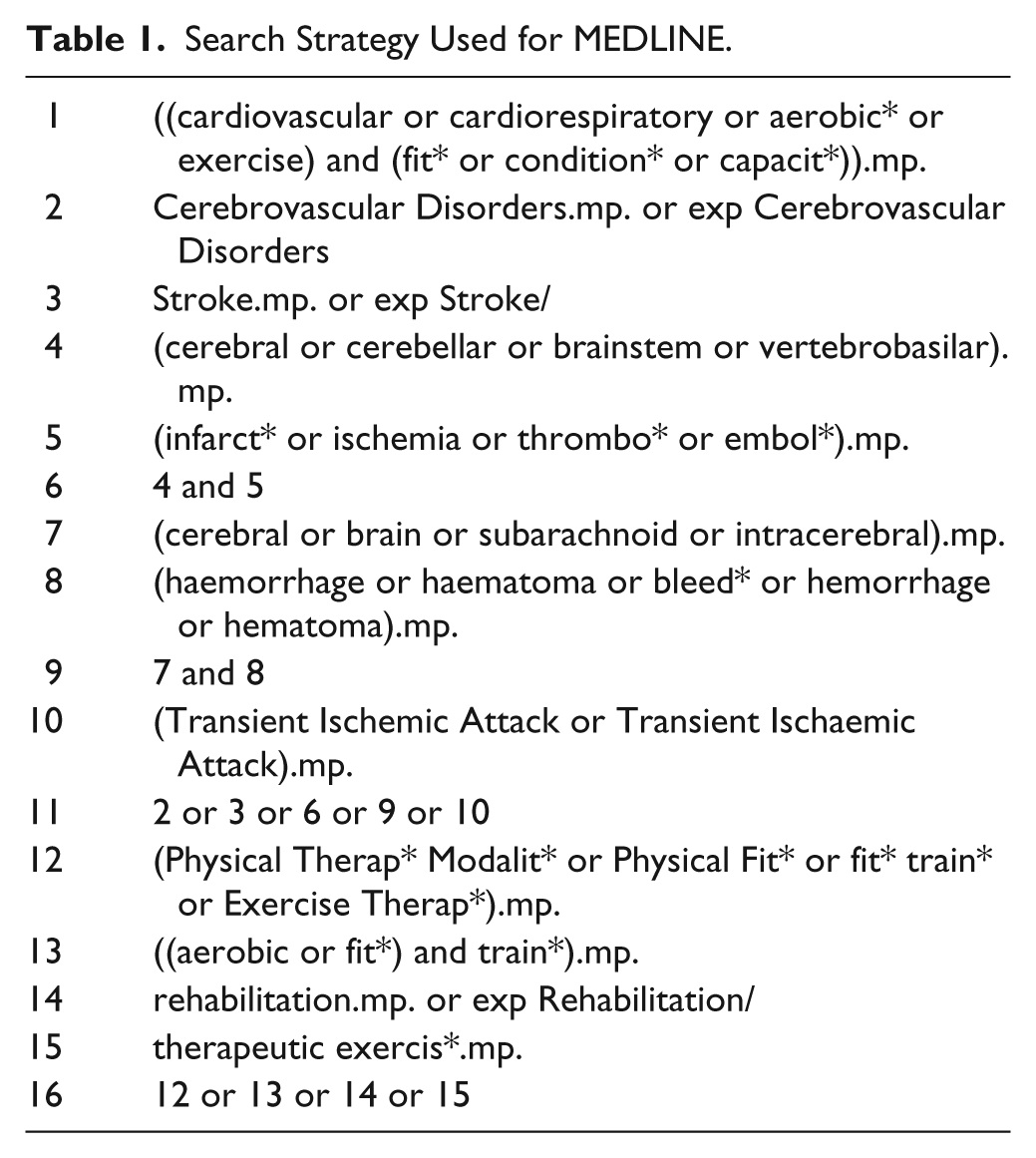
A systematic search was undertaken of MEDLINE, CINAHL, EMBASE, PscyINFO, AMED, SPORTDiscus, and COCHRANE databases from their inception to December 27, 2011. Terms used for the MEDLINE search are listed in Table 1. These were adapted as required to suit each database searched. Inclusion criteria were the following: people aged 18 years and over at any time poststroke or post–transient ischemic attack; controlled and noncontrolled trials published in a peer-reviewed, English language journal and containing primary data; peak or maximal oxygen consumption assessed using open-circuit spirometry via a progressive aerobic exercise test preintervention and postintervention; and an exercise intervention used that had the potential to improve cardiorespiratory fitness. Theses and articles published in abstract form only, including conference proceedings, were excluded.
Search Strategy Used for MEDLINE.
Study Selection
After duplicates were removed author DLM sorted the search results by title and abstract into “include” and “exclude,” and author AD reviewed for agreement. The full text for all included articles were obtained and reviewed by authors DLM and AD for a final decision, with any discrepancies discussed and a consensus agreed. Author RC was consulted if further clarification was required. Hand searching of articles identified in the reference lists of included articles was also undertaken.
