
Abstract
Introduction
Stroke is a major cause of adult neurological disability in North America, often resulting in significant muscle atrophy and weakness, mobility, and functional limitations as well as cardiorespiratory deconditioning that may adversely affect independence and quality of life.1-4 Epidemiological studies have consistently demonstrated an inverse association between both lean mass and muscle strength with all-cause mortality in healthy and chronic disease populations.5-10 Low cardiorespiratory fitness is also established as a strong predictor of cardiovascular disease risk and all-cause mortality, independent of age and other risk factors,11-15 and is associated with higher stroke risk.16,17 Given the positive effect that exercise can have on these sequelae, determining an optimal exercise strategy that will have the greatest impact on stroke recovery merits special attention. The American Heart Association (AHA) Scientific Statement for Physical Activity and Exercise Recommendations for Stroke Survivors first supported the prescription of both aerobic and resistance training (AT+RT) in 2004. 18 More recently, AT+RT has been recommended by the AHA/American Stroke Association Guidelines for Adult Stroke Rehabilitation and Recovery as a Class IIA, level A recommendation for recovery of gait capacity and gait-related mobility tasks. 19 However, the research focus has largely been on examining the effect of AT or RT alone, or to a lesser extent combined AT+RT, but in the absence of an AT exercise comparison group. 20 No study to date has shown that AT+RT benefits body composition or other functional and metabolic outcomes over standard-of-care AT treatment. Indeed, 1 short-term study (6 weeks) and 1 underpowered study of 12 participants per group failed to show a significant difference in 6-minute walk distance (6MWD) between AT and AT+RT groups.21,22
Nonetheless, AT and RT have the potential to mitigate stroke impairments, albeit via different mechanisms. Whereas AT provides the greatest cardiorespiratory fitness stimulus, RT may intensify the effects of AT by augmenting muscular strength and accretion of lean mass.23-26 Skeletal muscle atrophy and associated muscle weakness in both affected and nonaffected limbs is well documented poststroke27,28 and is associated with a lower metabolic rate, which can lead to gains in fat mass 29 and independently contributes to diminished exercise performance (VO2peak) in individuals with stroke and healthy individuals.30,31 Furthermore, the ability to perform day-to-day activities such as walking and stair climbing, and sit-to-stand performance depends in part on muscular strength, with up to 50% of the variance in gait performance accounted for by affected-side leg strength.3,32,33 These findings suggest that muscular strength and cardiorespiratory fitness are interrelated and that increasing muscle mass and strength poststroke may increase the response to aerobic conditioning and confer a possible mortality advantage. Surprisingly, exercise strategies that counteract the loss of lean muscle mass and strength poststroke have been rarely examined. 20
In spite of suggested benefits of combining RT and AT, there is presently no compelling evidence that RT combined with AT is more effective in enhancing poststroke physical recovery than AT alone. To address this important question, we compared AT+RT versus AT in a poststroke population after a 6-month exercise program using mobility, function, body composition, muscular strength, and cardiorespiratory fitness outcome measures. This article serves as an exploratory analysis of secondary outcomes that also has some utility as hypothesis generating.
Methods
Participants and Study Design
This was a 24-week randomized clinical trial. The study was conducted from April 2013 through February 2016. Participants (n = 73) referred to Toronto Rehabilitation’s Risk Factor Modification and Exercise Program following Stroke (TRI-REPS) were randomly assigned to AT (5 d/wk) or combined AT+RT (AT and RT 2 d/wk). A staff member uninvolved in the study and blinded to the possible training options assigned participants using a random number generator (random.org) to a treatment group. All study outcomes, except for muscular strength, were measured by an assessor blinded to treatment group. To reduce cross-contamination, the 2 treatment groups attended separate classes led by different case managers. Case Managers were Registered Kinesiologists with at least 8 years of experience prescribing exercise to people following stroke. The Case Managers had biweekly meetings to ensure consistency in AT prescription and progression. All other program components, including 13 educational sessions related to stroke recovery, were the same. The Toronto Rehabilitation Research Ethics Board approved the study. All participants gave informed consent. The results herein represent analyses of secondary outcomes from a study designed to measure cognition.
Participants were individuals living in the community following a hemorrhagic or ischemic stroke, referred from outpatient stroke rehabilitation programs, primary care physicians, and stroke specialists. Inclusion criteria were the following: (1) ability to walk at least 100 m independently with/without an assistive device with no severe limitations caused by pain, (2) living in the community at least 10 weeks poststroke with a stroke-related motor impairment score of <7 on the Chedoke-McMaster Stroke Assessment Scale (CMSA) of the leg or foot, 34 (3) no severe communication problems, and (4) no severe cardiovascular morbidities that would limit exercise.
Exercise Intervention
Supervised exercise training was performed once per week at the center for 6 months with the balance of the exercise conducted in the home/community, which has been proved to be both feasible and effective.35,36 AT was prescribed 5 times/wk to all participants in the first 1 to 3 weeks, after which the AT+RT group replaced 2 AT sessions with 2 RT sessions. Both AT and RT components were completed during the weekly supervised session. Meanwhile, the AT group continued with 5 AT sessions per week for the duration of the program. All participants received the same education session on “active living,” where they were encouraged to reduce prolonged sitting time in addition to completing prescribed preplanned exercise. All participants were trained to measure resting and exercise heart rates (HRs) and complete exercise diaries. Accuracy of HR measurement was checked at weekly visits to the center.
Aerobic Training Component
Walking overground was the primary mode of AT prescribed. For those unable to maintain the target training HR for ≥5 to 10 minutes during walking, a combination of modalities was used (walking with stationary recumbent/upright cycling). AT intensity was based on cardiopulmonary exercise test (CPET) results conducted at baseline and 3 months. The goal was to progress participants to 20 to 60 minutes of exercise, 5 times/wk. 37 The HR that occurred at the oxygen uptake at the ventilatory threshold (VO2VT) during the CPET was used to prescribe exercise intensity. 38 In the absence of a discernable VO2VT a combination of the following was used: 60% to 80% of HR reserve or peak oxygen uptake (VO2peak) and/or rating of perceived exertion (RPE) of 12 to 16 (somewhat hard to hard) on the Borg 39 6 to 20 Scale. 37 Owing to the reliance on the relationship between HR with VO2VT and VO2peak in prescribing exercise, the CPET was conducted at approximately the same time of day as the exercise class to control for HR-altering medications. AT routes close to the participants’ home were mapped out and a hard copy provided.
