
Abstract
Background
Although various repetitive transcranial magnetic stimulation (rTMS) and theta burst stimulation (TBS) protocols are used, their comparative effectiveness for treating poststroke hemineglect remains unassessed.
Objective
To investigate rTMS and TBS effects on clinical outcomes in poststroke hemineglect through a systematic review and network meta-analysis.
Methods
We searched PubMed, EMBASE, and Cochrane Library databases up to March 7, 2024, for trials on rTMS or TBS in poststroke hemineglect. Included studies involved rTMS or TBS with different protocols, sham, or no stimulation, assessing hemineglect severity or impact. The quality of the included studies was evaluated using the PEDro scale. The network meta-analysis was performed using ShinyNMA (version 1.01).
Results
We analyzed 13 studies with 309 participants. All studies included participants who had experienced right hemisphere stroke. All included studies had a fair to good quality based on PEDro score evaluation. Protocols included continuous TBS (cTBS), high-frequency rTMS (HF-rTMS), and low-frequency rTMS (LF-rTMS) targeting both contralesional and lesional sites. HF-rTMS on the lesional site significantly improved short-term results on the line bisection test and Catherine Bergego Scale; LF-rTMS on the contralesional site improved short-term line bisection; and cTBS on the contralesional site improved long-term line bisection. No severe adverse events or significant inconsistencies were reported.
Conclusions
Our findings indicate that HF-rTMS targeting the lesional site is the preferred therapeutic approach for the short-term management of poststroke hemineglect. LF-rTMS directed at the contralesional site is a practical alternative. Moreover, cTBS targeting the contralesional site is a viable option because of its long-term effect.
Introduction
Stroke is an acute focal neurological deficit primarily attributed to cerebrovascular causes. 1 Ischemic strokes, which account for 60% to 70% of all strokes, result from acute arterial occlusion. 1 Worldwide, it ranks as the second leading cause of death and the third leading cause of both death and disability combined. 1 About two-third of individuals who have had a stroke face challenges such as motor or sensory deficits, language difficulties, cognitive impairments, heightened depression and anxiety, or emotional instability. 2 These issues often result in struggles with performing daily tasks both at home and within their communities. 2
A complication of stroke is hemineglect, which often occurs in patients who have lesions in their right hemisphere. 3 Hemineglect results from damage to the neural networks critical to spatial attention and related cognitive and motor function.3-5 Based on an animal model, lesions centered on the second branch of the superior longitudinal fasciculus have been linked to inducing hemineglect by disrupting the connection between the posterior parietal cortex and the prefrontal cortex. 6 Functional magnetic resonance imaging (fMRI) studies on hemineglect reveal that this condition is often linked to damage in the right parietal lobe. 7 fMRI studies frequently show reduced activation in this region when participants with hemineglect attempt tasks requiring attention to the space or body opposite to a cerebral lesion. 7 Research also indicates altered activation in the fronto-parietal network and potential compensatory recruitment of left hemisphere regions. 7 Additionally, fMRI can track changes in brain activity during rehabilitation, highlighting both dysfunction and potential recovery pathways, and providing biomarkers to guide rehabilitation in patients with hemineglect. 7
Hemineglect typically presents as a failure to respond to or report stimuli presented on the contralesional side; an inability to initiate or complete movement toward the contralesional side; difficulty reporting, manipulating, or producing mentally stored information; or failure to maintain a centered gaze or body posture but instead deviating toward the ipsilesional side. 8 Rehabilitation strategies often focus on improving awareness and implementing compensatory techniques to help individuals manage their symptoms and regain function.9,10
Repetitive transcranial magnetic stimulation (rTMS) is a noninvasive procedure in which a pulsed magnetic field is used to stimulate electrical activity in the brain.11,12 Various types and combinations of stimulation, as well as the target brain region, can result in various biological effects. 13 In post-stroke patients with motor defects, rTMS over the motor cortex stimulates pyramidal cells, activating the pyramidal (corticospinal) tract and generating descending volleys to spinal motoneurons.14,15 This results in muscle contraction and a motor-evoked potential, which is recorded by EMG.14,15 The amplitude of this potential indicates corticospinal tract excitability.14,15 Post-stroke sensory dysfunction is common and may affect patients’ quality of life. 16 Studies have demonstrated that rTMS applied to the sensory cortex can promote the recovery of sensory function in stroke patients. 16
Several frameworks have been proposed to explain stroke recovery, with the neuroplasticity model and interhemispheric competition model being the most prominent.17-20 According to the neuroplasticity model, stroke-induced damage prompts surrounding healthy neural tissue to reorganize and adapt, compensating for lost functions.17-19 This phenomenon, rooted in the concept of neuroplasticity, involves the brain’s remarkable ability to adjust and adapt its functional organization in response to injury or environmental demands. 17 Through this process, which is known as cortical reorganization, the brain can compensate for a loss of function or restore function in the affected area.17,18 In interhemispheric competition model, the unaffected region in the contralesional hemisphere exerts an excessive inhibitory influence on the affected cortex in the ipsilesional hemisphere.18,20 This inhibitory interaction between hemispheres may impede or restrict the recovery process following stroke.18,21
Research has revealed that high-frequency (HF) stimulation (>5 Hz) exerts excitatory effects, whereas low-frequency (LF) stimulation (<1 Hz) exerts inhibitory effects on the brain.13,22 Theta burst stimulation (TBS) is a type of rTMS protocol with the advantage of a shorter delivery time compared with traditional rTMS. When applied to the motor cortex, intermittent TBS (iTBS) has been shown to induce excitatory aftereffects, whereas continuous TBS (cTBS) may result in inhibitory aftereffects. 23
Glutamate, the main excitatory neurotransmitter, and γ-aminobutyric acid, the primary inhibitory neurotransmitter, play key roles in maintaining the brain’s physiological balance.24,25 The balance between their excitatory and inhibitory effects is crucial for maintaining the brain’s physiological functions.24,25 Some drugs, such as antidepressants or antipsychotics, may act on these neurotransmitters and affect neural plasticity. 26 Similarly, rTMS can modify neurotransmitter systems, including striatal dopamine release, metabolite levels, and glutamate transporter and receptor expression, potentially addressing aberrant plasticity in certain cases.24,25 Chronic exposure to rTMS has been shown to impact neurotransmitter levels, including brain-derived neurotrophic factor, a key protein involved in neuroplasticity. 27 However, some studies suggest that while chronic rTMS can lead to sustained therapeutic benefits, it might also induce subtle changes in brain chemistry that warrant careful monitoring. 28
Studies concluded that rTMS is a viable treatment option for poststroke hemineglect.29,30 LF-rTMS and cTBS to the contralesional site were suggested to be suitable on the basis of the results of subgroup analysis. 30 However, the studies did not directly compare various stimulation protocols or stimulation sites. Therefore, we conducted a comprehensive literature review to identify randomized controlled trials (RCTs) on the use of rTMS or TBS in participants with poststroke hemineglect. Subsequently, we performed a network meta-analysis to compare the effectiveness of various stimulation protocols and sites for reducing the severity and impact of poststroke hemineglect. Our research questions were as follows:
RQ1: What are the outcomes of rTMS and TBS in participants with poststroke hemineglect?