Data Items and Extraction
Data from the included articles were extracted into Excel 2007* by DLM and checked by AD and included the following:
Study characteristics: study design, country, year published, inclusion and exclusion criteria, participant numbers, including gender ratio, attrition, quality
Participant characteristics: age, time since stroke
Interventions: type, dose (program length, session duration, frequency and intensity), advice regarding exercise outside of intervention, training setting, group/individual program, risks/adverse events, satisfaction, effect maintenance
VO2peak: testing method, results preintervention and postintervention in mL/kg/min
Study Quality and Risk of Bias
The Physiotherapy Evidence Database (PEDro † ) independently assesses studies against 10 criteria for quality. Ratings for the randomized controlled trials (RCTs) included in this review were extracted from PEDro and categorized by score: excellent (9-10), good (6-8), fair (4-5), and poor (<4). Quality was also evaluated by VO2peak equivalence at baseline and the inclusion of sample size calculations.
Synthesis of Results
Statistical analysis was undertaken using RevMan5. ‡ Meta-analyses were planned to compare change in the primary outcome—VO2peak in RCTs that used an intervention group and a control group with no intervention, sham training, or an intervention that would be unlikely to have an aerobic training effect. Four analyses with subgroups were planned: intervention type, time since stroke (≤3 months, >3 and ≤12 months, >12 months), program length (≤3 months, >3 months), and “met exercise recommendations for older adults” 16 (moderate intensity for at least 30 min/d on most days of the week). Because VO2peak data are continuous, a random-effects analysis model was used with mean difference at postintervention as the effect measure, with 95% CI. Standard errors were converted to standard deviations (SDs). 17 Post measures for 1 study 18 were not reported and so were calculated by adding the change score to the baseline score and using the baseline SDs. For Lee et al 19 where more than 1 intervention was compared with a shared control group, the total number of control participant numbers were split evenly between the intervention groups, with the means and SDs left unchanged. 17 Statistical heterogeneity was measured using the χ2, τ2, and I2 tests.
Results
Figure 1 outlines the flow of articles, including reasons for exclusion. From 3209 citations, 28 studies were included.
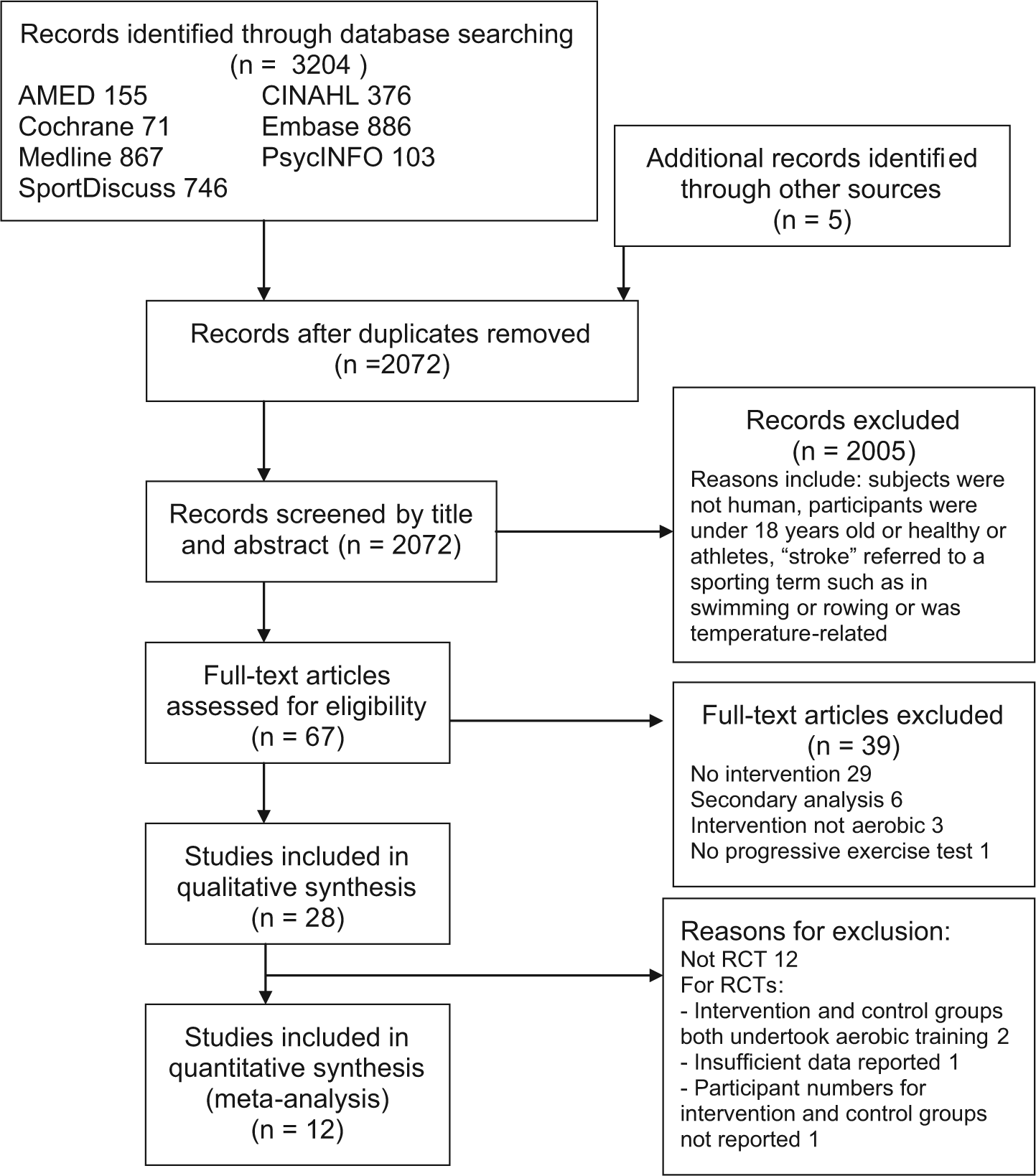
Flowchart for study selection
Characteristics of Studies
