
Abstract
Background and Purpose. Observation of action with intention-to-imitate (OTI) might enhance motor recovery. This early phase trial investigated whether OTI followed by physical practice (OTI + PP) enhanced the benefits of conventional physical therapy (CPT) on upper limb recovery early after stroke. Methods. Participants were 3 to 31 days poststroke. They had substantial paresis and ability to imitate action with their ipsilesional arm. After baseline measures, participants were randomized to either OTI + PP in addition to CPT or to CPT only. Outcome measures were made after 15 days of treatment. The measurement battery was the Motricity Index (MI) and the Action Research Arm Test (ARAT). Change, baseline to outcome, was examined using the Wilcoxon test for within group and Mann–Whitney U test for between groups. Results. Sixty-five of 570 stroke survivors were eligible, 55 were able to imitate, 37 gave informed consent, 7 were transferred out of area before baseline, and 29 were randomized. Outcome measures were completed with 13 CPT participants and 9 OTI + PP participants. Both groups showed statistically significant improvements for the MI (CPT median change 8, P = .003; OTI + PP median change 10, P = .012) but the median (95% confidence interval [CI]) between-group difference was 0.0 (−11, 16), P = 1.000. For the ARAT, only the CPT group showed a statistically significant improvement (median 9, P = .006). The median (95% CI) between-group difference of 1.0 (−18, 23) was not statistically significant (P = .815). Conclusions. These findings suggest that OTI + PP might add little to the benefits of CPT early after stroke.
Introduction
Action observation produces excitation in the motor pathways of the observer in the same temporal–spatial pattern as that of physically performing the movement.1,2 This congruence of activation is a function of the mirror neuron network.3-5 These indirect neuroimaging observations are confirmed by activation of the same neurons in the supplementary motor area and hippocampus during the observation and the performance of hand grasping, 6 recordings of increased activity in the muscles that would be used to perform an observed action,7,8 and the formation of motor memories in the primary motor cortex.9,10 Action observation produces the largest increase in corticospinal pathway excitability in healthy adults when undertaken with intent to imitate 11 and when combined with physical practice. 12 This activation congruence during action observation and physical performance of movement in healthy adults may be present in people after stroke.13-15 Thus, there is increasing interest in the potential use of observation of human movement (action observation) with intent to imitate (observation-to-imitate; OTI), with or without physical practice (PP) to enhance motor recovery after stroke.16-18 OTI therapy might be of most benefit when used to prime and/or augment excitation within the motor execution pathways of people with substantial paresis to bring them to the point at which they can participate sufficiently in repetitive task-specific training. 19 Physical imitation is therefore the clinical point of OTI.
Preliminary evidence of benefit of OTI on motor function after stroke is emerging,13,14,20-22 but interpretation is limited by potential bias. External validity is also limited. Findings do not provide proof-of-concept for people in the first month after stroke, with substantial paresis, for older persons, and in relation to use of conventional physical therapy (CPT).
This early phase trial investigates the provision of OTI + PP to people with substantial paresis of the upper limb between 3 and 31 days after stroke to determine justification for conducting a subsequent definitive phase III trial. Are there indications that OTI + PP given in addition to CPT enhances ability to voluntarily contract paretic muscle and ability to use the paretic upper limb in functional activity early after stroke more than CPT alone? Does OTI + PP given in addition to CPT produce more adverse events than CPT alone?
Methods
Participants
All participants were recruited from an inpatient stroke unit. Entry criteria included adults who had suffered a stroke between 3 and 31 days before recruitment but with an intact premotor area (ability to encode observed human actions), 23 as confirmed by the physician member of the clinical team that checked the record of the routine clinical neuroimaging; able to produce some movement in a substantially paretic upper limb as assessed by a score of at least 18 on the Motricity Index (MI) 24 but unable to produce a grip force of more than 65% of that of the ipsilesional side; free from observable contralesional upper limb movement deficits attributable to pathology other than stroke.
If people fulfilled these criteria, they were given full information about the trial and asked to consider providing written informed consent. Those providing informed consent were then screened for the ability to imitate action with their ipsilesional limb. This was assessed by the research therapist sitting alongside the potential participant on the nonparetic side. The therapist performed an upper limb activity 3 times, and potential participants were asked to observe and then perform the activity. This procedure was repeated for 4 other upper limb activities. The 5 pantomime actions were drawing a vertical line in front of body, bringing a cup to mouth, hammering a nail, turning a page, and unscrewing a lid. This assessment was digitally filmed and saved onto a computer. An independent assessor viewed the recordings and judged the accuracy of imitation of the observed activity on a 3-point scale 25 : 2 = correctly reproduced action; 1 = incorrectly reproduced action; 0 = not reproduced. Those scoring 8 out of 10 or above were considered to have the ability to imitate and confirmed as participants in this trial.
Study Design
Randomized, controlled, observer-blind efficacy trial. Registered on the Current Controlled Trials Database—ISCRTN 51553998: http://www.controlled-trials.com/ISRCTN51553998/51553998. Ethical approval was received from a local NHS Research Ethics Committee and R&D approval from the NHS Trust that hosted the study. All participants gave written informed consent.