Prescriptions were initially progressed by increasing duration to ≥20 minutes and then increasing intensity to target HR (maximal duration 60 minutes). Thereafter, training intensity was adjusted based on the midpoint CPET. Exercise diary information, HRs measured at the center, and communication with the participant assisted the case manager in deciding when to increase the prescription. Whereas progression of exercise was individualized, duration or intensity was increased approximately every 1 to 3 weeks. First, patients were progressed to 20 to 30 minutes of exercise prior to increasing the intensity, although some patients were ready for an earlier adjustment to intensity. The magnitude of each increase in duration and intensity was relative to the patients’ initial prescription. In general, exercise intensity was progressed by 0.2 to 0.3 km/h increments or distance by 200 to 800 m every 1 to 3 weeks. After completion of at least 4 weeks of continuous moderate-intensity aerobic exercise, higher-intensity interval training was considered when a faster pace did not preclude safety. This was conducted on a stationary cycle or by walking overground and was characterized by short periods (15 to 30 s) of increased exercise intensity (RPE ≥17) alternating with longer periods of lower-intensity exercise (1 to 2 minutes) for 20 minutes. The first interval included a gradual ramping up in speed/resistance. The number of intervals was gradually increased over time. Higher-intensity interval training was prescribed 2 times per week on nonconsecutive days, and moderate-intensity continuous exercise was continued 3 times per week with progression as indicated.
Resistance Training Component
An RT program was designed for the AT+RT group in the second supervised session. When the participant could perform the exercises with good technique (typically after 2-3 supervised sessions), they were provided with an instruction booklet, exercise bands, and dumbbells to continue the program at home. The exercises were determined by strength and range-of-motion assessments as well as gait analysis by observation. The exercises were task specific, with both multijoint exercises for incorporating muscle actions that are performed during daily activities and single-joint exercises to target specific muscle actions. Most participants were prescribed 1 to 2 sets of 10 to 11 exercises: lunge, squat, abdominal curl-up, heel raise, bicep curl (dumbbell), supine triceps extension (dumbbell), affected-side hip flexion/extension (elastic band), affected-side ankle dorsiflexion (elastic band), and single-limb knee extension and flexion (fixed-weight machines at the center and elastic band at home), although some required modification or replacement.
Participants were initially prescribed a weight load equivalent to 50% to 60% of 1 repetition maximum (1RM) and/or a resistance rated as 14 to 16 on the 6 to 20 RPE scale 39 on the last repetition of the set. Subsequent 1RM testing procedures occurred at weeks 7, 14, and 21, where the weight load was readjusted to 70% of 1RM.37,40 Between 1RM testing, participants gradually progressed from 10 to 15 repetitions and then increased resistance by 1.6 to 5 kg or 1 exercise band level and then reduced repetitions to 10 and repeated this process. Progression of movement velocity during concentric contractions to optimize dynamic muscle strength was introduced after at least 8 weeks of training for squat, lunge, hip flexion/extension, ankle dorsiflexion, and heel raise exercises. In addition, a series of progression exercises for squat, lunge, abdominal curl-up, and heel raises were prescribed (eg, from double-leg heel raise on a flat surface to double-leg heel raise on stair, to single-leg heel raise on stair, and then to maximal velocity in the concentric phase). Also, exercises that initially relied on the patients’ body mass as resistance were progressed by adding an external weight load (ie, dumbbell[s] in a knapsack).
The 1RM test was performed on ≥3 of 10 to 11 exercises (bicep curl, triceps extension, leg curl, leg extension) on affected and nonaffected sides separately. After 3 repetitions of a warm-up weight, a slightly heavier weight was attempted once following a 2-minute recovery period. One repetition at a heavier weight was attempted every 2 minutes until the participant was unable to lift the weight with proper technique.
Descriptive Measures
The National Institutes of Health Stroke Scale 41 (maximum score 42, most severe stroke-related neurological deficits) and the Montreal Cognitive Assessment scores were measured at baseline. 42 Motor recovery stage of the leg and foot of the stroke-affected side was classified on the CMSA Scale. 34
Outcome Measures
Cardiorespiratory Fitness
As described elsewhere, 43 a symptom-limited CPET was performed on a semirecumbent cycle ergometer with specialized pedals to secure feet (Ergoline, Ergoselect 1000, Blitz, Germany), upright cycle (Ergoselect 200P, Germany), or a treadmill depending on balance and ability to control the leg/foot position in pedals. The CPET was conducted on the same modality on subsequent assessments and at the same time of day as the supervised exercise class to minimize effects of HR-altering medication on exercise prescription. Breath-by-breath gas samples were collected via a calibrated metabolic cart (SensorMedics Vmax Encore, San Diego, CA) to determine VO2peak (mL kg−1 min−1). Twelve-lead ECG, RPE, and blood pressure were monitored throughout. VO2peak was calculated as the highest 20-s average recorded during the CPET. 44 The expected VO2peak (mL kg−1 min-1) was calculated from established age and sex norms. 45
VO2VT was determined by a combination of the V-slope method and the ventilatory equivalents methods, 46 as previously described.43,47 The V-slope method was defined as the point of departure from linearity of carbon dioxide output plotted against oxygen uptake. The ventilatory equivalent method was defined as the level corresponding to the rise in ventilatory equivalent of oxygen that occurs when the ventilatory equivalent of carbon dioxide remains relatively constant. The VO2VT is considered a valid measure, demonstrating high interrater reliability in the stroke population. 48 VO2VT was determined by 2 independent assessors blinded to group assignment. The final VO2VT was the average from the 2 assessors if their values were within <10%, otherwise they were resolved by consensus. The VO2VT was discernible at both baseline and 6 months in 26 (74.3%) and 25 (75.8%) of the AT and AT+RT participants, respectively.
Body Composition and Dietary Assessment
Total body and regional measurements of lean soft-tissue mass (kg) and percentage fat were acquired by dual-energy X-ray absorptiometry (DXA, Hologic Discovery W Densitometer, Hologic, Inc [Model QDR 4500W]) by an International Society for Clinical Densitometry certified technologist blinded to group allocation. Whole body scans were acquired and analyzed in a fasting, hydrated, and rested state using commercially available Hologic software (version 13.4.1:5 Auto Whole Body). All scans were completed at the same time of day and using the same densitometer, and quality control checks were completed daily and weekly as indicated by the manufacturer. Each participant completed a 1-day food log at baseline and 6 months. Records were analyzed using Nutritionist Pro, software version 4.3.0, Axxya Systems LLC (Stafford, TX).
