
Abstract
Background. The mirror neuron network provides a neural mechanism to prime the motor system through action observation in stroke survivors. Objective. To examine whether action observation training with immediate physical practice improves upper-limb function in chronic stroke. Methods. In a within-subject design, 14 chronic stroke survivors were assessed at baseline, then participated in 2 weeks of relaxation-sham plus physical practice (control) and reassessed. Thereafter, they participated in 2 weeks of action observation training coupled with immediate physical practice (intervention), followed by a final assessment. Duration of each action observation video sequence (priming exposure) was 30 s followed immediately by practice of the observed motor skill. Results. There were significant improvements in control and intervention phases on primary outcome measures—Upper Extremity Fugl-Meyer Motor Assessment (FMA) and Functional Test of the Hemiparetic Upper Extremity (FTHUE)—as well as secondary outcome measures of self-perceptions of arm use. Gains in the primary outcomes were greater during the intervention phase (action observation + physical practice; FMA, 10.64; FTHUE level, 0.79, and tasks, 1.57) than during the control phase (relaxation-sham plus physical practice; FMA, 6.64; FTHUE level, 0.43, and tasks, 1.00). Interviews with participants highlighted the added value of watching an actor perform the movement before physically attempting to perform the action. Conclusions. This study provides preliminary evidence of the additive value of action observation plus physical practice over relaxation-sham plus physical practice. There appears to be capacity for further recovery of upper-limb function in chronic stroke that persists at least in the short term.
Introduction
Observation of human actions has been reported to activate similar brain regions that are engaged when these actions are overtly executed.1,2 This network of neurons is known as the mirror neuron system.3,4 When an action is observed, however, with the intention to imitate the observed action, there is maximal activation of the mirror neuron network. 5 This neural level relationship between observation of action and action execution is also explained by the common-coding hypothesis at the behavioral level, where training perception can contribute to an action task and training action can contribute to a perception task.6,7 Accordingly, there is evidence that motor skills that are usually acquired with repetitive task-specific practice can also be acquired through observation of the motor skill alone.8,9
The capability of action observation to prime the motor system through the mirror neuron network provides a mechanism for promoting neuroplasticity and restitution of motor function after stroke hemiparesis that would otherwise be limited to use-dependent interventions.8,10 Recovery of function after stroke that is purportedly facilitated by engagement of the mirror neuron system has been attributed to reorganization within damaged areas and formation of new receptive fields as well as cortical remapping and substitution, with healthy tissues taking up functions of damaged areas.3,11,12 A recent functional magnetic resonance imaging (fMRI) study 13 compared neural activation during action observation in nondisabled age-matched individuals and those with left hemisphere stroke affecting the dominant right hand. Results demonstrated greater activation of the mirror neuron network in the left lesioned hemisphere of stroke survivors during observation of right-hand actions than that for nondisabled controls observing right-hand actions. Furthermore, in the stroke group, those with larger lesions involving regions of the mirror neuron network exhibited compensatory activation of adjacent brain regions during right-hand action observation. These important findings suggest that action observation (perception) and motor execution (action) regions in at least this limited sample of 12 are linked with perception-action coupling that appears to be preserved after stroke. Collectively, a theoretical basis exists for action observation training based on the linkage between perception and action through the induction of neuroplastic processes.
Evidence on the effectiveness of action observation as a tool for stroke rehabilitation is equivocal. Based on a focused literature search using the search phrase “action observation training in upper limb stroke,” only 5 studies were found that used action observation with physical practice to promote upper-limb recovery after stroke; 4 examined chronic and 1 examined acute stroke.14-18 These studies examined the use of action observation with physical practice compared with a conventional physical therapy group, 17 a control group that observed random images and geometric shapes,14,15 a control group completing no intervention, 18 and a control group that engaged in physical practice alone. 16 Findings of these studies vary—from the reports of Cowles et al 17 citing no differences between action observation and conventional physical therapy groups in acute stroke, to other reports of varying levels of improvements across a variety of outcome measures after action observation with physical practice compared with control groups.14-16,18
There are several methodological limitations of previous studies that are important for determining the value of these interventions and for understanding the nature of the effects on stroke recovery. First, the duration of action observation organized as a block ranged from 1 to 2 minutes up to 6 minutes, followed by a block of physical practice of a number of actions that ranged from 2 to 6 minutes, with 1 exception 16 in which participants practiced actions simultaneously (ie, imitation) while observing video clips of those actions. There is compelling evidence that once the mirror neuron system is primed through action observation, it remains engaged until the end of the performance sequence of the executed action. 19 Therefore, if the purpose of action observation is to prime the motor system through the mirror neuron network, then it follows that the action observation and opportunity to perform the action need to be contiguous in time to maximize the priming effect. Second, previous studies have not consistently included a physical practice control condition or group; hence, it is not possible to determine the additive benefit of action observation coupled with physical practice to recovery of functional skills. Given that it is well known that high levels of practice can enhance recovery even in chronic stroke, it is important to decouple the benefits of physical practice alone from action observation plus physical practice. Third, previous studies have used outcome measures with a limited range of functional motor skills—those primarily focused on grasping and dexterity. Fourth, there is little evidence pertaining to the patient’s perspective about action observation training and the perceived benefits or not, to motor function in chronic stroke survivors.14,15
This study aimed to address these limitations through a modified within-subject, 2-phase (relaxation-sham + practice, action observation + practice) protocol of action observation training in a group of individuals in the chronic stage after stroke. Behavioral evidence that demonstrates the immediate priming effect of action observation on functional recovery in chronic stroke is lacking. Therefore, the purpose of this within-subject consideration-of-concept trial 20 was to include a unique design that alternated action observation with physical practice for each motor task in the intervention phase. Our primary hypothesis, based on recent fMRI evidence 13 and available behavioral evidence,14,15,18 is that chronic stroke survivors will exhibit significant reduction in impairments and improvement in upper-limb function that will be greater in magnitude following the action observation plus practice intervention phase compared with a relaxation-sham plus practice control phase. The secondary hypothesis is that compared with the relaxation-sham plus practice control phase, participants’ self-perception of perceived benefits to motor function will be significantly higher for the action observation plus practice phase. 21
Method
Participants
A convenience sample of participants was recruited from the Australian National Stroke Foundation–facilitated stroke support groups held in Perth suburbs (see Figure 1). A total of 14 chronic stroke survivors (>6 months stroke duration) meeting the inclusion criteria were enrolled.* Inclusion criteria were the following: (1) at least 18 years of age and with no upper limit, (2) not enrolled in a hospital in-patient rehabilitation program at time of participation, (3) some movement in the paretic upper limb (ie, Fugl-Meyer Motor Assessment [FMA] score between 20 and 55; maximum score for FMA is 66 22 ), (4) a score at least 26 out of a maximum score of 30 on the Montréal Cognitive Assessment (MoCA) 23 and able to communicate effectively for assessments and intervention sessions, and (5) able to commit to time requirements of the study. Exclusion criteria were the following: (1) spatial neglect (impairment to the visual field), as indicated by the visuospatial assessment section of MoCA, and (2) located outside of a 60-km radius of Murdoch University’s South Street Campus. The study was approved by Murdoch University Human Research Ethics Committee and registered on the Australian New Zealand Clinical Trials Registry—ACTRN12313000937718. All participants gave written informed consent.