Randomization
Group allocation was computer generated in blocks of 4 by a university statistician before the trial began. Details of group allocation were placed into sequentially numbered, opaque, sealed envelopes. These were held by an independent administrator. After a participant had completed baseline measures, the research therapist telephoned the administrator who then opened the relevant envelope and divulged participant allocation details.
Sample Size
This was the first-ever investigation of OTI + PP with people with substantial paresis early after stroke and, therefore, no previous data on which to base a power calculation to estimate sample size were available. The general guidance is to avoid a formal power calculation and base the decision on pragmatic reasoning but with 30 participants to estimate parameters required for sample size estimation. 26
Interventions
All participants received CPT as deemed appropriate by the clinical therapists. The content and duration of routine therapy was recorded on the treatment schedule developed iteratively with clinical therapists. 27 Participants allocated to the control group received no therapy in addition to CPT. Participants allocated to the experimental group received OTI + PP from the research therapist. OTI + PP was to be provided in two 30-minute sessions, separated by a 10-minute rest, each day for 15 working days. Each 30-minute session was divided approximately into 6- to 8-minute periods divided by 2 to 4 minutes of resting. The rationale underlying the choice of intensity, duration, and spacing (dose) of therapy is provided by combining experimental evidence that 30 minutes of action observation and motor practice immediately encodes a motor memory in M1 in healthy older adults 28 and that beneficial effects were found for OTI + PP late after stroke from provision of 90 minutes a day for 18 days 13 and 30 minutes on 1 day. 14 The dose may need to be adapted for individual participants as after stroke people have reported difficulty maintaining concentration beyond 20 minutes. 29 The research therapist adapted daily intensity and spacing of OTI + PP in response to participant behavior and feedback while striving to maintain a total of 60 minutes each day.
The content of the OTI + PP activities was shaped by prior findings that accuracy of imitation is greater if the movement being observed is meaningful rather than meaningless,30,31 if the whole movement is observed, 32 or if the movement had been learned previously. 33 The experimental activities were therefore functional activities that people need to relearn after stroke: bring telephone to ear, transferring money/food (used dried pasta) from the table to a pot and vice versa, cleaning a table, taking a glass/bottle/pot from/placing on a shelf, pushing buttons on a telephone, bringing a cup to the mouth, turning cards and/or pages in a newspaper/magazine, placing pegs on a “washing line,” pouring water, and unscrewing/screwing lids of jars/bottles. Activities for OTI + PP, therefore, encompassed a variety of upper limb functional movements, for example, reaching, releasing grip, and hand dexterity. The emphasis was on training functional tasks using the contralesional upper limb. All tasks were unimanual.
The choice of the OTI + PP activity was made by participants and the research therapist. Activities were chosen that could be physically performed in part or with difficulty by the participant. No specific time limitation was set a priori for completion of imitation (physical performance). More than 1 activity would be used if the participant became either disheartened by perceived slow progress or was exhibiting signs of boredom. Activities were also changed if the participant improved to the point where they could be completed without difficulty. The instruction was to watch the research therapist perform the functional task for 1 to 2 minutes and to think about copying in preparation for doing exactly the same in time with the therapist for 4 to 6 minutes. Verbal correction was given but no physical contact was made. Verbal feedback on achievement was given to maintain motivation.
The therapist sat at a table alongside the participant on their paretic side and used the upper limb that matched the participant’s paretic side. This enabled demonstration of activity in the same plane as the movement to be produced by participant as corticomotor excitability is greatest in the first person orientation. 7 Participants had to rotate their head somewhat toward their paretic arm but this was very slight. The shoulders of the therapist and participant were almost touching so the head rotation was not much more than that required to watch the paretic upper limb during the imitated movement. For 1 to 2 minutes participants watched the activity with intent to imitate and then for 4 to 6 minutes they performed the activity simultaneously with the therapist who modulated timing as appropriate for the participant’s ability.9,14,28 The scientific rationale for viewing of real-life rather than video-filmed movements is that the former has been found to produce greater activation of the primary motor cortex. 34
Measurement Battery
Measurement points were before randomization, baseline, and within 3 working days of the end of the 15-day intervention period, outcome. All measures were made by an assessor blinded to treatment allocation. OTI + PP therapy is primarily directed at improving the ability to voluntarily contract paretic muscle after stroke. This was measured using the arm section of the MI 24 as the primary outcome. The secondary goal of OTI + PP therapy is to enhance recovery of the ability to use the paretic upper limb in functional activity. This was measured using the Action Research Arm Test (ARAT) 35 as a secondary outcome.
There was a small risk that for some people OTI + PP might lead to an “overuse” syndrome. We therefore monitored for participant report of upper limb pain, either verbal or behavioral (eg, grimacing, postural guarding), and for a decrease of at least 2 measurement levels in the MI. If the research therapist recorded these events on 3 consecutive working days, then the participant was withdrawn from the trial, but every effort was made to include them in outcome measures.