Maximal Isometric Strength
Two 3-s trials (2 minutes rest between trials) of maximal isometric strength of the affected and nonaffected side knee extensor and elbow flexor muscle groups were measured with a calibrated hand-held force gauge dynamometer (DFE-500; Chatillon-Ametek, Largo, FL) as previously described. 36 The highest force was recorded. The reliability and precision of hand-held dynamometer measurements has been established for people with stroke, and moderate to strong correlations with isokinetic measures have been demonstrated in neuromuscular disease. 49 Isometric assessments do not pose a limitation for those with restricted range of motion, mitigates the advantage of 1RM testing to the AT+RT group owing to similarity to the prescribed exercises, and does not encourage RT participation in the AT group.
Six-Minute Walk Test
This test measures the distance that an individual can quickly walk in a period of 6 minutes on a 30-m course according to standardized instructions. 50 Participants used gait aids if they were prescribed. Participants completed 2 6MWD tests on the same day, with 15 minutes’ rest between trials at baseline and 1 assessment at study completion. Data from the longest distance achieved were used for analysis. The expected 6MWD was calculated from age and sex norms. 51
Sit-to-Stand and Stair Climb Performance
Instructions were provided to stand fully from a 43-cm-high chair 5 times as quickly as possible and not to touch the back of the chair. Climb performance was measured as time to ascend 4 stairs as quickly as possible. The faster time (in seconds) of 2 trials, 2 minutes apart was recorded for both outcomes. Hand and railing support was standardized.
Exercise Logs
Participants were required to keep a detailed record of each exercise session, noting the precise distance walked, duration (walk/cycle), and resting and peak HR. RT records included the amount of weight lifted and number of repetitions and sets performed for each workout. This log was submitted and cross-validated by the case manager at weekly visits to the center.
Adherence to Exercise, Exercise Performance, and Adverse Event Reporting
Indices of exercise adherence were determined by the following: (1) attendance at prescheduled sessions and proportion of prescribed AT and RT sessions recorded on the exercise log, (2) mean of immediate post-AT exercise HR measured by a staff member at 3 consecutive weekly classes (to account for the effects of HR-altering medications) and mean of immediate postexercise HR recorded on the exercise log by the participant over 3 weeks both at baseline and end of intervention (reported relative to the baseline and 24-week VO2VT HR), and (3) adherence to weight load prescribed as reported on the exercise log, relative to percentage of 1RM performed at baseline and 21 weeks. Adverse events that were related or possibly related to participation in the exercise program or that suggested a potential increase in risk or harm to research participants or to others were recorded.
Statistical Analyses
This study was an analyses of secondary outcome measures, and we estimated that a sample size of ≥32 participants per group would provide 80% power to detect a mean (±SD) clinically important difference in 6MWD between groups of 30 ± 45 m, 52 at an α level of .05.
There is no established magnitude of change in lean mass that is predictive of clinically meaningful outcomes. However, a sample size of ≥33 participants per group would be sufficient to detect a 1.0 ± 2 kg difference between groups in lean mass as previously demonstrated in similar studies of cardiac rehabilitation participants.24,25 Differences between the groups at baseline were assessed using independent-sample Student’s t tests for continuous variables and χ2 tests or Fisher’s exact tests for categorical variables. Student’s t test for paired samples was used to determine within-group changes from baseline to posttraining. Between-group differences were analyzed using 2-way analysis of variance for repeated measures. In a sensitivity analysis based on post hoc observation, we adjusted for baseline measures that were imbalanced between the groups and had biological relevance. These included the National Institutes of Health Stroke Scale (NIHSS) score, elapsed time from stroke to start of the exercise intervention, and age. NIHSS scores are broadly predictive of clinical outcomes 1 year poststroke. 53 Normal Gaussian distributions of the data were verified by the Kolmogorov-Smirnov test. Variables that were not normally distributed were log-transformed to approximate normal distribution. All analyses were performed in SPSS (version 24.0, SPSS, IBM Corporation, Armonk, NY).
Results
Participants
A total of 73 participants were enrolled in the study, representing 60% of the people who were referred to the TRI-REPS program (Figure 1). Of these, 37 people were randomized to the AT group and 36 randomized to AT+RT. Overall, 93.2% of participants (n = 68) completed the study. Two people dropped out of the AT group (both had strokes unrelated to exercise), and 3 dropped out of the AT+RT group (return to work, n = 1; moved, n = 1; arthritis preprogram, n = 1). No significant injuries or cardiovascular complications related to AT or RT were incurred during the study.