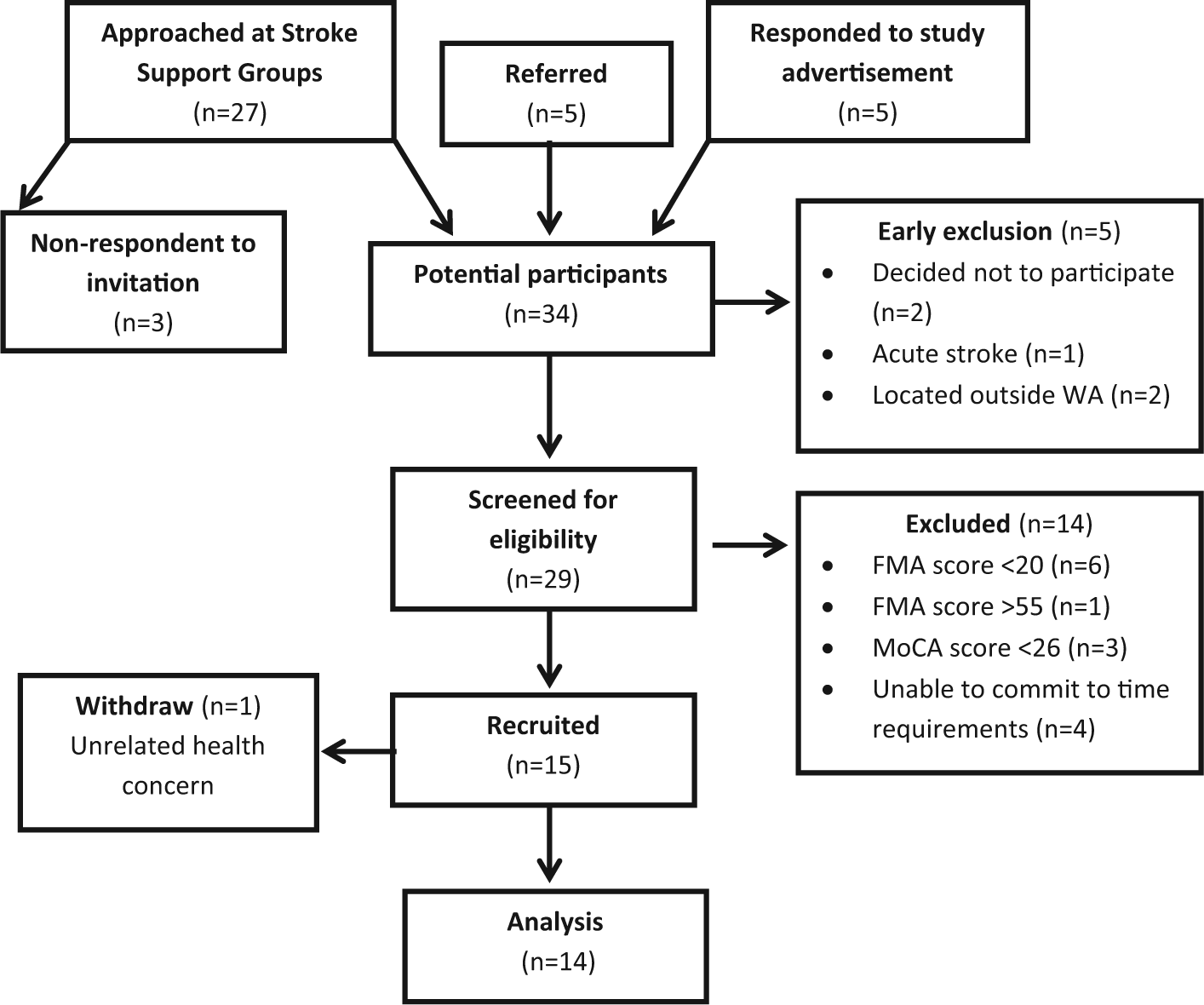
Consort diagram presenting participant flow from sampling to data analysis. Parentheses indicate number of subjects in each process.
Research Design
This study used a within-subject time series design where participants were their own controls. Figure 2 illustrates testing points and phases of the time series design. A pretest was followed by the control phase 1—relaxation-sham plus physical practice—identical to the intervention phase 2 in all aspects, except that the observed video consisted of neutral environmental scenery prior to the opportunity for physical practice of selected motor skills. The purpose of phase 1 was to establish a baseline contribution of physical practice alone to the pretest to posttest 1 change in motor function. Action observation training was delivered in phase 2 followed by a final test point, posttest 2. There was no additional time between the end of phase 1, posttest 1, and the beginning of phase 2. Action observation training included participants watching video footage of selected motor tasks followed by physical practice of the same action. The purpose of phase 2 was to determine the additional benefit, if any, of action observation prior to each motor task practice. This was achieved by comparing primary outcome measures obtained at posttest 1 with those obtained at posttest 2.