The study characteristics are summarized in Table 2. There were 16 RCTs, 1 controlled trial with matched participants, and 10 noncontrolled trials using pre-post testing of the cohort. The remaining study 20 undertook a post hoc pre-post analysis of the intervention groups of 2 RCTs. Only data from the German arm was extracted from this article because the United States arm 21 was included independently. All studies were published since 2000 except 1 (Potempa et al, 22 1995). The studies were undertaken in 9 countries, predominantly in North America (the United States [n = 16] and Canada [n = 4]). Study inclusion/exclusion criteria often included the following: more than 5 months poststroke (n = 18), mild to moderate stroke deficits (n = 10), independently ambulant (n = 21), mild or no cardiovascular/cardiopulmonary history (n = 19), no significant cognitive or communication issues (n = 12), no other major neurological condition (n = 7), and no major musculoskeletal problems or pain (n = 10). Also, 8 studies required participants to pass a treadmill (n = 6) or cycle (n = 2) screening test.
Characteristics of the Studies, Grouped By Training Type and Listed by Time Since Stroke.

Abbreviations: ACSMG, American College of Sports Medicine Guidelines; BP, blood pressure; C, control group; ConIn, contraindications; CMSA, Chedoke-McMasters Stroke Assessment; CV, cardiovascular; cyc, cycle; °, degrees; dur, duration; E, extension; F, flexion; FAC, Functional Ambulatory Classification; fMRI, functional magnetic resonance imaging; Grp, group; HF, heart failure; HR, heart rate; HT, hypertension; incl, including; indiv, individual; Inpt, inpatient; I, intervention group; I both, received both cycle and PRT; int, intensity; IQR, interquartile range; LL, lower limb; max, maximal MI, myocardial Infarction MMSE, Mini-Mental State Examination mod, moderate msk, musculoskeletal; nr, not reported; O2, oxygen; Outpt, outpatient; PAD, peripheral artery disease; PE, pulmonary embolism; PRT, progressive resistance training; RCT, randomized controlled trial; rehab, rehabilitation; revs/min, revolutions/minute; ROM, range of motion; SD, standard deviation; SEM, standard error of the mean; wks, weeks; wt, weight; X, exercise.
The 28 studies enrolled 1090 participants (male = 337 [30.9%], female = 191 [17.5%], not specified = 552 [52.6%]) and reported results on 920 participants (male = 437 [47.5%], female = 313 [34.0%], not specified = 170 [18.5%]). Attrition rates were reported in 22 studies and ranged from 0% (n = 5) to 41% of the control group in 2 studies. The main reasons for attrition included medical conditions unrelated to the study (39.9%), “noncompliance” (22.1%), “medical reason or noncompliance” (14.1%), transport/scheduling issues (6.1%), another stroke (3.1%), and a fall with hip fracture (3.1%).
Study Quality
Criteria ratings for 15 of the 16 included RCTs could be extracted from PEDro § (Table 3; see supplemental Table online at http://NNR.sagepub.com/supplemental). Letombe et al 23 was being rated at the time of this report. The ratings were: good (n = 5), fair (n = 9), and poor (n = 1). These 15 RCTs were all determined to have point estimates and variability, random allocation, and baseline comparability. No study had blinded participants or blinded therapists, and only 3 undertook intention-to-treat analysis. Of the 15 rated studies, 14 were similar for VO2peak at baseline for the intervention and control groups. Only 4 reported sample size calculations.