RQ2: Which stimulation protocol or site is most effective for achieving these outcomes?
Methods
This systematic review with network meta-analysis was registered in the International Prospective Register of Systematic Reviews (PROSPERO) database under the registration number CRD42024524061 on March 24, 2024. This study adhered to the guidelines in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) extension statement for network meta-analyses. 31
We included RCTs with a parallel or crossover design. To identify eligible studies, we applied the following participant (P), intervention (I), comparison (C), and outcome (O) criteria:
(P) Participants with a diagnosis of poststroke hemineglect.
(I) Intervention involving rTMS or TBS.
(C) Comparison groups receiving either a different rTMS and TBS protocol, sham control, or no stimulation as the control treatment.
(O) Outcomes measured through performance assessment for evaluating the severity or impact of hemineglect, including the line bisection test, Catherine Bergego Scale, and Behavioral Inattention Test, for both immediate and long-term assessments.
We excluded protocol papers, articles lacking a peer review, conference papers, and letters to the editor from our analysis. No language restrictions were applied in our search strategy.
Each author independently conducted a literature review, extracted data, and performed crosschecks in accordance with the PRISMA guidelines. 32 We conducted searches in the PubMed, EMBASE, and Cochrane Library databases for the period from their inception to March 7, 2024. Our search strategy incorporated terms related to poststroke hemineglect and rTMS and TBS along with equivalent terms (see Supplemental Appendix). RCTs were identified using the refined search function of the databases, where available. Additionally, we manually searched the reference lists of relevant articles to identify additional studies.
Two reviewers independently assessed the eligibility of the identified articles by screening titles and abstracts. Any disagreements were resolved through discussion with a third reviewer. The full texts of all remaining articles were screened to determine their eligibility.
Two authors independently extracted the following information from each article: type of RCT, phase of stroke, stimulation site, number and mean age of participants, protocol used in different groups, treatment duration, follow-up duration, and outcome measurements. Any discrepancies were identified and resolved through discussion with a third reviewer. When data were unclear or missing, we contacted the authors of the respective articles via email to request clarification.
Our primary outcome measure was the result of the line bisection test, which evaluates the severity of hemineglect. The secondary outcomes were results on the Catherine Bergego Scale and Behavioral Inattention Test, both of which assess the impact of hemineglect on the performance of activities of daily living. Considering that rTMS and TBS potentially influences the interhemispheric relationship depending on the specific protocol and targeted brain area,33,34 we categorized interventions accordingly. Data from immediate assessments or the longest follow-up were pooled in the network meta-analysis to provide comprehensive insights into the efficacy of the interventions.
The quality of the included studies was evaluated using the Physiotherapy Evidence Database (PEDro) scale, which has been recognized as a reliable tool for assessing the risk of bias in RCTs. 35 Inconsistencies in quality scores estimated by the 2 authors were resolved through discussion with a third reviewer. Scores on the PEDro scale are obtained by summing the ratings of items 2 to 11, resulting in a total score ranging from 0 to 10. 35 Scores less than 4, between 4 and 5, between 6 and 8, and between 9 and 10 are categorized as poor, fair, good, and excellent, respectively. 35 Despite the variation in PEDro score, all articles were included in this review to ensure a comprehensive analysis.
A network meta-analysis compares 3 or more interventions simultaneously by integrating direct and indirect analyses across a network of studies. 36 This analytical approach provides estimates of the relative effects of any pair of interventions within the network and often yields more precise estimates than do single direct or indirect analyses. 36 Additionally, a network meta-analysis can rank various interventions on the basis of their relative effects. 36 For our study, we utilized ShinyNMA (version 1.01; https://jerryljw.shinyapps.io/ShinyNMA_/), a freely accessible online cloud computing network meta-analysis tool. 37 ShinyNMA enables the creation of charts in accordance with the latest PRISMA 2020 guidelines 32 and synthesizes results while guiding the selection of R software packages (version 4.1.0), such as metafor (version 2.4-0), netmeta (version 1.3-0), and BUGSnet (version 1.0-4).