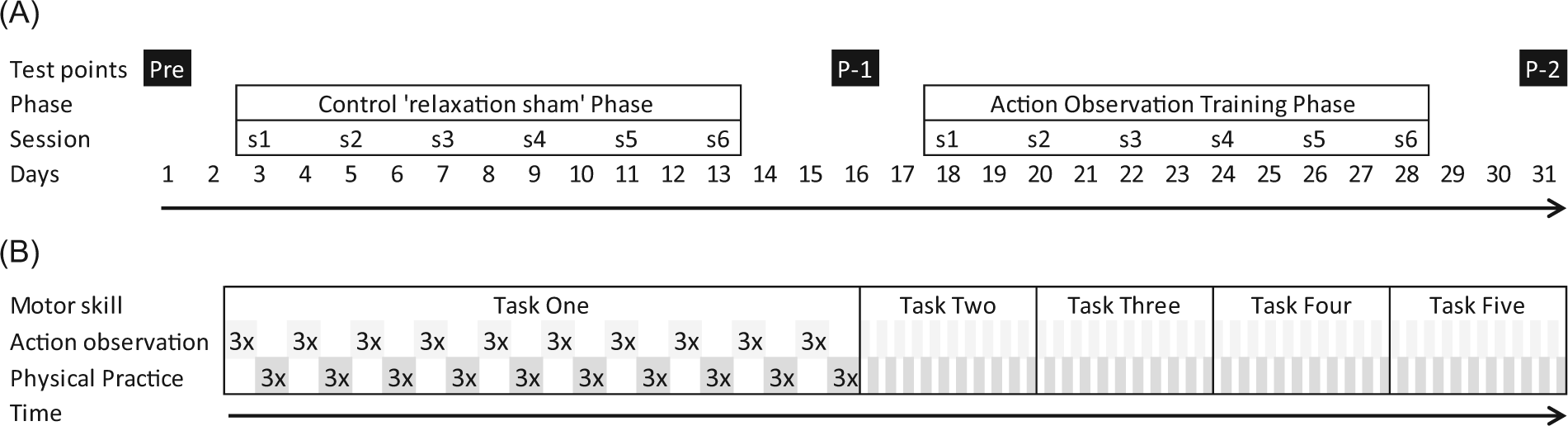
Timeline diagrams of (A) time series design of experiment and (B) structure of individual action observation training sessions. (A) Pre = pretest, P-1 = posttest 1, P-2 = posttest 2, s = session; progression of timeline in days as indicated by arrow. (B) Five different motor tasks are delivered in each session. The average time of individual video clips of the motor tasks is 10 s; this is shown 3 times consecutively followed by physical practice of the motor skill for 3 attempts. This process of observation and immediate physical practice of each motor task is repeated 10 times. Motor tasks 2 to 5 are as per motor task one but have been compressed for illustration purposes. Session time varied between 1 hour and 90 minutes depending on the individual participant level of function and motor skill complexity.
Procedure
FMA, Functional Test of the Hemiparetic Upper Extremity (FTHUE), 24 and an adapted version of the Confidence in Arm and Hand Movement Scale (CAHM) 25 measures were collected at each of the 3 assessment points. In addition to these measures, the Motor Activity Log (MAL) 26 and a structured interview were conducted at post 1 and 2. Testing and training phases were delivered by the same individual, an Accredited Exercise Physiologist (qualified allied health professional). Training sessions were conducted in participants’ homes using a portable table (standard height, 28 inches from ground to table top) that was also used for all assessments. The table was set up in an available open area in the living or dining room. All possible distractions were removed and sources of noise eliminated. Participants were seated at the table in front of a 15.5 inch laptop computer screen for viewing video footage. The screen was positioned 18 inches in front of the participant. The duration of the training session varied between an hour and 90 minutes, depending on task(s) difficulty and participant capability. The common feature of the video footage shared by the 2 training phases was the interleaved structure with environmental scenery or action observation (see eVideo 1 for video clip example of each) followed immediately by physical practice of the motor task within 1 to 2 s.
Motor skills practiced in each phase were selected from 1 of 2 lists (list A or B) designed to be equivalent on a range of tasks. The list of tasks assigned to each was counterbalanced, with half of the participants completing list A in phase 1 and then list B in phase 2, and the other half completing list B in phase 1 and then list A in phase 2.
Phase 1: Relaxation-Sham Plus Physical Practice
Participants were informed that the intention of the environmental footage was to relax them prior to physical practice. These instructions were given in an attempt to ensure that the participants engaged with watching random video images prior to physical practice. During physical practice, verbal instructions and cues were given pertaining to the goal of the motor skill, movement direction, and sequencing of movements to guide participants toward successful completion of the task. In cases where the participant had difficulty performing the task, a series of standardized strategies were suggested by the trainer across all participants. These strategies included trying the motor skill with the unaffected side or breaking the task down into parts and using a part-practice approach involving isolation of components (eg, if unable to grasp draw handle, start by just hooking over fingers and practicing the gross movement of pulling out the draw).
Phase 2: Action Observation Plus Physical Practice
Participants were asked to watch the video footage with the knowledge that they would then attempt to perform the same motor skill task after watching (ie, observation with intent to perform). During physical practice, the exact same verbal instructions were given as in phase 1. In cases where the participant had difficulty performing the task, again, the exact same series of standardized strategies were suggested as in phase 1.
Measures
A single assessor (first author) unblinded to study phase performed all outcome tests. Motor function was assessed with primary outcome measures FMA and the FTHUE. Secondary outcome measures, the CAHM scale and the MAL, as well as a structured interview gauged participants’ perception of their motor function.
Fugl-Meyer Assessment
The FMA is a stroke-specific measure of sensorimotor impairment.22,27 The FMA is among the most commonly used standardized assessment tools and is well recognized as a reliable and valid measure. 27 Interrater reliability of FMA for the single assessor is reported in eMethods 1.
Functional Test of the Hemiparetic Upper Extremity
The FTHUE measures motor function with examination of ability to achieve functional tasks with the hemiparetic upper extremity.24,28 In all, 17 functional tasks are used across 7 levels, increasing in difficulty with each higher level (level requirements can be seen in eTable 1). With the exception of the first task, time to task completion is recorded, with a maximum of 3 minutes allowed for each or 3 attempts, whichever is first. The performance of each functional task is graded plus or minus based on how the task was completed. To achieve a plus grade, the hemiparetic hand must assist functionally within its capability while not impeding progress toward reaching the task goal. Level is awarded as the highest level in which all tasks within the level are achieved as graded with a plus.
Video footage was captured during FTHUE assessment using a standard video camera placed perpendicular to the participant’s hemiparetic side. Captured video footage allowed for multiple observations of the collected FTHUE data for determining interrater and intrarater reliability (interrater and intrarater reliability for the FTHUE are reported in eMethods 2).