Participant Characteristics
The participant characteristics are outlined in Table 2. Mean ages ranged from 53 (no SD provided) to 71 (range = 61-79) years. The mean time since stroke ranged from 14.3 (6.1) days to 7.5 (range = 4-20) years, with the following distribution: within 1 month (n = 3); 2 to 3 months (n = 2); 1 to 3 years (n = 7) and greater than 3 years (n = 9). There were 7 studies that provided no details on time since stroke; however, 6 of these had inclusion criteria of more than 6 months, and for 1 study, it was greater than 12 months.
Interventions
The testing methods and intervention characteristics are summarized in Table 4 (see supplemental Table online at http://NNR.sagepub.com/supplemental).
Type
Of the 28 studies that met the search criteria, 16 used aerobic training20-22,24-36 (treadmill, n = 8; cycle, n = 6; deep-water exercise, n = 1; cycle and recumbent stepper, n = 1), 11 used a mixed intervention18,19,23,37-44 (an aerobic component in conjunction with usual care, strength, balance, and/or endurance activities), and one 45 used knee flexion/extension isokinetic training of the paretic leg, aimed at improving cardiorespiratory fitness.
Dose prescribed
All studies reported program length and planned intervention frequency and duration. Program length ranged from 2 to 3 weeks to 6 months, with 12 studies being between 3 and 6 months in length. Session durations ranged from 20 to 90 minutes, with most training lasting 30 to 60 minutes (n = 23). Frequency of sessions ranged from 2 to 5 times/wk, with most (n = 22) training 3 times/wk. Planned intensity was reported in 25 studies. Intensity was often calculated from baseline exercise testing and included percentage heart rate reserve (HRR; n = 11) and percentage power output (n = 6). Rating of perceived exertion was used as an adjunct measure in 5 studies. No study provided details regarding instructions to participants about trying to undertake further exercise outside of intervention sessions.
Dose delivered
Although training parameters were described, there was limited reporting of whether they were achieved. Adherence to training frequency was the most reported (n = 11), with all reporting greater than 72% of sessions attended. There was limited reporting of progression of parameters. Two studies25,34 reported progressions over 6 months in session duration, percentage HRR, treadmill velocity, and incline. Another study 38 reported target and achieved HR and duration for which target HR was sustained. They planned to progress the target HR zone; however, some participants could not progress past the initial 40% to 50% HRR, whereas other progressed to 70% to 80%. Only 1 study reported the proportion of prescribed dose achieved (63 ± 28%). 42
Training settings and individual/group program
Interventions were undertaken in outpatient rehabilitation settings (n = 6), inpatient settings (n = 4), university centers (n = 6), community centers (n = 2), at both a community center and at home (n = 2), and at home (n = 1); 7 studies did not specify but appeared center based. The majority of center-based interventions appeared to be provided on an individual basis (n = 18); 5 were group interventions, 1 was initially individual and progressed to group interventions, and it was unclear if 1 was an individual or a group intervention. The 2 programs with center and home interventions were carried out as a supervised group at the center and unsupervised individually at home. The home-only program used a supervised, individual approach.
Testing
A single ergometer modality was used to undertake progressive aerobic exercise tests in 25 studies. One study used 2 modalities, with the highest value obtained used for each patient, 43 whereas another chose the method that they thought best suited the participant. 42 Of the 28 studies, 27 used maximal protocols. The remaining study 27 used a “metabolic stress test” but did not specify the test type or equipment used. Baseline VO2peak in the studies ranged from 8.0 ± 2.1 to 22.5 ± 5.2 mL/kg/min, with a median of 14 mL/kg/min. Only 4 studies had mean baseline VO2peak measures above 18 mL/kg/min.
Adverse Events, Effect Maintenance, and Participant Satisfaction
Adverse events were not reported in 17 studies; 8 reported having no events during testing or training18,24-26,28,34,43,45; and 3 reported events that included the following: 5 low-impact falls by 4 participants with no injuries in the intervention group 38 ; 2 temporary musculoskeletal problems managed by altering the exercise regime, with the programs completed without interruption 42 ; and 2 events during testing, including a mild seizure and a drop in blood pressure, and 1 following an exercise session where the participant became dizzy and mildly incoherent but went on to complete the program. 39 No studies described instructions or a program to continue exercise after the completion of the intervention. Only 1 study undertook postprogram follow-up measures. 27 They showed a statistically significant difference between groups on completion of their 8-week intervention (P = .04) but no difference 8 weeks later at follow-up (P = .4). Only 1 study reported participant satisfaction. 42
Outcomes
Table 4 summarizes the VO2peak results preintervention and postintervention (see supplemental Table online at http://NNR.sagepub.com/supplemental).