We extracted continuous data by adjusting baseline measurements. For studies that did not report standard deviations, we either requested the necessary data from the study authors or calculated correlation coefficients by following the guidelines outlined in the Cochrane Handbook for Systematic Reviews of Interventions. 36 Utilizing a random-effects model, we conducted head-to-head comparisons of various rTMS and TBS protocols for poststroke hemineglect, and the standard mean difference (SMD) with its 95% confidence interval was estimated. Additionally, we assessed the distribution of probabilities of effectiveness for each rTMS and TBS protocol and stimulation site. To rank the treatments, we employed the P score, which measures the certainty that a treatment is superior to others, averaged across all competing treatments. 38 The P score ranges from 0 (lowest) to 1 (highest), with a higher score indicating greater certainty that 1 treatment is superior to another. 38 Furthermore, we evaluated network inconsistency by examining loop-specific heterogeneity and local incoherence estimates as well as by comparing differences in effect sizes between standard meta-analyses (direct comparisons) and indirect comparisons. 36 To assess clinical meaningfulness, we used SMDs calculated using Cohen’s d statistic. SMDs of <0.2, 0.2 to 0.5, 0.5 to 0.8, and >0.8 were interpreted as indicating clinically meaningless, small, moderate, and large effects, respectively. 39
Results
We initially identified 81 RCTs and then excluded 30 duplicates. After title and abstract screening, a further 21 studies that did not meet the inclusion criteria were excluded. Screening the full texts of the remaining 30 studies resulted in the exclusion of 6 that were not peer-reviewed, 2 that did not focus on rTMS or TBS, 4 study protocols, 1 study focusing on the same participants as included in another study, 1 dose–control study, and 2 studies for which no data were available. Finally, our network meta-analysis included 13 articles involving a total of 309 participants (Figure 1).40-52
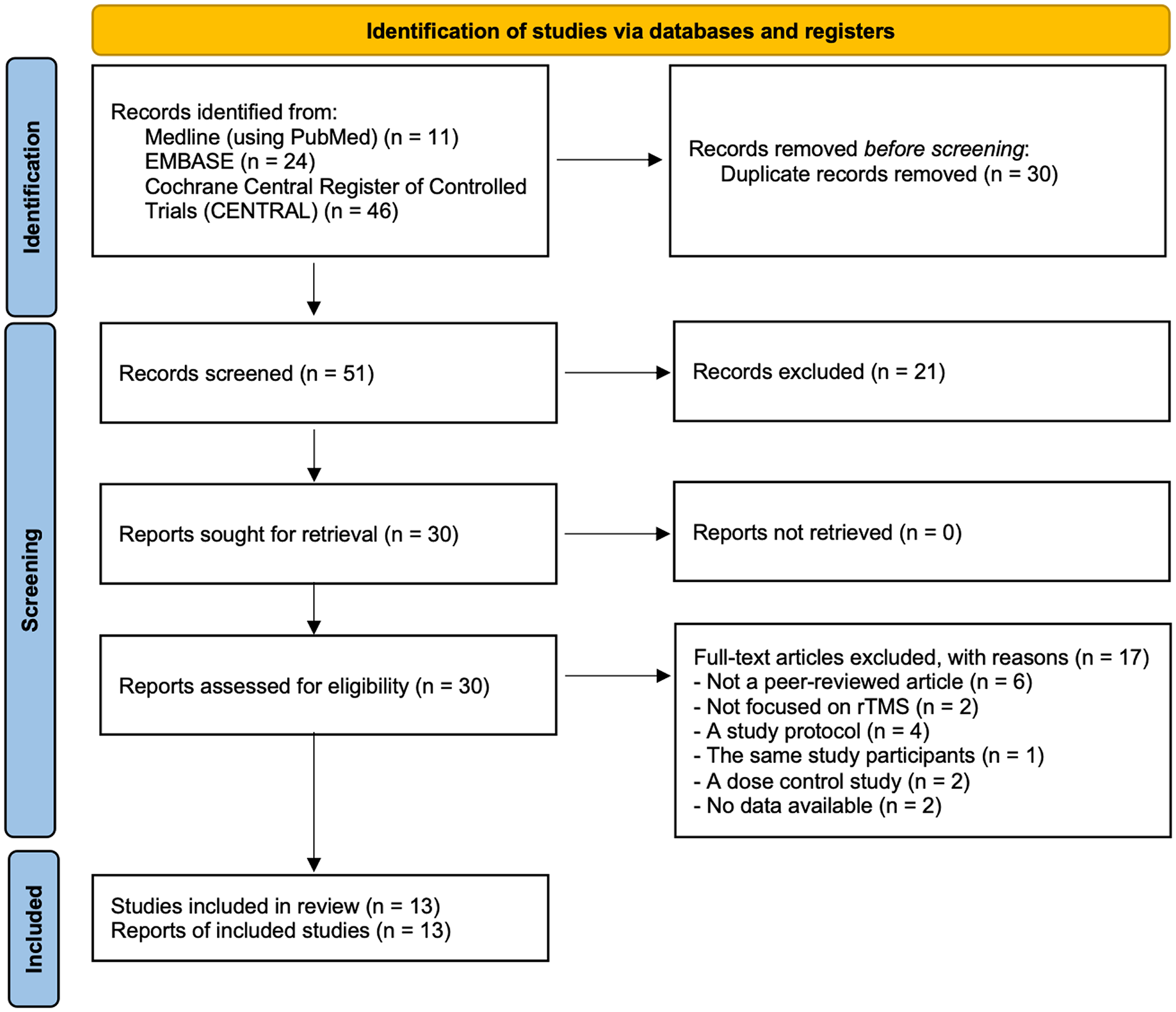
Article selection process.
Of the 13 included RCTs,40-50,52 12 were parallel RCTs40-50,52 and 1 was a crossover study. 51 According to the guidelines outlined in the Cochrane Handbook for Systematic Reviews of Interventions, including crossover studies in a network meta-analysis is acceptable. 36 In our network meta-analysis, we included the final outcome data rather than only the outcome data from the first period (before the crossover). All studies included participants who had experienced right hemisphere stroke.40-52 The included studies employed the following protocols: cTBS to the contralesional site,40,42,45,46,50,51 HF-rTMS to the contralesional site, 45 HF-rTMS to the lesional site, 49 LF-rTMS to the contralesional site,41,43,45,48,49,52 and LF-rTMS to the lesional site.44,47 Conventional rehabilitation therapy was employed in each group.40-52 Kim et al 49 conducted a 3-arm study comparing HF-rTMS, LF-rTMS, and sham stimulation. Yang et al 45 conducted a 4-arm study comparing HF-rTMS, LF-rTMS, cTBS, and sham stimulation. All the included studies conducted assessments at the end of the intervention,40-52 along with additional postintervention assessments at 3 weeks in 1 study, 51 1 month in 4 studies,43,45,46,50 and 3 months in 1 study. 41 A summary of the main characteristics of the 13 included RCTs is presented in Table 1.