Confidence in Arm and Hand Movement Scale
The CAHM scale is a self-efficacy questionnaire in which participants give a rating out of 100%, indicating confidence in ability to use their hemiparetic arm and hand for tasks listed. 25 A rating of 100% indicates that the participant is very certain that he or she can use the hemiparetic arm and hand for the task if attempted, with 0% on the other end of the scale indicating that the participant is very uncertain that he or she could do the task and is reluctant to attempt the task. The CAHM questionnaire was adapted from the original 20-item CAHM and used the same 0 to 100 confidence scale but for each of the 16 timed items of the FTHUE (see eMethods 3).
Motor Activity Log
The MAL uses a rating scale to gauge participants’ reflections on the use of their hemiparetic arm for functional activities at home. 26 Participants are asked to recall use of their hemiparetic arm in 28 items of functional activities around the home over the previous 2 days. In those items that the hemiparetic arm was used, participants indicate a “how well” rating between 0 and 5 of how well the activity was performed (see eMethods 4). A rating of 0 indicates that the hemiparetic arm was not used at all for that activity, and 5 indicates that the ability to use the hemiparetic arm for that activity was as good as before the stroke.
Structured Interview Questions
Based on an open-ended question, “How do you feel about the value of the training completed over the last two weeks for improving the function of your affected arm?” interviews were structured with selection of follow-up questions that depended on the participant’s response 29 (see eFigure 1). At the completion of the study, participants were also asked whether they had preferred or found either the environmental footage or the videos demonstrating the tasks (action observation) more beneficial.
Data Analysis
To determine the relative contribution of the relaxation-sham plus physical practice control and action observation intervention phases to the relevant primary and secondary outcome measures, repeated-measures statistical analyses of raw scores were conducted. FMA and FTHUE (level and number of tasks achieved) are ordinal scale data and, therefore, were analyzed using Friedman’s test comparing across testing points, with post hoc Wilcoxon signed-rank test and Bonferroni adjustment. Minimal clinically important differences (MCID) were estimated for each FMA and FTHUE level and the number of tasks achieved across each phase. Determined point changes from pretest to post 1 and post 1 to post 2 were calculated as a percentage, relative to the complete range of the scale for the FTHUE and the value taken from minimum FMA recruitment score (20) to maximum achievable (66) score for the FMA. 30 FTHUE task time average ratio scale data and CAHM interval scale data were checked for normality of skewness and kurtosis between ±1.96. 31 Repeated-measures ANOVA with post hoc Bonferroni test was used on these measures, comparing across testing points. The Greenhouse-Geisser correction was applied where the assumption of sphericity was not met. CAHM data were also analyzed at the item level to determine which items contributed to CAHM score changes for each phase. Group mean change in scores on each item from pretest to post 1 and post 1 to post 2 were calculated as a percentage change over the value remaining on the 100% rating scale from the previous test point. Ordinal scale MAL average rating and number of items rated were compared across post 1 and post 2 using the Wilcoxon signed rank test. The α level for all statistical tests was set at .05, and for relevant post hoc comparisons, a Bonferroni correction was applied that adjusted the α to .025. Qualitative data from structured interviews were analyzed using content analysis, coding data and enabling themes to emerge. 