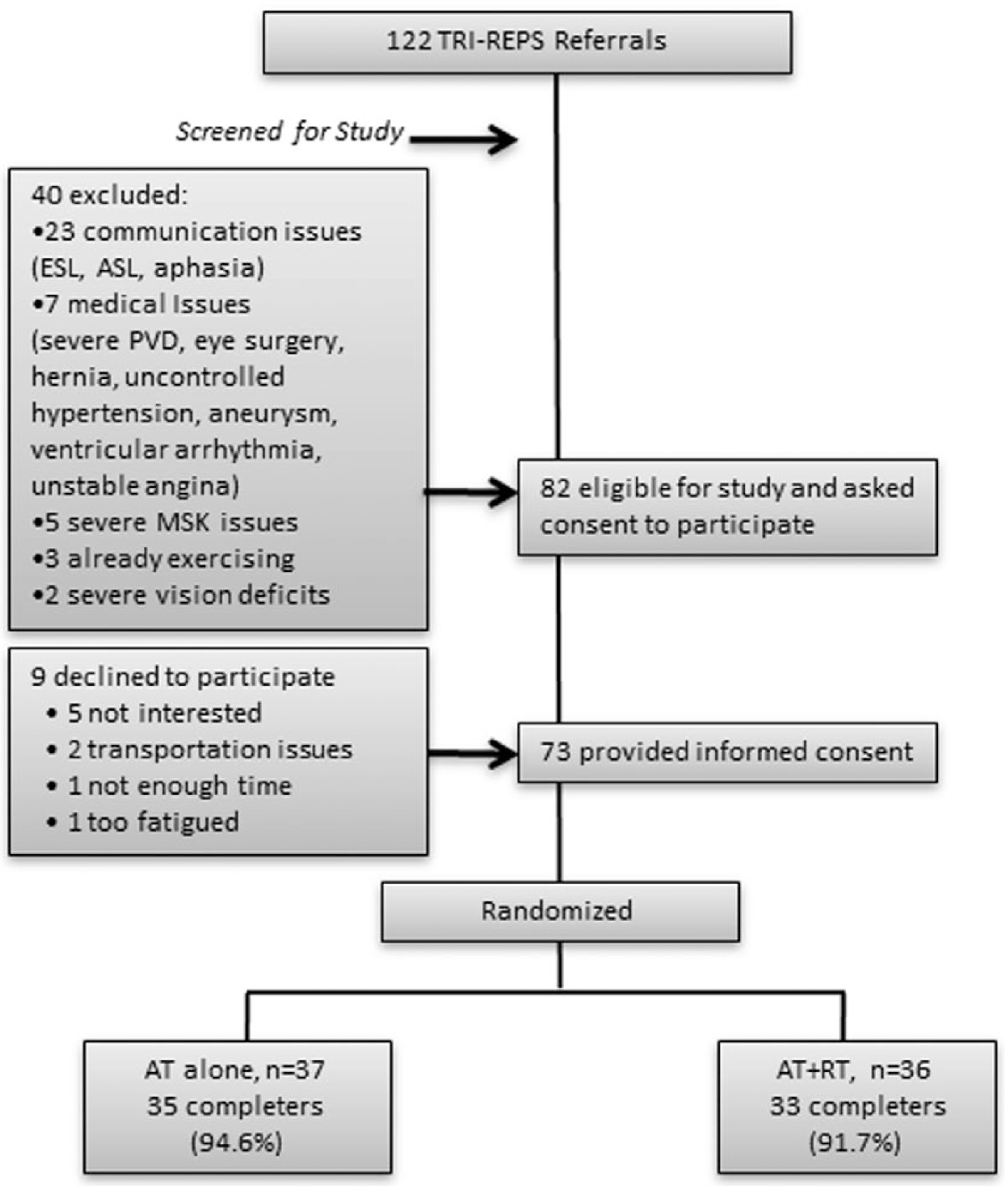
Enrollment process.
Baseline Characteristics
Table 1 shows the participants’ baseline characteristics. Randomization yielded a lower baseline body mass index and total and trunk percentage body fat for AT versus AT+RT but no difference in any measure of lean mass. There was an imbalance between groups in NIHSS score, elapsed time from stroke to start of the exercise intervention, and age. There was no change to significance of the probability values of the outcomes after adjustment for these 3 baseline measures, except for affected-side arm lean mass that became significant (P = .06 to P = .04; Table 2). Unadjusted analyses will be presented herein.
Baseline Characteristics of Participants. a
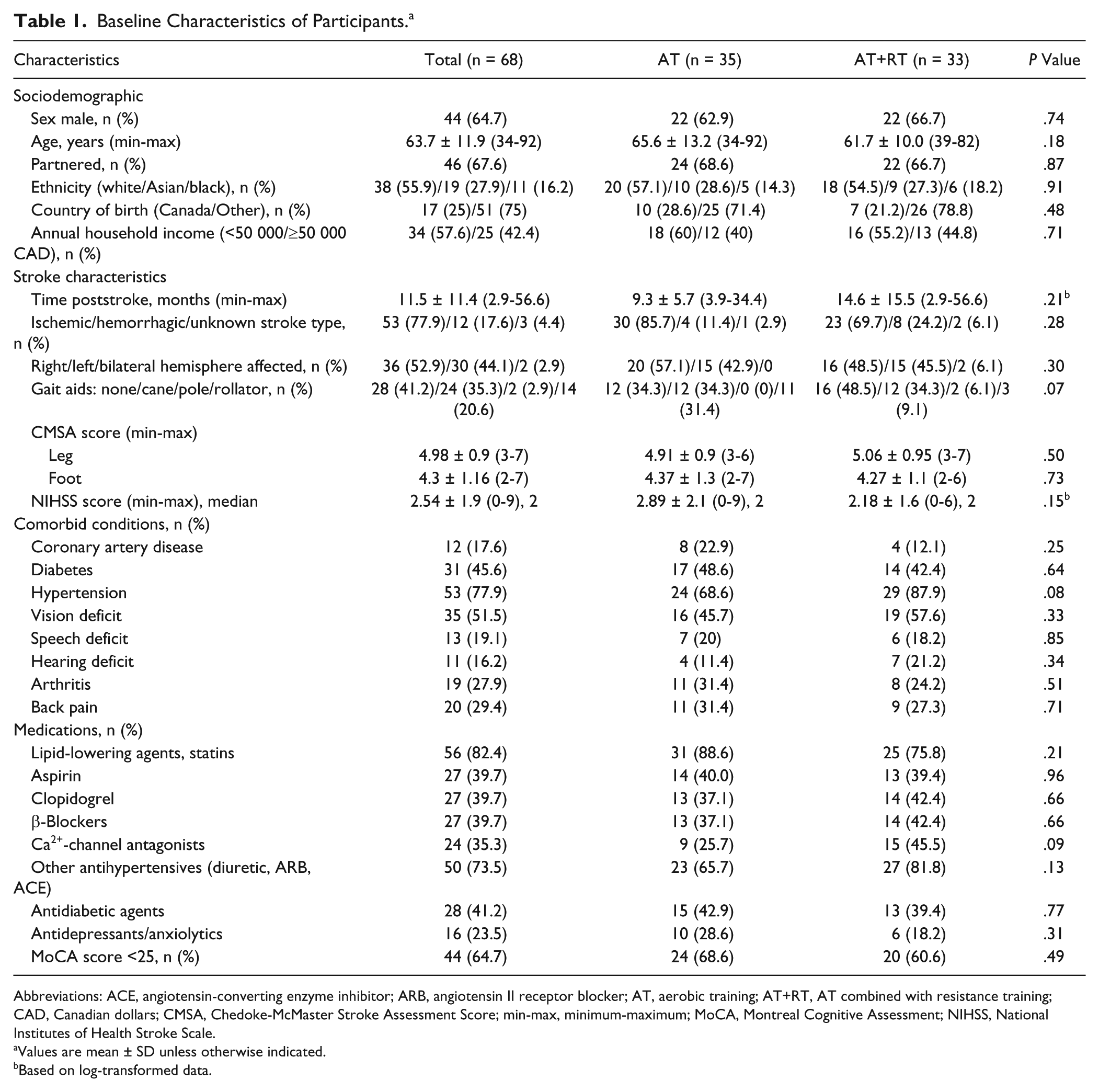
Abbreviations: ACE, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; AT, aerobic training; AT+RT, AT combined with resistance training; CAD, Canadian dollars; CMSA, Chedoke-McMaster Stroke Assessment Score; min-max, minimum-maximum; MoCA, Montreal Cognitive Assessment; NIHSS, National Institutes of Health Stroke Scale.