Characteristics of Selected Randomized Controlled Trials.
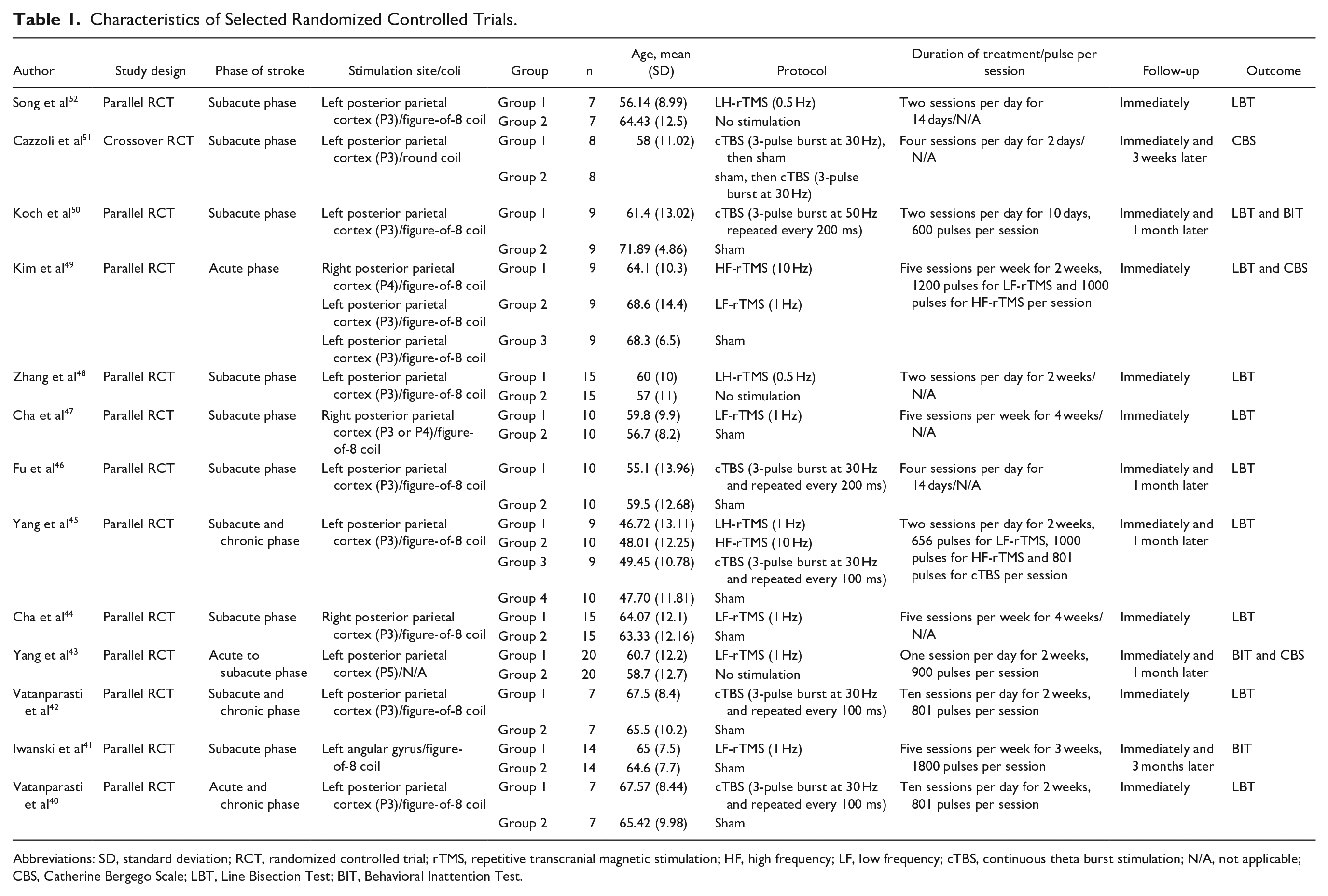
Abbreviations: SD, standard deviation; RCT, randomized controlled trial; rTMS, repetitive transcranial magnetic stimulation; HF, high frequency; LF, low frequency; cTBS, continuous theta burst stimulation; N/A, not applicable; CBS, Catherine Bergego Scale; LBT, Line Bisection Test; BIT, Behavioral Inattention Test.
The quality of the included RCTs was independently assessed using the PEDro scale. All included studies had a PEDro score between 5 and 8, with 1 study having fair quality 48 and the remaining 12 studies having good quality.40-47,49-52 The detailed results of the risk of bias assessment are listed in Supplemental Table 1.