32 Specifically, terms used by participants in response to questions were collectively mapped under each category (eg, value, feedback), and frequency of terms identified, according to methods outlined by Braun and Clarke. 32
Results
In all, 14 people met inclusion criteria. The group was on average 69 years of age, and 8.7 (range 1.8-41.5) years poststroke, with an upper-extremity Fugl-Meyer score of 33 (range = 21-49 out of 66), indicating moderate upper-limb impairment. Table 1 provides details of participant demographics. The average number of repetitions of physical practice participants actually completed per session was equivalent for the control and intervention phases (177 ± 24 standard deviation [SD]) and ranged between 147 and 300 repetitions across the 14 participants.
Demographics: Participants With Chronic Stroke, Characteristics and Values at Time of Recruitment. a
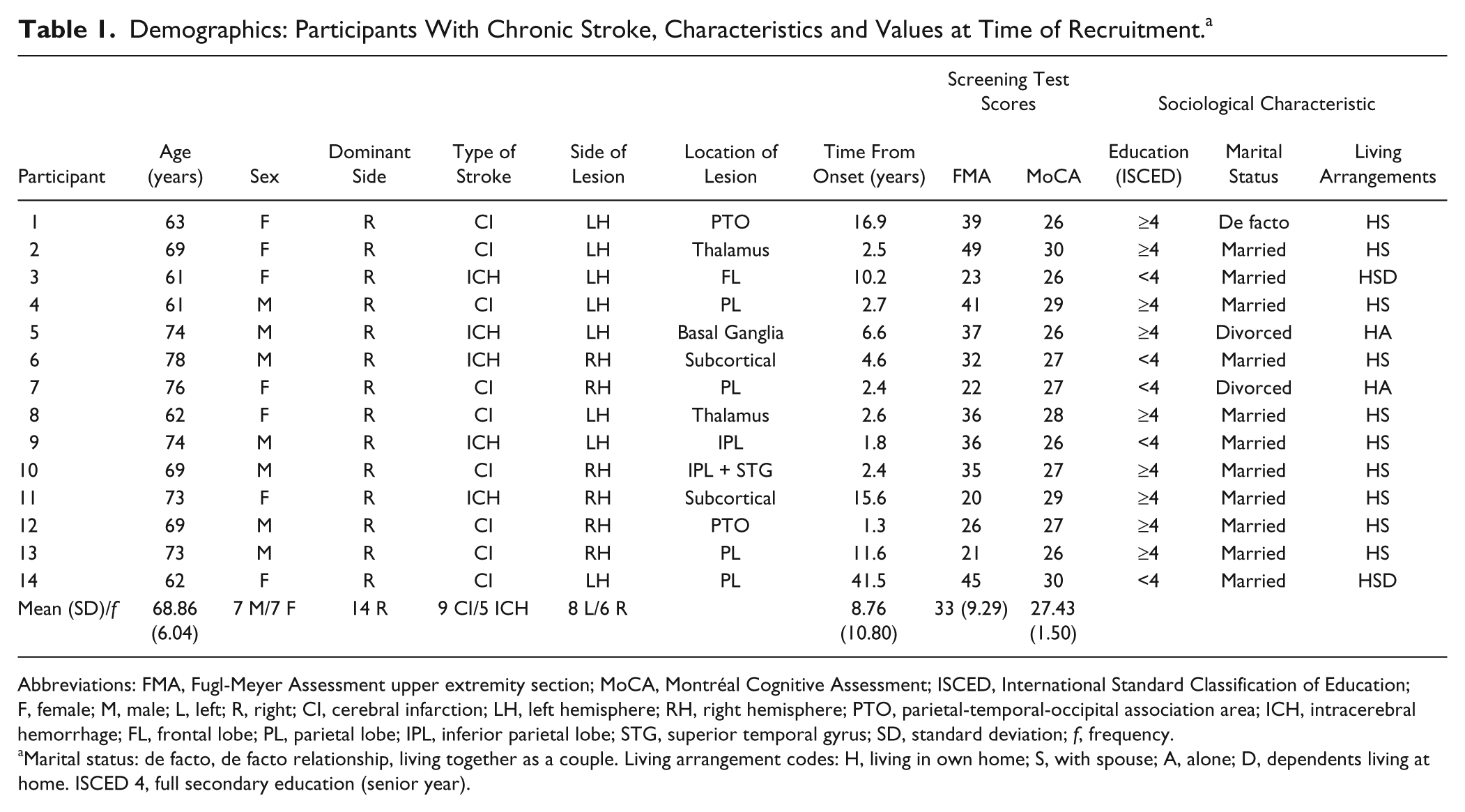
Abbreviations: FMA, Fugl-Meyer Assessment upper extremity section; MoCA, Montréal Cognitive Assessment; ISCED, International Standard Classification of Education; F, female; M, male; L, left; R, right; CI, cerebral infarction; LH, left hemisphere; RH, right hemisphere; PTO, parietal-temporal-occipital association area; ICH, intracerebral hemorrhage; FL, frontal lobe; PL, parietal lobe; IPL, inferior parietal lobe; STG, superior temporal gyrus; SD, standard deviation; f, frequency.
Marital status: de facto, de facto relationship, living together as a couple. Living arrangement codes: H, living in own home; S, with spouse; A, alone; D, dependents living at home. ISCED 4, full secondary education (senior year).
Primary Outcome Measures
Individual participant test scores and group descriptive statistics are reported in Table 2. Friedman’s test indicated a significant difference in FMA scores across time series testing points: χ2(2) = 28.000; P < .001. Post hoc Wilcoxon signed-rank tests revealed a significant difference between baseline to post 1 (Z, = −3.316; P = .001), with a score increase of 6.64 (SD = 10.26) points as well as a significant difference between post 1 to post 2 (Z, = −3.303; P = .001), with a larger score increase of 10.64 (SD = 12.10; see Figure 3A). MCID estimates revealed a 14.4% increase for phase 1 and 23.1% increase for phase 2.
Individual Participant Scores and Group Values for All Outcome Measures Across Time Series Assessments. a
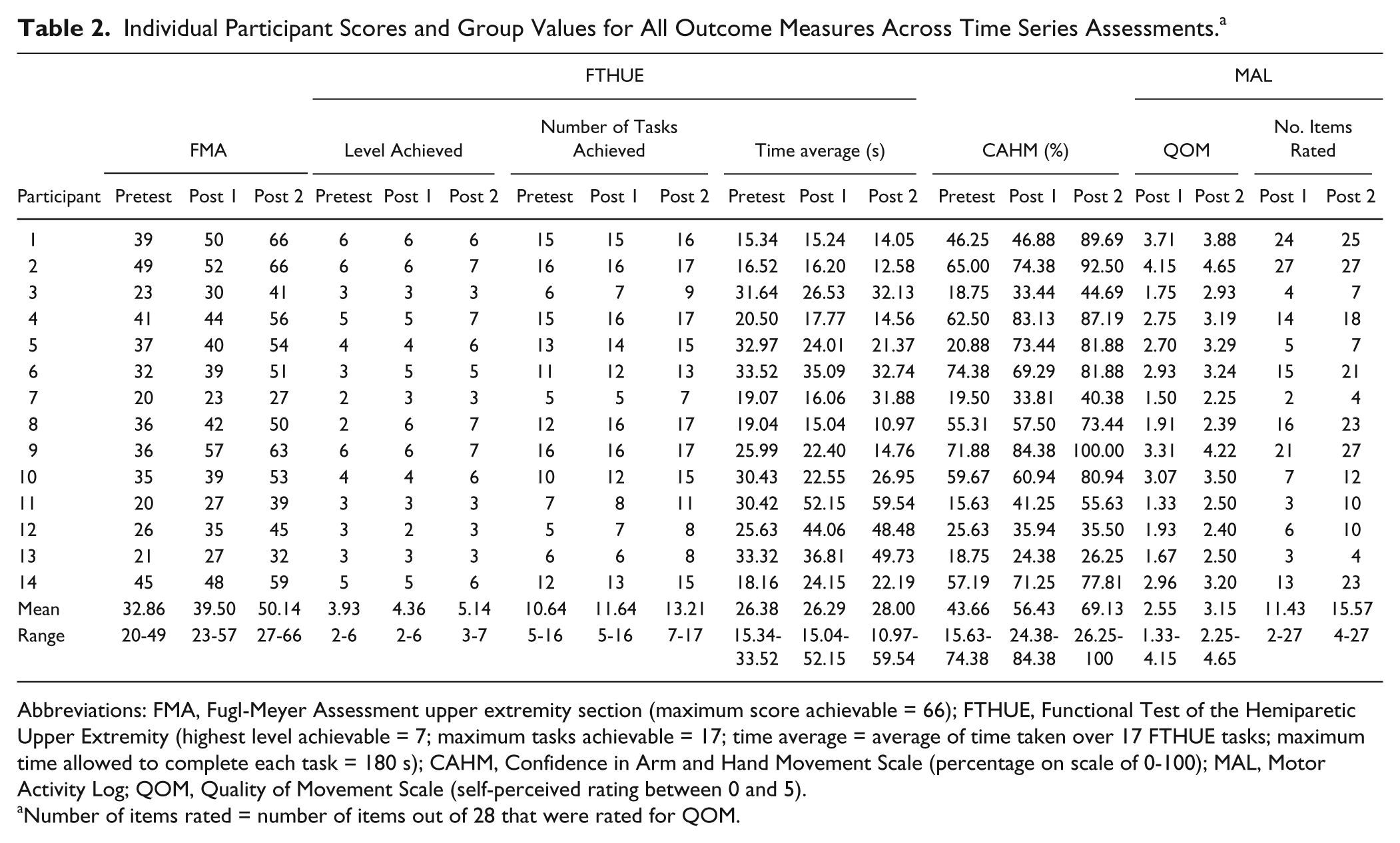
Abbreviations: FMA, Fugl-Meyer Assessment upper extremity section (maximum score achievable = 66); FTHUE, Functional Test of the Hemiparetic Upper Extremity (highest level achievable = 7; maximum tasks achievable = 17; time average = average of time taken over 17 FTHUE tasks; maximum time allowed to complete each task = 180 s); CAHM, Confidence in Arm and Hand Movement Scale (percentage on scale of 0-100); MAL, Motor Activity Log; QOM, Quality of Movement Scale (self-perceived rating between 0 and 5).