Meta-analyses of RCTs
Of the 16 RCTs, 12 contained data suitable for inclusion in the meta-analyses (Figure 1). The overall mean difference was 2.27 (95% CI = 1.58, 2.95) mL/kg/min and favored interventions to improve VO2peak. This equated to a 10% to 15% improvement from baseline. The studies were statistically homogeneous (τ2 = 0.00; χ2 = 6.92; I2 = 0%]. In the subgroup analyses, benefit was observed in aerobic and mixed interventions, which were almost equally effective (Figure 2), as were programs ≤3 months and >3 months in length (Figure 3). The “time since stroke” meta-analysis was not undertaken because of insufficient data for comparison, with only 2 studies18,37 conducted within 3 months and the remaining studies, more than 12 months poststroke. No study protocol dose “met recommendations for older adults,” so this subgroup analysis was not undertaken.
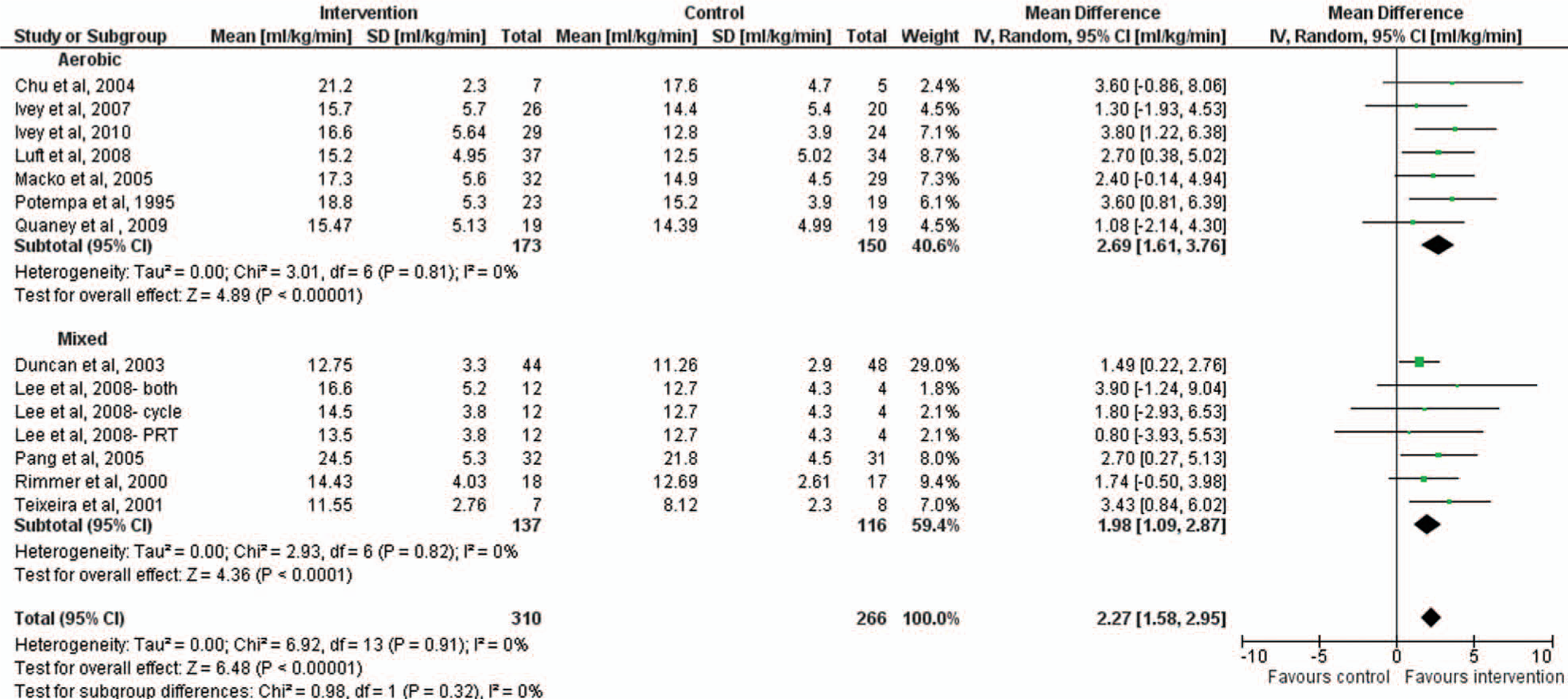
Forest plot of effect of intervention on VO2peak by Intervention Type.