Analysis
Participants were analyzed according to their group allocation regardless of the amount of therapy they actually received. Where subjects withdrew before outcome they were not included in the analysis, and imputation was not used since we felt it might be unstable for a sample size of this magnitude. All analyses were conducted using Stata/SE version 11.0.
The within-group change was assessed using the Wilcoxon signed rank 2-tailed test. The median difference and its 95% confidence interval (CI), based on the Hodges–Lehmann estimate of shift, were estimated. Between-group change (ie, outcome score − baseline score) was assessed using the Mann–Whitney U independent samples 2-tailed test. To express the magnitude of the effect, the differences in medians were estimated and their 95% CIs were calculated using the Hodges–Lehmann estimate of shift. Only those individuals with both baseline and outcome measures were included in the analysis.
The number of participants within each group who were deemed to have experienced an adverse event was expressed as a percentage.
Results
Screening, Recruitment, and Attrition (Figure 1)
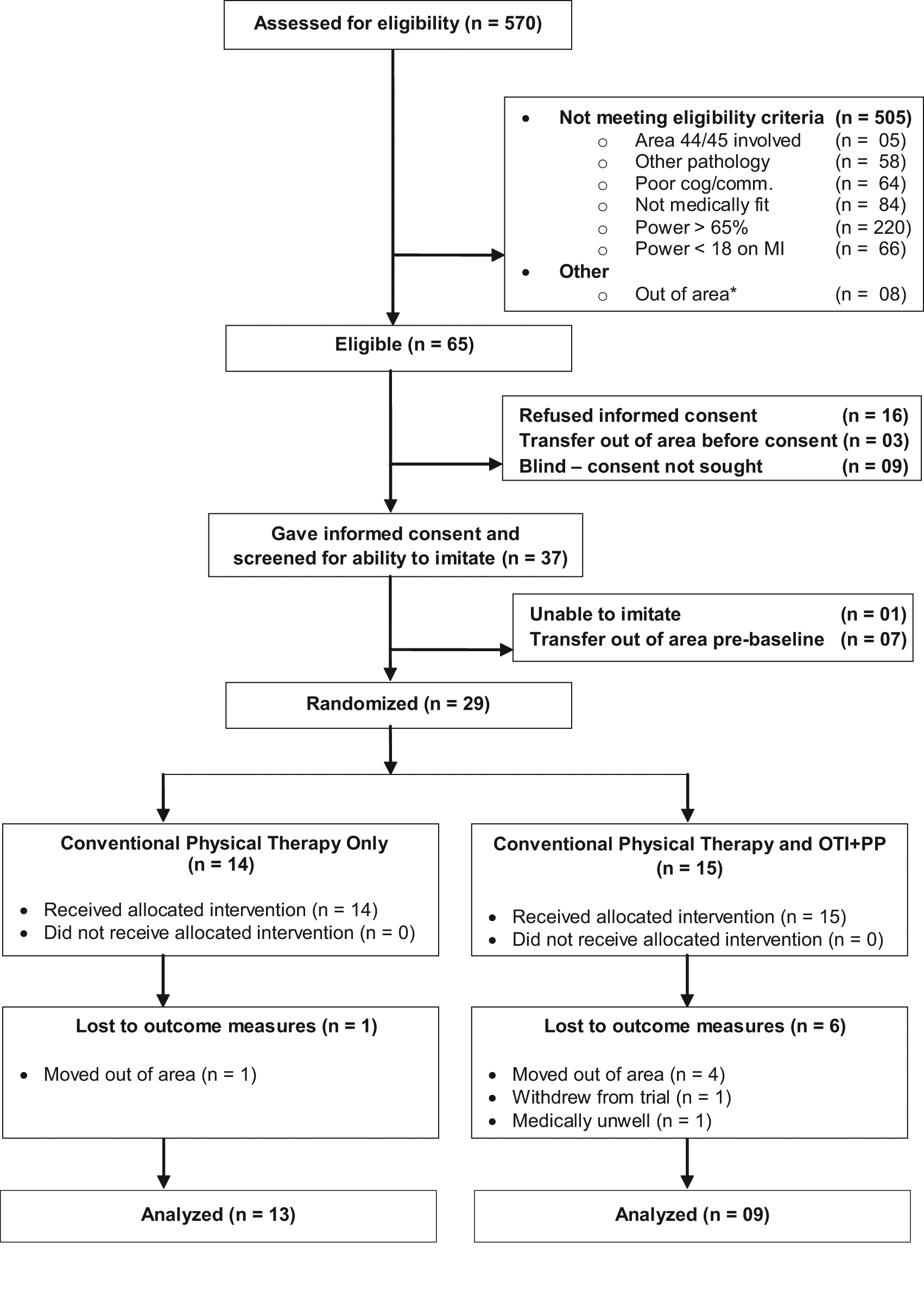
A total of 570 stroke survivors were screened with 65 (11.4%) meeting the eligibility criteria and being in the geographical area covered by the study. Ten people were unable to imitate, with 9 of these being blind (consent was not sought for these people). Of the 65 eligible people, 37 (57.0%) gave written informed consent and 29 participants were randomized (Figure 1). Outcome measures were completed on 13 participants in the CPT group and 9 in the OTI + PP group. One of the participants in the control group failed to fully comprehend the instructions for the MI at baseline so this score is missing. Consequently, Motricity data presented in this article for the control group is for 12 participants at both baseline and outcome. Reasons for attrition are provided in Figure 1.