Number of items rated = number of items out of 28 that were rated for QOM.
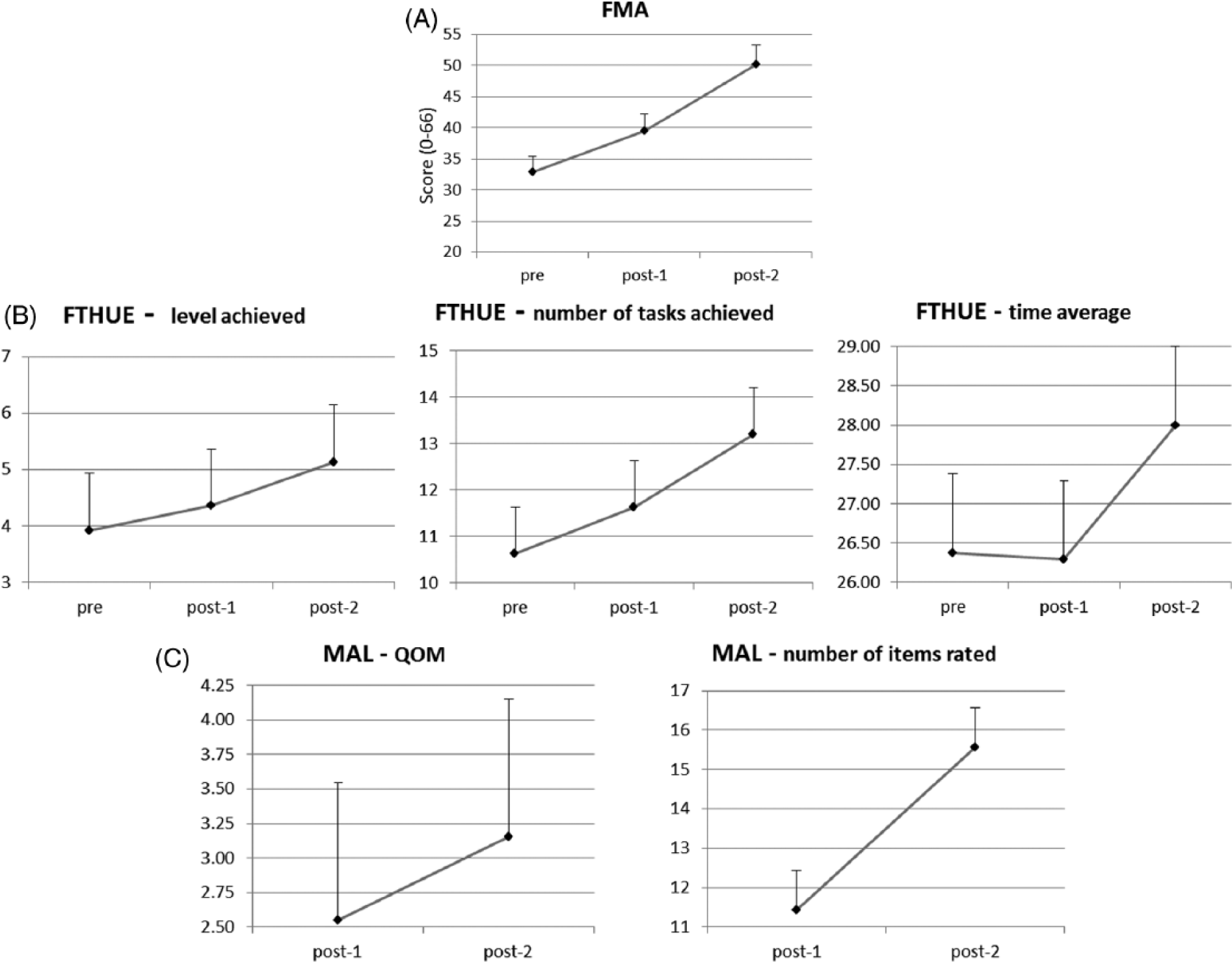
Group means for measures over testing time points: Accuracy of outcome measures denoted by error bars; representing standard error values. (A) Group mean for score achieved on Upper Extremity section of the Fugl-Meyer Assessment. (FMA; score out of 66). (B) Group mean scores for level achieved, number of tasks achieved, and time average on the Functional Test for the Hemiparetic Upper Extremity (FTHUE; level achieved out of 7, tasks achieved out of 17, and time average for tasks achieved in seconds). (C) Group means on the Motor Activity Log (MAL) for Quality of Movement (QOM) and the number of items rated. QOM as rated on “how well” scale between 0 and 5; number of items rated = number of items rated on MAL as having used affected arm for out of 28 items.
Friedman’s test indicated a significant difference in FTHUE scores across time for level achieved and number of tasks achieved, χ2(2) = 14.387, P = .001, and χ2(2) = 26.235, P < .001, respectively. Post hoc Wilcoxon signed-rank tests indicated no significant difference in level achieved from baseline to post 1 (Z, = −1.289; P = .197) despite a score increase of 0.43 points. However, there was a significant increase in level achieved from post 1 to post 2 (Z, = −2.598; P = .009), with a 0.79-point increase. Post hoc analysis also indicated a significant difference in number of tasks achieved between baseline to post 1 (Z, = −2.754; P = .006), with a 1-point score increase as well as a significant difference between post 1 to post 2 (Z, = −3.376; P = .001), with a 1.57-point increase (see Figure 3B). MCID estimates of FTHUE level and number of tasks achieved revealed a 6.1% increase in phase 1 and an 11.3% increase in phase 2, and a 5.9% increase in phase 1 and 9.2% increase for phase 2, respectively. Repeated-measures ANOVA with Greenhouse-Geisser correction revealed that FTHUE average time score across time was not significantly different: F(1.384, 17.992) = 0.331; P = .644.