Values are mean ± SD unless otherwise indicated.
Based on log-transformed data.
Effects of Exercise Modalities on Outcomes. a
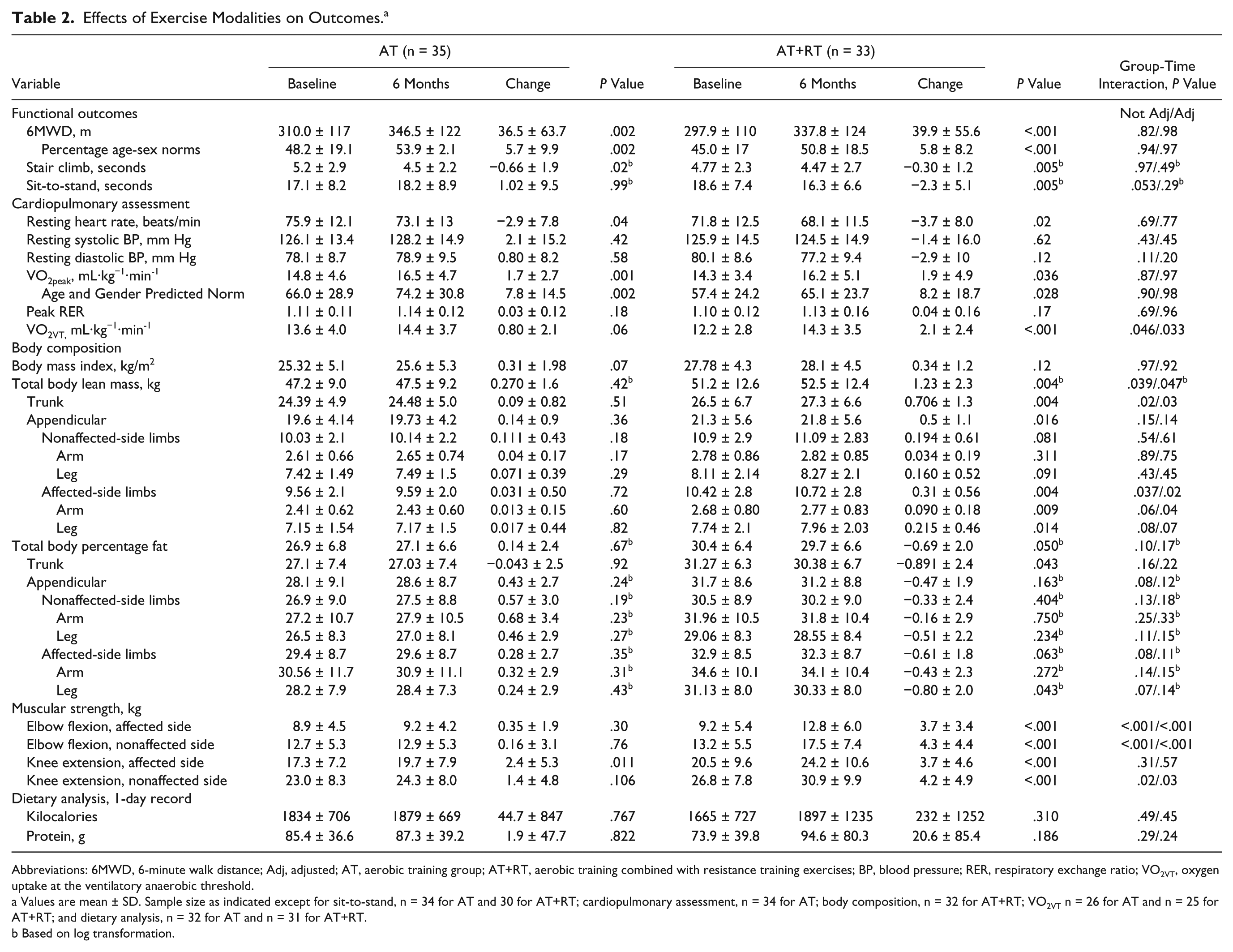
Abbreviations: 6MWD, 6-minute walk distance; Adj, adjusted; AT, aerobic training group; AT+RT, aerobic training combined with resistance training exercises; BP, blood pressure; RER, respiratory exchange ratio; VO2VT, oxygen uptake at the ventilatory anaerobic threshold.
Values are mean ± SD. Sample size as indicated except for sit-to-stand, n = 34 for AT and 30 for AT+RT; cardiopulmonary assessment, n = 34 for AT; body composition, n = 32 for AT+RT; VO2VT n = 26 for AT and n = 25 for AT+RT; and dietary analysis, n = 32 for AT and n = 31 for AT+RT.
Based on log transformation.
Cardiorespiratory Adaptations
Whereas both groups had significant and similar improvements in VO2peak, there was a greater improvement in VO2VT for AT+RT compared with AT alone (P = .046; Table 2; Figure 2B). There was no change within groups or difference between groups in peak respiratory exchange ratio, indicating the same relative effort at test termination.