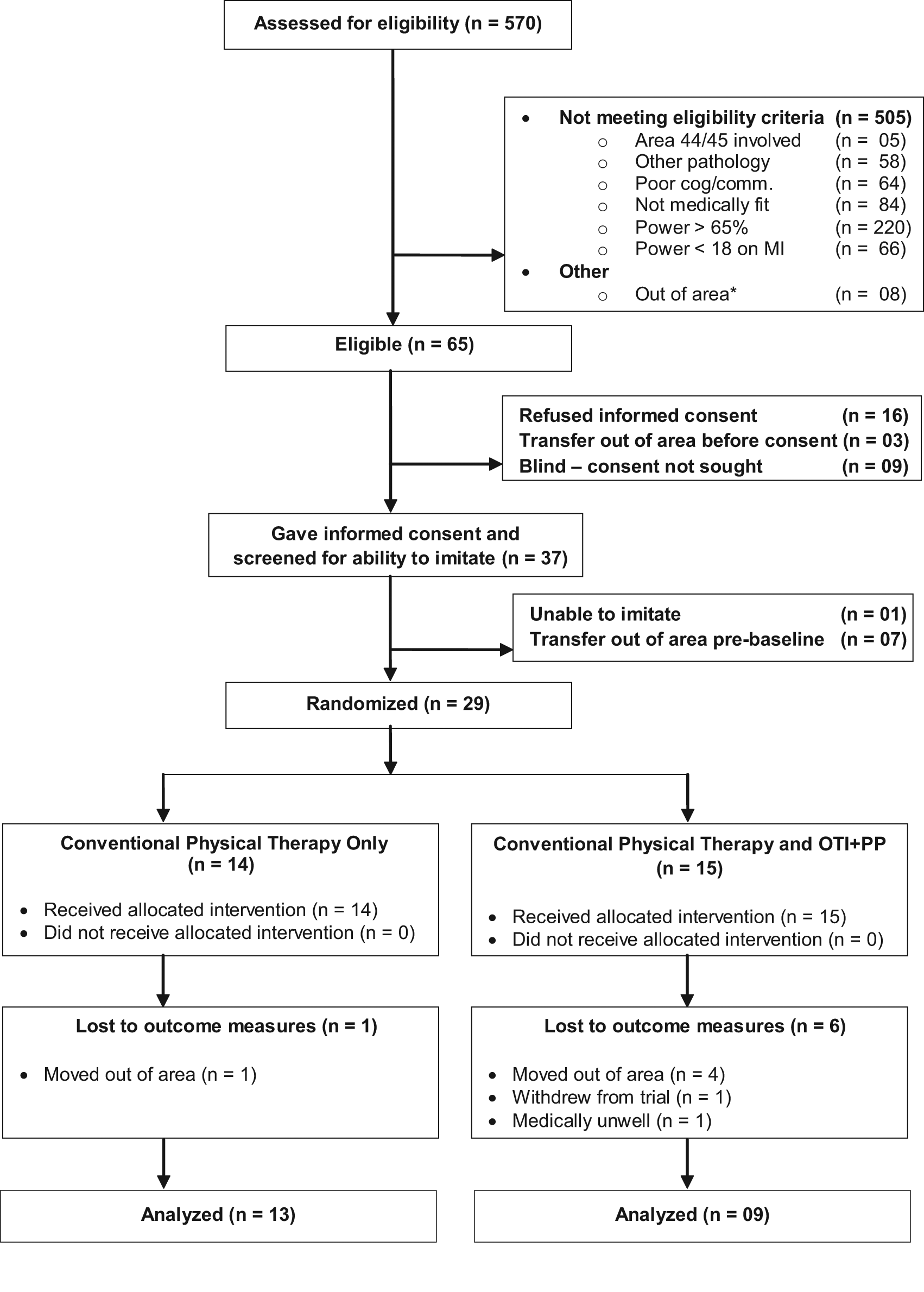
Trial flowchart. *Individuals who were transferred out of area before consent, baseline, or outcome could be obtained or whose permanent residence was outside of Norfolk.
In summary, 29 participants were recruited (Table 1). Their mean age was 77.2 (SD 10.4) years, and 17 were men (58.6%). The only obvious differences between the groups were that the OTI + PP group had a larger proportion of people with left-side paresis; a smaller proportion of people with a lacunar stroke (LACS) and a larger proportion of people with a partial anterior circulation stroke (PACS). It is possible that the difference in paretic side influenced results but unlikely as all participants were able to imitate.