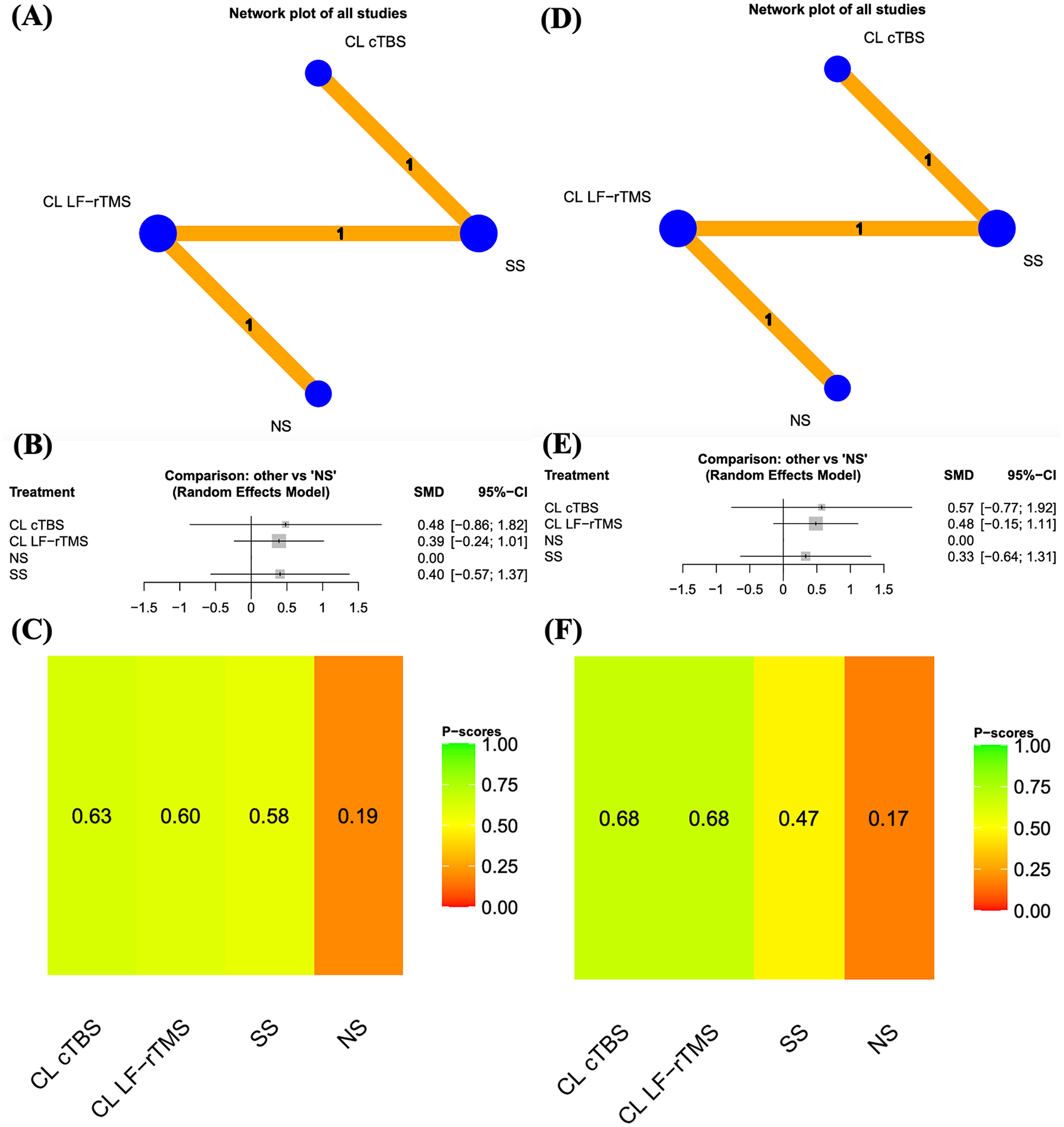
Figure 2A depicts a network diagram illustrating the effects of rTMS protocols on the line bisection test results in the immediate assessment. The pooled SMDs of the rTMS protocols revealed that HF-rTMS to the lesional site and LF-rTMS to the contralesional site were significantly more effective than was no stimulation (Figure 2B). Furthermore, we conducted separate analyses of head-to-head studies to determine differences between rTMS protocols. Supplemental Table 2 presents the results of pairwise meta-analysis and network meta-analysis of the short-term line bisection test results achieved with various rTMS protocols. Additionally, we analyzed the distribution of probabilities of effectiveness for each rTMS protocol; ultimately, the rTMS protocols were ranked from the most to the least effective, as follows: HF-rTMS to the lesional site, LF-rTMS to the lesional site, LF-rTMS to the contralesional site, HF-rTMS to the contralesional site, cTBS to the contralesional site, sham stimulation, and no stimulation (Figure 2C).
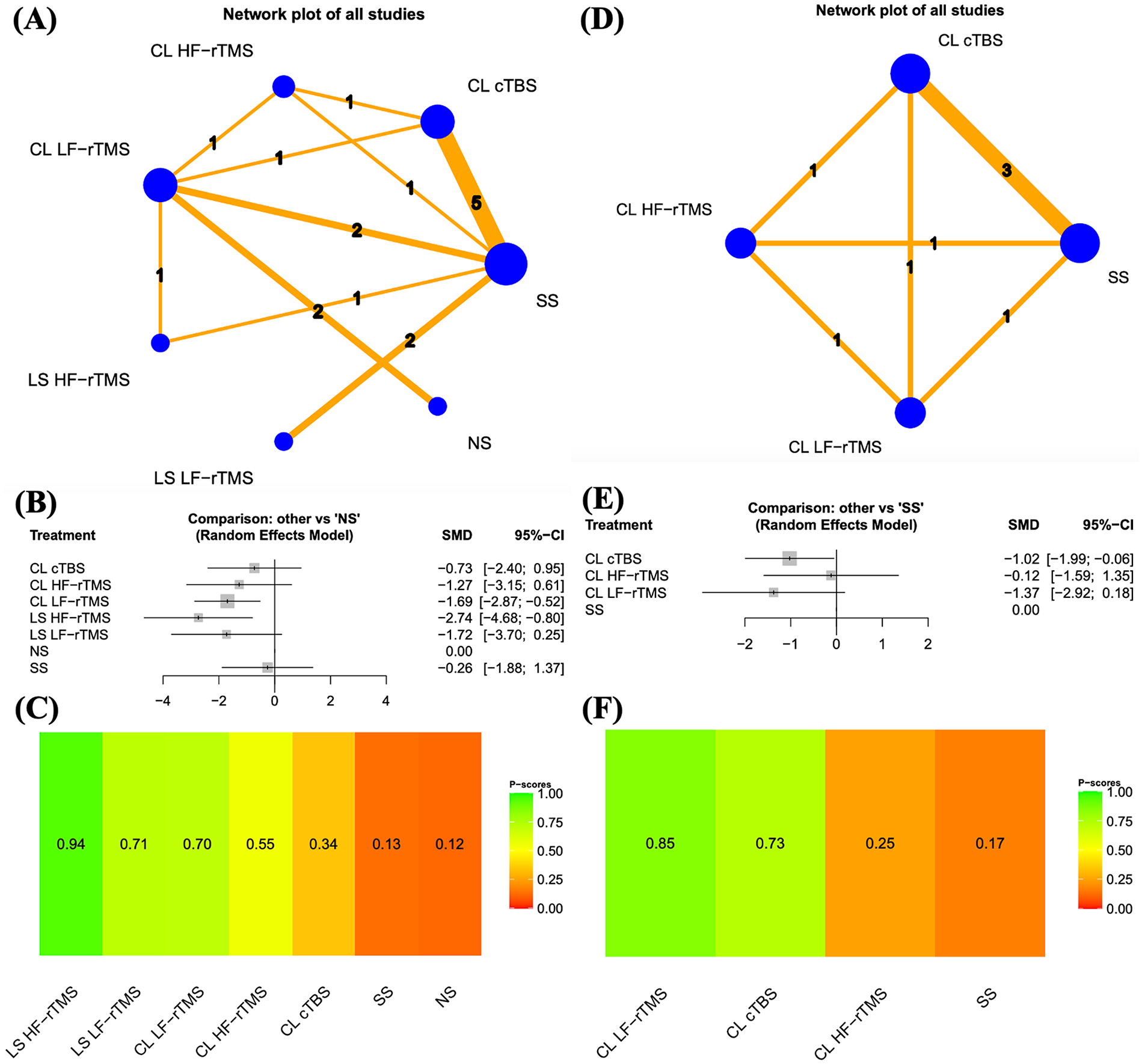
Results of the line bisection test. (A) Network plots of all studies in immediate assessment. (B) Forest plots of all results in immediate assessment. (C) Distribution of probabilities of effectiveness for each rTMS protocol in immediate assessment. (D) Network plots of all studies in long-term assessment. (E) Forest plots of all results in long-term assessment. (F) Distribution of probabilities of effectiveness for each rTMS protocol in long-term assessment. The node size, edge width, and numbers above the lines all represent the number of studies. In the forest plot, the left side indicates a favoring of the intervention.
Our network plot (Figure 2A) comprised 4 triangle loops (connecting LF-rTMS to the contralesional site and HF-rTMS to the lesional site and sham stimulation; LF-rTMS to the contralesional site and HF-rTMS to the contralesional site and cTBS to the contralesional site; cTBS to the contralesional site and sham stimulation and LF-rTMS to the contralesional site; and LF-rTMS to the contralesional site and HF-rTMS to the contralesional site and sham stimulation). A loop-specific heterogeneity test revealed no significant inconsistency in the results of direct and indirect comparisons (Supplemental Table 3).
We assessed the results of the Catherine Bergego Scale and Behavioral Inattention Test for the immediate assessment of our secondary outcomes (Figures 3 and 4 and Supplemental Tables 4 and 5). The pooled SMD of the Catherine Bergego Scale score revealed that HF-rTMS to the lesional site was significantly more effective than was no stimulation (Figure 3B). We also examined the probabilities of effectiveness on the basis of the results of the Catherine Bergego Scale for immediate assessment in all rTMS protocols. The rTMS protocols were ranked from the most to the least effective, as follows: HF-rTMS to the lesional site, LF-rTMS to the contralesional site, no stimulation, cTBS to the contralesional site, and sham stimulation (Figures 3C and 4).