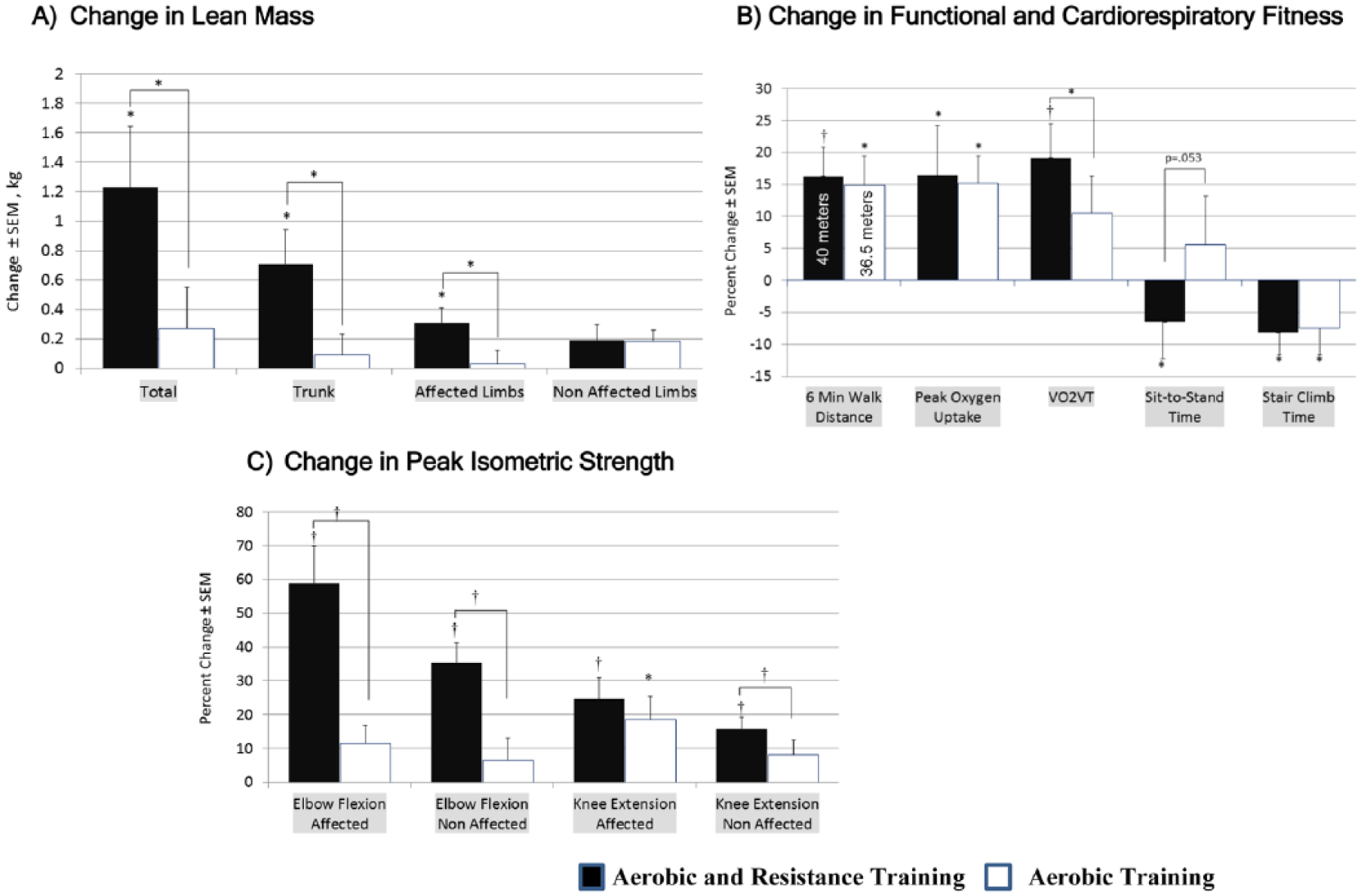
Change in body composition, functional and cardiorespiratory fitness, and strength during interventions.a
Body Composition and Dietary Analysis
There was a significantly greater increase in total lean mass in AT+RT compared with AT alone (1.23 ± 2.3 vs 0.27 ± 1.6 kg, respectively; P = .04), specifically in the region of the trunk (0.71 ± 1.3 vs 0.09 ± 0.82 kg, P = .02) and affected limbs (0.31 ± 0.56 vs 0.031 ± 0.5 kg, P = .04); see Table 2, Figure 2A. Although there was no between-group difference, there was a significant reduction in percentage fat of the trunk and affected leg in AT+RT (P < .05), with no change for AT (P > .4). There was no within- or between-group change for total kilocalories or protein consumed.
Peak Isometric Muscular Strength
AT+RT demonstrated significant improvements in all measures of isometric strength. Only affected-side knee extension peak force improved in AT (P = .01); see Table 2, Figure 2C. There was a significant between-group difference favoring AT+RT in all measures except affected-side knee extension peak force.
Functional Outcomes
Both groups had significant improvements in 6MWD and stair climb performance, with no between-group difference (P > .8); see Table 2, Figure 2B. Only AT+RT had a significant improvement in sit-to-stand performance, with a trend for greater improvement when compared with AT alone (P = .053).
Exercise Performance and Adherence to Training
There were no significant between-group differences in session attendance, number of diaries submitted, and proportion of prescribed AT sessions completed (Table 3). As expected, according to study design, the AT group completed more AT sessions than the AT+RT group. There was a significant and similar progression of all parameters of the AT prescription for both groups. There was no between-group difference in the mean AT intensity (percentage of the HR that occurred at VO2VT) determined from the exercise log measured by the participant during home exercise or when measured by a staff member during supervised sessions. There were significant increases in upper- and lower-body 1RM scores and weight load performed in AT+RT. The weight load performed fell within the targeted training level of 50% to 60% 1RM at baseline and 70% at 21 weeks of training.
Exercise Performance, Prescription, and Adherence to Training.