Participant Characteristics
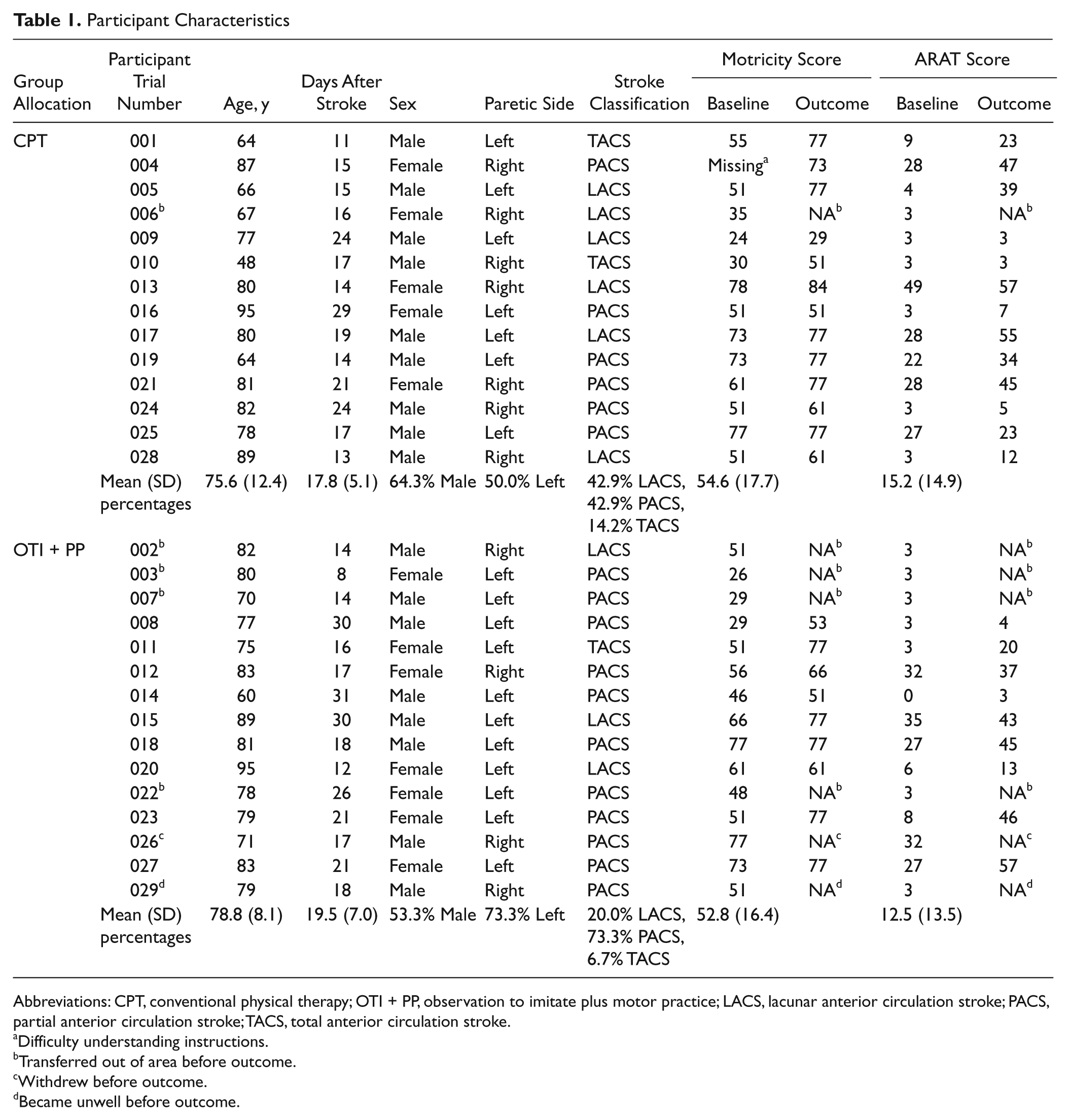
Abbreviations: CPT, conventional physical therapy; OTI + PP, observation to imitate plus motor practice; LACS, lacunar anterior circulation stroke; PACS, partial anterior circulation stroke; TACS, total anterior circulation stroke.
Difficulty understanding instructions.
Transferred out of area before outcome.
Withdrew before outcome.
Became unwell before outcome.
Intervention Received by Participants
Content and duration of CPT received by both groups was essentially the same (Table 2, Figure 2). The OTI + PP group received a mean of 11.24 (SD 3.28) hours of OTI + PP (Table 2): 75% of the 15 hours planned. Most participants needed more rest than anticipated and were unable to tolerate the planned two 30-minute sessions, separated by a 10-minute rest. Adapting to 20-minute sessions, separated by a 10-minute rest, was more acceptable to participants.