Results of the Catherine Bergego Scale. (A) Network plots of all studies in immediate assessment. (B) Forest plots of all results in immediate assessment. (C) Distribution of probabilities of effectiveness for each rTMS protocol in immediate assessment. The node size, edge width, and numbers above the lines all represent the number of studies. In the forest plot, the left side indicates a favoring of the intervention.
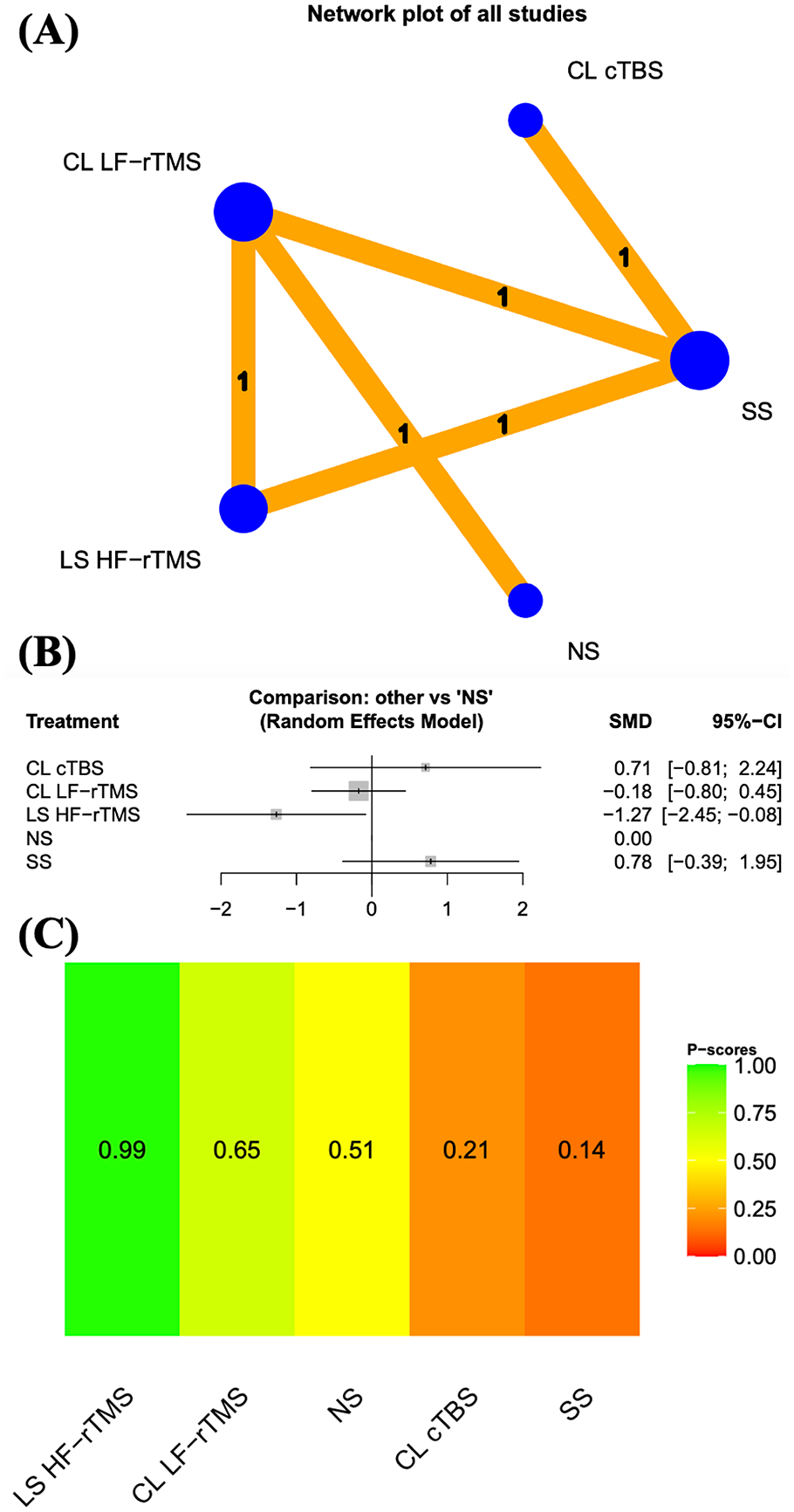
Results of the Behavioral Inattention Test. (A) Network plots of all studies in immediate assessment. (B) Forest plots of all results in immediate assessment. (C) Distribution of probabilities of effectiveness for each rTMS protocol in immediate assessment. (D) Network plots of all studies in long-term assessment. (E) Forest plots of all results in long-term assessment. (F) Distribution of probabilities of effectiveness for each rTMS protocol in long-term assessment. The node size, edge width, and numbers above the lines all represent the number of studies. In the forest plot, the right side indicates a favoring of the intervention.
We also assessed the effects of rTMS protocols on the results of the line bisection test and Behavioral Inattention Test obtained from the longest follow-up period (Figures 2 and 4 and Supplemental Tables 6–8). Figure 2D presents a network diagram illustrating the effects of the rTMS protocols on the line bisection test results obtained from the longest follow-up. The pooled SMDs of the rTMS protocols revealed that cTBS to the contralesional site was significantly more effective than was sham stimulation (Figure 2E). Furthermore, we conducted separate analyses of head-to-head studies to identify differences between rTMS protocols. Supplemental Table 6 provides the results of pairwise meta-analysis and network meta-analysis of the line bisection test results achieved with various rTMS protocols. Additionally, we analyzed the distribution of probabilities of effectiveness for each rTMS protocol. The rTMS protocols were ranked from the most to the least effective, as follows: LF-rTMS to the contralesional site, cTBS to the contralesional site, HF-rTMS to the contralesional site, and sham stimulation (Figure 2F). Our network plot (Figure 2D) comprises 4 triangle loops: cTBS to the contralesional site, HF-rTMS to the contralesional site, and LF-rTMS to the contralesional site; HF-rTMS to the contralesional site, LF-rTMS to the contralesional site, and sham stimulation; LF-rTMS to the contralesional site, sham stimulation, and cTBS to the contralesional site; and sham stimulation, cTBS to the contralesional site, and HF-rTMS to the contralesional site. A loop-specific heterogeneity test revealed no significant inconsistency in the results of direct and indirect comparisons (Supplemental Table 7).