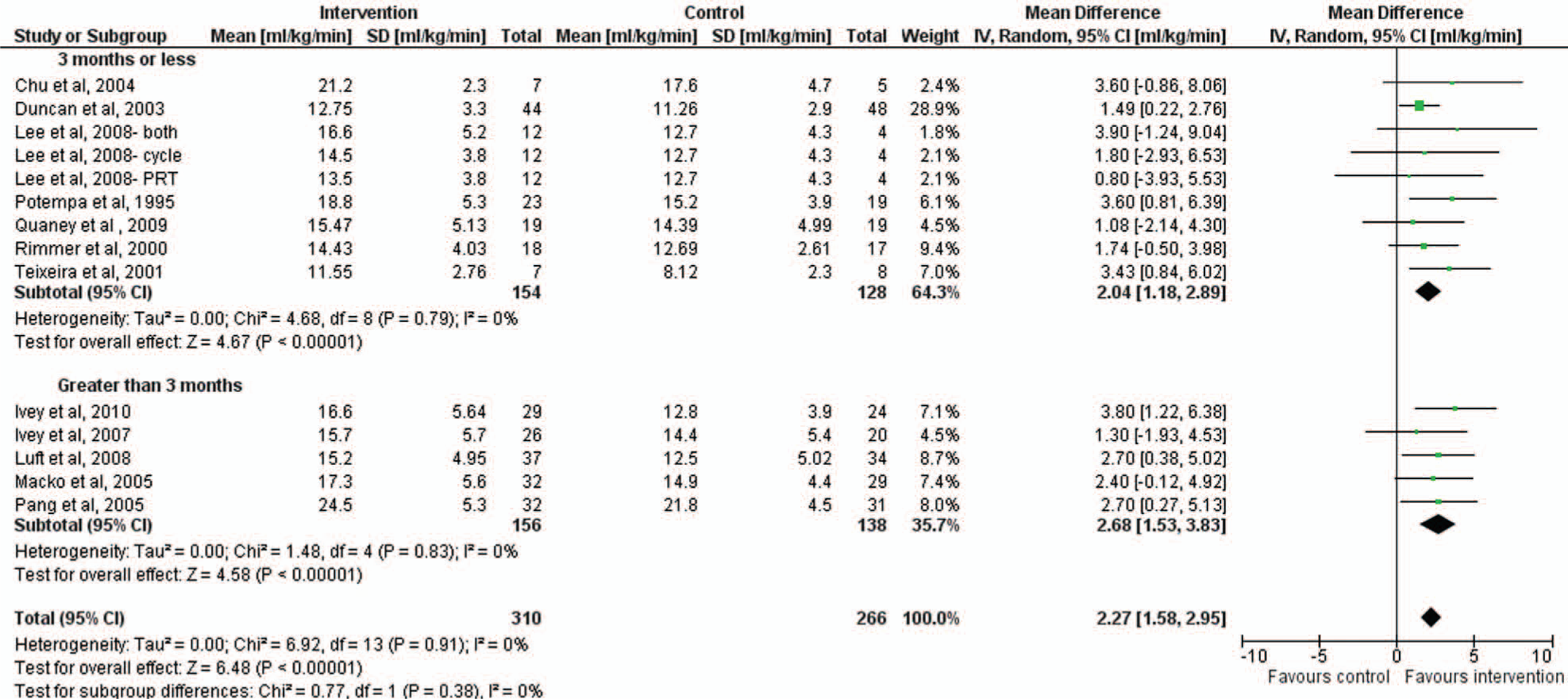
Forest plot of effect of intervention on VO2peak by Program Length.
Non-RCT Studies
Improvements in VO2peak in the non-RCT trials occurred in 5 of the 6 aerobic trials, with significant (P < .05) increases ranging from 10% 34 to 27.4%. 20 Of the 4 mixed-intervention non-RCT trials, 2 showed statistically significant increases of 9% and 16%, respectively.42,44 The isokinetic training of the paretic leg intervention produced no significant improvement (P = .413); however, this program was only 4 weeks long. 45
Discussion
Significant Benefit With Cardiorespiratory Training
This review highlights the fact that interventions that are aerobic or have an aerobic component can improve fitness by approximately 10% to 15%, even with modest doses of exercise. The observed improvement of 2.27 mL/kg/min (95% CI = 1.58, 2.95) in the meta-analysis of 12 RCTs in this review provides further confirmation of the positive effect of cardiorespiratory training, with a result similar to the 2.14 (95% CI = 0.50, 3.78) mL/kg/min observed in the recent Cochrane review based on 4 studies. 4 The dose protocols of the studies included in the meta-analysis were relatively modest, with none meeting the recommendation of 30 minutes of moderate-intensity physical activity most days of the week. 46 Despite this, they were still effective in generating improvements. The subgroup analysis identified programs of less than and greater than 3 months in length, both resulting in improvements of approximately 10% to 15% VO2peak. This finding is similar to the review by Shephard of aerobic training responses in the healthy elderly, where gains in VO2peak with training ranged from 12.9% for the short-term (8-10 weeks), 14.1% for the medium-term (12-18 weeks), and 16.9% for longer-term (24-52 weeks) programs. 8 Cardiorespiratory training appears to be beneficial for people at any time, from weeks to many years poststroke. The results also appear to indicate that a key factor in improving cardiorespiratory fitness is to incorporate aerobic activity, with the exact intervention appearing to be less important. A larger dose of these programs or different interventions may lead to greater improvements in cardiorespiratory fitness levels after stroke.