Duration of Upper-Limb Treatment Recorded for Each Participant Who Undertook Outcome Measurement
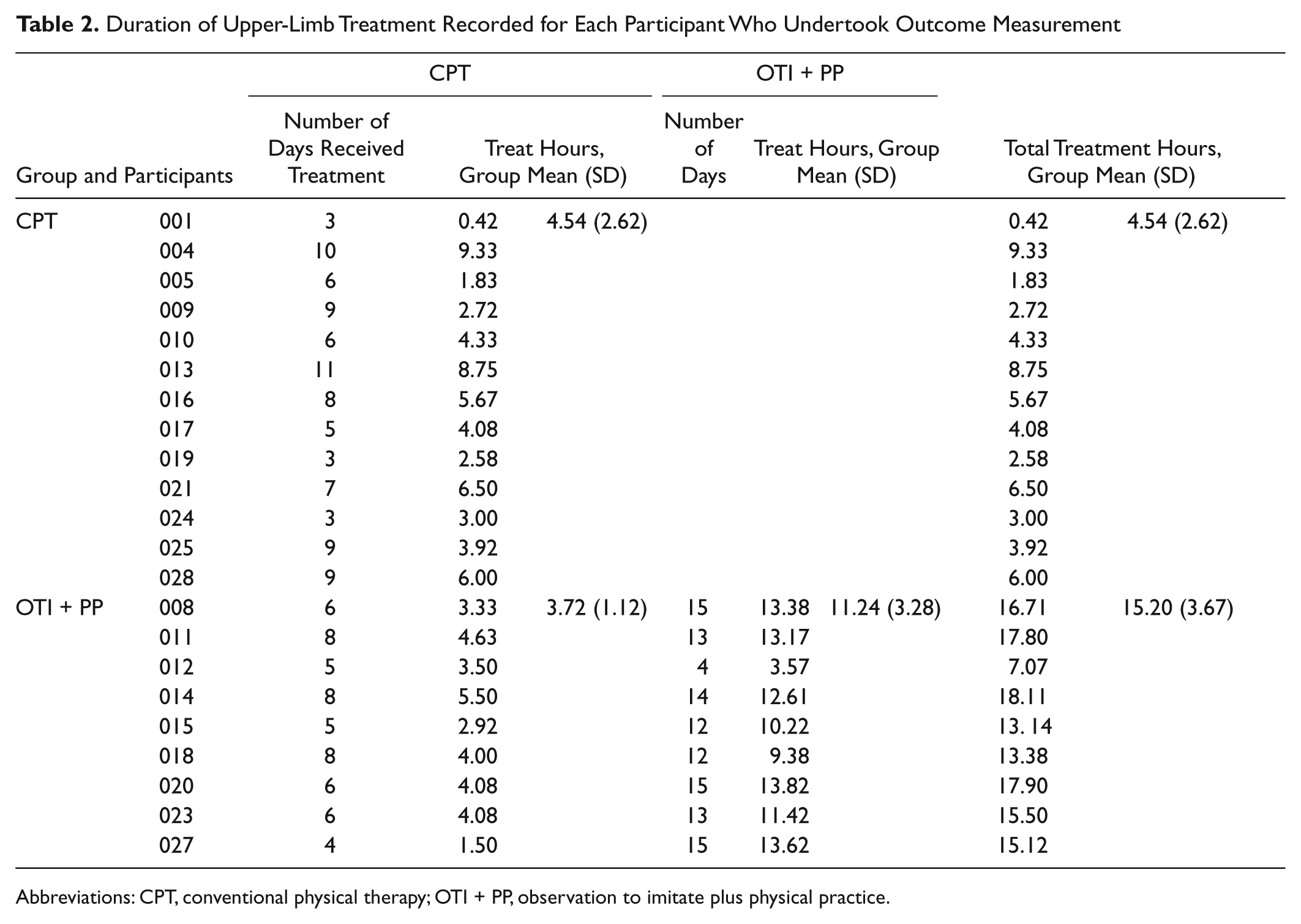
Abbreviations: CPT, conventional physical therapy; OTI + PP, observation to imitate plus physical practice.
Type of conventional physical therapy received by participants from clinical physiotherapists.
Clinical Efficacy
Both groups improved in MI score between baseline and outcome (Table 3). The significant median change was 8 points in the CPT group, P = .003, and 10 points in the OTI + PP group, P = .012. The median (95% CI) between-group difference was 0.0 (−11, 16), with a nonsignificant P value of 1.000 (Table 3). The median ARAT change was a significant 9 points for the CPT group (P = .006) and a nonsignificant 8 points for the OTI + PP group (P = .077). The median (95% CI) between-group difference 1.0 (−18, 23) was not statistically significant (P = .815; Table 3). No adverse events occurred in either group.