Of the 13 included RCTs, 7 studies examined adverse events.42,43,46,49-52 Of these, 1 study documented 2 participants experiencing mild headaches during cTBS stimulation. 46 The other studies did not report any adverse events throughout the procedure.42,43,49-52 This result suggests that the interventions were well tolerated by the participants.
Discussion
rTMS is a noninvasive treatment that precisely influences neural functions in specific cortical areas. 49 Through the rTMS equipment, a powerful current is delivered, and this current generates a magnetic field.45,53 The rapidly changing magnetic field induces an electric field that stimulates neurons or modifies the resting membrane potential in the underlying cortex.53,54 Research has demonstrated that LF stimulation (<1 Hz, LF-rTMS) of the cerebral cortex has inhibitory effects, whereas HF stimulation (>5 Hz, HF-rTMS) enhances cortical activity.43,45,55,56 cTBS exerts inhibitory effects by promoting long-term depression through continual stimulation consisting of either 300 pulses lasting 20 s each or 600 pulses lasting 40 s each.50,57
Our comprehensive analyses revealed that HF-rTMS targeting the lesional site and LF-rTMS targeting the contralesional site resulted in significant amelioration of hemineglect severity, which was quantified using the line bisection test and indicated by the results of immediate assessment. Our ranking probability analysis identified HF-rTMS at the lesional site as the optimal intervention strategy. Furthermore, HF-rTMS at the lesional site was found to enhance the performance of activities of daily living, as appraised by the Catherine Bergego Scale and as revealed by immediate assessment. However, regarding long-term outcomes, only cTBS applied to the contralesional site was found to be efficacious for mitigating the severity of hemineglect, as determined by the line bisection test. No study has yet conducted a long-term follow-up of HF-rTMS at the lesional site. All statistically significant findings also demonstrated clinical significance, as indicated by SMD values exceeding 0.8, representing a large effect. When compared to the individual RCTs included, the effect size of our findings correlates with each study. On the basis of these robust findings, we advocate for HF-rTMS at the lesional site as the preferred therapeutic modality for poststroke hemineglect in the short term, with LF-rTMS at the contralesional site as a practical alternative. Moreover, cTBS at the contralesional site is a viable treatment option because of its long-term effect.