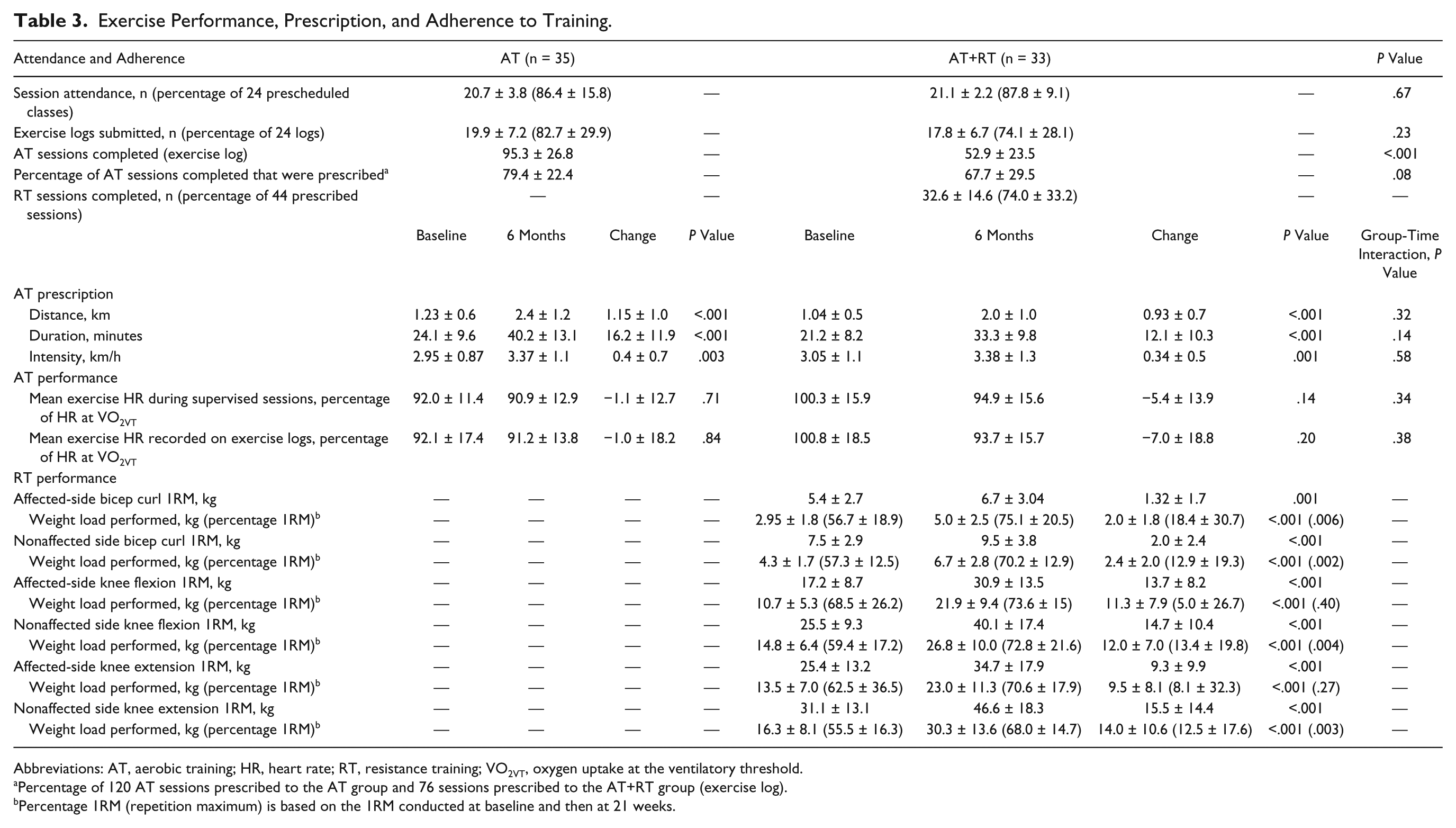
Abbreviations: AT, aerobic training; HR, heart rate; RT, resistance training; VO2VT, oxygen uptake at the ventilatory threshold.
Percentage of 120 AT sessions prescribed to the AT group and 76 sessions prescribed to the AT+RT group (exercise log).
Percentage 1RM (repetition maximum) is based on the 1RM conducted at baseline and then at 21 weeks.
Discussion
The results of this study help elucidate an exercise treatment strategy aimed at mitigating future vascular and metabolic risk as well as functional impairments for people with persisting mobility deficits following stroke. To our knowledge, this is the first study to demonstrate that replacing 2 AT sessions with 2 RT sessions results in nearly 5 times more total body muscle mass accretion, greater improvements in muscular strength and VO2VT, and a trend toward improved performance on the sit-to-stand test than 5 AT sessions per week. Furthermore, only AT+RT resulted in significant reductions in percentage trunk and leg fat. Although AT+RT did not improve 6MWD more than AT alone, this treatment model did not compromise improvements in mobility, cardiorespiratory fitness, or stair climb performance, despite 40% less aerobic exercise prescribed. These outcomes were achieved with a program model that included only 1 supervised group session combined with 4 weekly unsupervised home sessions, using low-cost, accessible exercise equipment. In a cohort in which more than half (54%) of all participants had a diagnosis of coexisting coronary artery disease and/or diabetes, and at least mild cognitive impairment (61%), both exercise interventions resulted in high levels of adherence to the exercise prescribed, with completion rates of more than 90% and no exercise-related adverse events.
Lean Mass
The greater increase in lean mass following AT+RT of 1.23 kg compared with the nonsignificant change in the AT-alone group (0.27 kg), has important clinical implications for people poststroke. Recent data derived from DXA scanning in large epidemiological studies provide compelling evidence of the importance of lean mass accretion for mortality outcomes; in adjusted analyses from both the Cardiovascular Health Study and National Health and Nutrition Examination Survey (NHANES), greater muscle mass was associated with a protective effect from all-cause and/or cardiovascular mortality in middle-aged and older populations.5,6 Both studies showed that the lowest event rates occurred in the high lean mass/low-fat group and the highest event rates occurred in the low lean mass/low-fat group. These data are consistent with previous reports of an inverse association between muscle strength, RT participation, and mortality in healthy and chronic disease populations.7-10,54 The increase in lean mass and reduction in percentage trunk fat in the AT+RT group not observed in the AT group, despite no difference between groups in dietary protein and kilocalorie intake, may also play a role in improved metabolic health. A recent meta-analysis demonstrated that combined AT+RT has a greater effect on glycemic control than either modality alone in people with type II diabetes. 55 This is an important consideration given the high prevalence of abnormal glucose metabolism (77%) and coexisting diabetes (~35%) in people with chronic stroke. 56
Despite the importance of lean mass accretion, few studies have measured the effect of exercise on the body composition of people poststroke by DXA scan. Three single-group studies that included RT interventions alone (n = 10 to 18 participants) did not result in a change in total body lean mass likely owing to an insufficient total body stimulus (2 sets of 3 lower-extremity exercises).57-59 Furthermore, an earlier study conducted by our group failed to demonstrate a significant increase in total body lean mass by DXA in 41 poststroke participants after 6 months of AT+RT. 47 Similar to the current study, the RT program targeted all major muscle groups (1 to 2 sets of 10 to 11 exercises) and was progressed by a combination of increasing repetitions and weight load. Progression methods were the same as in the present study but without repeated 1RM testing. One of the most important determinants of muscle hypertrophy and strength is the magnitude of the weight load lifted, 60 and thus, repeat 1RM testing is likely important for optimizing lean mass. Remarkably, the magnitude of change in lean mass in the current study was similar to that in a previous study by our group in people with coronary artery disease. 25 We reported that 6 months of AT+RT (2-3 sets) yielded a significantly greater lean mass gain than AT alone (1.5 vs 0.4 kg, P < .01, respectively). This similar change in lean muscle mass and the fact that there was a greater magnitude of change in lean mass accretion in affected limbs than nonaffected limbs suggests that motor impairment did not preclude accretion of lean mass in the current study. The underlying reasons for this may be multifactorial. First, greater change would be expected on the affected limbs because baseline levels are lower when compared with nonaffected limbs. 2 Also, fast-twitch muscle fibers are more prominent in affected-side limbs, and lean mass accretion is more likely to occur in these fibers than other fiber types. 61 Finally, the RT program emphasized independent limb action to eliminate overcompensation by the nonaffected side. These results and safety record of the current study suggest that RT exercises can be successfully modified to accommodate mild to moderate motor impairment. Furthermore, progression to a weight load equivalent to ~70% of 1RM is not only safe but can effect significant lean mass accretion in appropriately screened people with mobility deficits.