Change Baseline to Outcome for Muscle Strength (Motricity Index) and Functional Ability (Action Research Arm Test)
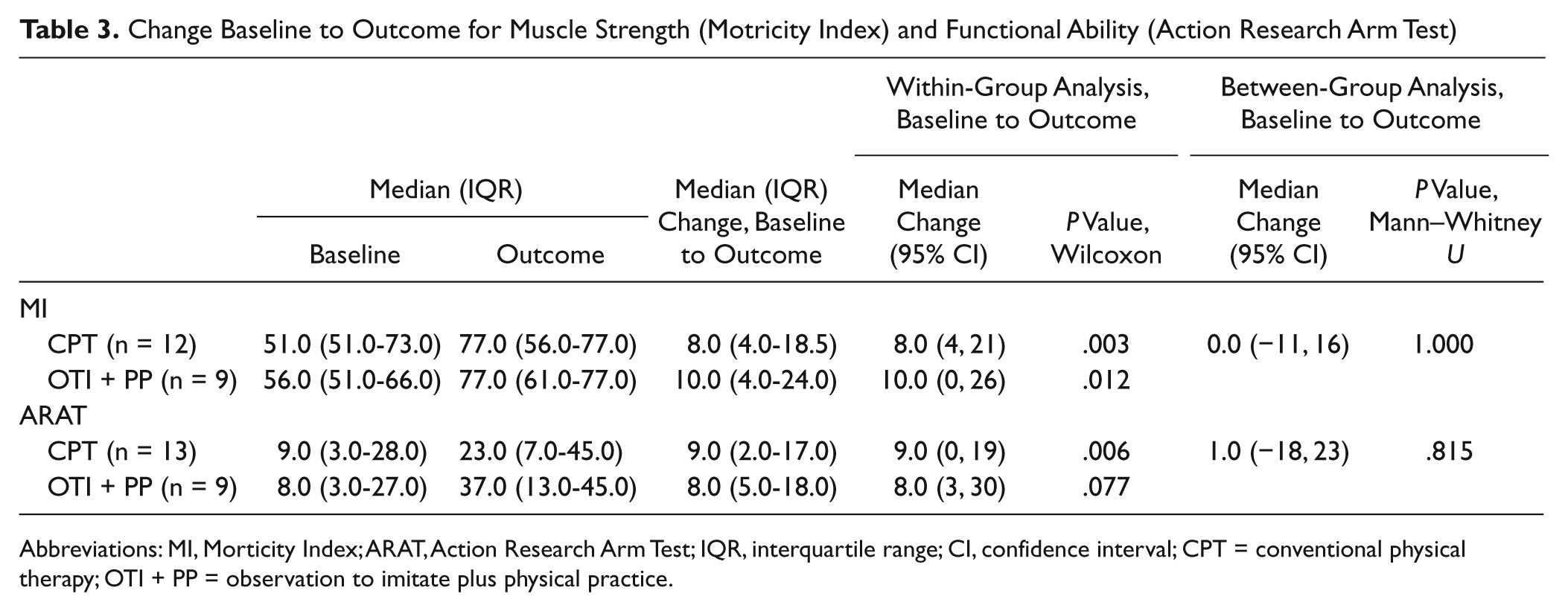
Abbreviations: MI, Morticity Index; ARAT, Action Research Arm Test; IQR, interquartile range; CI, confidence interval; CPT = conventional physical therapy; OTI + PP = observation to imitate plus physical practice.
Discussion
Both groups showed statistically significant improvements from baseline to outcome for ability to voluntarily contract paretic muscle (MI). The CPT group showed statistically significant improvement from baseline to outcome for functional ability (ARAT). There were no discernable differences between groups for either the MI or ARAT. These findings add to knowledge of the efficacy of OTI + PP as this is the first investigation of its use in people in the first month after stroke; the first randomized controlled trial (RCT) of the use of OTI + PP for people with severe paresis and that excluded potential participants who could not physically imitate an observed action; and the first to investigate the potential benefit from adding OTI + PP to routine physical therapy.
The equivocal findings of the present trial differ from the conclusions of earlier studies that suggest OTI + PP is a beneficial treatment strategy after stroke.13,14,20-22 On the other hand, 3 of these earlier studies were not RCTs. One was an experimental investigation of the immediate effects of 1 session of OTI + PP, 14 one was a before and after case study of 1 person, 20 and one was a before and after uncontrolled observational study of 28 people. 21 Although the findings of significant improvements, reported here, within the OTI + PP group from baseline to outcome support and extend these earlier observational findings into the first month after stroke, they do not support the interpretation that OTI + PP is a beneficial addition to CPT at this point after stroke for people with substantial paresis. The only previous studies to randomize people to either an OTI + PP or control group did find a significant improvement in the OTI + PP group compared with the control group. However, one of these may have a greater risk of bias than the present trial as details of generation and concealment of group allocation were not given, blinded assessment of outcomes does not appear to have been used, and there is some confusion about the number of sets of participant behavioral data. 13 Eight were reported in the abstract, 15 in the methods section, and baseline data for 16 people were presented in the results section. 13 The other randomized clinical trial has a low risk of potential bias and found a significant benefit for the OTI + PP group for functional dexterity (measured by the Box and Block Test) but not for measures of upper limb motor impairment or for functional independence. 22 Four other key differences between previous trials and that reported here are time after stroke, the different control interventions used, the form of delivery of the OTI + PP therapy, and the severity of paresis experienced by participants in the trials.14,22
First, participants in this present trial were earlier after stroke than either of the previous randomized clinical trials.14,22 One of these trials did recruit people at 30 days after stroke, 22 which is not that much later than the mean of 18.7 days for the participants in the study reported here. The other randomized clinical trial, however, recruited people much later. Interestingly, evidence is beginning to emerge to suggest that the beneficial results found from physical therapies late after stroke are not necessarily replicated early after stroke.36,37 Conversely, other studies involving people early after stroke have reported significant improvements in response to repetitive interventions.38,39 Resolution of this uncertainty is being addressed through investigation of the underlying neurological mechanisms of response to and prognostic indicators for response to specific physical therapies in well-characterized participants. 40
Second, the control interventions used in this and the earlier RCTs were different. Unlike the present trial, the earlier RCTs provided some control for a potential black box effect of action observation. These control conditions were video-films of geometric shapes 13 and practice of the movement tasks used in OTI but with instructions from a therapist and video-films of static objects and PP of movements of shoulder and/or elbow. 22 Physical practice of functional tasks was also provided to participants allocated to the control group for the present trial, but it only formed 14% of the CPT delivered to both groups (Figure 2). The remainder of the CPT provided to all participants in the present trial was a more passive form of physical therapy that may be less effective than task-specific practice. Future research could test whether the different control interventions are likely to contribute to the observed difference in results.