Recent evidence-based guidelines provide a recommendation with applying cTBS to the contralesional left posterior parietal cortex, using 30 or 50 Hz with 2 or 4 trains per session. 58 No further recommendations are given for other protocols. To provide the most up-to-date clinical evidence, we employed a network meta-analysis method, which allows for the simultaneous comparison of 3 or more interventions by integrating direct and indirect evidence across a network of studies. 36
Based on our analyses, we recommend HF-rTMS at the lesional site as the first-line treatment for poststroke hemineglect in the short term, as it improves both the severity of the condition and performance in activities of daily living. This approach is grounded in the neuroplasticity model, where excitatory stimulation at the lesional site promotes adaptive neural reorganization in response to brain injury. The protocol used in the included study was 10 Hz rTMS over the right posterior parietal cortex (P4), administered in 5 sessions per week for 2 weeks. 49
An alternative approach involves LF-rTMS at the contralesional site, which has also been shown to improve poststroke hemineglect in the short term. This method is based on the interhemispheric competition model, which suggests that stroke causes an imbalance in neural activity between the hemispheres. Protocols for LF-rTMS varied, with frequencies of 0.5 or 1 Hz applied over the left posterior parietal cortex (P3 or P5), 1 or 2 sessions per day for 2 weeks.41,43,45,48,49,52
For long-term management, cTBS at the contralesional site may be an effective option, as it has been shown to improve the severity of poststroke hemineglect. The mechanism is similar to that of LF-rTMS at the contralesional site, relying on the interhemispheric competition model. The protocols for cTBS involved 3-pulse bursts at 30 or 50 Hz, repeated every 100 or 200 ms, with 2, 4, or 10 sessions per day for 2 weeks over the left posterior parietal cortex (P3).40,42,45,46,50,51
This study has several strengths. First, this is the first network meta-analysis of RCTs exploring the effects of various rTMS and TBS protocols at distinct stimulation sites in participants with poststroke hemineglect. Second, to identify relevant RCTs, we employed broad inclusion criteria, searched major databases, and imposed no language restrictions. Third, according to PEDro scores, the quality of the included RCTs was mainly good. Finally, no significant inconsistencies were discerned in the results of direct and indirect comparisons, which is indicative of favorable coherence.
This study also has several limitations. First, the rTMS and TBS treatment regimens varied between studies, making it challenging to offer a definitive recommendation regarding the most effective treatment regimen. Second, long-term follow-up is lacking, with the longest follow-up duration being only 3 months after the end of the intervention. Third, few studies focused on certain rTMS and TBS protocols, which posed challenges for conducting further analyses. Fourth, although the risk of bias was generally deemed low, the lack of blinding among participants or therapists in most of the studies (due to the nature of the interventions) is noteworthy. Fifth, the included studies involved and combined different phases of stroke—acute, subacute, and chronic—as well as different types of stroke, including both ischemic and hemorrhagic, making it challenging to perform further analysis based on these characteristics.
There are several directions for future studies. First, more specific treatment protocols, such as stimulation site, frequency, dosage, and treatment sessions, should be assessed. Second, long-term follow-up data could be established to evaluate the sustained effects of rTMS or TBS. Third, studies could focus on more specific participant groups, such as narrowing down to a single phase or type of stroke. Overall, to address these limitations, high-quality, large-scale, and better-designed RCTs are needed.
This systematic review and network meta-analysis of current RCTs aimed to ascertain the effects of rTMS and TBS on poststroke hemineglect. Our findings indicate HF-rTMS at the lesional site should be the preferred therapeutic approach for the short-term management of poststroke hemineglect, with LF-rTMS at the contralesional site as a practical alternative. Moreover, cTBS at the contralesional site is a viable option for the long-term management of poststroke hemineglect. However, to corroborate the benefits of these interventions, high-quality and large-scale RCTs with longer follow-ups and investigating various stimulation sites and rTMS and TBS protocols are necessary.
Supplemental Material
sj-docx-1-nnr-10.1177_15459683241309572 – Supplemental material for Effects of Repetitive Transcranial Magnetic Stimulation on Poststroke Hemineglect: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials
Supplemental material, sj-docx-1-nnr-10.1177_15459683241309572 for Effects of Repetitive Transcranial Magnetic Stimulation on Poststroke Hemineglect: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials by Fu-An Yang, Chueh-Ho Lin, Hung-Ning Chung, Yi-Chun Kuan, Reuben Escorpizo and Hung-Chou Chen in Neurorehabilitation and Neural Repair
Supplemental Material
sj-docx-2-nnr-10.1177_15459683241309572 – Supplemental material for Effects of Repetitive Transcranial Magnetic Stimulation on Poststroke Hemineglect: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials
Supplemental material, sj-docx-2-nnr-10.1177_15459683241309572 for Effects of Repetitive Transcranial Magnetic Stimulation on Poststroke Hemineglect: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials by Fu-An Yang, Chueh-Ho Lin, Hung-Ning Chung, Yi-Chun Kuan, Reuben Escorpizo and Hung-Chou Chen in Neurorehabilitation and Neural Repair
Supplemental Material
sj-docx-3-nnr-10.1177_15459683241309572 – Supplemental material for Effects of Repetitive Transcranial Magnetic Stimulation on Poststroke Hemineglect: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials
Supplemental material, sj-docx-3-nnr-10.1177_15459683241309572 for Effects of Repetitive Transcranial Magnetic Stimulation on Poststroke Hemineglect: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials by Fu-An Yang, Chueh-Ho Lin, Hung-Ning Chung, Yi-Chun Kuan, Reuben Escorpizo and Hung-Chou Chen in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
This manuscript was edited by Wallace Academic Editing.
Author Contributions
Fu-An Yang: Conceptualization; Data curation; Resources; and Writing—original draft. Chueh-Ho Lin: Methodology. Hung-Ning Chung: Formal analysis. Yi-Chun Kuan: Software. Reuben Escorpizo: Project administration. Hung-Chou Chen: Conceptualization and Writing—review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.