Secondary Outcome Measures
Repeated-measures ANOVA indicated that mean CAHM scores differed significantly across time: F(2, 26) = 25.72; P < .001. Post hoc Bonferroni test indicated a significant difference from baseline to post 1 (P = .015) and post 1 to post 2 (P = .002). Mean CAHM score increased from baseline to post 1 by 12.76 points and between post 1 and post 2 by 12.70 points. All individual items showed improvements across phases 1 and 2. In phase 2, however, 12 items showed improvements greater than phase 1, with 4 of these items showing at least a 2-fold improvement over phase 1 (eg, item 6, stabilize a package with your weaker hand while wrapping the package with your other hand: 25% improvement over phase 1 vs 59.8% improvement over phase 2).
Wilcoxon signed-rank test showed a significant difference in MAL scores between post 1 and post 2 (Z, = −3.296; P = .001), with a score increase of 0.60 points from 2.55 to 3.15 (see Figure 3C).
Content analysis of structured interviews conducted at post 1 and post 2 demonstrated positive value comments such as feedback on improvements in function of their hemiparetic upper extremity and training aspects participants thought contributed to functional improvements (see Table 3 for more specific details). As regards whether the environmental or action observation footage was valuable, one participant felt as though they did not find a difference between the videos, whereas 13 participants reported that watching video demonstrations of tasks (action observation) was more beneficial.
Themes Drawn From Participant Responses to Structured Interviews Conducted Posttest 1 and Posttest 2. a
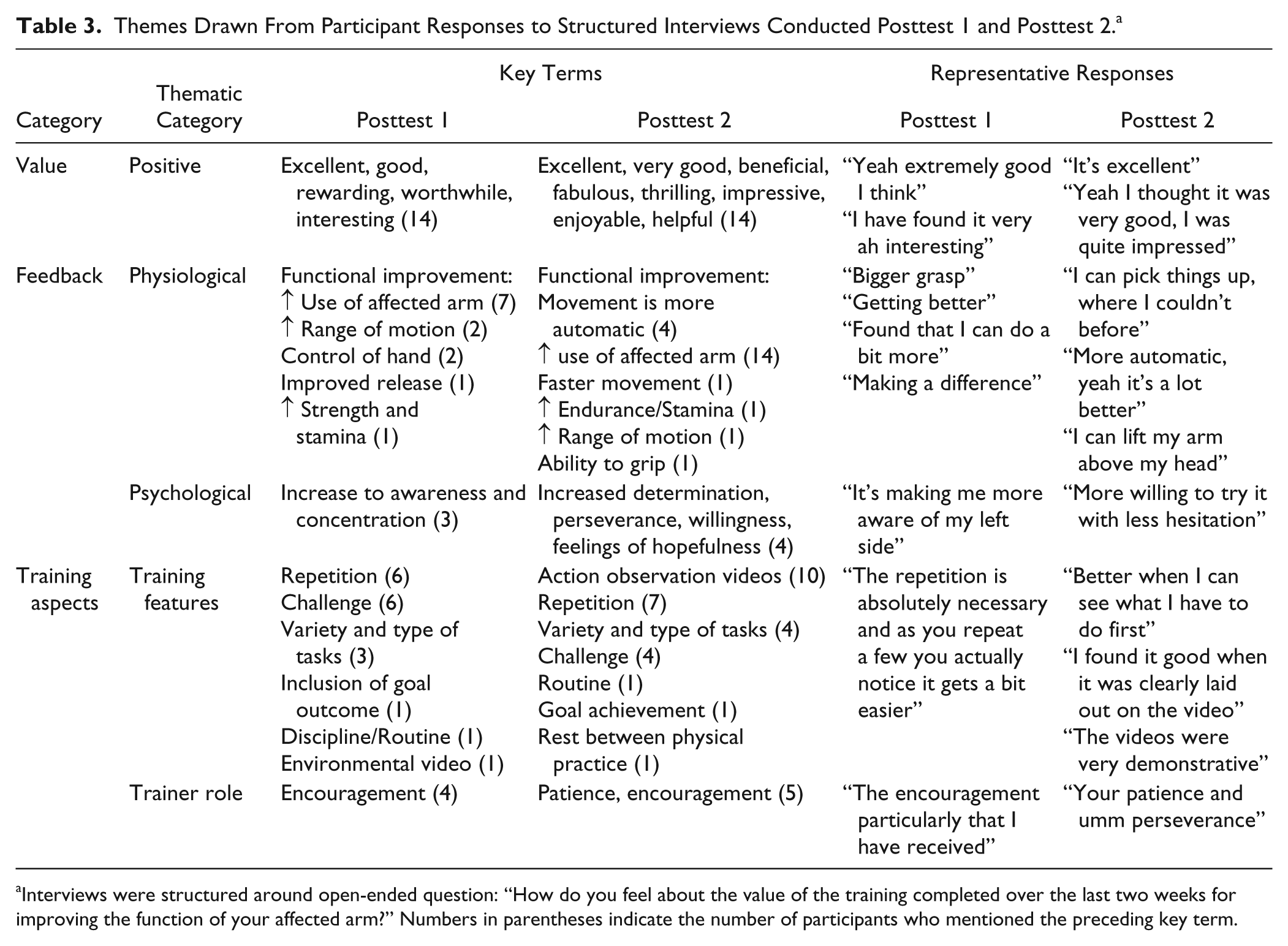
Interviews were structured around open-ended question: “How do you feel about the value of the training completed over the last two weeks for improving the function of your affected arm?” Numbers in parentheses indicate the number of participants who mentioned the preceding key term.
Discussion
This study advances our understanding of how action observation may benefit upper-extremity recovery after stroke. It highlights the unique design in which action observation training was juxtaposed with physical practice soon after observation of each motor skill. This was done in an attempt to provide more optimal activation of the mirror neuron network to prime the motor system for recovery-supportive practice.5,19 The findings support our primary hypotheses, with significantly greater reduction in impairments (ie, FMA) and greater improvements in function (ie, FTHUE) after the action observation training phase than in the relaxation-sham plus physical practice control phase. Our secondary hypothesis was only partially supported with self-perceived benefits found across both phases.