Third, the form of delivery of the OTI + PP therapy was different in this trial than in the earlier ones. Ertelt and colleagues delivered OTI via video-film of activities from 3 different perspectives and then participants undertook PP. 13 Franceschini and colleagues also used video-films. 22 The first person perspective was used. Whereas participants in the present trial watched a therapist perform the activity in the first person perspective (OTI) and then the participant performed the activity while the therapist continued to do so (PP). Although there is a scientific rationale for the form of OTI + PP evaluated in this trial, it is possible that delivery of OTI via video-film followed by independent PP is a more efficacious form. This possibility needs to be tested.
Fourth, although an exact comparison is not possible because of different measures used, it is probably fair to infer that the participants in the present trial had more severe paresis than those in the earlier trials.13,22 This could be important in explaining differences as severe paresis is associated with a slower and poorer recovery of function. 41 Animal model studies indicate that brain reorganization and subsequent upper limb recovery requires around 400 repetitions of an activity. 42 This amount of therapy is substantially more than participants within this study actually completed. Indeed, many of them did not manage the planned dose of 60 minutes per day. So the number of repetitions of activities in the present trial was probably less than the number of repetitions of activity provided in the 90 13 and 60 minutes of treatment a day. 22 This difficulty of delivery of intense therapy to people with substantial paresis early after stroke has also been highlighted in trials of other physical therapy interventions.43-45 This challenge of how to provide intense therapy to people with severe paresis early after stroke was also found in the present trial as we had to change the planned two 30-minute sessions to two 20-minute sessions. An earlier study of delivery of Motor Imagery to stroke patients also found that they reported difficulty concentrating after 20 minutes. 29 It is probably advisable to undertake such an iterative investigation with people with severe paresis early after stroke to determine the most appropriate spacing over a working day of OTI + PP.
It is possible that the larger proportion of people with a LACS classification in the CPT group could have eroded any potential difference between the 2 groups as these people would be expected to have better motor recovery. 6 However, severity of motor impairment is also associated with motor recovery. 40 As the groups were balanced for severity of motor impairment (measured by MI), it is unlikely that the imbalance between groups in stroke classification affected the results. It would be advisable, however, for future investigations to characterize the stroke lesion in terms of what brain structures are involved in the stroke lesion as some brain areas may be more crucial for motor recovery than others.
Another possible influence on the results is that the randomization was blocked in groups of 4 and the research therapist was aware of this process. This could be a source of unintentional bias. Although this is unlikely as the groups were balanced for the prognostic indicator of severity of motor impairment 41 and the results were equivocal.
Not all mirror neurons may show increased activity in response to action observation. Electrophysiological recordings from area F5 of the ventral premotor cortex of adult macaque monkeys found increased excitability in one population of pyramidal tract neurons and suppressed activity in another.47 As the pyramidal tract neurons from which recordings were made probably project to the spinal cord, it is likely that the consequence is not always increased activity in an effector muscle. In other words, there is experimental evidence to suggest that action observation may not always enhance ability. Action observation could suppress central excitability.
Conclusions
This early phase trial will inform the design of subsequent trials particularly in terms of dosing and form of delivery (video-film or not) of OTI + PP to people early after stroke, recruitment, and the provision of estimation of treatment effect variance and attrition rate to inform a sample size calculation. It is important to note that the present finding that OTI + PP might add little to the benefits of physical therapy early after stroke may not be upheld. These early phase findings of a possible clinically important benefit of OTI + PP justify proceeding with this line of investigation but maybe not straight to a definitive trial. The findings of this present trial suggest that it would be advisable to undertake early phase trials to determine which form OTI + PP should take, which individuals may benefit from this type of therapy, and the most appropriate dose to deliver.
Footnotes
Acknowledgements
We are grateful to all participants and to our clinicians.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Dunhill Medical Trust provided the funding.