Very Low Levels of Baseline Fitness
The very low levels of baseline cardiorespiratory fitness of stroke survivors are highlighted in this review. Baseline VO2peak levels in all but 4 studies were below the 18 mL/kg/min suggested as being a minimum required for independent living, 8 and all studies showed baseline values well below normative data for an elderly population (29 ± 7.3 and 27 ± 5.8 mL/kg/min for healthy men and women, aged 70-79 years, respectively 47 ). This is despite the studies typically including highly selected participants: ambulatory with limited comorbidities. It is very likely that fitness levels in the general stroke population are even lower. Many stroke survivors are likely to be limited in day-to-day activities by their cardiorespiratory fitness. This is in addition to any disability caused by the more widely recognized major physical impairments of stroke, including muscle weakness, poor balance, loss of coordination, and spasticity. The results highlight the large room for improvement in cardiorespiratory fitness poststroke.
Exercise Dose, Intensity, and Timing
“Dose” of exercise is governed by frequency (per week), duration (per session), and intensity (and for how long this is maintained within a session). Data in healthy populations indicate that exercise intensity is a key variable to maintain and improve cardiorespiratory fitness. 46 One study in our review compared 2 trials with similar interventions and found higher intensity was the only training variable that predicted better gains in cardiorespiratory fitness. 20 However, as highlighted by Pang et al, 38 the ability of participants to increase intensity varies, with the maximum achieved after 19 weeks of training ranging from unchanged from the initial 40% to 50% HRR up to 70% to 80% HRR. This intensity was maintained for 15 minutes compared with the recommended 30 minutes. Studies in the healthy elderly have reported greater improvements with higher intensity 8 ; however, lower intensities may be effective in untrained populations. 48 For this very unfit population, commencement of training at a lower intensity level with progression as tolerated is likely to be required. The dose of exercise required to maintain or enhance cardiorespiratory fitness after stroke remains unclear. Although frequency, duration, and intensity levels were prescribed in the majority of the studies, only 1 calculated the proportion of prescribed dose achieved (63% ± 28%). 42
Timing after stroke may also be a key factor, particularly in any contribution cardiorespiratory fitness training may make to functional recovery. Surprisingly, only 5 studies were within 3 months after stroke. This should be a key time for preventing cardiorespiratory deconditioning and promoting brain reorganization, both of which require meaningful and challenging physical activity. 49 Inpatient environments have the potential to routinely incorporate cardiorespiratory fitness training into their programs; however, they are consistently identified as settings deprived of activity poststroke.50,51 One systematic review indicated that only 32.8 minutes (60%) of inpatient physiotherapy sessions was spent being active. 52 Other studies have shown that little or no time during inpatient physiotherapy sessions was spent in a HR range that would be expected to improve cardiorespiratory fitness.53,54
Mode of Delivery of Interventions
Given the current health economic climate, interventions designed to increase cardiorespiratory fitness need to be resource-efficient as well as effective. Only a few of the studies in this review used group programs (n = 5), unsupervised home interventions (n = 2) or community center programs (n = 4). A number of interventions appeared quite resource intensive; 19 used 1-to-1 supervision, and 14 were greater than 3 months (Table 4; see supplemental Table online at http://NNR.sagepub.com/supplemental). A review of physical activity programs for older adults identified health benefits and improved function that were gained through both center- and home-based programs. 55 The home-based programs had better adherence, particularly in the long term. 55 Redesign of services to include cardiorespiratory fitness training within existing budgets may be more likely to be generalizable, rather than relying on service enhancements. One study redesigned their inpatient program to compare 20 minutes of treadmill training with the usual 20 minutes of standard gait training. 37 The therapy time was unchanged. Two studies used a combined center and home program, which may be a feasible way to assist stroke survivors to be active on most days of the week.41,43 Redesign may occur through the use of groups, including circuit classes, as inpatient, outpatient, and community-based programs. 56 Participation in groups has the advantage of increased ratio of group leader to participants 56 and the added benefits of social interaction and peer motivation. 57
Comparison With Other Chronic Diseases
A number of the issues identified above are common to other chronic diseases. A recent review of exercise and Parkinson’s disease identified that interventions were predominantly highly supervised, center-based programs, trialled in cognitively intact participants with mild-to-moderate disease. 58 Reviews of the effect of exercise-based rehabilitation on coronary heart disease 59 and heart failure 60 highlighted the fact that participants were predominantly middle-aged men with low and low to moderate risk, respectively. Exercise interventions may improve health-related quality of life and improve exercise capacity without increased risk of death in heart failure patients. 60 However, in this population, it does not reduce all-cause mortality, nor could a minimum dose of exercise be recommended because of the variation in programs. 60 Following exercise, there was no reduction in recurrent myocardial infarction or revascularization for coronary heart disease participants. However, for those followed up for more than 12 months, there was a reduction in all-cause and cardiac mortality. Further investigation in stroke is required to investigate the very important health-related quality of life, secondary prevention, and mortality outcomes.