The improvement in FMA scores is consistent with earlier studies of action observation training when considering pre-post change scores. 15 In terms of improvements on the FTHUE there is limited evidence in the literature of improvement in the level and number of tasks achieved. One group (Filiatrault, Arsenault, Dutil, Bourbonnais 33 ) found a strong positive correlation between the FMA and the FTHUE, providing some external validity for the FMA and corresponding FTHUE improvements reported here. The lack of improvement in the time average changes for the FTHUE could have been a result of more difficult tasks with longer movement times overshadowing improvements in easier tasks or a trade-off between attention to quality of movement (ie, skill) for task completion as opposed to time to task completion. Collectively, more immediate priming of the motor system using action observation appears to have yielded greater reduction in impairments and gains in function from the intervention phase compared with the relaxation-sham control phase of this within-subject study.
The improvements to impairment and function that we found are clinically relevant. In particular, the FMA showed a greater magnitude of improvement after the action observation phase, which was more than double the MCID criterion (10%) as reported in the literature.34,35 There is no established MCID for the FTHUE. However, the functional benefits were well over the 10% criterion for the action observation phase but only for FTHUE level achieved. In addition, improvement on the number of FTHUE tasks achieved was near the MCID criterion for the action observation training phase. Therefore, action observation training not only yielded statistically significant improvements to impairment and function, but also these improvements appear to be clinically relevant in that they provide evidence to justify use of action observation training in clinical practice for rehabilitation of upper-limb function in chronic stroke survivors.
Together with physical performance measures, significant improvement was found in participants’ perception of functional capability (self-efficacy) and self-reported use of the paretic arm. Significant improvement in CAHM scores across both control and action observation training phases indicates that confidence in use of the paretic arm continued to improve but was not differentially influenced by action observation or control phases as it was for the functional measures. Improvement of items after the relaxation-sham control phase 1 were primarily those representing static stabilizing movements (eg, stabilize a pillow with weaker arm and put pillow case on with other hand), whereas items that contributed to greater perceived confidence after the intervention phase 2 were those representing more complex movements, such as the capability to combine mass flexion and extension patterns with complete grasp and release. The original CAHM has not been used for assessing self-efficacy in stroke survivors undergoing action observation training. However, Chen et al 25 reported a moderately positive relationship between the CAHM score and FMA score, implying that as impairment is reduced, confidence in paretic arm use continues to improve. This linkage between impairment reduction and increased self-efficacy for use provides one possible explanation for the results herein. It is important to note that the MAL score associated with the intervention phase was significantly higher than that after the relaxation-sham control phase. As such, self-reported use of the hemiparetic arm and hand in activities around the home benefited from the intervention phase of training. Specifically, the MAL average for the group increased from 2.55 (post 1) to 3.15 (post 2) following the intervention phase. A rating of 3 or more is a marker of when the affected arm is used for the activity without assistance from the unaffected arm; it represents a clinically meaningful indicator of improvement. 36 Therefore, action observation plus physical practice training resulted in a reduction in impairment and functional gains that appear to have translated into increases in self-reported use of the paretic arm in daily activities.
Structured interviews revealed that the majority of participants favored the action observation training phase over the relaxation-sham plus physical practice control phase for improving function of the affected arm and hand. Participants found the action observation training videos beneficial, and 4 participants reported the first instances of their movements becoming automatic since stroke occurrence. This theme can be linked with functional improvement on FTHUE with action observation training contributing to achievement of higher levels that combine flexion and extension patterns and require force modulation for more controlled movements. Structured interviews about arm recovery from stroke survivors is limited. For example, Sabini et al 37 used thematic analysis with stroke survivors and reported the theme of repetitive practice, which is consistent with reports in this study, although this study reports the additional theme of the value of action observation training. Collectively, action observation training plus physical practice demonstrated successive benefits to impairment, function, and self-reported use of the arm in daily activities to clinically meaningful levels and positive perception from observation of “normal” actions during rehabilitation, with no evidence of an impediment to confidence in future use of the arm.
A crucial aspect that the within-subject time series design revealed was the additive value of action observation training over relaxation-sham plus physical practice. There are limitations, however, to this design that are outlined below. There is no doubt that task-specific practice leverages use-dependent neuroplastic mechanisms that have been shown to benefit functional recovery of the hemiparetic hand and arm 36 ; the implementation of action observation coupled with physical practice may yield additional benefits to functional recovery. Therefore, it appears that from a behavioral level, action observation contributes to motor relearning in upper-limb stroke survivors—an observation that is consistent with recent evidence at the neural level, where greater (compared with age-matched nonstroke brains) activation of the mirror neuron network is observed in the impaired hemisphere of the stroke brain. 13
In conclusion, this study offers preliminary evidence in support of the effectiveness of action observation with physical practice as a rehabilitation tool that benefits function of the upper limb as well as self-perceptions associated with these improvements in chronic stroke. Furthermore, the use of a within-subject design revealed the added value of action observation over and above that of task-specific practice alone. A single-baseline assessment may have impeded baseline stability in our study; however, other action observation studies have used a single-baseline measure with a similar chronic stroke cohort. 16 Likewise, it may be argued that the lack of a washout period may have caused carryover effects from the sham control phase to the intervention phase. However, because both the control and the intervention phases included physical practice and a counterbalanced order of physical practice tasks from 2 different, but equitable lists, it is less likely that there would be any advantage imparted to the intervention phase from the sham control phase. Future research is needed to address these limitations; a demonstration-of-concept randomized control trial with a larger sample size is warranted to test the robustness of these findings in a between-group design, with blinded assessments and follow-up retention tests as well as inclusion of a neuropsychological evaluation to rule out possible side effects such as depressive bias that might have influenced the motor response, and validation of the adapted CAHM and the structured interview questions is needed to determine the durability of the findings and the added value of action observation with physical practice for promoting functional recovery after stroke.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was part funded by a grant from the McCusker Charitable Foundation.
Supplementary Material
*
Sample size was projected based on changes in functional test scores. 14 G-power statistical analysis software was used to estimate sample size required. Using an effect size of .85, α = .05, and 80% power, analysis indicated a sample size of at least 10 participants.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.