Cardiorespiratory Fitness
Despite similar and significant improvements in VO2peak in both cohorts, there was an almost 2-fold greater improvement in VO2VT in the AT+RT group than in AT alone. Recently, VO2VT has been identified as an important adjunct to VO2peak for establishing cardiovascular mortality risk 62 and as a significant prognostic marker for postsurgical risk.63,64 The literature also suggests that VO2VT may be a more reliable index of overall cardiorespiratory fitness that may more accurately represent aerobic capacity than VO2peak in people poststroke with disability.43,47,48 We previously reported that among 98 individuals undergoing a CPET poststroke, only 18% reached a “true” physiological maximum (VO2max), whereas 67% had a discernible VO2VT. 43 Measurement of VO2max is limited by motor and neurological impairments, thereby mitigating the utility of VO2peak as a measure of cardiorespiratory fitness.43,48 A reason for the greater increase in VO2VT for the combined training group may be because RT protocols, specifically moderate repetitions with moderately heavy weights, as prescribed in the current study, rely on anaerobic glycolysis, which results in higher acute peripheral lactate responses (~6 to 9.5 mmol/L) 65 than is typically produced during AT performed at the recommended training intensity (~4 mmol/L). 66 These greater lactate levels result in superior training adaptations related to improved clearance of lactate, as demonstrated in people with coronary artery disease undergoing AT+RT compared with AT alone.25,67
Six-Minute Walk Distance and Strength
Despite less prescribed aerobic exercise, AT+RT resulted in a comparable change in 6MWD to AT alone; this was beyond the threshold of 29 m, which is reported as the minimal detectable change in people within 1 year from stroke.52,68 Thus, the results do not support the recommendation to include RT to AT to enhance 6MWD poststroke. These results are concurrent with previously conducted studies of similar design. One study was underpowered, with only 12 participants per group, and reported no significant within- or between-group change in 6MWD with AT+RT (24 m) or AT alone (12.1 m) or compared with sham exercise training (5 m). 21 Similarly, Sullivan et al 22 reported that 6 weeks of body weight–supported treadmill exercise combined with either upper-extremity ergometry (AT) or lower-extremity RT, both resulted in significant improvements in 6MWD (22.5 ± 34.8 and 45.3 ± 33.5 m, respectively) with no between-group difference. A recent meta-analysis comparing AT versus control (n = 16 studies) and AT+RT versus control (n = 7 studies) demonstrated that both exercise interventions result in significant improvements in 6MWD and walking speed poststroke. 20 A further subgroup analysis revealed no significant difference between these 2 exercise interventions. Thus, our results and those of others suggest that the addition of RT to AT provides no supplementary benefit to 6MWD. A possible reason is that the AT group, despite no change in leg lean mass, had a similar and significant improvement in affected-side leg strength as the AT+RT group. As previously mentioned, leg strength, specifically on the affected side, explains some of the variance in gait performance. 3
Limitations
This study lacked an inactive control group, and thus, spontaneous recovery may have contributed in part to our observations. However, the relative magnitude of the physiological changes suggests a significant and clinically meaningful training effect associated with AT+RT and AT alone that exceeds that reported in control groups of previous studies.23,25,69-76
Moreover, participants started exercise remote from their stroke diagnosis when the magnitude of spontaneous change in physiological recovery is reported to be diminished. 77 In addition, there was little impact on between-group differences after adjusting for time from stroke, age, and NIHSS score. Although the present study was strengthened by exploring multiple physiological domains, the risk of type I error should be acknowledged as a potential limitation. Reducing the number of comparisons could be accomplished by creating a composite measure of strength or eliminating regional measures of lean mass. However, these regional measures contribute to our understanding of the underlying mechanisms for change and for hypothesizing the exercise training characteristic likely responsible for the outcome. Thus, this article serves as an exploratory analysis of secondary outcomes that also has some utility as hypothesis generating. In addition, although VO2VT is not always discernible in all participants in practice, 75.8% and 74.3% of participants in the AT+RT and AT groups, respectively, in the current study achieved VO2VT on both baseline and 6-month CPET results, which is similar to previous reports,43,47,78 and was not different between groups. It is also possible that our study was not powered to detect change in some variables. Our study included participants in the middle range of motor function, and results may not generalize to all individuals poststroke.
Conclusion
This study provides evidence for incorporating both RT and AT into poststroke rehabilitation to improve recovery in those with mobility deficits. Despite the lack of advantage to 6MWD, combined training enhances stroke recovery by improving components of cardiorespiratory fitness, muscular strength, and muscle mass accretion. The cardiovascular advantage offered by supplementing AT sessions with RT as well as the safety record, acceptable adherence, and the possible long-term mortality advantage offered by this strategy support this recommendation. Additional studies to corroborate these findings are warranted.
Footnotes
Acknowledgements
The authors would like to acknowledge those who volunteered for this study and the contribution of the Rehabilitation Staff, including Danielle Lawrence, Suban Kangatharan, Rachel Goodman, Merrisa Martinuzzi, Nemanja Dovijarski, Daryl Dooks, Karen Dobson, Sonia Watson, and Rene Belliard.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Heart and Stroke Foundation Canadian Partnership for Stroke Recovery and the Ontario Stroke Network (OSN1207-000144). SM received fellowship funding from Heart and Stroke Foundation Canadian Partnership for Stroke Recovery.