Strengths and Limitations
The use of the PRISMA and CONSORT statements guided the unbiased conducting of the review with meta-analysis. The meta-analysis was statistically homogeneous, indicating that like studies were being compared, had reasonable participant numbers, and provided a more robust estimate of likely benefit than the individual studies alone. There were some unavoidable limitations. Only studies published in English were included. There are relatively few RCTs in the field, and not all could be included in the meta-analysis. Study quality of the RCTs included in the meta-analysis was variable, with ratings of good (n = 5) and fair (n = 7). Only 4 of the studies used an intention-to-treat analysis, with most reporting data only for those who completed the program. This, combined with high attrition rates in some studies, may introduce considerable bias. Attrition rates, when reported, varied from 0% to 41%, and the main reasons provided were medical problems not related to the program and noncompliance, although this term was not explained. Studies were conducted in people with mild to moderate deficits; therefore, there is limited generalizability of the results to those with greater stroke deficits or multiple comorbidities.
Suggestions for Reporting in Future Studies
To improve the understanding of the effects of training on cardiorespiratory fitness, it would be useful for studies to consistently report several data items. As VO2peak is measured in mL/kg/min it is influenced by change in weight, which may occur over time. Future studies should report both in L/min for absolute change and mL/kg/min to give an indication of cardiorespiratory fitness level. Although dose was prescribed, it was difficult to ascertain the dose that was delivered. This has also been identified as an issue in heart failure interventions. 60 To gain a better understanding of the stimulus required for benefit, studies should quantify the proportion of dose achieved in terms of sessions attended, intensity, and duration of the sessions. Reporting of the progression of parameters would also provide insight to effects of training on stroke survivors’ endurance and exercise tolerance. Few adverse events were reported during testing or training, and the majority were minor. Lack of reporting on the presence or absence of adverse events and reasons for attrition is common with exercise interventions in other chronic disease populations.58,59 All studies should report these to help inform the risks versus benefits of training. This may inform tailoring interventions for the heterogeneous stroke population.
Implications for Future Research
Despite the positive results highlighted in this review, many questions are yet to be answered. Further investigation is required into what actual dose, as opposed to prescribed dose, of aerobic activity is adequate to gain the benefit demonstrated and what is required in an intervention, in terms of aerobic training programs and dose, to obtain even greater improvements. Most studies undertook very traditional center-based, supervised treatment sessions rather than assisting participants in adopting cardiorespiratory fitness training as part of a “lifestyle change” for a chronic disease. The results of this analysis suggest that inclusion of any aerobic exercise is far more important than the specific program; therefore, future studies should focus on broadly generalizable interventions that are able to be delivered within existing budgets. Investigation is also required into strategies to engender long-term behavior change and maintain improvements postprogram. Larger-scale studies, including outcomes for functional improvement, recurrent stroke, cardiovascular events, death, or dependence, would help confirm likely additional benefits of exercise poststroke and enhance clinical uptake. Studies are required to determine whether improved levels of cardiorespiratory fitness can also be obtained in those with greater impairments poststroke, for older and younger patients, and those with significant comorbidities as well as to determine the importance of timing of the intervention poststroke.
Conclusion
This study provides clear evidence that important cardiorespiratory fitness benefits can be obtained from training, whether aerobic or mixed with an aerobic component. Training can increase cardiorespiratory fitness in people with mild-moderate impairment after stroke, reducing the percentage VO2peak at which people have to work to undertake everyday tasks. Cardiorespiratory fitness is a relatively new area of stroke research and requires further investigation to inform practice. This review provides strong evidence that exercise training is feasible and effective in at least a subset of people after stroke, and given the available evidence in other related diseases, it suggests that such training programs should be incorporated into routine poststroke care.
Footnotes
Acknowledgements
We would like to acknowledge Debbie Booth (Faculty Librarian—Health, University of Newcastle) for assistance with the systematic search and Patrick McElduff (Associate Professor of Biostatistics, University of Newcastle) for advice on the meta-analyses.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: DL Marsden is supported by the Heart Foundation and the University of Newcastle through the provision of a postgraduate scholarship and by the Hunter Stroke Service. Her research is supported through grants from the National Stroke Foundation, John Hunter Hospital Charitable Trust, and the Hunter New England Allied Health Research Committee Research Grants. A Dunn is supported by the University of Newcastle through the provision of an Australian Post-Graduate Award scholarship. CR Levi is a National Health and Medical Research Council Practitioner Fellow and Senior Staff Specialist Neurologist, Hunter New England Local Health District. NJ Spratt was supported by a health professional research fellowship from the National Health and Medical Research Council and by the Greater Building Society/Hunter Medical Research Institute.
*
Resource: Excel 2007, Microsoft Corporation.
†
Resource: Review Manager (RevMan) [Computer program]. Version 5.1. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011.